
Abstract
Background
Pomalidomide (POM) can cause skin rash, although it is generally considered less frequent than lenalidomide (LEN)-induced rash. However, skin rash remains a clinically relevant adverse event that may lead to treatment interruption in patients with multiple myeloma. This study aimed to identify clinical risk factors for POM-induced skin rash.
Methods
We retrospectively analyzed 76 patients who received POM-containing regimens between 2015 and 2022. The incidence, severity, and timing of skin rash were evaluated. Clinical variables were compared between patients with and without POM-induced skin rash, and multivariate logistic regression was performed to identify independent risk factors.
Results
POM-induced skin rash occurred in 22.4% of patients, with 17.1% experiencing Grade ≥2 rash. Treatment interruption due to rash occurred in 4 patients. A history of LEN-induced skin rash (p = 0.025) and no recent proteasome inhibitor exposure (p = 0.038) were identified as independent risk factors for POM-induced skin rash.
Conclusion
Patients with a prior history of LEN-induced skin rash or with long intervals since proteasome inhibitor exposure are at increased risk for POM-induced skin rash. Pharmacists should identify these high-risk patients before initiating POM therapy and implement early monitoring and supportive care to prevent unnecessary treatment interruption.
Introduction
Pomalidomide (POM) is an immunomodulatory drug (IMiD) that is widely used to treat patients with relapsed and refractory multiple myeloma (MM). It is an effective treatment option for patients who have become refractory to lenalidomide (LEN), another IMiD. 1 POM was initially used in combination with dexamethasone only, 2 but is now combined with proteasome inhibitors (bortezomib, carfilzomib, and ixazomib) and anti-CD38 antibody drugs (daratumumab and isatuximab), making it an essential medication for the treatment of relapsed and refractory cases.3–6
Among IMiDs, LEN has the highest frequency of skin rash adverse events.7–9 The frequency of these events is generally lower with POM than with LEN, and patients are sometimes switched to POM when LEN-induced skin rash necessitates the discontinuation of IMiDs. While LEN is associated with a high frequency of rash, with numerous studies examining its risk factors and management strategies,9–11 information on POM-related skin rash remains limited. Consequently, clinical studies have yet to demonstrate the safe administration of POM to patients with LEN-induced skin rash, and the safety of switching from LEN to POM has not been established. Therefore, we retrospectively analyzed risk factors for skin rash in patients treated with POM, including a history of LEN-induced skin rash, and investigated the incidence, severity, and timing of POM-induced skin rash.
Methods
Patients and methods
We retrospectively analyzed patients with relapsed/refractory MM who received a POM-containing regimen between August 2015 and July 2022 in the Department of Hematology at Eiju General Hospital. Inclusion criteria consisted of cases of relapsed/refractory MM treated with POM. Exclusion criteria included cases without a history of prior treatment for MM, those whose treatment with LEN or POM was initiated outside Eiju General Hospital, and those who discontinued POM treatment within 28 days for reasons other than POM-induced skin rash, because evaluation of skin rash incidence requires completion of at least one treatment cycle to appropriately capture both early- and late-onset skin rash events. The protocol for this study was reviewed and approved by the Ethics Committee of Eiju General Hospital (approval number: 2022-12).
All data from the medical records of eligible patients were extracted, and the following baseline information was collected: age, sex, M protein type, Eastern Cooperative Oncology Group performance status (PS), the International Staging System (ISS) stage, previous therapy, concomitant medications, and the development of skin rash during the administration of POM and LEN. In patients who developed skin rash, the date of rash onset, severity, whether treatment was interrupted, and the corresponding treatment type were also investigated.
Rash definition
Rash grade was classified using the Common Terminology Criteria for Adverse Events (CTCAE), Version 5.0 (https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5 × 7.pdf). Grade 1 corresponded to skin rash covering <10% of the body surface area (BSA), with or without associated symptoms. Grade 2 corresponded to rash covering 10–30% of BSA, with or without associated symptoms. Grade 3 corresponded to rash covering >30% of BSA, with or without associated symptoms. In cases in which the grade was defined as 2 or higher, a hematologist consulted with a dermatologist for final grading. The attribution of skin rash to POM was determined by hematologists and dermatologists based on clinical judgment, including temporal association, response to treatment interruption, and exclusion of alternative causes.
Statistical analysis
The chi-square test was used to compare categorical data. Regarding continuous variables, the Mann–Whitney U test was applied to compare non-normally distributed variables between patients with and without skin rash. A multivariable logistic regression analysis was performed to identify independent risk factors for skin rash. Factors with a p-value less than 0.1 from a univariate analysis were included in a multivariate analysis. A p-value less than 0.05 was considered to be significant. Because this was an exploratory retrospective study, a formal sample size calculation was not performed, and all eligible patients during the study period were included in the analysis. All statistical analyses were conducted using JMP® Pro 15 software (SAS Institute Inc., Cary, NC, USA).
Results
Patients
At Eiju General Hospital, 86 patients with relapsed/refractory MM were treated with POM. Of these, 4 patients who had treatment with LEN or POM initiated at other hospitals and 6 patients who discontinued POM treatment within 28 days due to disease progression or transfer to another hospital were excluded, leaving 76 patients eligible for evaluation. Patient characteristics are shown in Table 1.
Patient characteristics.
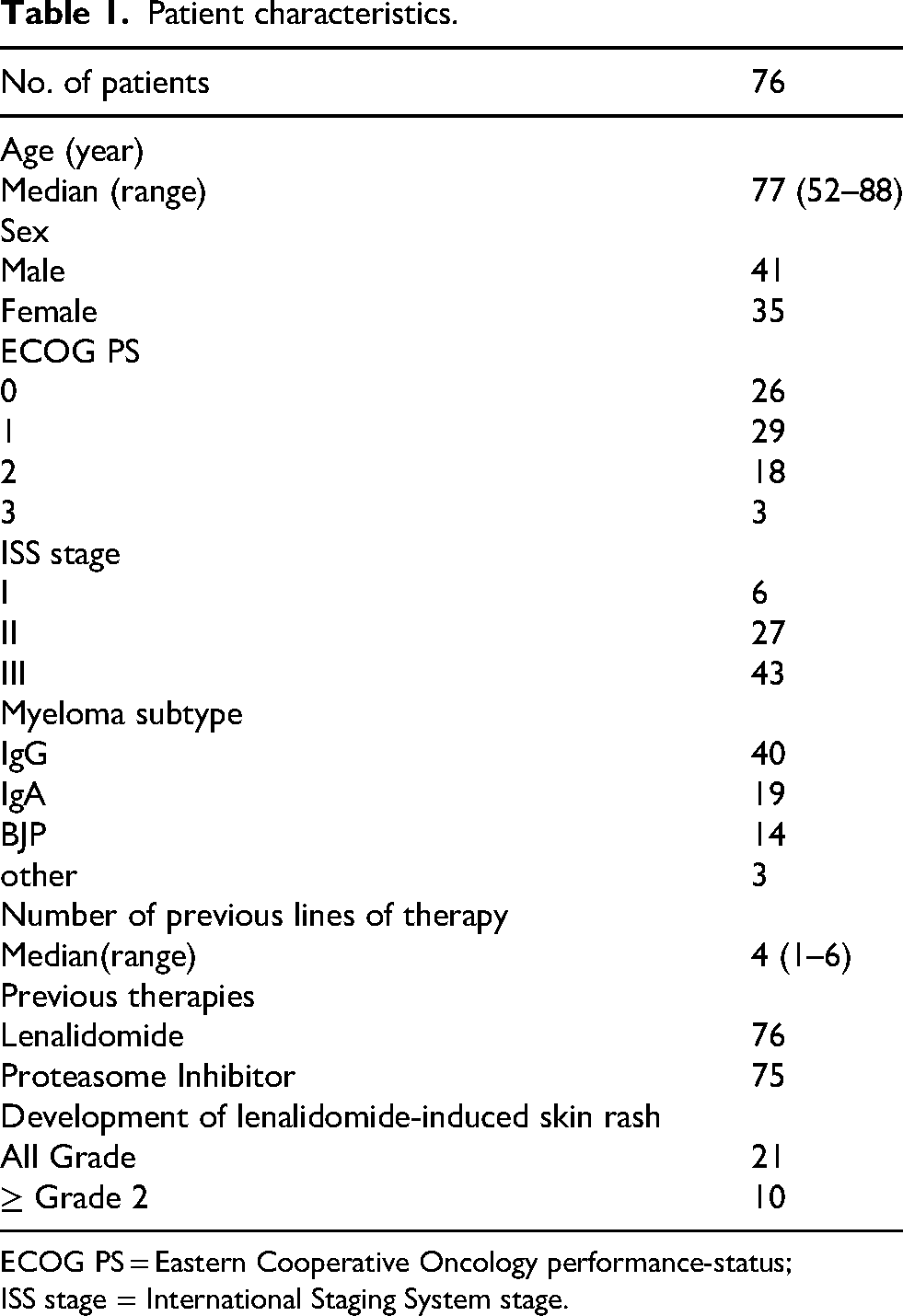
ECOG PS = Eastern Cooperative Oncology performance-status;
ISS stage = International Staging System stage.
The median age of the study population was 77 years. Among 76 patients, 35 were female and 41 were male. Myeloma types were as follows: IgG in 40 patients, IgA in 19, Bence-Jones protein in 14, and other types in 3. Of the 76 patients with a defined ISS classification, 6, 27, and 43 had stages 1, 2, and 3 diseases, respectively. PS was 0 in 26 patients, 1 in 29, 2 in 18, and 3 in 3. The median number of previous therapies was 4 (range: 1–6). All 76 patients were previously treated with LEN, while 75 had prior treatment with proteasome inhibitors. During the administration of LEN, skin rash occurred in 21 patients of all grades, with grade 3 or higher being observed in 10 patients. The median observation period was 3.7 months (range: 0.9–23.3).
Incidence of skin rash
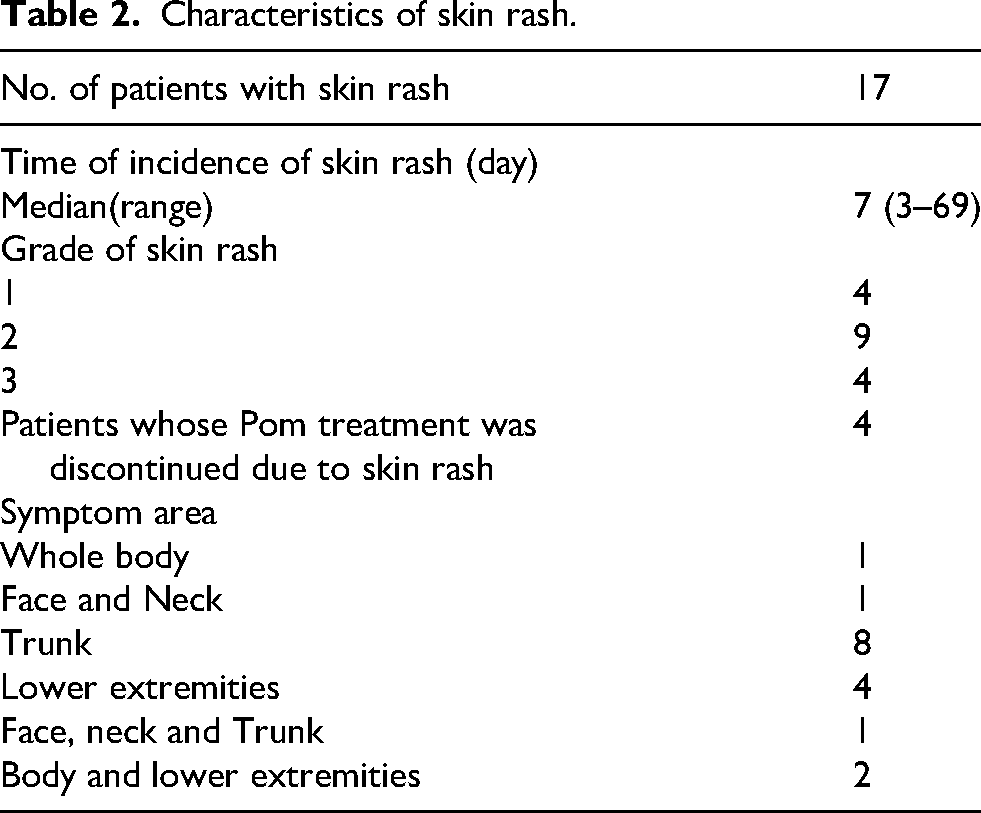
Seventeen patients (22.4%; 95% CI, 13.8–33.5%) developed skin rash during their POM-containing treatment (Table 2). Among those who developed skin rash, 4 patients (5.3%) had Grade 1, 9 (11.8%) had Grade 2, and 4 (5.3%) had Grade 3 skin rash. For Grade 1 rash, antihistamines were used in 1 patient and topical corticosteroids in 2 patients, and all patients continued POM without interruption. Among the 9 patients with Grade 2 rash, antihistamines were administered in 6 patients, topical corticosteroids in 1 patient, and systemic corticosteroids in 6 patients. Temporary treatment interruption occurred in 3 patients, and permanent discontinuation occurred in 1 patient at the patient's request. Re-administration was successful in 3 patients after temporary interruption. Among the 4 patients with Grade 3 rash, antihistamines and systemic corticosteroids were administered in all cases. POM treatment was permanently discontinued in 3 patients, including 1 patient who failed desensitization therapy. Two patients underwent desensitization therapy, and 1 patient was successfully re-administered POM. 12 Overall, 10 of 17 patients (58.8%) were able to continue POM treatment with supportive care or after temporary interruption, whereas 4 patients (23.5%) permanently discontinued POM due to skin rash. The median time for skin rash onset was 7 days (range: 3–69). The most common site of skin rash occurrence was the trunk in 9 patients (2 of whom also had skin rash on the lower extremities, and 1 simultaneously had skin rash on the face and neck). Skin rash was observed on the lower extremities in 6 patients (2 of whom also had skin rash on the trunk) (Table 2).
Characteristics of skin rash.
Relationship between patients with LEN-induced skin rash and POM-induced skin rash
Twenty-one patients developed LEN-induced skin rash. Of these, 10 patients had severe symptoms, including those for whom LEN administration was discontinued due to recurrent rash despite being Grade 2 and those who experienced Grade 3 skin rashes. Among the 45 patients without LEN-induced skin rash, 8 (17.8%) developed POM-induced skin rash. Among the 21 patients with LEN-induced skin rash, 9 (42.8%) developed POM-induced skin rash. Additionally, among the 10 patients who experienced severe LEN-induced skin rash, 4 (40.0%) developed POM-induced skin rash. The univariate analysis of the incidence of POM-induced skin rash in patients without LEN-induced skin rash and those with LEN-induced skin rash showed a p-value of 0.013, while that of patients without LEN-induced skin rash and those with severe LEN-induced skin rash showed a p-value of 0.078. Regarding severe skin rash, all cases of Grade 3 POM-induced skin rash occurred exclusively in patients with a prior history of LEN-induced skin rash, whereas no severe skin rash was observed in patients without such a history. Notably, among patients who experienced severe LEN-induced skin rash, 4 cases developed POM-induced skin rashes, with 1 being Grade 2 and 3 being Grade 3 (Figure 1). Although formal risk factor analysis for severe skin rash was not feasible due to the limited number of Grade 3 events, this consistent pattern suggests that a history of LEN-induced skin rash may be particularly relevant when assessing the risk of clinically significant POM-induced skin rash.
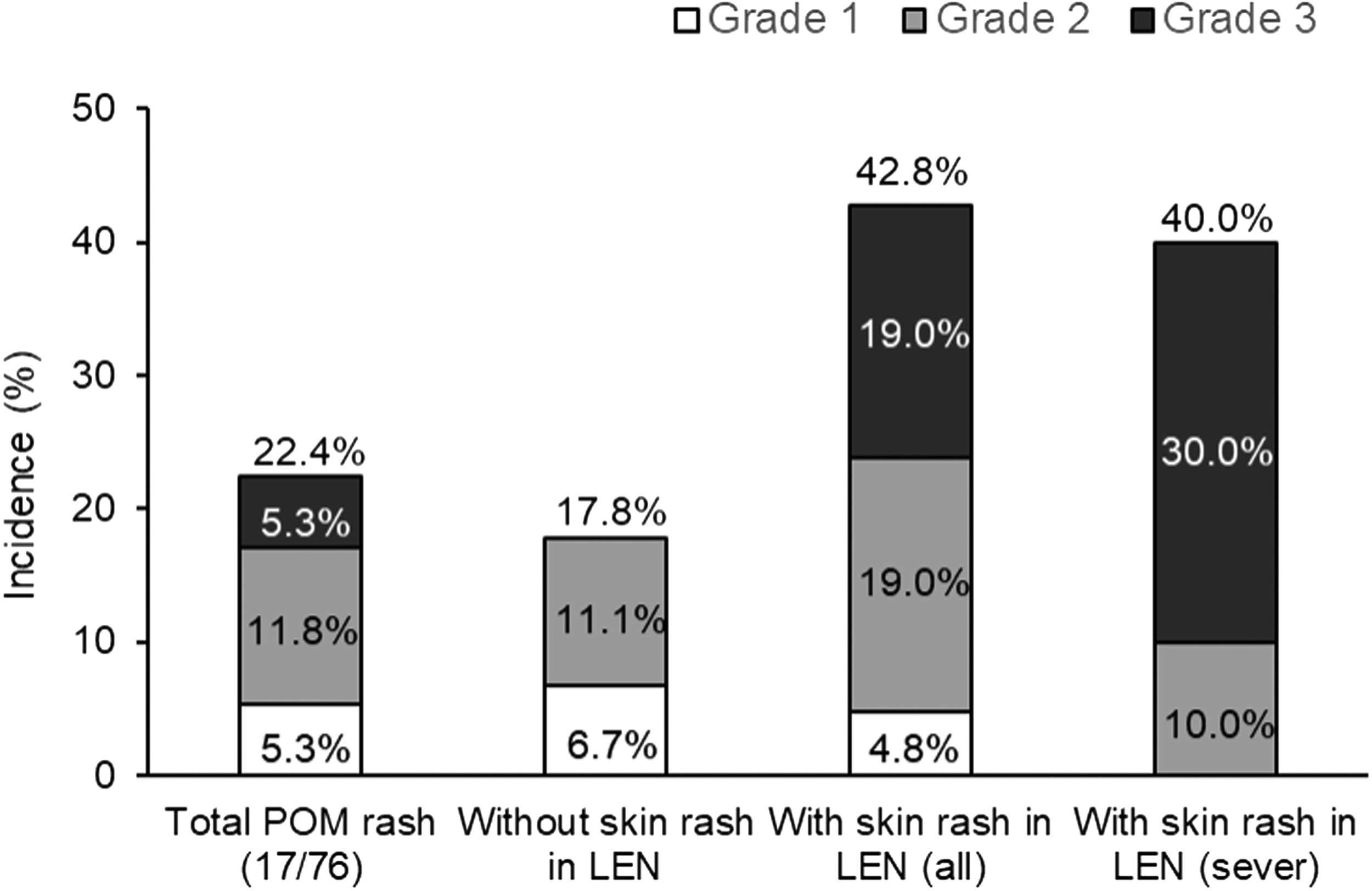
Incidence of Pomalidomide-induced skin rash according to prior Lenalidomide-induced skin rash status.
Analysis of risk factors
The results of the univariate analysis of the characteristics of patients with and without POM-induced skin rash are shown in Table 3. The following factors were identified as significant risk factors (p < 0.1): a history of skin rash induced by LEN (p = 0.008) and the use of proteasome inhibitors just before the POM-containing regimen (p = 0.024) (Table 4).
Risk factors associated with POM-induced skin rash from univariate analyses.
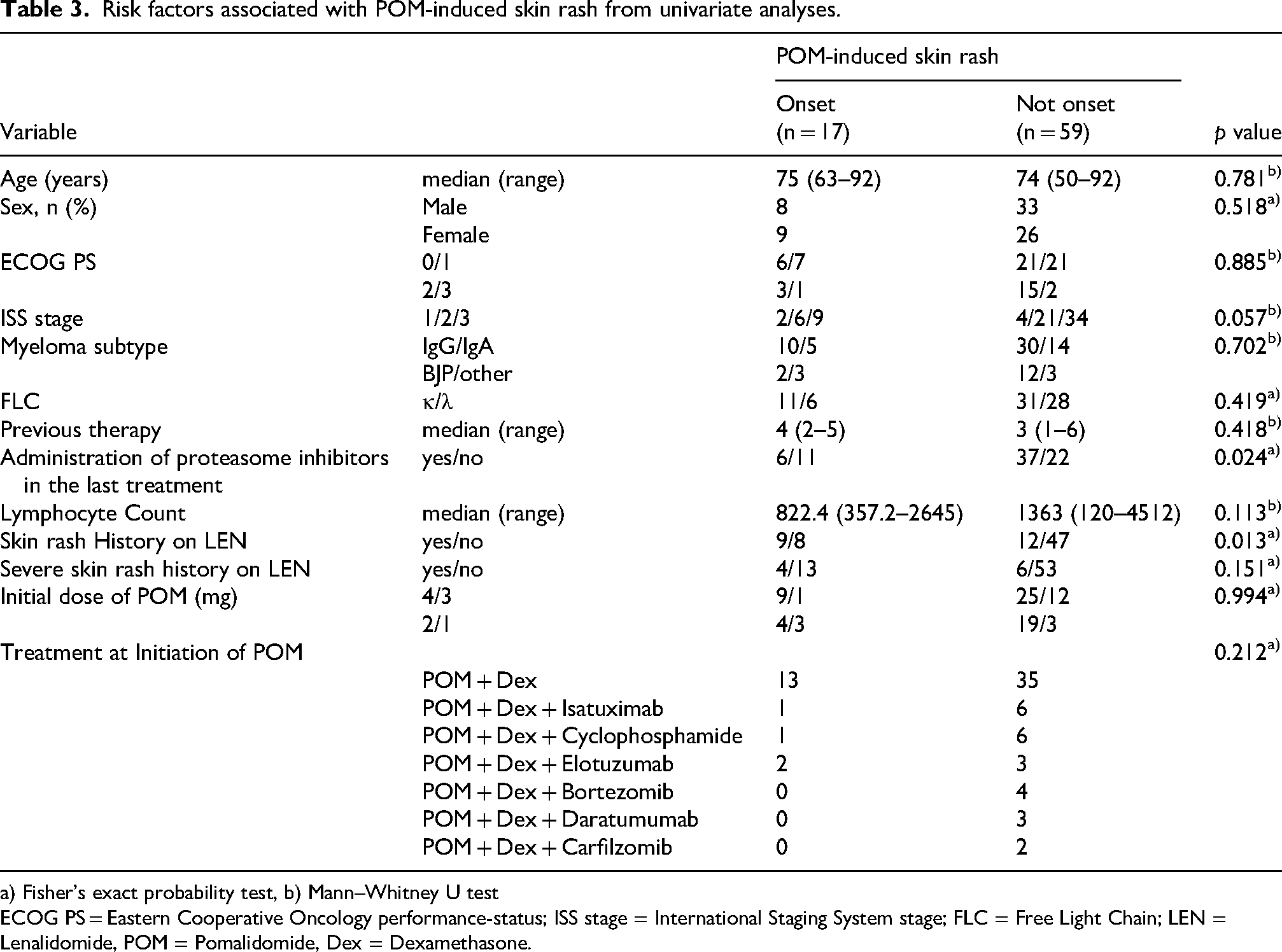
a) Fisher's exact probability test, b) Mann–Whitney U test
ECOG PS = Eastern Cooperative Oncology performance-status; ISS stage = International Staging System stage; FLC = Free Light Chain; LEN = Lenalidomide, POM = Pomalidomide, Dex = Dexamethasone.
Risk factors associated with POM-induced skin rash from multivariate analyses.
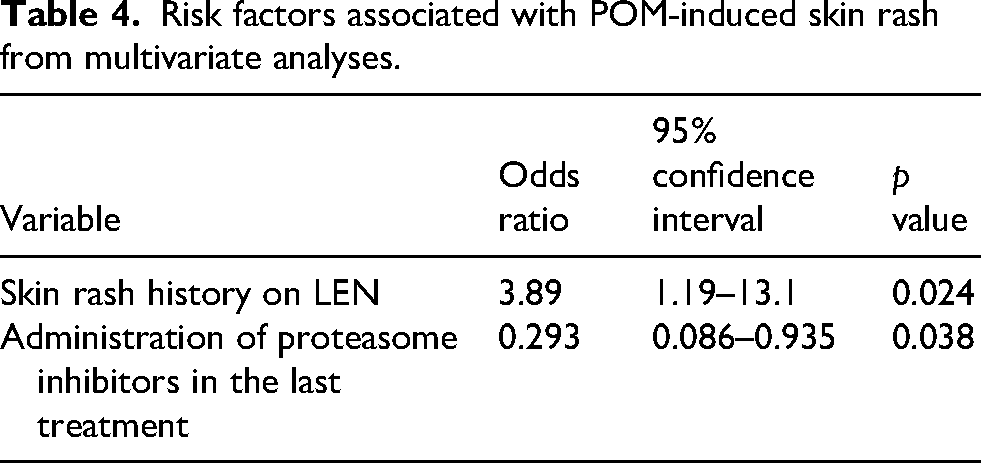
The results of the multivariate logistic regression analysis revealed that a history of skin rash induced by LEN (OR = 3.89; 95% CI, 1.19–13.1; p = 0.025) and the use of proteasome inhibitors just before the POM-containing regimen (OR = 0.293; 95% CI, 0.086–0.935; p = 0.038) correlated with the risk of skin rash (Table 3).
Discussion
The present study showed that POM-induced skin rash developed in 42.8% of patients with a history of LEN-induced skin rash and in 17.8% of patients without a history of LEN-induced skin rash, indicating a significantly higher incidence of POM-induced skin rash in patients with a history of LEN-induced skin rash. Severe skin rash (Grade 3) was only observed in patients with a history of LEN-induced skin rash, suggesting that POM-induced skin rash is slightly more severe in patients with severe LEN-induced skin rash. These results emphasize the importance of assessing the occurrence of skin rash during the administration of LEN in advance for patients transitioning from LEN to POM. Greater attention is needed when starting POM for patients with a history of LEN-induced skin rash.
POM and LEN are key drugs in the treatment of MM. Both drugs, similar to thalidomide, are classified as IMiDs. IMiDs exert potent direct tumor-killing and immune-enhancing effects by binding to cereblon (CRBN), a protein in the E3 ubiquitin ligase complex, leading to the subsequent proteasomal degradation of the transcription factors Ikaros (IKZF1) and Aiolos (IKZF3).13,14 Furthermore, they possess potent immunomodulatory properties by activating T/NK cells through the transcriptional repression of FoxP3, which suppresses regulatory T (Treg) cells.15,16 POM and LEN have several differences. LEN is widely used as a treatment option for newly diagnosed MM as well as relapsed or refractory MM. In contrast, POM is only indicated for relapsed or refractory MM and is administered to patients who were previously treated with LEN, proteasome inhibitors, antibody drugs, and similar therapies, as in the patients selected for this study. POM and LEN also differ pharmacologically in several aspects. For example, POM exhibits higher potency against CRBN, different substrate degradation kinetics, and a distinct gene activation profile that leads to unique antitumor and immunostimulatory properties.13,14,17,18 POM has demonstrated efficacy in LEN-resistant cell lines and animal models. 19 This activity has been documented in clinical trials where patients resistant to LEN derived clinical benefit from POM.2–6,20
Regarding drug-induced skin rash, the incidence of LEN-induced skin rash (27.2–50.0%) was higher than that of POM-induced skin rash (9.3–22.3%),9,10 with most previous studies focusing on LEN skin rash.9,10,21,22 A recent study reported that MM patients with LEN-induced skin rash had longer progression-free survival and overall survival than MM patients without LEN-induced skin rash. 23 Additionally, elderly patients were previously reported to be at a higher risk of developing LEN-induced skin rash, and a history of proteasome inhibitor administration prior to the initiation of LEN treatment (particularly immediately before starting LEN) reduced this risk. Some patients who developed skin rash were found to have elevated eosinophil levels.10,24 The mechanisms underlying the development of LEN-induced skin rash remain unclear; however, previous studies suggested a number of mechanisms, such as the enhancement of allergic reactions mediated by helper type 2 T (Th2) cells 25 or the activation of Th2 due to a decrease in the function of Treg cells from the administration of IMiDs, which was considered to be a delayed allergic reaction. 26 The validity of LEN is supported by reports of skin rash symptoms, the favorable timing of skin rash onset, and elevated eosinophils.9,10,24 Although information on POM-induced skin rash remains limited, POM is considered to cause skin rash through similar mechanisms to LEN because they share the same mechanism of action.
In addition to the history of LEN-induced skin rash, recent exposure to proteasome inhibitors immediately prior to POM initiation emerged as an independent factor associated with a lower risk of POM-induced skin rash in the present study. This finding suggests that the immune milieu shaped by recent proteasome inhibitor therapy may attenuate T-cell–mediated hypersensitivity reactions triggered by immunomodulatory drugs. The median (range) onset time of POM-induced skin rash was 7 days (3–69), which is consistent with a delayed-type of T-cell-mediated hypersensitivity reaction occurring more than 48 h after drug exposure. Furthermore, POM-induced skin rash was suppressed by the immediate prior administration of a proteasome inhibitor, which inhibited T-cell-mediated immunity in a manner similar to LEN-induced skin rash, 26 suggesting that POM-induced skin rash develops through the same mechanisms as LEN-induced skin rash. Although we planned to monitor eosinophils in the present study, we were unable to do so due to the lack of routine clinical measurements and missing data in most cases. However, eosinophils were measured in two patients with Grade 3 skin rash at the time of rash onset and were found to be elevated, indicating that some patients with POM-induced skin rash also have hypereosinophilic skin rash.
Based on the results of this study and POM-induced skin rash potentially occurring more frequently in patients with LEN-induced skin rash, we do not recommend the administration of POM as an alternative to LEN in patients with severe LEN-induced skin rash without careful consideration. Before the initiation of POM, it is important to review the history of skin rash during LEN treatment and the history of proteasome inhibitor administration. In patients with a history of severe skin rash caused by LEN and no recent proteasome inhibitor administration, careful monitoring is needed when initiating POM. If symptoms occur, early intervention with antihistamines, topical corticosteroids, or systemic corticosteroids is recommended.
The limitations of this study include its retrospective nature, small sample size, heterogeneity in patients’ prior treatment history and POM regimens, and the lack of uniformity in laboratory values after skin rash onset. Additionally, POM may have been administered to patients with advanced disease or a poor general condition immediately after its approval, and it is possible that some patients were difficult to interview and relatively mild symptoms were overlooked. Therefore, the true incidence may not have been accurately assessed. A well-designed prospective study with a large sample size is needed to resolve these issues. In addition, the limited number of Grade 3 skin rash events precluded formal risk factor analysis specifically for severe POM-induced skin rash in this study. In addition, because this was a retrospective study based on medical records, the peak severity of skin rash may not have been fully captured in some cases, potentially leading to underestimation of rash grade.
At the time these patients were treated, it was generally believed based on expert opinion that LEN-induced skin rash did not necessarily predict intolerance to POM, and prophylactic antihistamine use was not routinely performed. However, our findings suggest that LEN-induced skin rash history warrants heightened monitoring and proactive supportive care when initiating POM.
Following this analysis, our institution implemented pharmacist-led preventive strategies, including standardized patient education, early-cycle monitoring, and selective prophylactic antihistamine administration or inpatient initiation for high-risk patients.
Pharmacist-led practice implications
In our institution, pharmacists have been consistently involved in monitoring skin toxicity associated with IMiDs. The monitoring approach used for POM was originally adapted from our established management practices for LEN-induced skin rash. Since 2020, based on our previous institutional study identifying that patients without prolonged proteasome inhibitor exposure were at higher risk for LEN-induced skin rash,10,27 pharmacists have paid particular attention to patients with long intervals since their last proteasome inhibitor treatment. In this study, a similar association was demonstrated for POM-induced skin rash, reinforcing the clinical relevance of pharmacist-led treatment history review before therapy initiation. For inpatients, pharmacists conducted daily skin assessments during the first cycle, while for outpatients, pharmacists provided counseling at dispensing regarding early-onset rash and reassessed symptoms at the beginning of the second cycle. These findings highlight that pharmacists are well positioned to identify high-risk patients and implement targeted early monitoring. Developing standardized pharmacist-driven monitoring pathways may reduce unnecessary treatment interruptions and optimize therapeutic continuity in MM care.
Conclusion
This is the first study to demonstrate that a history of LEN-induced skin rash and lack of recent proteasome inhibitor exposure are clinically relevant risk factors for POM-induced skin rash. When initiating POM therapy, it is important to review both prior treatment regimens and adverse events, particularly the presence and severity of LEN-induced skin rash. Oncology pharmacists are well positioned to identify high-risk patients before treatment initiation and to provide early monitoring and supportive care to prevent unnecessary treatment interruption. Further prospective studies are warranted to validate pharmacist-led monitoring strategies and optimize treatment continuity in multiple myeloma care.
Footnotes
Author note
Ryota Kushi was affiliated with Eiju General Hospital at the time of the study.
He is currently affiliated with Mitsui Memorial Hospital.
Acknowledgments
We would like to express our deepest gratitude to the patients involved in this study. We thank Medical English Service for English language editing.
Ethical approval
This study was approved by the Ethics Committee of Eiju General Hospital (approval number: 2022-12).
Consent to participate
Because this study was retrospective and used anonymized data, the requirement for written informed consent was waived, and an opt-out approach was implemented in accordance with institutional and national ethical guidelines.
Consent for publication
Not applicable. This study does not contain identifiable individual data.
Authors’ contributions
TS, RK, HH, and MH designed the study protocol. TS, RK, HN, YI, and MI collected clinical data. TS and RK analyzed and interpreted the data. TS drafted the manuscript. HH, HN, YI, MI, RIN, and MH critically reviewed and revised the manuscript. All authors read and approved of the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.