
Abstract
Background
This exploratory study aimed to assess the impact of temozolomide (TMZ) timing—administered prior to radiotherapy (adaptive pre-RT TMZ) versus standard post-radiotherapy (post-RT TMZ)—on hematological toxicity and survival in adult patients with mixed-grade gliomas with unavoidable treatment delays.
Methods
A retrospective analysis was conducted on 134 patients with World Health Organization (WHO) grade 2–4 gliomas, Karnofsky performance status (KPS) ≥ 50 and residual disease. Cohorts received pre-RT TMZ (n = 39, ≥2 cycles) or post-RT TMZ (n = 95, ≥1 cycle). Progression-free survival (PFS), overall survival (OS), and toxicity were evaluated using multivariate Cox models and Fisher's exact tests.
Results
The median follow up was 88 months. The cohorts were well balanced. The adaptive pre-RT TMZ demonstrated a favorable safety profile; when censoring planned radiotherapy interruptions, severe toxicity-induced delays (> 4 weeks) were absent in the pre-RT arm compared to 11.6% in the post-RT arm (p = 0.033). While adaptive pre-RT TMZ was associated with longer unadjusted median OS (81 vs. 65 months) and PFS (47 vs. 37 months), multivariate analysis revealed no independent survival advantage (OS adjusted Hazard Ratio (aHR) 0.83, p = 0.520; PFS aHR 0.82, p = 0.420). A significant interaction was observed between TMZ timing and Isocitrate dehydrogenase-1 (IDH1) status (OS p = 0.046, PFS p = 0.055). In IDH1 wild-type tumors, adaptive pre-RT TMZ showed hypothesis-generating protective trends for PFS (aHR 0.50, p = 0.057) and OS (aHR 0.50, p = 0.074).
Conclusions
Adaptive pre-RT TMZ is a safe bridging strategy for RT delays, but confers no independent survival advantage in mixed-grade cohorts. Protective trends in IDH1 wild-type gliomas warrant prospective validation, particularly with O(6)-methylguanine-DNA methyltransferase (MGMT) promoter status profiling.
Introduction
Gliomas are the most common primary brain tumors in adults and are characterized by infiltrative growth and derivation from glial cells. Although treatment has progressed incrementally, curative therapies remain elusive in this field. 1 Adult glioma management typically involves maximal surgical resection, radiotherapy (RT), and chemotherapy. A critical concern is the interval between surgery and postoperative RT, during which residual tumor cells may proliferate and lead to recurrence. For low-grade gliomas (LGG), the EORTC 22845 trial showed that immediate postoperative RT improves progression-free survival (PFS) but not overall survival (OS) compared with delayed RT. 2 For high-grade gliomas (HGG), particularly glioblastoma multiforme (GBM), concurrent chemoradiotherapy (CCRT) typically begins within 6 weeks post-surgery. Analysis of WHO Grade 3/4 astrocytomas found that each week of RT delay increased the risk of death by 8.9%, and a 6-week delay reduced the median survival by 11 weeks. 3 Patients with HGG who received CRT ≥ 8 weeks post-surgery showed worse PFS. 4 However, some data indicate that early RT may not be optimal for all patients. A Radiation Therapy Oncology Group (RTOG) database analysis found that patients with GBM who started RT 4 weeks post-surgery had better median survival (12.5 months) than those who started RT within 2 weeks (9.2 months). 5 A study by Lee et al. showed that post-resection patients benefited from CCRT starting beyond 21 days, whereas biopsy-only patients favored earlier CCRT initiation. 6
Given the conflicting results in the literature, this exploratory study aimed to investigate the effects of initiating adjuvant temozolomide (TMZ) treatment prior to standard RT. Specifically, our objective was to capture the realities of real-world clinical management in a high-volume tertiary center, where patients with various glioma grades often face similar logistical delays in radiotherapy. Here, we present our findings regarding early hematological toxicity and long-term survival outcomes in this mixed-grade cohort.
Materials and methods
Study design and population
This retrospective study was approved by the ethics committee and the institutional review board. This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines to ensure rigorous and transparent reporting of our retrospective findings. Medical records from June 2016 to December 2019 were reviewed. The primary objective of the study was to report the early hematological toxicity and survival (overall and progression free survival) outcomes between the post-RT TMZ (one cycle/no adjuvant TMZ before RT) and adaptive pre-RT TMZ (≥2 cycles before RT) groups. The inclusion criteria were as follows: 1) age ≥18 years, 2) WHO grades 2–4 with incomplete resection/residual disease, 3) adjuvant RT and TMZ, and 4) Karnofsky Performance Status (KPS) ≥ 50. The exclusion criteria were as follows: 1) age < 18 years, 2) palliative/hypofractionated RT, 3) definitive RT/CRT, 4) prior RT to the brain/head and neck, and 5) recurrent glioma.
Molecular analysis
IDH analysis was performed using immunohistochemistry with an antibody for the mutant IDH1-R132H protein (H09, Dianova, dilution 1:100), reported as negative, focally positive, or positive. Focal positivity and positivity were both IDH1 mutation positive. ATRX was analyzed using an antibody against the ATRX protein (M/S Sigma-Aldrich).
Adaptive treatment strategy
Patients with RT appointments extending beyond 3 months, or those facing logistical problems starting RT within 28 days received TMZ during the waiting period which was discontinued 4 weeks prior to RT initiation. Patients were subsequently grouped based on TMZ timing into a post-RT TMZ group (≤1 cycle before RT) and an adaptive pre-RT TMZ group. Specifically, ‘adaptive pre-RT TMZ’ was defined as a treatment strategy utilizing at least two cycles of temozolomide as a bridging therapy for patients experiencing logistical delays in the initiation of radiotherapy, rather than a standardized or planned adaptive pre-RT protocol.
Conventional/conformal RT was performed at the discretion of the oncologist. The clinical target volume included the postoperative bed/residual disease, with a 1.5 cm expansion for grade 2 and 2 cm for grade 3/4, including T2 Fluid-Attenuated Inversion Recovery (FLAIR). The Planning Target Volume had a 0.3 cm expansion. Grade 2 patients received 56 Gy in 28 fractions, and grade 3/4 patients received 60 Gy in 30 fractions, with concurrent TMZ at 75 mg/m2 daily. Weekly RT reviews included the hemograms. Adjuvant TMZ was started four weeks post-RT at 150 mg/m2 for cycle 1 and 200 mg/m2 for cycles 2–6 (days 1–5 each 28-day cycle) (Figure 1).
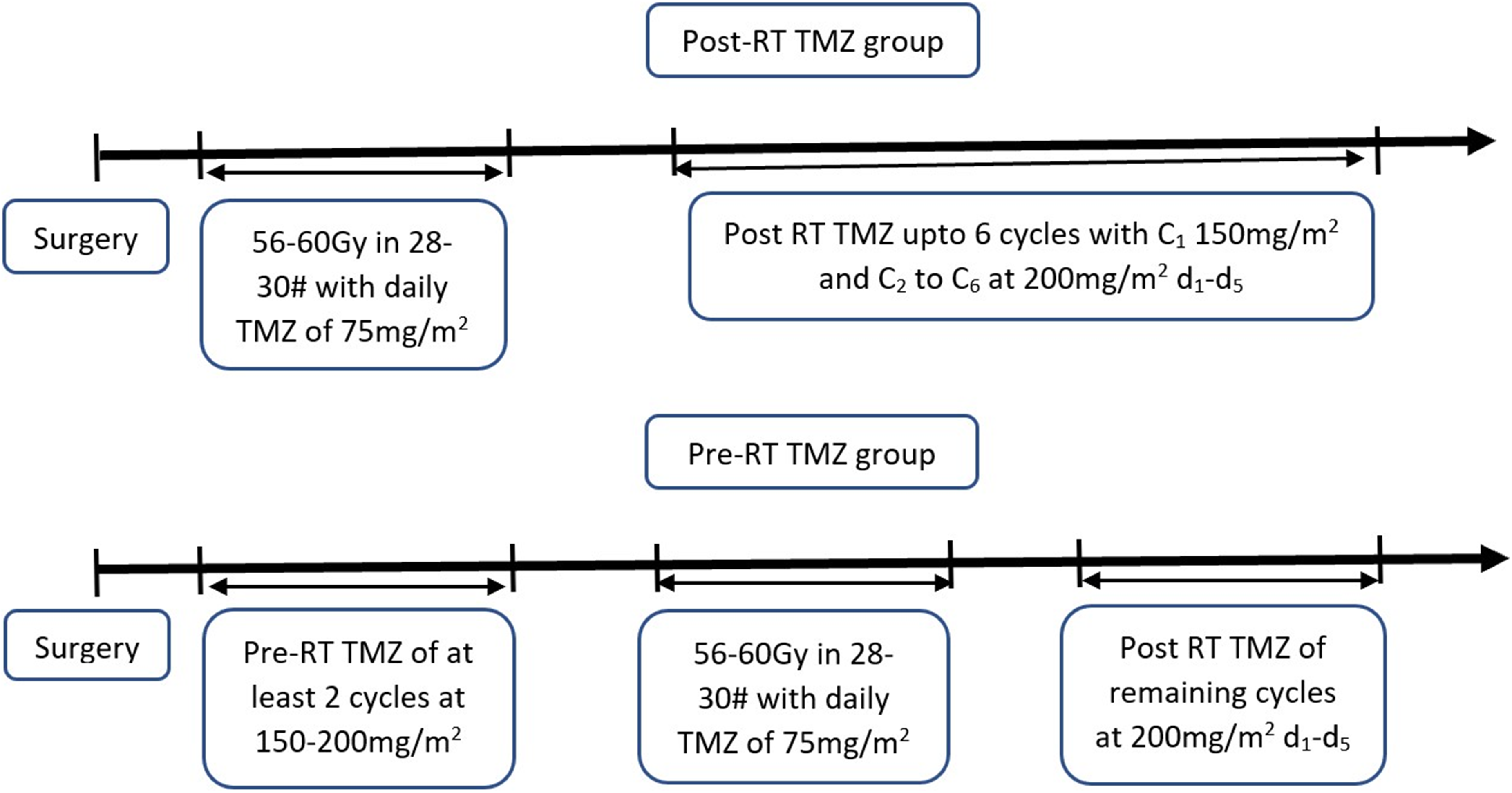
Treatment schema for patient groups.
Toxicity and safety definitions
TMZ toxicity monitoring was performed using a complete hemogram for each cycle. To evaluate the clinical impact and manageability of hematological toxicities, treatment adherence, and toxicity-induced regimen modifications, we systematically analyzed the data. Clinically meaningful dose reductions were defined a priori as a decrease of ≥50 mg/m2 compared to the administered dose of the immediately preceding cycle. True toxicity-induced cycle delays were calculated by measuring the interval between consecutive adjuvant chemotherapy cycles; an interval exceeding the standard 28-day protocol was classified as a delay. To isolate genuine hematological recovery intervals from protocol-mandated logistics, the planned treatment interruption required for the administration of definitive concurrent chemoradiotherapy (CCRT) in the adaptive pre-RT cohort was explicitly censored from the delay analysis.
Response assessment
Patients underwent interim response assessment with brain Magnetic Resonance Imaging (MRI) after three adjuvant TMZ cycles. Post-treatment monitoring included clinical examination every three months and MRI every six months. RT and TMZ toxicities were assessed using the RTOG/EORTC Acute Radiation Morbidity criteria, and treatment response was assessed using the Response Assessment in Neuro-Oncology (RANO) criteria. 7
Statistical analysis
Baseline characteristics were compared between the post-RT TMZ and adaptive pre-RT TMZ groups using Chi-square or Fisher's exact tests for categorical variables and t-tests or Mann-Whitney U tests for continuous variables. To evaluate the clinical impact and manageability of hematological toxicities, treatment adherence, and toxicity-induced regimen modifications, we systematically analyzed the data. The frequencies of categorical toxicity outcomes, including dose reductions, specific weekly delay thresholds, and treatment cessation rates, were compared between cohorts using Fisher's exact test to account for small subgroup frequencies. For survival analysis, progression-free survival (PFS) was defined as the time from surgery to tumor progression or death, and overall survival (OS) was defined as the time from surgery to death from any cause. Survival distributions were estimated using the Kaplan-Meier method, with median survival times and 95% confidence intervals (CIs) calculated, and group differences assessed using the log-rank test. Univariate Cox proportional hazard models were used, followed by multivariate analyses to evaluate the effects of TMZ sequencing effects and identify independent prognostic factors, yielding adjusted hazard ratios (aHRs) and 95% CIs. The proportional hazards assumption was tested; when violated, the variables were analyzed as time-varying covariates. Subgroup analyses were performed to examine the effects of TMZ timing on patient and tumor characteristics and interaction models were evaluated using likelihood ratio tests. All statistical analyses were performed using Stata version 14 (StataCorp LLC, College Station, TX, USA). All statistical tests were two-sided, with a p-value of < 0.05 considered statistically significant.
Results
Patient baseline characteristics and treatment logistics
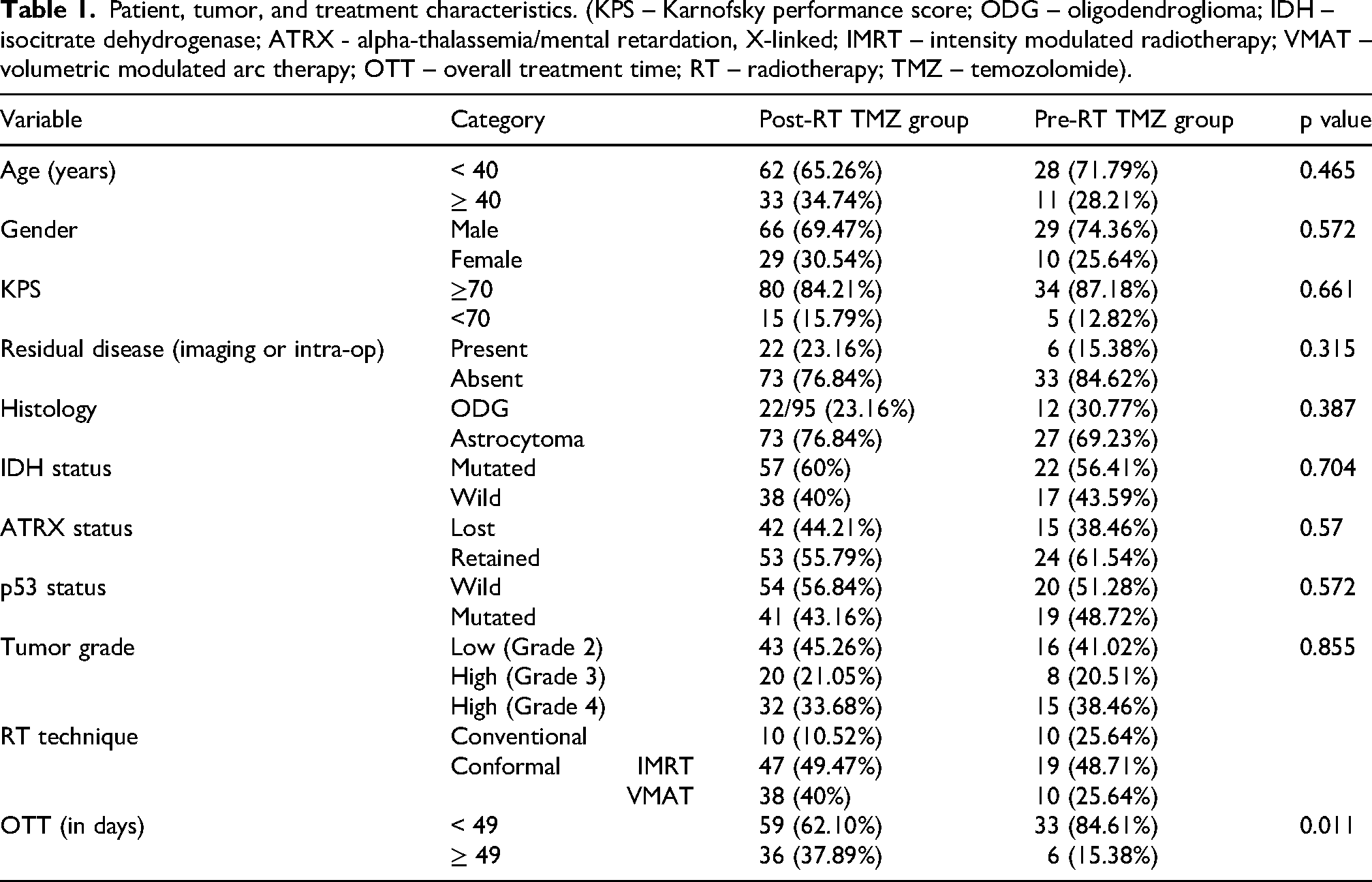
Of the initially screened 885 patients, 134 of them were eligible for the study (Supplementary Figure 1). Baseline clinicopathological characteristics were well-balanced between the post-RT (n = 95) and pre-RT (n = 39) cohorts (see Table 1; p > 0.05 for all). The pre-RT group demonstrated a higher rate of radiotherapy completion within 49 days than the post-RT group (84.61% vs. 62.10%, p = 0.011). Furthermore, the median radiotherapy duration was significantly shorter in the pre-RT arm at 44 days (range, 13–70) than in the post-RT arm at 46 days (range, 19–113) (p = 0.0049).
Patient, tumor, and treatment characteristics. (KPS – Karnofsky performance score; ODG – oligodendroglioma; IDH – isocitrate dehydrogenase; ATRX - alpha-thalassemia/mental retardation, X-linked; IMRT – intensity modulated radiotherapy; VMAT – volumetric modulated arc therapy; OTT – overall treatment time; RT – radiotherapy; TMZ – temozolomide).
Hematological toxicity and clinical manageability
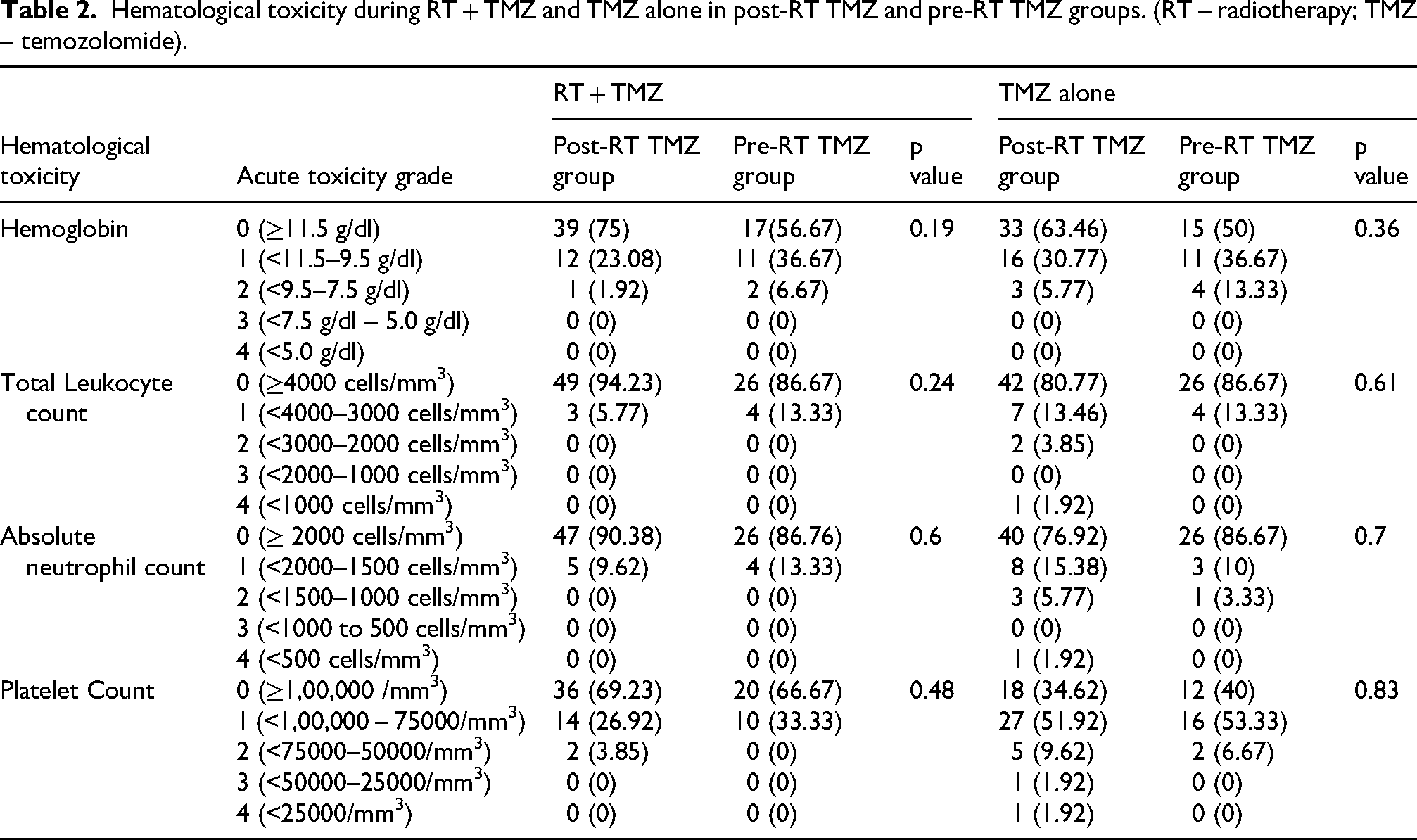
Hematological toxicity profiles during concurrent chemoradiotherapy and TMZ monotherapy phases showed no significant differences between the treatment groups (see Table 2). Treatment tolerability was high, and permanent chemotherapy discontinuation due to unmanageable toxicity was rare. One patient in the post-RT cohort developed grade 4 leukopenia, neutropenia, and thrombocytopenia during adjuvant therapy. The need for clinically meaningful dose reductions—defined as a ≥ 50 mg/m2 decrease from the preceding cycle—was comparable; 7.37% (7/95) in the post-RT group versus 12.82% (5/39) in the adaptive pre-RT group (p = 0.31).
While tolerability was similar, notable differences emerged regarding treatment adherence and timelines. Adjuvant treatment completion rates were 54.7% (52/95) in the post-RT group and 76.9% (30/39) in the adaptive pre-RT group. To isolate the true hematological recovery intervals, we censored the planned radiotherapy window. Following this, toxicity-induced delays exceeding 2 weeks were noted in 24.2% of post-RT patients compared to only 7.7% of adaptive pre-RT patients (p = 0.031). Most notably, severe toxicity delays of over 4 weeks were recorded in 11.6% of the post-RT arm, whereas no patients (0%) in the adaptive pre-RT arm experienced delays of this magnitude (p = 0.033). The comparative analysis of clinical treatment intensity and recovery intervals are presented in Supplementary Table 1.
Hematological toxicity during RT + TMZ and TMZ alone in post-RT TMZ and pre-RT TMZ groups. (RT – radiotherapy; TMZ – temozolomide).
Treatment chronology
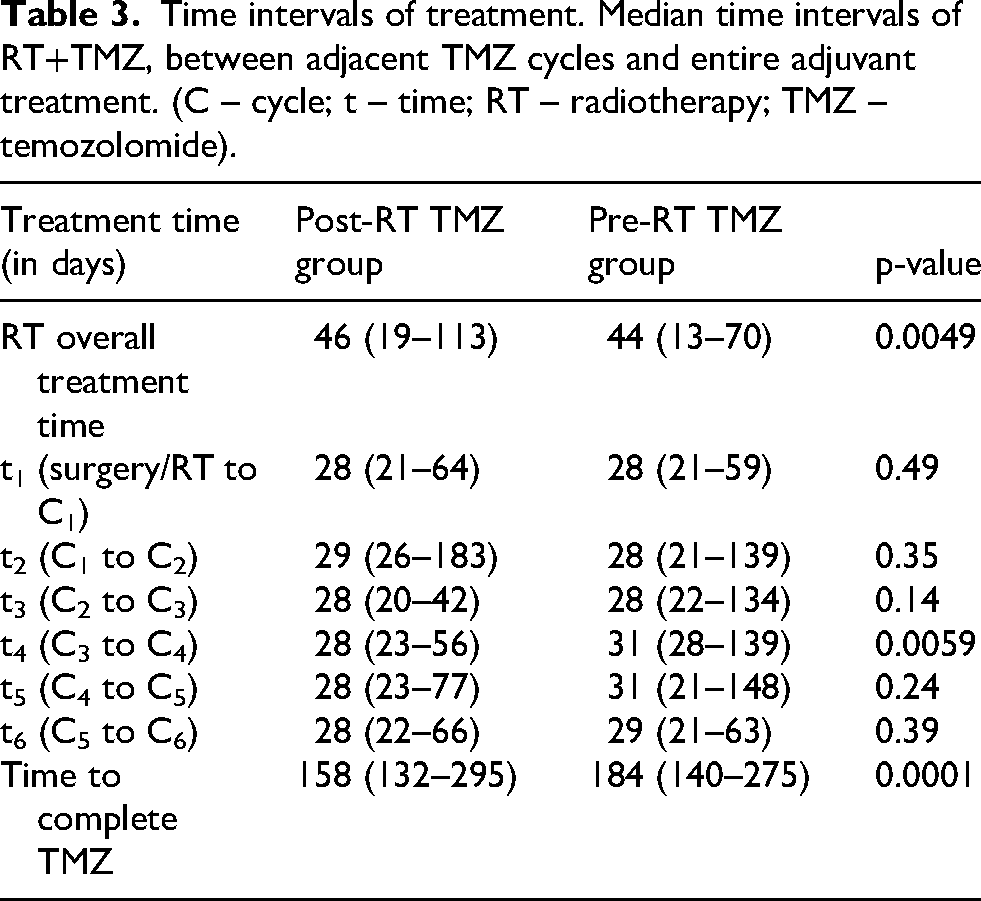
The median follow-up period for the entire cohort was 88 months (95% CI: 83–91). Regarding adjuvant treatment chronology, the median interval from surgery or radiotherapy completion to the first TMZ cycle (t1) was 28 days in both groups. The inter-cycle intervals for cycles 1–3 and 5–6 showed no significant differences between the cohorts. However, the median interval between the third and fourth cycles (t4) was significantly shorter in the post-RT group (28 days, range 23–56) than that in the adaptive pre-RT group (31 days, range 28–139; p = 0.0059). The overall median duration of the planned TMZ course was shorter for post-RT patients (158 days, range 132–295) than for adaptive pre-RT patients (184 days, range 140–275; p = 0.0001) (Table 3).
Time intervals of treatment. Median time intervals of RT+TMZ, between adjacent TMZ cycles and entire adjuvant treatment. (C – cycle; t – time; RT – radiotherapy; TMZ – temozolomide).
Survival outcomes and independent predictors
The median OS was 65 months (95% CI, 50–90 months), and the median PFS was 41 months (95% CI, 27–56 months). Given the biological heterogeneity inherent in a mixed-grade population (WHO grades 2–4), these pooled estimates are provided solely for descriptive context and should be interpreted with caution. The post-RT TMZ group (n = 95) showed a median OS of 65 months (95% CI: 45–90) and PFS of 37 months (95% CI: 24–56). The adaptive pre-RT TMZ group (n = 39) had a median OS of 81 months (95% CI: 41–Not Reached) and PFS of 47 months (95% CI: 21–73). Table 4 shows survival rates at 12, 24, and 60 months. KPS, histology, Grade, IDH1 status, and p53 status showed significant differences in PFS and OS within the groups (Figures 2 and 3).
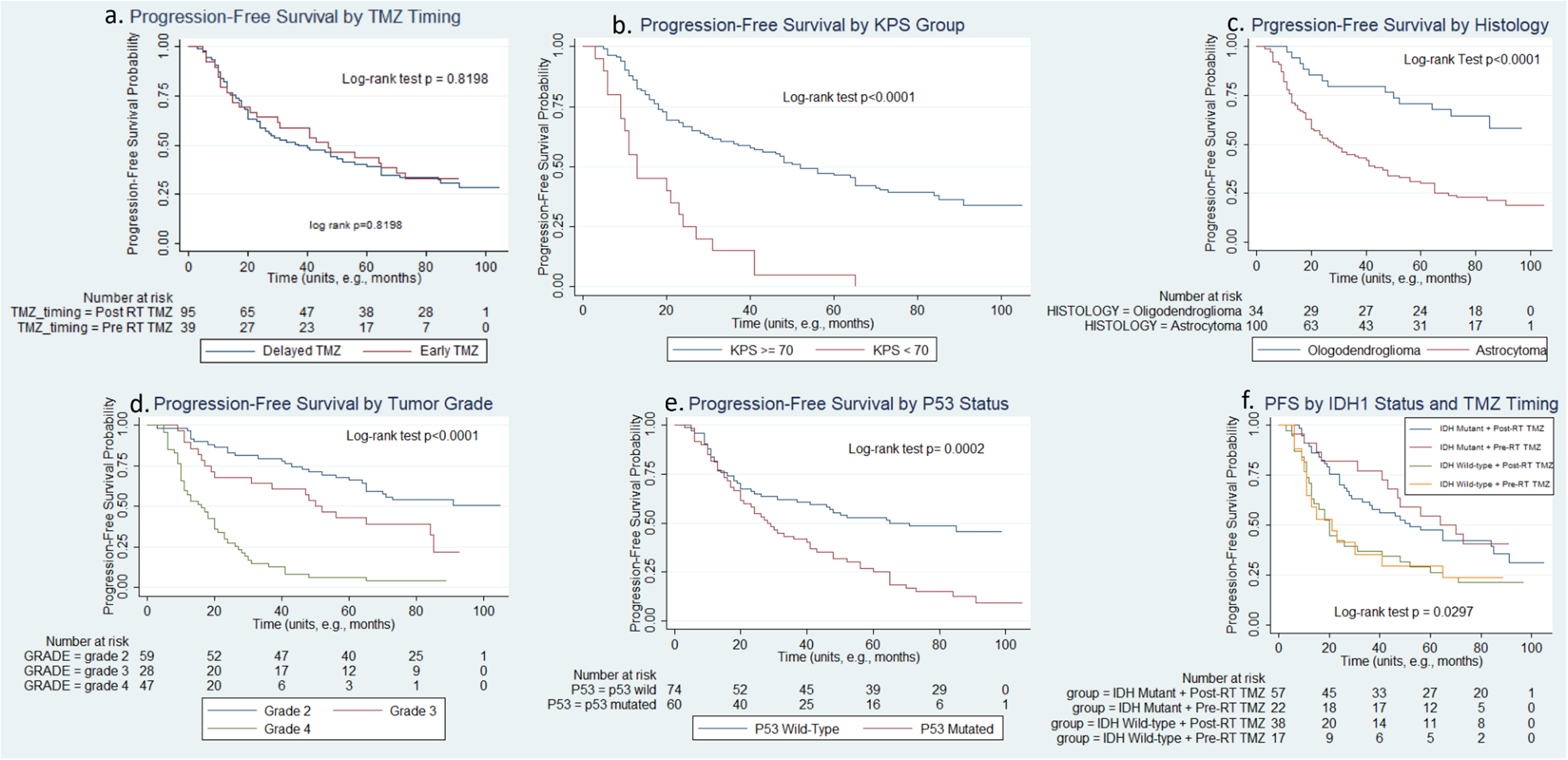
Kaplan-Meier Curves for Progression-Free Survival (PFS). (a) PFS by TMZ Timing (b) PFS by KPS Group (c) PFS by Histology (d) PFS by Tumor Grade (e) PFS by P53 Status (f) PFS by IDH1 Status and TMZ Timing. Each panel displays Kaplan-Meier curves for Progression-Free Survival (PFS), with log-rank test p-values and the number of patients at risk indicated.
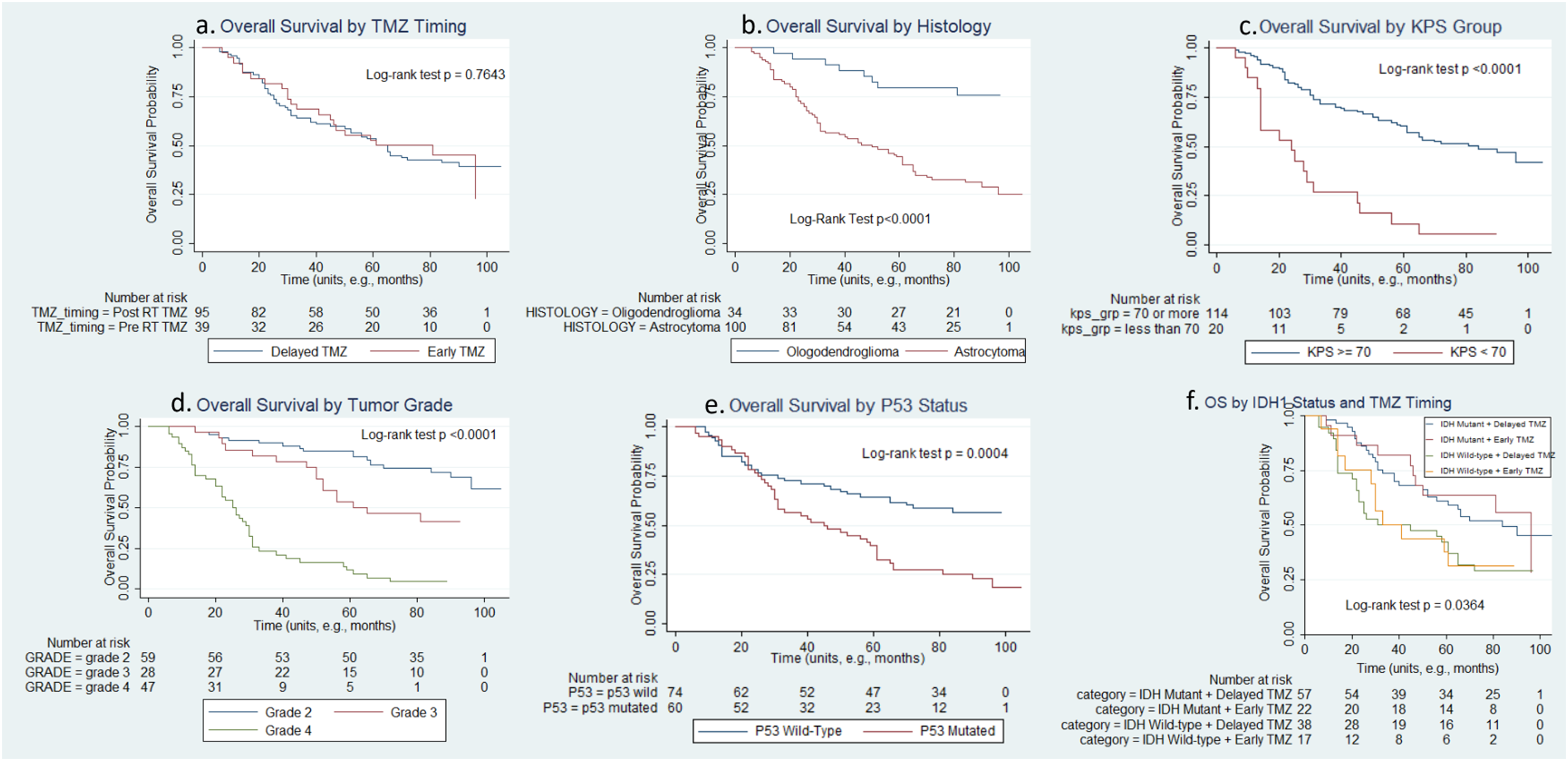
Kaplan-Meier curves for overall survival (OS). (a) OS by TMZ Timing (b) OS by Histology (c) OS by KPS Group (d) OS by Tumor Grade (e) OS by P53 Status (f) OS by IDH1 Status and TMZ Timing. Each panel displays Kaplan-Meier curves for Overall Survival (OS), with log-rank test p-values and the number of patients at risk indicated.
PFS and OS survival times. Progression-free survival (PFS) and overall survival (OS) rates for the entire cohort and stratified by temozolomide (TMZ) timing. (PFS - progression-free survival; OS - overall survival; RT - radiotherapy; TMZ - temozolomide. Data are presented as probabilities with 95% Confidence Intervals in brackets).

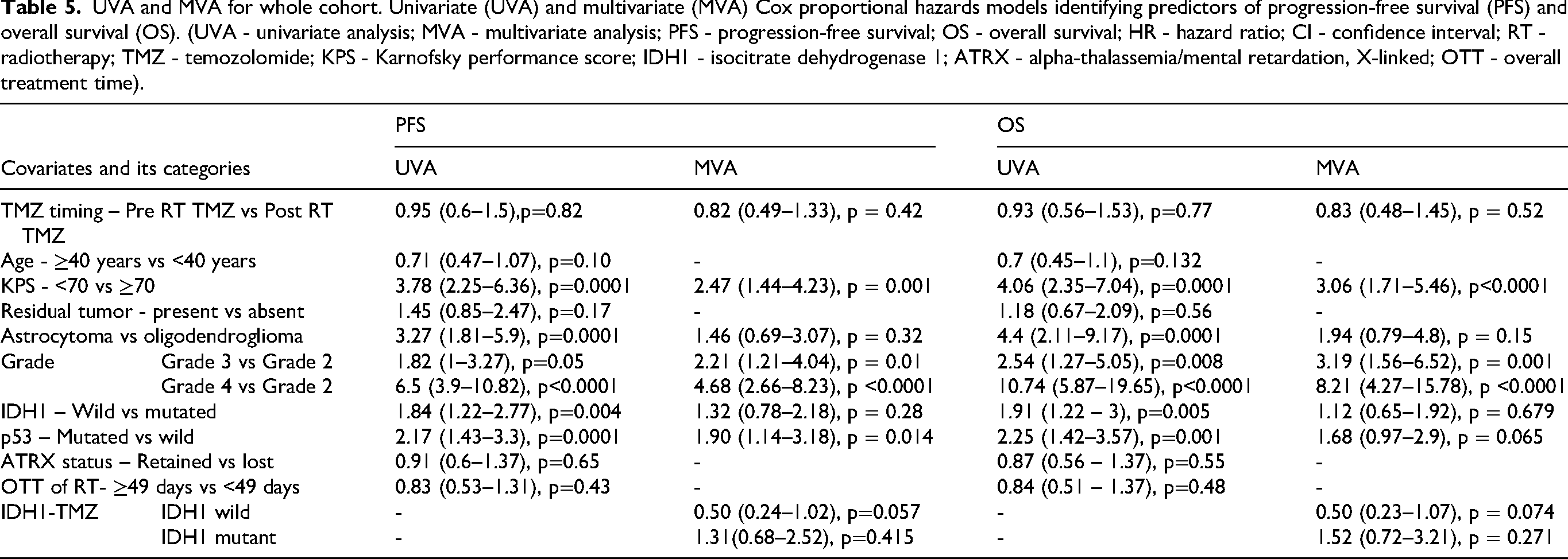
The Cox proportional hazards analysis identified significant predictors of PFS and OS, detailed in Table 5. A KPS < 70 increased hazards for both PFS (HR 3.78, 95% CI: 2.25–6.36, p < 0.001) and OS (HR 4.06, 95% CI: 2.35–7.04, p < 0.001). Astrocytoma histology heightened hazards for PFS (HR 3.27, 95% CI: 1.81–5.90, p < 0.001) and OS (HR 4.40, 95% CI: 2.11–9.17, p < 0.001) compared to oligodendroglioma. Grade 3 tumors had higher hazards than Grade 2 for PFS (HR 1.82, p = 0.050) and OS (HR 2.54, p = 0.008), while Grade 4 tumors showed higher hazards (PFS: HR 6.50, OS: HR 10.74, p < 0.001). IDH1 wild-type and mutant p53 predicted poorer PFS and OS outcomes (p < 0.005). In the multivariate analysis (Table 5), poor performance status (KPS < 70) and higher tumor grade (Grades 3 and 4) remained strong, independent predictors of significantly worse PFS and OS (p ≤ 0.01 for all). The p53 mutation affected PFS (aHR 1.90, p = 0.014) but violated the proportional hazards assumption (χ2 = 5.93, p = 0.015) as shown in Supplementary Table 2. We subsequently analyzed p53 as a time-varying covariate. The baseline mutation was initially associated with a borderline reduced hazard (HR 0.176, p = 0.050). However, the time-interaction effect demonstrated that the hazard significantly increased over time (HR 2.198, p = 0.005).
UVA and MVA for whole cohort. Univariate (UVA) and multivariate (MVA) Cox proportional hazards models identifying predictors of progression-free survival (PFS) and overall survival (OS). (UVA - univariate analysis; MVA - multivariate analysis; PFS - progression-free survival; OS - overall survival; HR - hazard ratio; CI - confidence interval; RT - radiotherapy; TMZ - temozolomide; KPS - Karnofsky performance score; IDH1 - isocitrate dehydrogenase 1; ATRX - alpha-thalassemia/mental retardation, X-linked; OTT - overall treatment time).
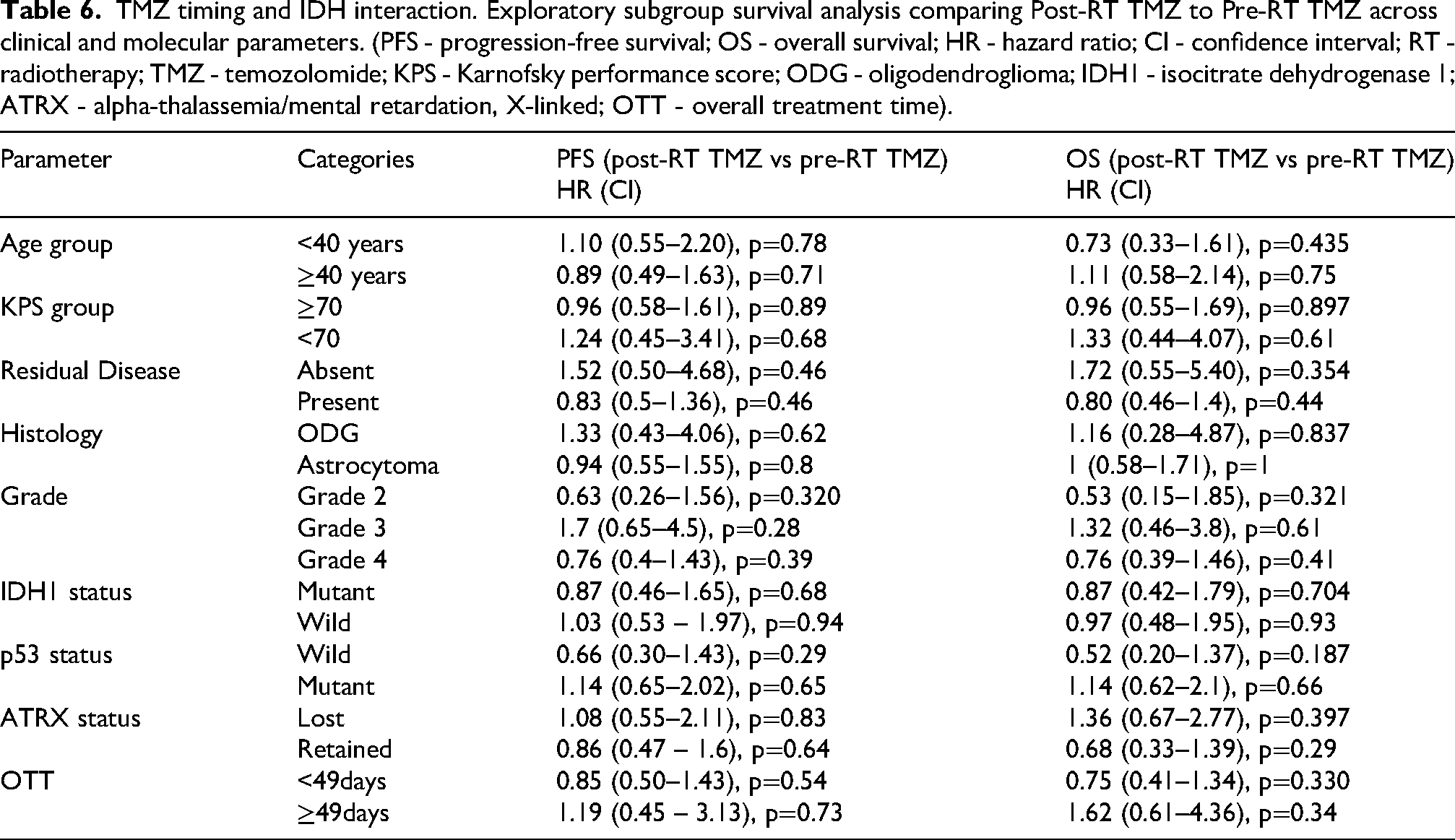
TMZ timing and IDH interaction. Exploratory subgroup survival analysis comparing Post-RT TMZ to Pre-RT TMZ across clinical and molecular parameters. (PFS - progression-free survival; OS - overall survival; HR - hazard ratio; CI - confidence interval; RT - radiotherapy; TMZ - temozolomide; KPS - Karnofsky performance score; ODG - oligodendroglioma; IDH1 - isocitrate dehydrogenase 1; ATRX - alpha-thalassemia/mental retardation, X-linked; OTT - overall treatment time).
Exploratory subgroup analysis by WHO tumor grade
To address the clinical and biological heterogeneity of the mixed-grade cohort, survival outcomes were explicitly stratified according to the WHO Tumor Grade. As anticipated, a higher tumor grade was a strong independent prognostic factor for poorer outcomes. Kaplan-Meier analysis demonstrated a significant stepwise decrease in both PFS and OS as the tumor grade increased (Figures 2(d) and 3(d)). In the multivariate Cox proportional hazards model, compared to grade 2 tumors, grade 3 tumors exhibited significantly elevated hazards for progression (aHR 2.21, p = 0.010) and mortality (aHR 3.19, p = 0.001) (Table 5). Grade 4 tumors demonstrated the highest risk, with an aHR of 4.68 for PFS (p < 0.001) and an aHR of 8.21 for OS (p < 0.001) (Table 5).
Interaction analysis and molecular subgroup trends
After evaluating the direct impact of the variables on survival, the Interaction Models determined whether the predictor effects varied across other predictors (Supplementary table 3). Although these analyses are constrained by the limited sample size of the adaptive pre-RT TMZ cohort (n = 39) and should be viewed as hypothesis-generating, no significant interactions were observed between TMZ timing and KPS, histology, grade, or p53 status. The IDH1 status model showed a significant interaction (LR χ2(8) = 79.39, p < 0.0001), with aHR of 0.38 (95% CI: 0.14–1.02, p = 0.055). For IDH1 mutant tumors, no significant PFS effect was observed between adaptive pre-RT TMZ and post-RT TMZ (aHR = 1.31, 95% CI: 0.68–2.52, p = 0.415). For IDH1 wild-type tumors, adaptive pre-RT TMZ showed a protective trend (aHR = 0.50, 95% CI: 0.24–1.02, p = 0.057). The OS interaction model was significant (LR χ2(3) = 7.99, p = 0.046), indicating that the impact of TMZ timing depended heavily on the tumor's IDH1 mutation status. In IDH1 mutant tumors, adaptive pre-RT TMZ showed no significant OS difference (aHR = 1.522, 95% CI: 0.721–3.213, p = 0.271). Conversely, in IDH1 wild-type tumors, adaptive pre-RT TMZ demonstrated a protective trend for overall survival, although it did not reach statistical significance (aHR = 0.500, 95% CI: 0.234–1.069, p = 0.074).
IDH1-timing interaction
To determine whether the timing of temozolomide administration had a differential impact based on tumor aggressiveness, an exploratory subgroup analysis was performed within each specific grade. Adaptive pre-RT TMZ did not show any statistically significant difference in survival compared to standard post-RT TMZ among the mixed-grade or any individual grade cohort. For Grade 2 gliomas, the hazard ratios comparing post-RT to adaptive pre-RT TMZ timing were 0.63 for PFS (p = 0.320) and 0.53 for OS (p = 0.321). Similarly, no significant survival differences based on TMZ sequencing were observed in the grade 3 (PFS HR 1.70, p = 0.28; OS HR 1.32, p = 0.61) or grade 4 (PFS HR 0.76, p = 0.39; OS HR 0.76, p = 0.41) subgroups (Table 6).
Discussion
The patient population in our study presented distinct characteristics compared to typical HGG cohorts, particularly those focusing on glioblastoma. Comprising a majority of patients under 40 years and approximately 41-45% with WHO Grade 2 gliomas, our demographic is more comparable to cohorts in studies of high-risk LGG, such as RTOG 0424 (median age, 49 years) 8 or mixed anaplastic glioma studies, such as RTOG BR0131. 9 Consequently, the superior median overall survival (OS) in our cohort (65–81 months) compared to standard GBM outcomes (median OS of 13.4–19 months) 10 is anticipated. This reflects the inclusion of established favorable prognostic factors, specifically younger age, low grade tumors, and a significant proportion (∼60%) of IDH-mutant cases. 11
Adaptive rationale and treatment delays
The standard management of HGG involves maximal safe surgical resection followed by RT, typically concurrent and adjuvant TMZ. 12 , 13 The interval between surgery and the initiation of RT is a period of clinical concern, during which residual tumor cells may proliferate. While surgery-to-RT delays are historically linked to poorer survival, logistical constraints in high-volume tertiary care settings often render these delays unavoidable.
In our cohort, these delays were primarily driven by systemic resource limitations and extended waitlists rather than postoperative clinical deterioration, as evidenced by the high KPS scores maintained across both groups leading up to RT. Consequently, adaptive pre-RT TMZ was strictly deployed as a pragmatic adaptive bridging strategy to provide continuous systemic disease control during the administrative waiting period. While some reports suggest that modest surgery-to-CRT delays (up to 12 weeks) may not adversely affect OS in GBM, 14 understanding whether chemotherapy during unavoidable delays can mitigate negative impacts or even improve outcomes remains unclear.
Clinical manageability of hematological toxicity
The rates of severe hematological toxicity observed in our cohort appear to be on the lower end compared to several literature reports, especially those involving exclusively HGG populations or more intensive adaptive pre-RT chemotherapy regimens. 9 This may be attributable to the mixed grade and younger patient demographics showing better chemotherapy tolerance. TMZ dosing in the adaptive pre-RT phase, described as “adjuvant TMZ” (standard 150–200 mg/m2 for 5 days), might be less intensive than formal neoadjuvant schedules. The clinical manageability of this adaptive strategy is underscored by a safety profile that compares favorably with the established standards.
Permanent discontinuation, specifically due to unmanageable toxicity, was exceptionally rare, aligning with the high adherence rates reported in the landmark Stupp trial. 13 Furthermore, the incidence of clinically significant dose reductions ≥50 mg/m2) was comparable between cohorts (12.8% pre-RT vs. 7.4% post-RT; p = 0.315), suggesting that early TMZ initiation does not compromise cumulative dose intensity, consistent with the findings of the RTOG 0525 trial. 15 Notably, after censoring planned radiotherapy interruptions to isolate true hematological recovery, severe toxicity-induced delays (>4 weeks) were absent in the adaptive pre-RT arm compared to 11.6% in the post-RT arm (p = 0.033). This significant improvement in recovery intervals relative to conventional adjuvant scheduling indicates that separating initial TMZ cycles from the lymphodepleting effects of concurrent chemoradiotherapy may optimize marrow resilience. 16 Consequently, the pre-RT window offers a safe therapeutic opportunity that maintains the standard dose intensity without compromising the timely delivery of definitive radiotherapy.
Survival outcomes and prognostic factors
Our study showed a numerical trend towards improved PFS and OS with adaptive pre-RT TMZ on Kaplan-Meier analysis. However, in the multivariate Cox proportional hazard analysis, after adjusting for prognostic covariates, TMZ timing did not emerge as an independent predictor of the outcome. The absence of statistical significance suggests that these differences may be due to chance, confounding factors, or other prognostic factors. Scientific conclusions from non-randomized studies should be based on adjusted analyses.
KPS <70 was a strong independent adverse prognostic factor, consistent with its established role across glioma grades.11 As expected, a higher WHO tumor grade (grade 3 and particularly grade 4 versus grade 2) was associated with significantly worse PFS and OS. Histology (astrocytoma vs. oligodendroglioma) showed a better prognosis for oligodendrogliomas in the univariate analysis, consistent with the literature,11 although this did not retain significance in the multivariate analysis, possibly due to the strong influence of tumor grade and molecular markers.
A notable divergence was that the IDH1 mutation status, while significant in the univariate analysis, was not an independent prognostic factor in the multivariate OS model. This was due to strong prognostic weight of tumor grade (HR for IDH1 changed from 1.91, p = 0.005 to 1.06, p = 0.826 when grade was added). This finding was interesting, as IDH status showed a significant interaction with TMZ timing. Mutated p53 has emerged as an independent adverse prognostic factor for PFS. This is plausible, as p53 positivity has been linked to lower survival in LGG, 17 and its role in HGG is complex. 18 The nuanced observation from our study that the p53 hazard increased over time suggests that its negative impact may escalate, which is a clinically relevant insight. Finally, ATRX status was not found to be a significant prognostic factor in the univariate analysis. This is somewhat unexpected when a substantial proportion of astrocytomas were IDH-mutant/ATRX-loss, as ATRX loss is characteristic of IDH-mutant astrocytomas and has prognostic implications. 11
Molecular subgroups and literature context
The impact of administering TMZ before standard RT appears to be highly dependent on the patient population, chemotherapy regimen, and the control arm definition. Our findings contrast with those of the NEOTEM trial in GBM, where neoadjuvant TMZ (three cycles) resulted in significantly worse outcomes than standard chemoradiotherapy (CRT).
19
This discrepancy likely arises from differences in patient populations (pure GBM vs. mixed-grade gliomas in our study), specific neoadjuvant regimens, and underlying molecular characteristics of the tumors. Conversely, the RTOG BR0131 study of pre-RT TMZ (up to six cycles) in anaplastic oligodendrogliomas and mixed oligoastrocytomas showed excellent outcomes, particularly for 1p/19q co-deleted tumors.
9
The inclusion of oligodendrogliomas (23–31%) and grade 3 tumors (20–21%) in our cohort might contribute to the better outcomes seen in our adaptive pre-RT arm, aligning somewhat with these positive findings for specific subgroups.
• IDH1 wild-type Insights: Interaction analysis between TMZ timing and IDH1 status yielded interesting findings. For IDH1 wild-type tumors, a protective trend for adaptive pre-RT TMZ was observed for PFS (aHR 0.50, p = 0.057) and OS (aHR 0.50, p = 0.074). This is counterintuitive, as IDH1 wild-type tumors are typically TMZ-resistant, especially those with unmethylated MGMT promoters, and sharply contrast with the NEOTEM trial. One hypothesis is that early cytotoxic pressure from TMZ in these rapidly proliferating tumors may curb proliferation while waiting for radiotherapy. However, our adaptive pre-RT TMZ group reflected an adaptive response to unavoidable logistical delays rather than a planned neoadjuvant delay. The definitive detriment observed in the unmethylated subgroup of the NEOTEM trial strongly underscores the critical necessity of incorporating MGMT promoter status into any clinical decision regarding early TMZ administration. The absence of molecular data in our cohort remains a significant limitation, reiterating the need for extreme caution in interpreting our IDH1 wild-type trends. • IDH Mutant Insights: Conversely, for IDH1-mutant tumors, our study suggested no significant benefit and possibly a non-significant detrimental trend (aHRs >1 for PFS/OS) with adaptive pre-RT TMZ administration. While IDH-mutant gliomas are generally recognized for their enhanced chemosensitivity,11,20 our findings align with those of the CATNON trial, where concurrent TMZ (an early form of TMZ administration) did not benefit patients with grade 3 anaplastic astrocytomas.11,21 Furthermore, the risk of TMZ-induced hypermutation, particularly in IDH-mutant gliomas with longer natural histories, must be considered when using early or extended TMZ schedules.
22
Although the statistical interaction between temozolomide timing and IDH1 status presents an intriguing hypothesis-generating signal, it is imperative to emphasize that the clinical application of these findings remains premature. These results cannot yet guide routine practice and require rigorous prospective validation.
Study limitations
In evaluating these findings, it is essential to acknowledge the inherent weaknesses of the retrospective data. In this cohort, allocation to the ‘adaptive pre-RT TMZ’ group was driven by real-world logistical delays rather than randomization. Consequently, unmeasured clinical, socioeconomic, or institutional variables, such as nuanced differences in postoperative recovery trajectories, exact tumor volume remnants, or variations in regional resource access, may have influenced both the radiotherapy delay and ultimate survival outcomes. While our multivariate Cox proportional hazards models were meticulously adjusted for known major prognostic factors (e.g., KPS, tumor grade, IDH1, and p53 status), statistical adjustment cannot fully eradicate the influence of unmeasured confounders.
The second significant limitation is the relatively small overall sample size (n = 134), particularly the limited number of patients in the adaptive pre-RT TMZ cohort (n = 39). This imbalance restricts the overall statistical power of the study, which inherently increases the risk of type II errors. This constraint is especially impactful for exploratory subgroup and interaction analyses, potentially masking true survival differences between treatment arms within specific molecular or histological subgroups (such as the IDH1 and grade-specific models).
Finally, a critical molecular limitation is the unavailability of MGMT (O(6)-methylguanine-DNA methyltransferase) promoter methylation data, the definitive predictive biomarker of temozolomide efficacy in gliomas. Without these data, it is impossible to determine whether the observed survival trends—particularly the counterintuitive protective trend in the IDH1 wild-type subgroup—are genuine therapeutic effects of adaptive TMZ timing or merely statistical artifacts caused by an unequal distribution of MGMT-methylated tumors between the cohorts. Because retrospective associations cannot substitute for prospective causality, this omission significantly weakens the interpretability of the findings. Therefore, these findings must be viewed strictly as hypothesis-generating and interpreted with caution.
Conclusion
Our exploratory study on adaptive TMZ timing in a mixed-grade glioma cohort showed no significant independent survival advantage for adaptive pre-RT TMZ in the multivariate analysis. While subgroup analyses revealed potential protective trends associated with early TMZ in IDH1 wild-type gliomas, these findings must be validated prospectively, considering the MGMT promoter status. These results underscore the need for randomized trials to precisely define the role and molecular stratification of adaptive pre-RT TMZ in managing unavoidable RT delays.
Supplemental Material
sj-docx-1-opp-10.1177_10781552261451881 - Supplemental material for Timing of temozolomide in adult glioma: An exploratory study of an adaptive pre-radiotherapy approach in a mixed-grade cohort
Supplemental material, sj-docx-1-opp-10.1177_10781552261451881 for Timing of temozolomide in adult glioma: An exploratory study of an adaptive pre-radiotherapy approach in a mixed-grade cohort by Kunhi Parambath Haresh, Arun Thimmarayappa, Swarnaditya Roy and Subhash Gupta in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-docx-2-opp-10.1177_10781552261451881 - Supplemental material for Timing of temozolomide in adult glioma: An exploratory study of an adaptive pre-radiotherapy approach in a mixed-grade cohort
Supplemental material, sj-docx-2-opp-10.1177_10781552261451881 for Timing of temozolomide in adult glioma: An exploratory study of an adaptive pre-radiotherapy approach in a mixed-grade cohort by Kunhi Parambath Haresh, Arun Thimmarayappa, Swarnaditya Roy and Subhash Gupta in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-docx-3-opp-10.1177_10781552261451881 - Supplemental material for Timing of temozolomide in adult glioma: An exploratory study of an adaptive pre-radiotherapy approach in a mixed-grade cohort
Supplemental material, sj-docx-3-opp-10.1177_10781552261451881 for Timing of temozolomide in adult glioma: An exploratory study of an adaptive pre-radiotherapy approach in a mixed-grade cohort by Kunhi Parambath Haresh, Arun Thimmarayappa, Swarnaditya Roy and Subhash Gupta in Journal of Oncology Pharmacy Practice
Footnotes
Ethical considerations
The study was approved by the institutional ethics committee of the All India Institute of Medical Sciences, New Delhi, on 11 November 2020 (Approval number: IEC-1023/03.10.20, RP-13/2020).
Consent to participate
The requirement for informed consent was waived by the institutional ethics committee due to the retrospective nature of the study and the use of anonymized data from medical records.
CRediT (contributor roles taxonomy) author statement
SG: Conceptualization, Methodology, Investigation, Writing – original draft, Writing – review & editing, Supervision. AT: Conceptualization, Methodology, Investigation, Formal analysis, Writing – original draft, Writing – review & editing. KPH: Conceptualization, Methodology, Investigation, Writing – original draft, Writing – review & editing. SR: Methodology, Investigation, Formal analysis, Writing – original draft, Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author, Subhash Gupta, upon reasonable request after data-anonymization.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.