
Abstract
Introduction
Azacitidine-venetoclax has improved outcomes in older or intensive chemotherapy-ineligible acute myeloid leukemia (AML) patients. However, real-world experience and pharmacoeconomic evidence remain scarce in resource-limited settings, particularly in North Africa, where drug pricing and supportive care constraints significantly shape clinical practice.
Methods
A retrospective single-center study was conducted at a tertiary military teaching hospital in Morocco (December 2019–December 2025). Fifteen older or unfit AML patients receiving azacitidine-based regimens were included. Venetoclax was dose-reduced to 100 mg/day under concomitant voriconazole prophylaxis based on CYP3A4 inhibition principles. Kaplan-Meier survival analysis was performed. An exploratory pharmacoeconomic analysis was conducted from a hospital perspective, incorporating drug acquisition costs, infection-related hospitalization expenses, and quality-adjusted life-years (QALYs) derived from the literature.
Results
Complete remission was achieved in 78% of first-line azacitidine-venetoclax recipients (n = 9) and 50% with azacitidine alone (n = 4). Infectious complications occurred in 73.3% of patients. Median overall survival was not reached; estimated survival probabilities were 76% at 12 months and 57% at 24 months. The incremental cost-effectiveness ratio (ICER) of azacitidine-venetoclax versus azacitidine alone was approximately 183,000 MAD per QALY gained (≈2× Morocco's GDP per capita) after incorporating infection-related costs. Venetoclax acquisition price was the primary cost-effectiveness driver on sensitivity analysis.
Conclusions
Pharmacology-guided azacitidine-venetoclax regimens are clinically feasible in resource-limited settings, with encouraging survival outcomes. Infection management, antifungal prophylaxis strategies, and targeted drug pricing negotiations are key determinants of cost-effectiveness. Prospective multicenter studies are warranted.
Keywords
Introduction
Acute myeloid leukemia (AML) is a malignant hematologic disorder characterized by clonal proliferation of myeloid blasts leading to bone marrow failure, with hemorrhagic and infectious complications. 1 In older patients, AML is frequently associated with comorbidities, reduced tolerance to intensive chemotherapy (IC), and adverse biological features, making therapeutic decision-making challenging. 2 At tertiary care centers in Morocco, management is adapted to patient characteristics and local resources, with a substantial role for lower-intensity approaches when IC is not feasible. 3
Azacitidine plus venetoclax (Aza-Ven) has demonstrated survival benefits in pivotal trials, 1 but venetoclax exposure is markedly increased by strong CYP3A inhibitors, requiring substantial dose reductions to mitigate toxicity.4,5 Strong CYP3A inhibitors such as posaconazole and voriconazole necessitate at least a 75% reduction of the venetoclax maintenance dose from 400 mg to 100 mg daily to avoid excessive drug exposure and associated toxicity.4,5 In the Moroccan context, access to comprehensive cytogenetic and molecular profiling remains heterogeneous, and budgetary constraints at hospital level require careful consideration of both clinical effectiveness and economic feasibility when implementing innovative therapies.
We aimed to describe the real-world implementation of a pharmacology-guided, dose-reduced venetoclax regimen with azacitidine using voriconazole prophylaxis in older or intensive chemotherapy-ineligible AML patients treated at a Moroccan tertiary center between December 2019 and December 2025, to report clinical outcomes including overall survival, and to provide exploratory hospital-perspective cost-effectiveness estimates with explicit modeling of infection-related resource use.
Methods
Study design, setting, and period
This was a single-center retrospective descriptive study conducted in the Clinical Hematology Department of a tertiary military teaching hospital in Morocco, from December 2019 to December 2025.
Study population
We included AML patients diagnosed according to WHO 2022 criteria,6,7 aged ≥65 years and/or deemed ineligible for intensive chemotherapy by the treating hematologist, with exploitable medical records. Ineligibility for IC was determined by physician assessment based on frailty, comorbidities (cardiac, renal, hepatic dysfunction), poor performance status (ECOG ≥2), or anticipated intolerance to anthracycline-based induction. We excluded patients who were eligible for IC, patients with acute leukemia other than AML, and incomplete or non-exploitable medical records.
Baseline assessment and collected variables
Baseline evaluation included history and physical examination, complete blood count, bone marrow aspirate, immunophenotyping, cytogenetic and molecular testing when available. Routine biochemistry, coagulation tests, blood group/phenotyping, viral serologies (HBV/HCV/HIV), imaging, and cardiac assessment (ECG, echocardiography with LVEF) were collected as per departmental practice. Because molecular testing was not systematically available, proportions for molecular variables are reported only among patients with documented results.
Treatment approach (departmental practice)
For patients eligible for IC, the reference induction regimen was 7 + 3 (cytarabine for 7 days plus an anthracycline for 3 days). 8 In older or comorbid patients ineligible for IC, a lower-intensity strategy was favored using azacitidine alone or Aza-Ven, depending on drug access and clinical feasibility.
In the Aza-Ven regimen used at this center, azacitidine was administered at the standard dose of 75 mg/m2/day for 7 days. Venetoclax was escalated (100 mg day 1, 200 mg day 2, 300 mg day 3) and then administered at 100 mg/day with concomitant voriconazole 200 mg twice daily for 28 days in cycle 1, with subsequent cycles adapted (21 to 7 days of venetoclax based on AML profile, response and tolerability).9,10 This practice is consistent with the pharmacologic principle that strong CYP3A inhibitors warrant at least a 75% venetoclax dose reduction after ramp-up; at steady dosing the 100 mg daily maintenance dose represents a 75% reduction from the commonly used 400 mg daily target dose in the absence of strong inhibitors.4,5 The local rationale for using voriconazole was dual: primary antifungal prophylaxis and pharmacology-guided venetoclax dose reduction to reduce costs while maintaining expected therapeutic effectiveness based on pharmacokinetic principles.
Outcomes and definitions
Clinical complications were collected and categorized as infectious, metabolic, and digestive events as reported in the medical records. Clinical outcomes included complete remission (CR), early death (death during induction before response assessment), early relapse (<12 months from documented CR), failure (no response after first cycle), and status at last follow-up as recorded. Response assessment was performed after the first treatment cycle using bone marrow aspiration between days 28 and 42, in addition to peripheral blood count assessment. Given the retrospective nature of the study, outcome definitions reflect chart documentation; CR as reported may not strictly distinguish between morphologic CR and CR with incomplete count recovery (CRi). Future analyses should explicitly standardize response criteria (e.g., ELN 2022 definitions) and time-to-event endpoints.
Data handling and statistical analysis
Data were extracted using a standardized collection form and analyzed descriptively using Microsoft Excel, with means, medians, ranges, and frequencies as appropriate. All data were anonymized, and no nominative identifiers were included in the analysis dataset. Missing data were handled using a complete-case approach. Variables with missing information were not imputed and were excluded from specific analyses when unavailable. The number of patients included in each analysis is specified where applicable.
Overall survival was analyzed using the Kaplan-Meier method, with survival time defined as the interval between treatment initiation and death from any cause or last follow-up (censored observation). Median survival and 95% confidence intervals were estimated using the Kaplan-Meier estimator. Survival probabilities at 12 and 24 months were calculated from the survival function. Survival analyses were performed using R statistical software version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria). 11
Exploratory pharmacoeconomic analysis
We conducted an exploratory cost and cost-effectiveness analysis from the hospital perspective comparing azacitidine alone versus azacitidine plus venetoclax in older or intensive chemotherapy-ineligible AML patients.12,13 Costs were expressed in Moroccan dirhams (MAD) using 2024–2025 values and were discounted at 3% annually. The time horizon of the base-case model corresponded to six treatment cycles, with extrapolation of survival beyond this period based on the observed distribution of clinical outcomes (remission, relapse, failure, death) in the cohort.
This assumption reflects local hospital practice and may not be generalizable to centers where same-patient next-day use of reconstituted azacitidine is not operationally feasible.
Scenario analysis: full-dose versus pharmacology-guided venetoclax dosing with azole prophylaxis
To explore the economic implications of our pharmacology-guided dosing strategy, we conducted a scenario analysis comparing two alternative implementations of azacitidine–venetoclax over six cycles. Scenario A represented a hypothetical full-dose regimen without strong CYP3A inhibition, with venetoclax given at 400 mg/day for 28 days per cycle and no systematic voriconazole prophylaxis. Scenario B represented our local practice, combining azacitidine with venetoclax dose reduction under azole prophylaxis, modeled as the departmental regimen (3100 mg total in cycle 1 followed by 21 days of 100 mg/day in cycles 2–6) plus oral voriconazole 200 mg twice daily for 28 days per cycle.
Using publicly available PPV data from the AMMPS national database, venetoclax at full dose (Scenario A: 400 mg/day × 28 days × 6 cycles = 672 tablets of 100 mg) would cost approximately 376,368 MAD over six cycles, versus approximately 76,170 MAD with pharmacology-guided dose reduction (Scenario B: 136 tablets of 100 mg over six cycles). This represents a venetoclax acquisition saving of approximately 300,000 MAD, which substantially exceeds the additional voriconazole prophylaxis cost of approximately 23,251 MAD over the same period. The net drug acquisition saving of pharmacology-guided Scenario B versus full-dose Scenario A is therefore approximately 277,000 MAD over six cycles — a greater than 50% reduction in total venetoclax-related expenditure. These findings confirm that pharmacology-guided venetoclax dose reduction under azole prophylaxis represents a strongly cost-advantaged strategy in the Moroccan context, provided clinical and pharmacokinetic assumptions underlying the dose adjustment are met.
In a context where both venetoclax and azole antifungals are relatively costly, the net budget impact of choosing a reduced-dose venetoclax plus voriconazole strategy versus a full-dose venetoclax regimen without azole prophylaxis therefore depends critically on their relative prices, reinforcing the need for coordinated price negotiations for both agents.
Primary antifungal prophylaxis cost-effectiveness
In addition to the comparison between azacitidine alone and azacitidine–venetoclax, we explored the potential economic impact of systematic primary antifungal prophylaxis within the azacitidine–venetoclax strategy. In our departmental protocol, oral azole prophylaxis is already implemented (voriconazole 200 mg twice daily for 28 days per cycle), and was therefore included in the base-case costs. Using our assumptions, this prophylaxis represents an additional drug cost of approximately 23,000 MAD per patient over six cycles, whereas each infectious episode in the azacitidine–venetoclax group was costed at 18,900 MAD (7 days of hospitalization and intensive intravenous antibiotics). Under these parameters, primary prophylaxis would need to avert more than one severe infectious episode per patient to become cost-saving purely from a hospital-cost perspective, which is not compatible with the observed mean infection rate of 1.1 episodes per patient in our cohort. These exploratory estimates suggest that, under the current cost assumptions and the modeled infection rates, primary antifungal prophylaxis would need to avert more than one severe infectious episode per patient to become cost-saving from a hospital-budget perspective alone. However, this purely cost-driven inference must be interpreted with extreme caution given the very limited sample size (n = 15) and the fact that the only early infection-related death in this cohort occurred in the azacitidine–venetoclax group, highlighting the life-threatening consequences of invasive fungal disease in this population. Accordingly, the decision to implement primary antifungal prophylaxis should be guided primarily by clinical considerations — notably the prevention of invasive fungal infections and associated mortality — rather than by hospital cost estimates derived from a small retrospective series. Any net impact on QALYs and overall cost-effectiveness warrants evaluation in larger, prospective datasets.
Ethical approval
This retrospective analysis used routinely collected clinical data. All data were anonymized prior to analysis and no nominative identifiers were extracted. According to institutional policy for retrospective observational studies using anonymized data, formal ethics committee approval was not required. The study complied with the ethical principles of the Declaration of Helsinki and applicable local regulations.
Results
Baseline demographic and clinical characteristics
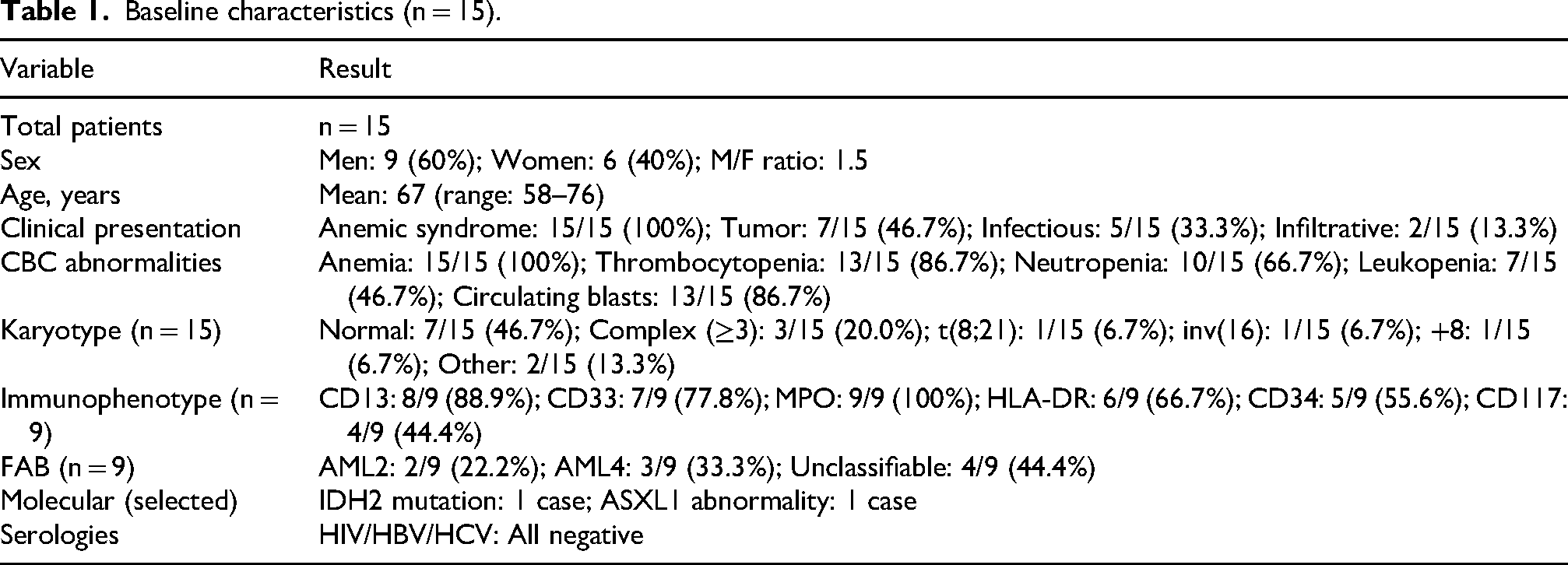
Fifteen older or unfit AML patients were managed between December 2019 and December 2025, including 9 men (60%) and 6 women (40%), with a mean age of 67 years (range 58–76). The most frequent clinical presentation was an anemic syndrome (100%), followed by tumor syndrome (7/15, 46.7%), infectious syndrome (5/15, 33.3%), and infiltrative manifestations (2/15, 13.3%). On complete blood count, anemia was present in all patients (15/15, 100%), with frequent thrombocytopenia (13/15, 86.7%), neutropenia (10/15, 66.7%), leukopenia (7/15, 46.7%), and circulating blasts (13/15, 86.7%) as reported in the files. Reported comorbidities and medical history included diabetes, smoking, heart disease, prior myelodysplastic syndrome, myeloproliferative neoplasms, solid cancer, and others with interindividual heterogeneity.
Hematologic and biological features
Bone marrow morphology classification (FAB) included AML2 (2/9, 22.2%), AML4 (3/9, 33.3%), and unclassifiable cases (4/9, 44.4%) as documented among patients with available FAB classification (n = 9). Immunophenotyping confirmed myeloid lineage in all tested patients (n = 9), with frequent expression of CD13 (8/9, 88.9%), CD33 (7/9, 77.8%), and MPO (9/9, 100%), and variable expression of HLA-DR (6/9, 66.7%), CD34 (5/9, 55.6%), and CD117 (4/9, 44.4%). Cytogenetics were available for all 15 patients and were normal in 7/15 (46.7%) of cases. Among the abnormal karyotypes, complex karyotype (≥3 abnormalities) was the most frequent (3/15, 20.0%), followed by other diverse abnormalities in 2/15 (13.3%). Specific recurrent abnormalities included t(8;21) in 1/15 (6.7%), inv(16) in 1/15 (6.7%), and isolated trisomy 8 (+8) in 1/15 (6.7%). Molecular testing was heterogeneous and incomplete; one IDH2 mutation (PCR) and one ASXL1 abnormality (NGS) were reported, while several tested patients had no detected abnormality. Systematic HIV/HBV/HCV serologies were negative in the series. Baseline characteristics are summarized in Table 1.
Baseline characteristics (n = 15).
Treatment, complications, and outcomes
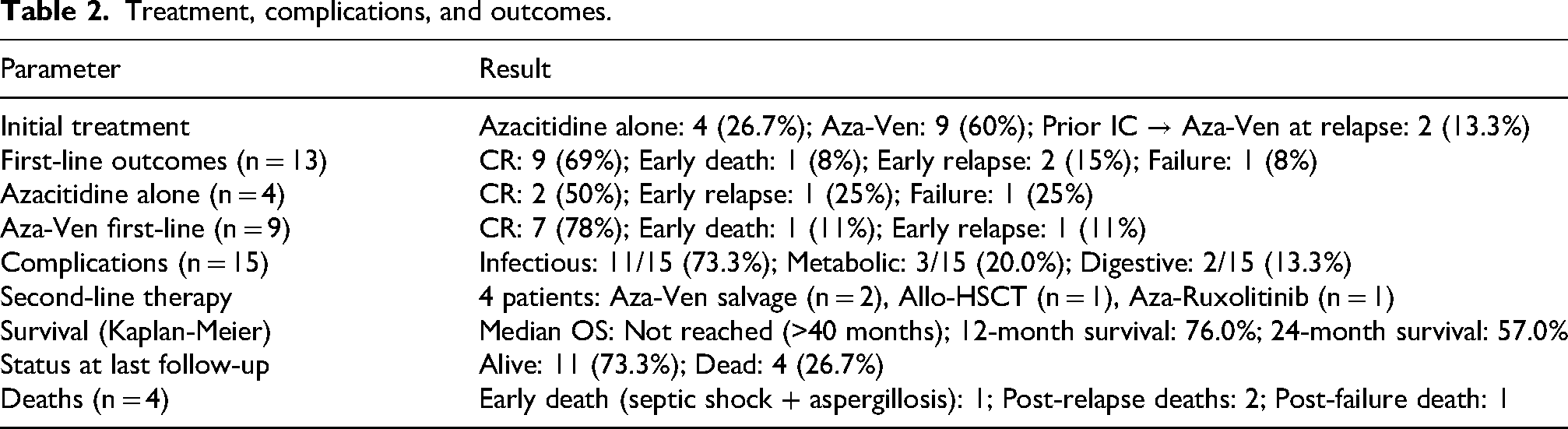
Initial treatment consisted of azacitidine alone in 4 patients (26.7%) and azacitidine-venetoclax in 9 patients (60%), while two patients (13.3%) had previously received intensive 7 + 3 induction elsewhere and were later managed at relapse with azacitidine-venetoclax.
Of note, the only early infection-related death (septic shock with invasive aspergillosis) occurred in the azacitidine–venetoclax subgroup (1/9 first-line patients, 11%), underscoring the importance of antifungal prophylaxis and vigilant supportive care in this setting.
Survival analysis
Kaplan-Meier survival analysis was performed for the entire cohort (n = 15). The median overall survival was not reached, with more than 50% of patients alive beyond 40 months of follow-up. At 12 months, the estimated survival probability was 76.0%, and at 24 months, the estimated survival probability was 57.0%. The Kaplan-Meier curve is shown in Figure 1.
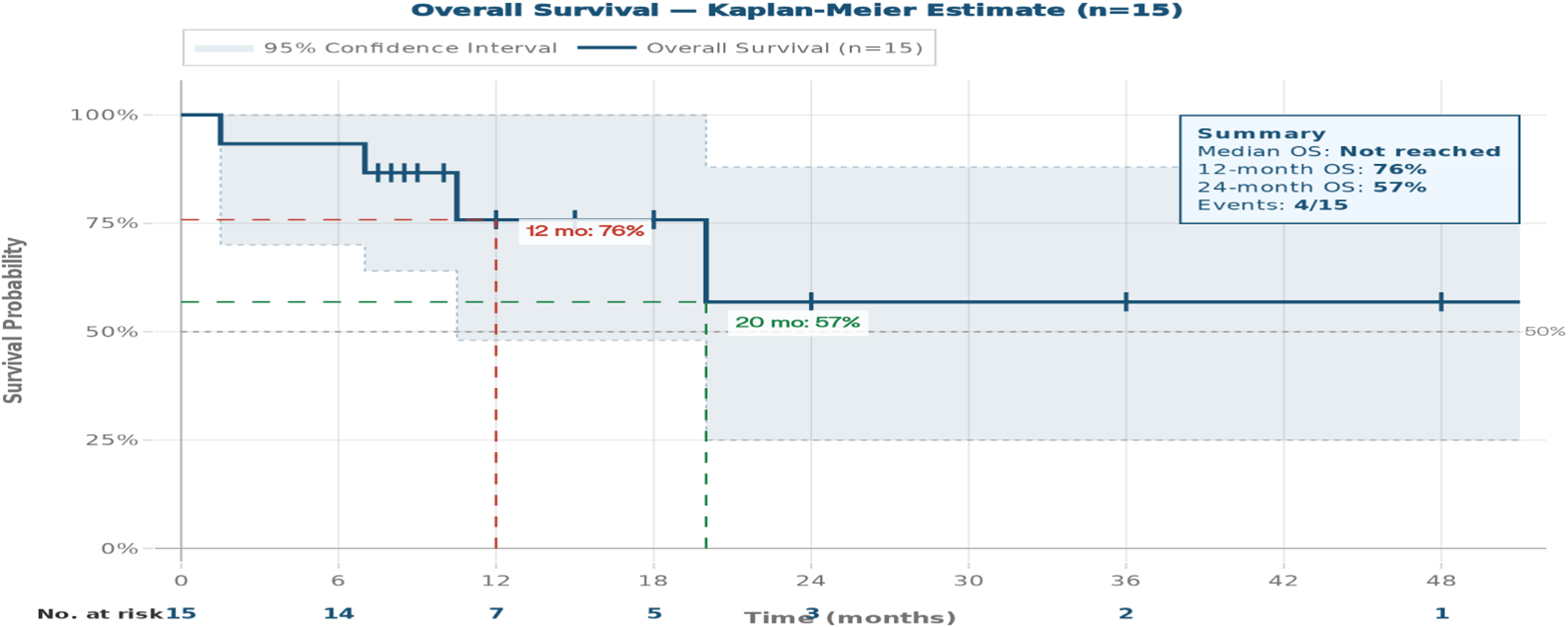
Kaplan-Meier overall survival curve for the entire cohort (n = 15). The Kaplan-Meier curve shows overall survival for all 15 patients treated with azacitidine-based regimens (azacitidine alone or azacitidine-venetoclax) between December 2019 and December 2025. The median overall survival was not reached, with more than 50% of patients alive beyond 40 months of follow-up. The estimated survival probabilities were 76.0% at 12 months and 57.0% at 24 months. Censored observations (patients alive at last follow-up) are indicated by vertical tick marks. The shaded area represents the 95% confidence interval.
Status at last follow-up: At last follow-up, 11 patients (73.3%) were alive and 4 (26.7%) had died. The four deaths included one early death from septic shock with invasive aspergillosis during first-line induction in the azacitidine–venetoclax subgroup, two deaths after early relapse despite second-line therapy (one post-transplant), and one death after primary failure and subsequent treatment. Treatment outcomes are summarized in Table 2
Treatment, complications, and outcomes.
Exploratory pharmacoeconomic results
Using publicly available Moroccan prices as proxies and modeling six treatment cycles under the assumptions described above, the initial base-case analysis without explicit breakdown of infection-related costs estimated the mean total direct medical cost per patient at approximately 112,626 MAD for azacitidine alone and 212,206 MAD for azacitidine-venetoclax. Corresponding mean QALYs were 0.9 and 1.5, respectively, yielding an incremental cost of 99,580 MAD and an ICER of approximately 165,966 MAD per QALY gained for azacitidine-venetoclax versus azacitidine alone.
When infection-related costs (hospitalization days and intravenous antibiotic therapy for infectious complications) were explicitly incorporated, the mean infection-related cost per patient was estimated at 10,500 MAD for azacitidine alone and 20,790 MAD for azacitidine-venetoclax. Adding these costs to the previously modeled drug and other direct medical costs increased the total mean cost per patient to 123,126 MAD for azacitidine alone and 232,996 MAD for azacitidine-venetoclax. This resulted in a revised incremental cost of 109,870 MAD, while the incremental QALY gain remained at 0.6, yielding an updated ICER of approximately 183,000 MAD per QALY gained. Compared with the initial base-case ICER (approximately 165,966 MAD/QALY), this refined estimate suggests that explicitly accounting for infectious complications modestly worsens the cost-effectiveness profile of the azacitidine-venetoclax strategy, reflecting the higher burden of infection-related resource use in this group. Results are summarized in Table 3.
Exploratory cost-effectiveness results with explicit infection-related costs.
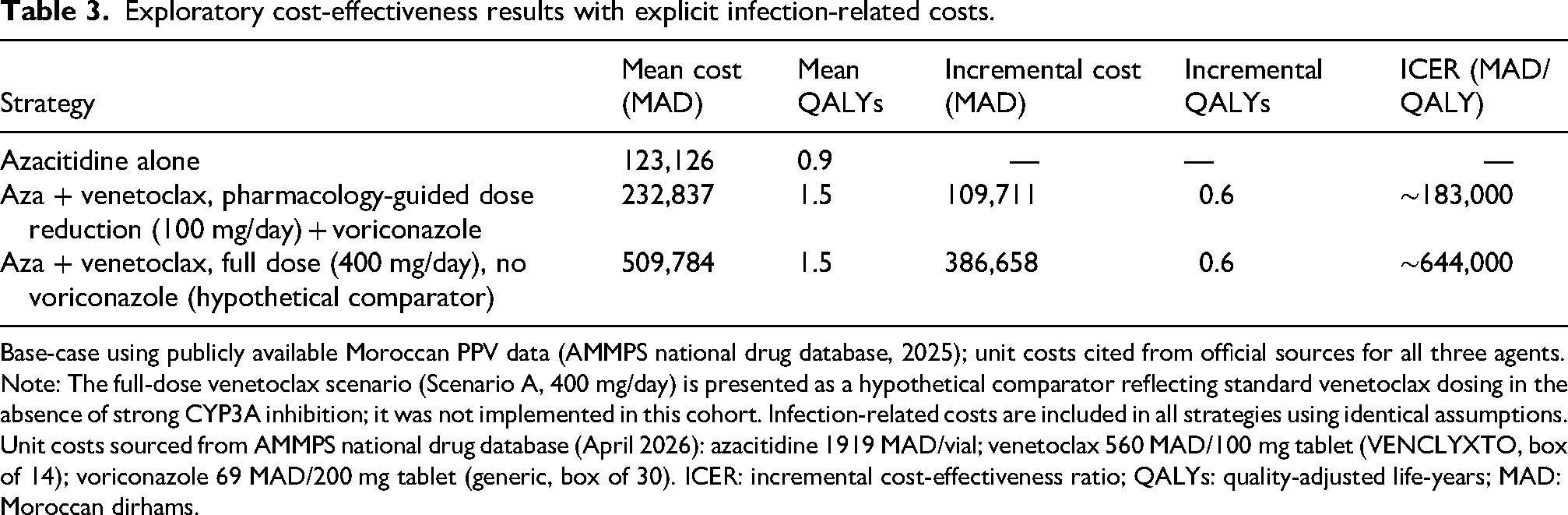
Base-case using publicly available Moroccan PPV data (AMMPS national drug database, 2025); unit costs cited from official sources for all three agents.
Note: The full-dose venetoclax scenario (Scenario A, 400 mg/day) is presented as a hypothetical comparator reflecting standard venetoclax dosing in the absence of strong CYP3A inhibition; it was not implemented in this cohort. Infection-related costs are included in all strategies using identical assumptions. Unit costs sourced from AMMPS national drug database (April 2026): azacitidine 1919 MAD/vial; venetoclax 560 MAD/100 mg tablet (VENCLYXTO, box of 14); voriconazole 69 MAD/200 mg tablet (generic, box of 30). ICER: incremental cost-effectiveness ratio; QALYs: quality-adjusted life-years; MAD: Moroccan dirhams.
To further contextualize the economic benefit of pharmacology-guided dose reduction, a hypothetical full-dose venetoclax scenario (400 mg/day without azole prophylaxis) was added as a third comparator in Table 3, using the same PPV-based unit costs. At full dose, the estimated total cost per patient over six cycles would reach 509,784 MAD, yielding an ICER of approximately 644,000 MAD/QALY — more than seven times Morocco's GDP per capita — compared with ∼183,000 MAD/QALY for the pharmacology-guided dose-reduced strategy.
Discussion
This single-center real-world series describes predominantly marrow failure at presentation (including universal anemia and frequent thrombocytopenia) and a high burden of infectious morbidity among older or IC-ineligible AML patients. Lower-intensity approaches predominated (azacitidine alone in 26.7% and azacitidine-venetoclax in 60%), reflecting tolerance constraints, comorbidities, and drug availability in the Moroccan setting.
Pharmacology-Guided venetoclax dosing
Our departmental regimen relied on pharmacology-guided venetoclax dose reduction under voriconazole prophylaxis. This approach aligns with the general recommendation to reduce venetoclax by at least 75% when strong CYP3A inhibitors are necessary, to mitigate excessive exposure and toxicity risk.4,5 The 100 mg daily maintenance dose used in our protocol represents this 75% reduction from the standard 400 mg dose used without inhibitors. This strategy served a dual purpose: antifungal prophylaxis in a high-risk population and cost reduction while maintaining expected therapeutic effectiveness based on pharmacokinetic principles.
The scenario analysis comparing full-dose venetoclax (400 mg/day without voriconazole, Scenario A) versus our dose-reduced regimen with azole prophylaxis (Scenario B) highlighted that the pharmacology-guided strategy substantially reduced venetoclax milligram use (approximately 4.9-fold reduction over six cycles) but added approximately 23,000 MAD in voriconazole acquisition costs. The net budget impact therefore depends critically on the relative prices of venetoclax and azole antifungals. Our findings reinforce that, to fully leverage the economic benefit of venetoclax dose reduction strategies under strong CYP3A inhibition, pricing policies must address both the targeted agent and the mandatory antifungal prophylaxis through coordinated price negotiations or patient access schemes.
Furthermore, our analysis of primary antifungal prophylaxis within the azacitidine–venetoclax strategy indicated that, under current cost assumptions, prophylaxis would need to prevent more than one severe infectious episode per patient to become cost-saving from a hospital perspective. Given the observed infection rate of 1.1 episodes per patient in our cohort, primary prophylaxis is unlikely to reduce total hospital costs and should instead be justified primarily on clinical grounds—namely, prevention of life-threatening fungal disease and associated mortality—with potential QALY gains requiring evaluation in larger prospective cohorts.
Clinical outcomes and survival
Despite encouraging remission reporting (69% CR rate among first-line patients, 78% in the azacitidine-venetoclax subgroup), infectious complications were frequent (73.3%), emphasizing that supportive care and anti-infective prevention pathways are central to safely delivering venetoclax-based regimens in this population. The single early death (8% of first-line patients) was associated with septic shock and invasive aspergillosis, highlighting the vulnerability of this patient population.
The observed CR rate of 78% with Aza-Ven in our first-line subgroup is numerically higher than the CR rate reported in the pivotal VIALE-A trial (36.7%), and appears consistent with some real-world series that have described higher response rates in routine practice.1,17,18 However, this apparent difference must be interpreted with extreme caution given our very small sample size (n = 9 in the first-line azacitidine-venetoclax group), retrospective single-center design, potential differences in baseline risk profiles, and lack of standardized ELN response criteria and time-to-event endpoints. Similarly, the 50% CR rate observed with azacitidine alone in our limited sample (n = 4) is higher than the 17.9% reported in VIALE-A, but the small denominator in our cohort precludes any robust comparative conclusion and should be viewed as purely descriptive.
Kaplan-Meier survival analysis of the entire cohort showed that median overall survival was not reached, with more than 50% of patients alive beyond 40 months of follow-up, and estimated survival probabilities of 76.0% at 12 months and 57.0% at 24 months. While the VIALE-A trial reported a median OS of 14.7 months for the azacitidine-venetoclax arm versus 9.6 months for azacitidine alone, 1 direct comparison with our mixed cohort (including both azacitidine alone and azacitidine-venetoclax patients, as well as salvage cases) is not appropriate given the small sample size, heterogeneous treatment groups, and retrospective design. Nevertheless, the proportion of patients alive at last follow-up (73.3%) and the observed survival curve suggest that pharmacology-guided dose-reduced venetoclax regimens can achieve clinically meaningful survival outcomes in routine practice, although prospective studies with larger cohorts and standardized follow-up are needed to confirm these findings.
Cost-Effectiveness considerations
From an exploratory hospital-perspective pharmacoeconomic standpoint, azacitidine-venetoclax was associated with higher estimated direct medical costs and higher estimated QALYs compared with azacitidine alone. In the initial base-case analysis using drug and other direct medical costs but without explicit breakdown of infection-related resource use, the ICER was approximately 165,966 MAD per QALY gained. When hospital days and intravenous antibiotic therapy for infectious complications were explicitly incorporated, the total mean cost per patient increased to 123,126 MAD with azacitidine alone and 232,996 MAD with azacitidine-venetoclax, resulting in a revised incremental cost of 109,870 MAD and an updated ICER of around 183,000 MAD per QALY gained. This value corresponds to roughly 1.5–2.0 times Morocco's 2024 GDP per capita (approximately 90,000 MAD), and can be viewed against historically proposed willingness-to-pay benchmarks of 1–3× GDP per capita for middle-income countries, while recognizing that these thresholds are increasingly debated and should be interpreted as flexible reference points rather than rigid decision rules. 19
The refined analysis highlights that, beyond drug acquisition prices, infection-related resource use is a non-trivial driver of overall costs, particularly in this frail elderly AML population receiving venetoclax-based regimens. Because medication costs were approximated using public PPV/list prices rather than confidential hospital acquisition costs, utilities were derived from international literature rather than local preference data, and infection-related resource use was modeled using average assumptions instead of detailed patient-level micro-costing, the resulting ICERs should be interpreted as exploratory and hypothesis-generating for Moroccan decision-makers rather than definitive reimbursement evidence.
The addition of the full-dose venetoclax comparator to Table 3 further underscores the economic rationale for pharmacology-guided dose reduction. At full dose (400 mg/day without azole prophylaxis), the estimated ICER would reach approximately 644,000 MAD/QALY — more than seven times Morocco's GDP per capita — rendering this approach economically untenable by any standard willingness-to-pay threshold applicable in Morocco. By contrast, the pharmacology-guided dose-reduced strategy with voriconazole achieves an ICER of approximately 183,000 MAD/QALY (−2× GDP per capita) at a net drug acquisition saving of approximately 277,000 MAD over six cycles. This demonstrates that the economic benefit of pharmacology-guided dosing is not marginal but transformative in a resource-limited setting, and reinforces the need for coordinated price negotiations for both venetoclax and azole antifungals.
Nevertheless, the sensitivity of the ICER to venetoclax price and to infection-related costs suggests that targeted price negotiations, patient access schemes, and optimized supportive care and antimicrobial stewardship could meaningfully improve the value-for-money profile of azacitidine-venetoclax in routine practice.
Limitations
This study has several important limitations. Its retrospective, single-center design and small sample size (n = 15) limit statistical power and preclude robust comparative inference between treatment strategies. Incomplete molecular profiling constrained formal ELN risk stratification, and the variable follow-up duration limits the precision of survival estimates. The exploratory pharmacoeconomic analysis relies on several assumptions: drug costs were approximated using public list prices rather than actual hospital acquisition costs; azacitidine cycle costing also reflected a local reconstitution workflow designed to minimize vial wastage, which may not be replicable across all centers; health-state utilities were derived from international literature, and infection-related resource use was modeled using average assumptions rather than patient-level micro-costing. Accordingly, the resulting ICERs should be interpreted as illustrative and hypothesis-generating rather than definitive. These findings should therefore be viewed strictly as descriptive, supporting the need for larger prospective multicenter studies with standardized response criteria, explicit time-to-event endpoints, and detailed local cost data.
Clinical and policy implications
These findings reinforce the need for several concrete actions at clinical and policy levels:
Conclusions
In this Moroccan cohort of 15 older or intensive chemotherapy-ineligible AML patients, pharmacology-guided venetoclax dosing (100 mg daily with concomitant voriconazole) plus azacitidine was frequently used and associated with encouraging complete remission rates (78% in the first-line azacitidine-venetoclax subgroup) and prolonged survival (median not reached at 40 months; 76% alive at 12 months, 57% at 24 months), albeit at the cost of a high burden of infectious complications (73.3%). While the exploratory cost-effectiveness analysis, which explicitly incorporated infection-related resource use, suggested potential quality-adjusted survival gains at increased incremental cost (base-case ICER approximately 183,000 MAD/QALY, approximately 1.5–2.0× GDP per capita), these findings remain highly uncertain and should primarily be viewed as generating hypotheses for future research and policy dialogue.
The scenario analysis comparing dose-reduced venetoclax with voriconazole prophylaxis versus full-dose venetoclax without azole highlighted the critical importance of coordinated pricing strategies for both the targeted agent and mandatory concomitant prophylaxis. Furthermore, our analysis of primary antifungal prophylaxis indicated that, under current cost structures, prophylaxis is unlikely to be cost-saving from a hospital budget perspective and should instead be justified primarily on clinical grounds, with potential QALY gains requiring validation in larger prospective studies.
Overall, our results highlight both the clinical feasibility of implementing azacitidine-venetoclax regimens with pharmacology-guided venetoclax dose reduction in a North African tertiary care setting, and the parallel need for optimized supportive care pathways, strengthened anti-infective prevention, broader access to comprehensive diagnostic work-up, and context-appropriate strategies to secure sustainable financing of innovative AML therapies in Morocco. These exploratory findings, derived from a small single-center cohort, support the need for prospective, multicenter studies to confirm efficacy, refine treatment strategies, and further improve survival and quality of life in elderly AML patients in resource-limited settings.
Footnotes
Acknowledgements
The authors thank the medical and nursing staff of the Clinical Hematology Department for their contribution to patient care and data availability. No writing assistance or third-party editorial support was received in the preparation of this manuscript
Author contributions
All authors have read and approved the final version of the manuscript and consent to its submission to the Journal of Oncology Pharmacy Practice.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
The data that support the findings of this study are not publicly available due to institutional confidentiality policies and patient privacy regulations. Anonymized, aggregated data may be made available from the corresponding author upon reasonable request and subject to applicable ethical and institutional approvals.