
Abstract
Background
This study examined the association between social determinants of health (SDOH) and access to first-line therapy, time to treatment (TTT), and overall survival (OS) among patients with metastatic non–small cell lung cancer (mNSCLC).
Methods
This retrospective study used data from the Generating Evidence Excellence research environment, incorporating de-identified U.S. patient-level claims, electronic medical records, and neighborhood-level SDOH data from the American Community Survey. Adults with newly diagnosed mNSCLC were included. Patient characteristics, treatment patterns, and SDOH were analyzed descriptively. Kaplan–Meier methods estimated OS, and multivariable logistic regression evaluated associations between selected SDOH and receipt of first-line treatment.
Results
Among 869 patients, median follow-up was 11.5 months; median age was 67 years; 53% were female, 83% were White, and 10% were Black. Overall, 77% (n = 665) received systemic first-line treatment. Among treated patients, 44% received immunotherapy (IO) plus chemotherapy, 22% chemotherapy alone, 20% other IO regimens, and 14% other treatments. Black patients were less likely than White patients to receive first-line IO (odds ratio 0.47; P = 0.0346). Median TTT was longer among Black patients (49 days) compared with White patients (40 days). Median OS was numerically shorter among Black patients (11.2 months) than White patients (13.6 months), though differences were not statistically significant.
Conclusions
Race was associated with differences in first-line treatment patterns and TTT among patients with mNSCLC. Black patients were less likely to receive IO and experienced longer TTT compared with White patients, highlighting potential disparities in treatment access and timing and supporting continued evaluation of strategies to promote equitable cancer care delivery.
Keywords
Introduction
Recent research into health disparities has shifted from single-dimension models to complex, multilevel frameworks integrating biological and social analyses. 1 The medical community's interest in social determinants of health (SDOH) has increased due to their impact on patient outcomes and healthcare costs. 2
The World Health Organization defines SDOH as “the non-medical factors influencing health outcomes, […] the conditions in which individuals are born, grow, live, work, and age, as well as the broader set of forces and systems shaping conditions of daily life. [These] include economic policies and systems, developmental agendas, social norms, social policies and political systems”. 3 Examples include income, social protection, education, unemployment, job security, working life conditions, food insecurity, housing, basic amenities, environmental conditions, early childhood development, social inclusion, and non-discrimination, structural conflict, and access to affordable health services. 3
The United States (US) government Healthy People in 2030 initiative organizes SDOH into five domains: economic stability, education access and quality, healthcare access and quality, neighborhood and built environment, and social and community context. 4 Discrimination based on factors such as race (racism) is a vital issue in the US. 5 Defined as a socially structured action that is unfair or unjustified and harms individuals and groups, discrimination may occur at both structural and individual levels. 5
Traditionally, racism was described as a driver of SDOH through housing and education, but structural racism is increasingly recognized as a distinct SDOH. 6 Studies have identified social factors such as income, education, neighborhood environment, and discrimination based on race/ethnicity that correlate with healthcare outcomes.4,6–12 These factors outweigh healthcare or lifestyle choices, accounting for 30–55% of health outcomes. 3
Neighborhood-level SDOH are better predictors of care delivery than traditional sources of real-world information, such as claims data. They provide greater nuance and contextual understanding of the factors influencing health outcomes. 12
Examining the effects of SDOH on healthcare and patient outcomes presents a challenge owing to limited or absent information on SDOH in health records and insurance claims, and no standardization in the definition, collection, and sharing of SDOH data. 13 Reflecting the growing interest in SDOH, US payer organizations and other stakeholders are collaborating on a unified approach, utilizing International Classification of Diseases, tenth edition, Clinical Modification (ICD-10-CM) codes to standardize SDOH data capture. 14 Data vendors are also leveraging resources to create novel databases containing both patient-level health data and variables such as income, credit scores, crime rates, environmental toxins, social vulnerability, and education, averaged at a state, county, census tract, ZIP code, or neighborhood block level. Combining these data sources to understand the current treatment landscape may help reduce time to treatment (TTT) and healthcare costs.
Lung cancer is the leading cause of cancer-related mortality in the US. 15 The American Cancer Society estimated over 238,000 new lung cancer cases in 2023, along with 127,000 deaths. 16 Lung cancer incidence and mortality rates vary substantially by race/ethnicity; Black males have the highest incidence rate (71.2/100,000 persons) compared with other racial/ethnic groups (35.1–65.3/100,000 persons). 1 This disproportionate incidence persists after accounting for correlations with smoking prevalence. 1 Moreover, patients with non-small cell lung cancer (NSCLC) who are Black, uninsured, or covered by Medicaid, or living in more socioeconomically deprived circumstances are less likely to receive appropriate cancer treatment.17–22 Patients from minority ethnic and racial groups are significantly underrepresented in US lung cancer clinical trials, impacting the generalizability of trial results and the development of effective treatments for this population.23–25 However, research on the influence and interplay of multiple SDOH on the care or outcomes of patients with NSCLC has been limited, particularly in the commercially insured population.22,26
This study aimed to understand how SDOH affect first-line treatment patterns and outcomes within the commercially-insured US population.
Methods
Study design and data source
This retrospective, non-interventional study used data from the Generating Evidence Excellence (GEX) research environment, combining de-identified US patient-level claims, electronic medical records (EMRs), and neighborhood-level (American Community Survey [ACS] census block group level) data on SDOH such as income and education.
Neighborhood-level data within GEX are sourced from the 2017 five-year ACS (census block group level) and the 2017 US Department of Agriculture Food Access Research Atlas (FARA; census tract level) and are linked to patients through geocoding to the nine-digit ZIP code of the patient's most recent available address. These variables are delivered as binary and quintile categories to comply with the Health Insurance Portability and Accountability Act Safe Harbor provision. The study period spanned between Jan 1, 2014, and 31 Mar, 2023.
Patient selection
Patients were included if they had Stage IV NSCLC or an initial diagnosis of NSCLC followed by a metastatic diagnosis in claims on or after the initial diagnosis of NSCLC. The index date was the metastatic diagnosis date and had to fall between Jan 1, 2018, and Mar 31, 2023. Patients had to be ≥ 18 years of age at the index date. Patients were excluded if they had other primary cancers before their index date, evidence of metastatic disease prior to their metastatic diagnosis date, and/or evidence of clinical trial participation at any time during the study period (identified using International Classification of Diseases [ICD], 9th Edition V707 and/or ICD-10 Z006). To be included in the SDOH variable analyses, patients were required to have neighborhood-level tract information.
Study measures
Due to the observational nature of the study, there was no randomization or blinding, and patients were managed according to routine clinical practice. Patients were followed from the index date until the earliest date of the following: disenrollment from the health plan, last observed clinic visit or medication administration, end of study, or death. Baseline demographics and clinical characteristics were calculated for all patients at, or closest to, the index date. These included age, gender, index year, geographic region, length of follow-up, patient status (deceased vs. alive), and Eastern Cooperative Oncology Group (ECOG) performance status (PS).
Treatment patterns for both first-line and second-line therapy were collected during the follow-up period. This included the number and percentage of patients who received first-line/second-line treatment, the regimens used in first-line/second-line, TTT (defined as time from index date to start of first-line, or time from end of first-line to start of second-line), and the duration of first-line/second-line treatment (defined as time between initial first-line/second-line therapy start date and last first-line/second-line therapy end date [end date − start date +1]).
Overall survival (OS) was measured as the time from the index date to the date of death for any reason (event) or until the data were censored.
SDOH were also collected based on the patient's neighborhood block level from the 2017 five-year ACS, as follows:
Socioeconomic status (SES) index: composite population measure of unemployment rate, poverty rate, median household income, median home value, rate of no high school diploma, rate of college degree, and crowding. A numerically higher quintile signifies patients with greater affluence Race: American Indian or Alaska Native, Asian, Black, White, Other/unknown/missing Ethnicity: Hispanic/Latino, not Hispanic/Latino, unknown/missing Insurance type: consumer-directed health plan, preferred provider organization, health maintenance organization, other-insured, unknown The ratio of the population below poverty 200%: The percentage of the population with an income < 200% of federal poverty level. A numerically higher quintile signifies worse status (ie, more impoverished people) Educational attainment of high school or above: the percentage of the population aged ≥ 25 years with a high school degree, General Educational Development certificate, or above. A numerically higher quintile signifies higher educational attainment Educational attainment of less than 9th grade: the percentage of the patient population aged ≥ 25 years with < 9 years of education. A numerically higher quintile signifies lower educational attainment Population geography (urban vs. rural): “urban” denotes urban tracts. De-identification certification requires SDOH record redaction for patients for whom the combination of the values populating the remaining six SDOH variables and the region variable relates to fewer than five census block groups; “one” signifies urban tract (urbanized area or urban cluster) Low-access tract using vehicle access and at 20 miles: “LATractsVehicle20” denotes a food desert, defined as a tract where ≥ 100 households do not have a vehicle, and are > 0.5 miles from a supermarket; 1 signifies low access tract after accounting for vehicle access
Statistical analysis
As this was a retrospective observational study using real-world data, no formal sample size or power calculation was conducted. The sample size was determined by the number of patients meeting prespecified eligibility criteria during the study period. Descriptive statistics were used to describe patient characteristics, SDOH, and treatment patterns. A multivariate logistic regression model was used to analyze any association between SDOH (race, SES index), patient characteristics (gender, age category, region, ECOG PS) and receipt of immunotherapy (IO) vs. chemotherapy as first-line therapy. Other neighborhood-level SDOH variables (e.g., education, poverty ratio, food access, and urbanicity) were examined descriptively but excluded from the multivariable model in order to avoid unstable estimates, owing to small cell sizes and high correlation with the SES index.
Kaplan–Meier product limit estimation was used to generate OS medians and associated 95% confidence intervals (CIs), overall and by race. Patients were further defined by treatment status and divided into subgroups (for demographic and clinical characteristics, SDOH, treatment patterns, and OS) as follows:
Systemic treatment: patients with evidence of any systemic treatment following the index date No evidence of systemic treatment: patients without any evidence of systemic treatment following the index date. The subgroup analyses did not consider evidence of surgery and/or radiation as treatment
Results
Demographic and clinical characteristics
The study included 869 patients (Supplemental Figure 1); median age at index was 67 years, 53% were female, 75% were aged < 75 years. The most common index year was 2018 (30%), followed by 2019 (28%) (Table 1). Most patients were in the Midwest (41%) followed by the South (27%).
Baseline demographic and clinical characteristics.
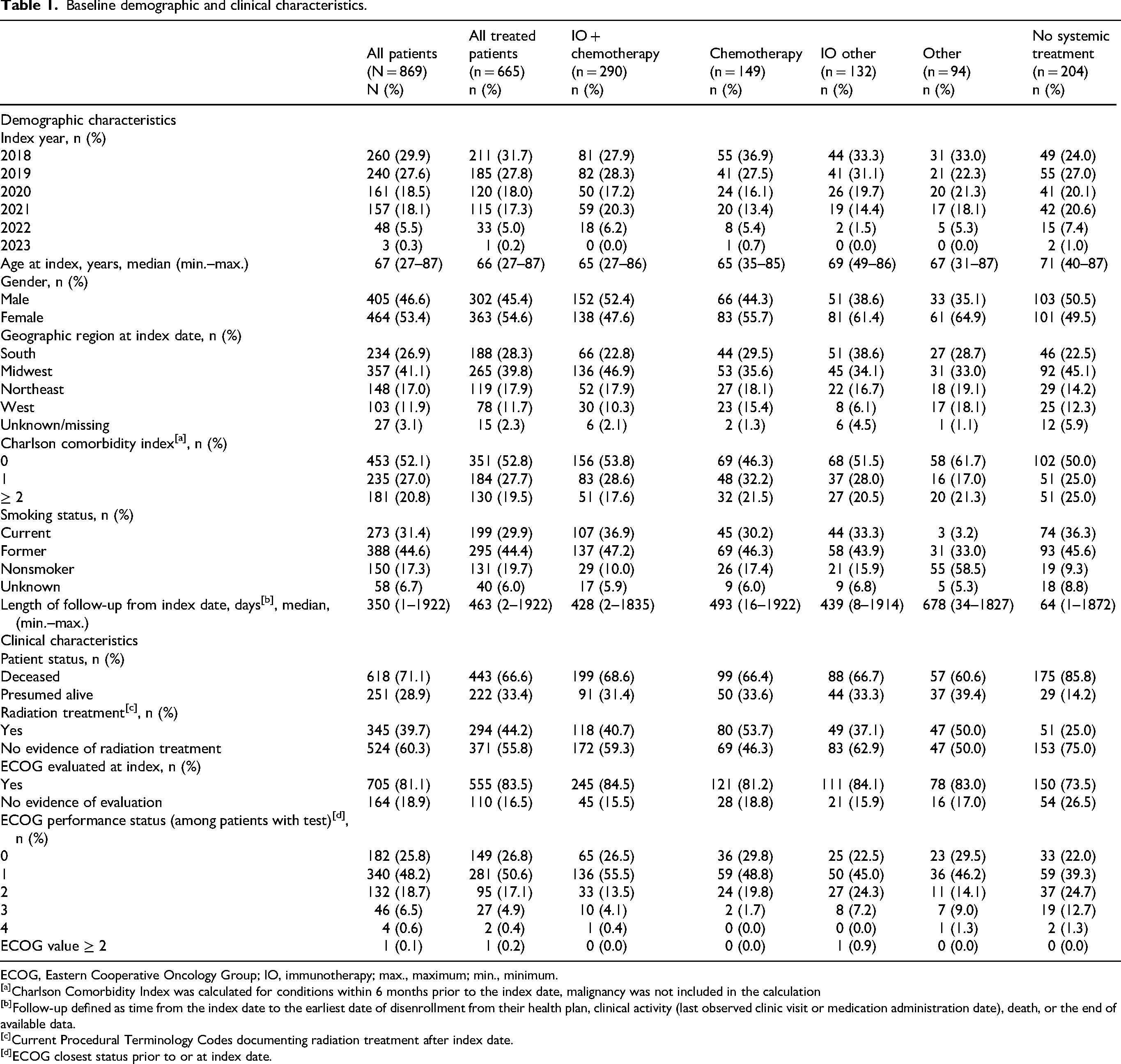
ECOG, Eastern Cooperative Oncology Group; IO, immunotherapy; max., maximum; min., minimum.
Charlson Comorbidity Index was calculated for conditions within 6 months prior to the index date, malignancy was not included in the calculation
Follow-up defined as time from the index date to the earliest date of disenrollment from their health plan, clinical activity (last observed clinic visit or medication administration date), death, or the end of available data.
Current Procedural Terminology Codes documenting radiation treatment after index date.
ECOG closest status prior to or at index date.
Treatment patterns
Of the included patients, 290 received IO + chemotherapy, 149 received chemotherapy, 132 received IO other (these patients had no evidence of chemotherapy at the time of IO initiation), 94 received other medications, and 204 received no systemic treatment (Table 2). The most common first-line treatment regimen was carboplatin, pembrolizumab, and pemetrexed (29%). The median TTT for first-line was 38 days (minimum–maximum: 0–1357), and the median duration of first-line treatment was 64 days (minimum–maximum: 1–1759). The most common second-line treatment regimen was docetaxel and ramucirumab (11%). The median TTT for second-line (time from a first-line end date to second-line start date) was 32 days (minimum–maximum: 0–1429), and the median duration of second-line therapy was 43 days (minimum–maximum: 1–1658).
Treatment patterns.
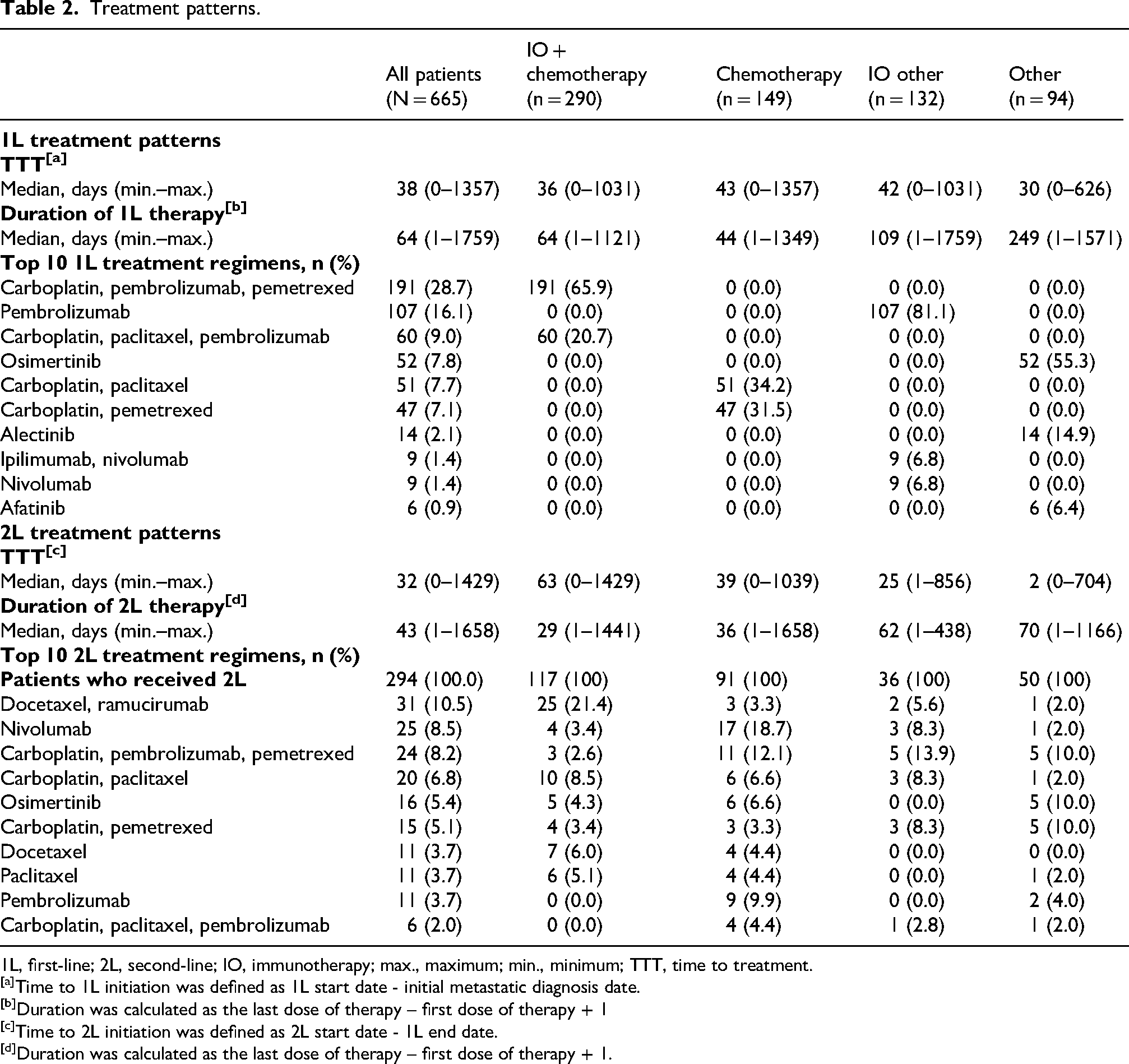
1L, first-line; 2L, second-line; IO, immunotherapy; max., maximum; min., minimum; TTT, time to treatment.
Time to 1L initiation was defined as 1L start date - initial metastatic diagnosis date.
Duration was calculated as the last dose of therapy – first dose of therapy + 1
Time to 2L initiation was defined as 2L start date - 1L end date.
Duration was calculated as the last dose of therapy – first dose of therapy + 1.
SDOH
The largest proportion of patients (29%) were in the 4th quintile (scores from 54.5215 to ≤ 58.234) for neighborhood-area SES which signifies greater affluence (Table 3), and median follow-up was 11.5 months. Most patients were White (83%). Overall, Black patients were less likely to receive IO at first-line than White patients (odds ratio [OR]: 0.47, 95%CI 0.24–0.95, P = 0.0346) (Table 4). Among treated patients with all SDOH variables available (n = 448), median TTT was 40 days (minimum-maximum: 0–1031) in White patients (n = 370), 49 days (minimum–maximum: 9–632) in Black patients (n = 47), and 45 days (minimum-maximum: 11–1357) in other patients (n = 31).
SDOH.
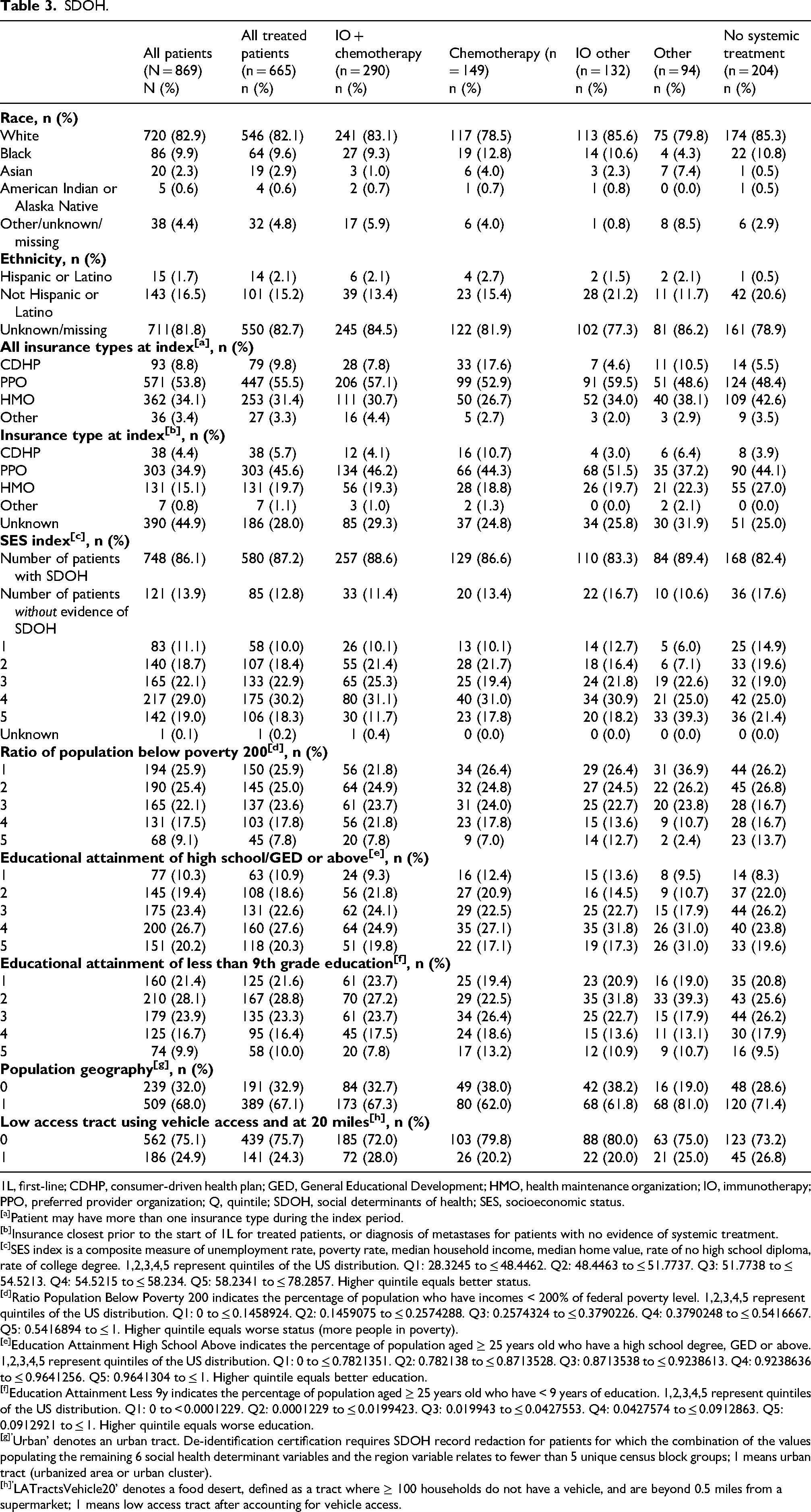
1L, first-line; CDHP, consumer-driven health plan; GED, General Educational Development; HMO, health maintenance organization; IO, immunotherapy; PPO, preferred provider organization; Q, quintile; SDOH, social determinants of health; SES, socioeconomic status.
Patient may have more than one insurance type during the index period.
Insurance closest prior to the start of 1L for treated patients, or diagnosis of metastases for patients with no evidence of systemic treatment.
SES index is a composite measure of unemployment rate, poverty rate, median household income, median home value, rate of no high school diploma, rate of college degree. 1,2,3,4,5 represent quintiles of the US distribution. Q1: 28.3245 to ≤ 48.4462. Q2: 48.4463 to ≤ 51.7737. Q3: 51.7738 to ≤ 54.5213. Q4: 54.5215 to ≤ 58.234. Q5: 58.2341 to ≤ 78.2857. Higher quintile equals better status.
Ratio Population Below Poverty 200 indicates the percentage of population who have incomes < 200% of federal poverty level. 1,2,3,4,5 represent quintiles of the US distribution. Q1: 0 to ≤ 0.1458924. Q2: 0.1459075 to ≤ 0.2574288. Q3: 0.2574324 to ≤ 0.3790226. Q4: 0.3790248 to ≤ 0.5416667. Q5: 0.5416894 to ≤ 1. Higher quintile equals worse status (more people in poverty).
Education Attainment High School Above indicates the percentage of population aged ≥ 25 years old who have a high school degree, GED or above. 1,2,3,4,5 represent quintiles of the US distribution. Q1: 0 to ≤ 0.7821351. Q2: 0.782138 to ≤ 0.8713528. Q3: 0.8713538 to ≤ 0.9238613. Q4: 0.9238636 to ≤ 0.9641256. Q5: 0.9641304 to ≤ 1. Higher quintile equals better education.
Education Attainment Less 9y indicates the percentage of population aged ≥ 25 years old who have < 9 years of education. 1,2,3,4,5 represent quintiles of the US distribution. Q1: 0 to < 0.0001229. Q2: 0.0001229 to ≤ 0.0199423. Q3: 0.019943 to ≤ 0.0427553. Q4: 0.0427574 to ≤ 0.0912863. Q5: 0.0912921 to ≤ 1. Higher quintile equals worse education.
Urban’ denotes an urban tract. De-identification certification requires SDOH record redaction for patients for which the combination of the values populating the remaining 6 social health determinant variables and the region variable relates to fewer than 5 unique census block groups; 1 means urban tract (urbanized area or urban cluster).
LATractsVehicle20’ denotes a food desert, defined as a tract where ≥ 100 households do not have a vehicle, and are beyond 0.5 miles from a supermarket; 1 means low access tract after accounting for vehicle access.
Multivariate logistic model for 1L treatment: any io therapy vs. chemotherapy.
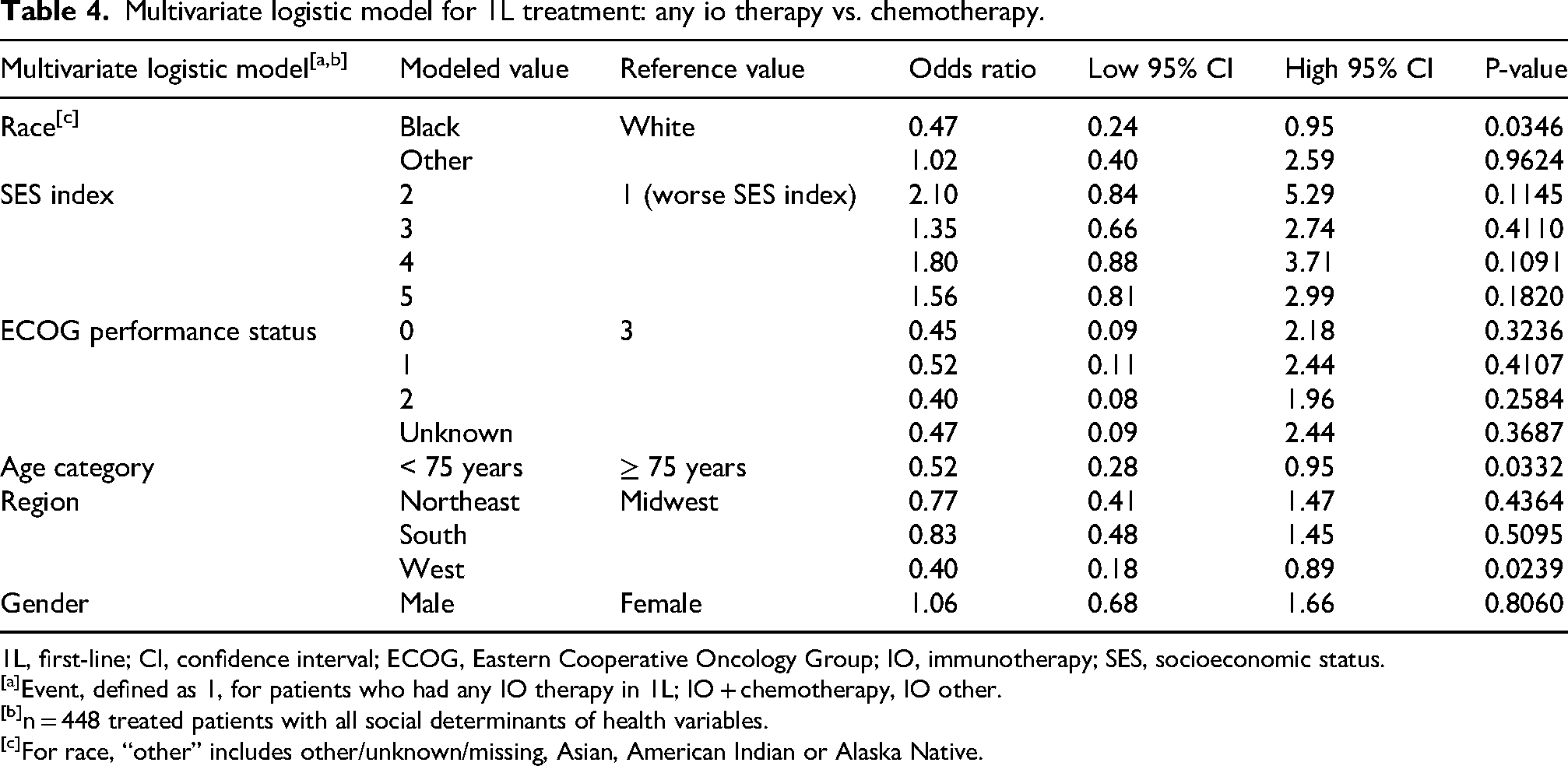
1L, first-line; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; IO, immunotherapy; SES, socioeconomic status.
Event, defined as 1, for patients who had any IO therapy in 1L; IO + chemotherapy, IO other.
n = 448 treated patients with all social determinants of health variables.
For race, “other” includes other/unknown/missing, Asian, American Indian or Alaska Native.
Overall survival
The median OS was 13.6 months (95%CI 11.4–15.9) (Figure 1). Survival probability in the overall population at six months was 67% (SE 1.6%), and 26% (SE 1.7%) at 36 months. Median OS was 11.2 months (95%CI 6.7–20.4) in Black patients and 13.6 months (95%CI 11.1–16.1) in White patients (Figure 1).
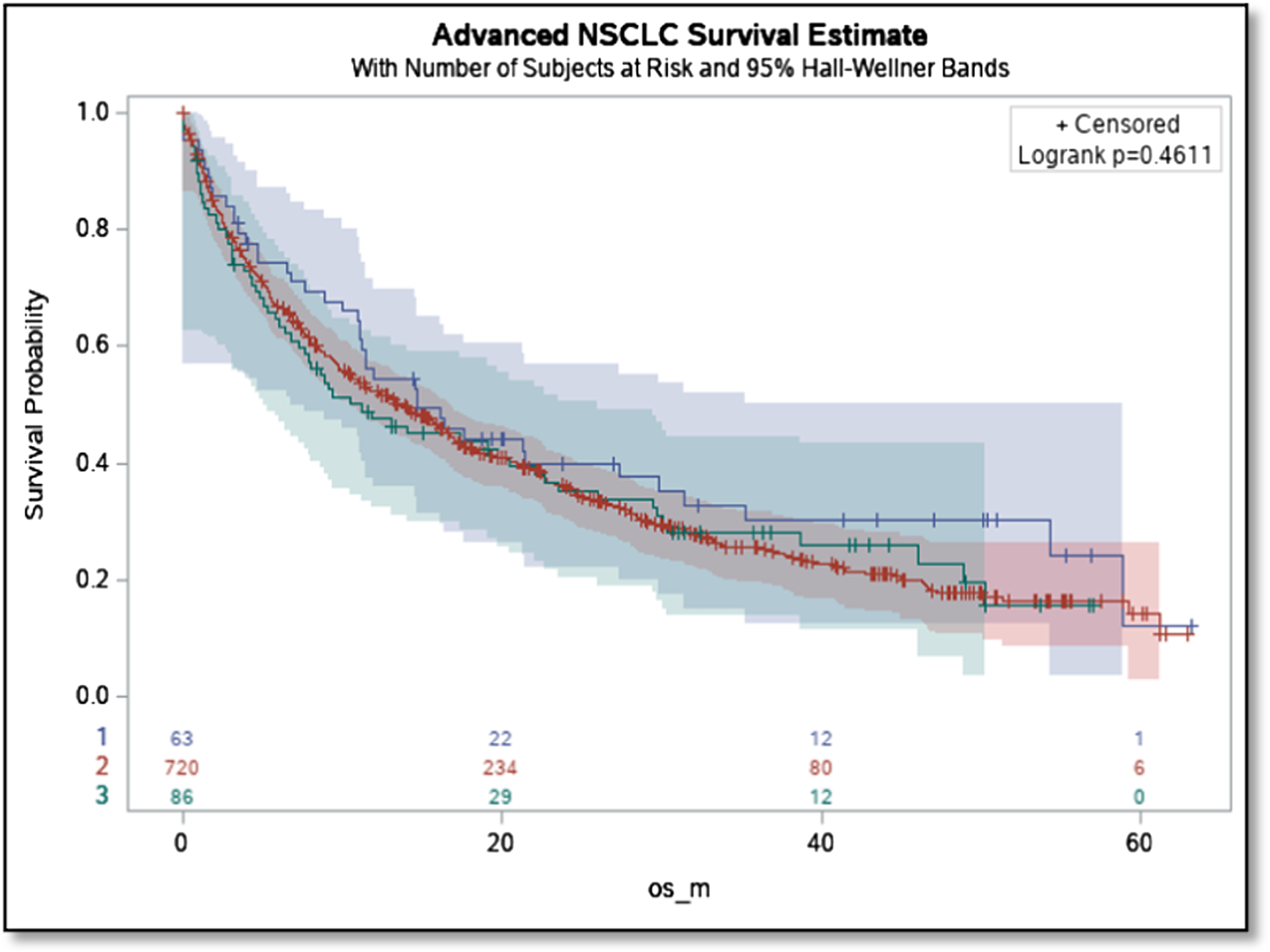
Os by race. NSCLC: non small-cell lung cancer; OS: overall survival. Red: White race; Green: Black race; Purple: Other race.
Discussion
Given the observational design of this study, all findings represent associations and should not be interpreted as causal relationships. In the current study, the racial component of SDOH emerged as an important factor associated with treatment patterns among patients with NSCLC. We observed differences in first-line treatment use by race, with Black patients being less likely to receive IO compared with White patients. Prior studies have reported that Black patients often experience delayed treatment and suboptimal care.27–29 These findings suggest that social and structural factors, such as residential segregation and structural racism, may contribute to observed differences in care delivery. 30 However, the underlying mechanisms could not be assessed in this analysis.
Our findings are generally consistent with previous research demonstrating disparities in immunotherapy use and treatment access by race and socioeconomic context.16,19,31–33 Observations from an earlier study suggest that non-Hispanic White patients with advanced NSCLC residing in higher-income areas were more likely to receive IO than their non-Hispanic Black counterparts. 33 Previous research has also found that Black patients have similar survival compared with White patients when receiving first-line IO. 32
The longer TTT in Black patients observed in our study aligns with previous research showing racial differences in treatment initiation among patients with NSCLC. 34 However, the specific contributors to treatment delays that have been reported in the literature, such as insurance plan requirements, healthcare access barriers, or system-level factors, could not be examined in this study and warrant further investigation.
Although our analysis identified numerically shorter OS among Black patients compared with White patients, this difference did not reach statistical significance. Therefore, survival findings should be viewed as descriptive and hypothesis generating, rather than confirmatory. Prior literature has documented racial differences in lung cancer outcomes that may relate to differences in stage at diagnosis, treatment receipt and access to care.29,31,35–36 However, causal inferences cannot be drawn from the current analysis.
In previous research, when adjusted for clinical and demographic factors, Black patients were less likely to receive any treatment, and when treated were less likely to undergo surgery. Univariate survival for Black patients was worse, and this was the same when accounting for confounding and treatment type. 37 In a more recent study, Black patients were substantially less likely to undergo surgery with curative intent, and lower SES (more pervasive within Black communities in the US) was linked to higher incidence of lung cancer, reduced utilization of surgery, and poorer post-surgical outcomes. 21 In our study, patients residing in neighborhoods with lower SES index were numerically less likely to receive IO than those with a higher index, although these associations were not statistically significant. Together, these findings underscore the importance of continued efforts to promote equitable care delivery, while recognizing the limitations of observational data.
Previous research suggests that improving early detection and ensuring timely, efficacious treatment across populations may reduce disparities in lung cancer outcomes. 38 While our findings cannot establish causality, they support continued evaluation of how social and structural factors intersect with treatment access in metastatic NSCLC.
From an oncology pharmacy and health-system perspective, the observed differences in IO use and longer TTT among Black patients highlight opportunities for targeted, practical interventions, including pharmacist-led efforts to streamline prior authorization processes, proactively monitoring treatment initiation timelines, and facilitation of timely completion and review of biomarker testing. In addition, investments in patient navigator programs and transportation support, along with integrating awareness of neighborhood-level SDOH variables into oncology workflows may help identify patients at increased risk for treatment delays and inform targeted strategies to promote equitable access to care.
Limitations
This study has several limitations related to data source and measurement. The analysis relied on de-identified commercial claims linked to EMR data, which may not fully represent the broader US population with NSCLC and may limit generalizability. Inclusion required availability of neighborhood-level location information, potentially introducing selection bias, and the geographic distribution of patients may not reflect the US population as a whole. Furthermore, neighborhood-level data sourced from the 2017 5-year ACS (census block group level) and the 2017 US Department of Agriculture FARA (census tract level) were categorized into binary and quintile categories rather than reflecting individual-level socioeconomic characteristics.
As with other real-world data sources, the information was not captured for research purposes and may be missing or incomplete. Claims and EMR data lack detailed clinical context and decision-making processes, limiting the ability to determine underlying reasons for observed differences in treatment patterns. Therefore, associations identified in this study, such as lower IO use among Black patients, cannot be attributed to specific factors such as provider recommendations, patient preferences, or structural barriers. Additionally, the dataset lacked detailed molecular biomarker information (e.g., PD-L1 expression, EGFR mutation or ALK fusion) and specific contraindications to immunotherapy, which are key determinants of first-line treatment selection. Although comorbidity burden was captured using the Charlson Comorbidity Index, limited clinical granularity may affect interpretation of treatment patterns and outcomes. Lastly, the treatment landscape for NSCLC evolved during the study period, and patients captured at the beginning of this study may have had different treatment choices than those toward the end, when IO was increasingly available.
Conclusion
Race was associated with differences in first-line treatment patterns among patients with metastatic NSCLC. Black patients were less likely to receive IO therapy and experienced a longer time to initiation of first-line therapy compared with White patients. Although Black patients had numerically shorter OS, this difference was not statistically significant. These findings highlight potential disparities in treatment access and timing and support further evaluation of strategies aimed at reducing treatment delays, improving access to approved therapies, and addressing barriers that may disproportionately impact Black patients and those living in lower SES settings.
Supplemental Material
sj-docx-1-opp-10.1177_10781552261449764 - Supplemental material for Impact of social determinants of health on treatment patterns and outcomes in metastatic non-small cell lung cancer
Supplemental material, sj-docx-1-opp-10.1177_10781552261449764 for Impact of social determinants of health on treatment patterns and outcomes in metastatic non-small cell lung cancer by Nathan R. Hill, Amanda Crosbie, Rick Szymialis, Afraim Botros, Ying Zhang and Umit Tapan in Journal of Oncology Pharmacy Practice
Footnotes
Ethics declaration
This is secondary-use data already approved for research purposes; therefore, institutional review board approval and informed patient consent were not required.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by NRH, AC, RS, AB, and YZ. The first draft of the manuscript was written by NRH, and all authors commented on previous versions of the manuscript. All authors read and approved of the final manuscript.
Funding
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NRH reports a relationship with Bristol Myers Squibb that includes: employment and equity or stocks. AC reports a relationship with Bristol Myers Squibb that includes: employment. RS reports a relationship with Bristol Myers Squibb that includes: employment and equity or stocks. AB reports a relationship with Bristol Myers Squibb that includes: employment. YZ reports a relationship with Bristol Myers Squibb that includes: employment and equity or stocks. UT reports a relationship with GSK that includes: consulting or advisory and travel reimbursement; a relationship with Amgen that includes: consulting or advisory and travel reimbursement; a relationship with Pfizer that includes: funding grants; a relationship with HMP Education that includes: speaking and lecture fees.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.