
Abstract
Introduction
Rasburicase is a high-cost medicine indicated for the prevention and treatment of tumour lysis syndrome (TLS). Growing evidence supports low fixed-dose rasburicase regimens (3–6 mg), however, uncertainty remains regarding their ability to prevent progression to clinical TLS, particularly in high-risk populations. Some institutions implement medicine governance strategies, such as a medicines formulary, to optimise safe, effective, and economical use through specific criteria, risk stratification and dosing stipulations, to facilitate appropriate prescribing. This study aimed to evaluate biochemical TLS (BTLS) and clinical TLS (CTLS) outcomes with rasburicase and characterise compliance with institutional prescribing criteria.
Methods
A retrospective, single-centre, observational study was conducted of adults with haematologic malignancies who received at least one dose of rasburicase between March 2017 and March 2025. Rasburicase indication, dosing, TLS outcomes, and compliance with prescribing criteria were analysed.
Results
Out of the 144 patients, 114/144 (79%) were high-risk for TLS and 99/144 (69%) received rasburicase prophylactically. Fixed low-doses predominated, with 61% receiving a single dose. Urate normalisation within 24 h occurred in 92% of all patients and 97% of prophylaxis patients. Despite rapid biochemical response, 47/99 (47%) of prophylaxis patients demonstrated LTLS and 14/99 (14%) developed CTLS, where 9/14 (64%) had pre-existing kidney impairment. Prescribing criteria compliance was 85%, with non-compliance primarily attributed to early biochemical changes or urgent need for anti-cancer therapy.
Conclusion
This study confirmed the clinical and economic validity of low fixed-dose rasburicase for TLS prophylaxis in high- and intermediate-risk patients and TLS treatment, while demonstrating high compliance with institutional prescribing criteria.
Introduction
Tumour lysis syndrome (TLS) is a significant oncological emergency in patients with haematologic malignancies. 1 TLS can occur spontaneously, but it primarily occurs 6 to 72 h following systemic anticancer therapy (SACT) or radiation initiation. 1 TLS involves the destruction of malignant cells, which rapidly release intracellular contents and their metabolites into the systemic circulation. 1 Subsequent metabolic derangements such as hyperuricaemia, hyperkalaemia, hyperphosphataemia and secondary hypocalcaemia can precipitate severe clinical consequences, including kidney impairment, cardiac arrhythmias, seizures, neurological complications and sudden death. 1 Early identification of at-risk patients, initiation of TLS prophylactic measures prior to SACT, and prompt management of TLS if it occurs, are essential.
Cairo-Bishop classify TLS as either laboratory TLS (LTLS) or clinical TLS (CTLS). 1 LTLS is characterised by laboratory evidence of two or more metabolic abnormalities associated with TLS within 3 days before or 7 days after SACT, in the absence of symptoms. 1 Laboratory evidence includes abnormal levels of urate (≥0.476 mmol/L), potassium (≥6.0 mmol/L), phosphate (≥1.45 mmol/L), or calcium (≤1.75 mmol/L), or a 25% change from baseline in any of these. 1 CTLS is defined as the presence of LTLS accompanied by the development of at least one known clinical consequence of TLS not caused by SACT, including a creatinine level ≥1.5 x upper limit of normal (ULN), cardiac arrhythmia, seizure and sudden death.1,2
The reported incidence of TLS varies widely due to differences in patients, malignancy type, SACT protocol and prophylaxis strategy. 2 Of particular concern, with the development of highly effective SACT, the overall TLS incidence has increased, with LTLS reported more frequently than CTLS. 2 To mitigate TLS risk, current guidelines recommend appropriate risk stratification, aggressive hydration, and the use of anti-hyperuricaemic therapy prophylaxis for patients at intermediate- and high-risk of TLS.3,4
Anti-hyperuricaemic therapy for TLS typically involves either allopurinol, a xanthine oxidase inhibitor, or rasburicase, a recombinant urate oxidase, or both. Allopurinol prevents the formation of new urate but does not reduce existing urate levels. In contrast, rasburicase catalyses the enzymatic conversion of urate into allantoin, a more soluble and readily excretable metabolite. 5 This mechanism allows rasburicase to rapidly eliminate circulating urate, making it highly effective for both the prophylaxis and treatment of TLS-related hyperuricaemia. Despite adoption of early risk identification strategies and prophylactic therapy, TLS remains a significant treatment-related complication in haematological malignancies. 4 CTLS, while rare, is reported to affect 3–6% of patients with high-grade tumours, and associated with an increased risk of mortality, highlighting the importance of optimising anti-hyperuricaemia strategies.3,4
The place in therapy for rasburicase varies internationally according to regulatory approval and formulary access. The Therapeutic Goods Administration (TGA), Australia's government agency responsible for regulating medicines, has rasburicase 1.5 mg vial registered for the prophylaxis and treatment of acute hyperuricaemia, in patients with haematologic malignancies at risk of a rapid tumour lysis using a weight-based regimen of 0.2 mg/kg/day for 5 to 7 days. 5 This regimen, while effective, imposes a significant cost burden at approximately AUD $200 (USD $142) per 1.5 mg vial.5,6
In the study context, access to rasburicase is not authorised on the state level adult medicines formulary. 7 Access for prophylactic use is governed through a directorate-level formulary, which specifies eligibility criteria based on TLS risk stratification at a lower fixed-dose of 3 mg or 6 mg (rather than the TGA approved regimen) (Table 1). This governance structure streamlines administration of urgent therapy for TLS prophylaxis, reducing delays in therapy, workload and financial burden. A 3 mg dose would cost AUD $400 (USD $284) versus AUD $14,935 (USD $10,633) for an 80 kg adult prescribed 7 days treatment. Use of rasburicase for the treatment of established TLS at this institution, however, requires individualised governance approval on a case-by-case basis.
Institutional prescribing criteria for prophylactic rasburicase use in haematologic malignancy in doses of 3 mg or 6 mg according to TLS risk category.
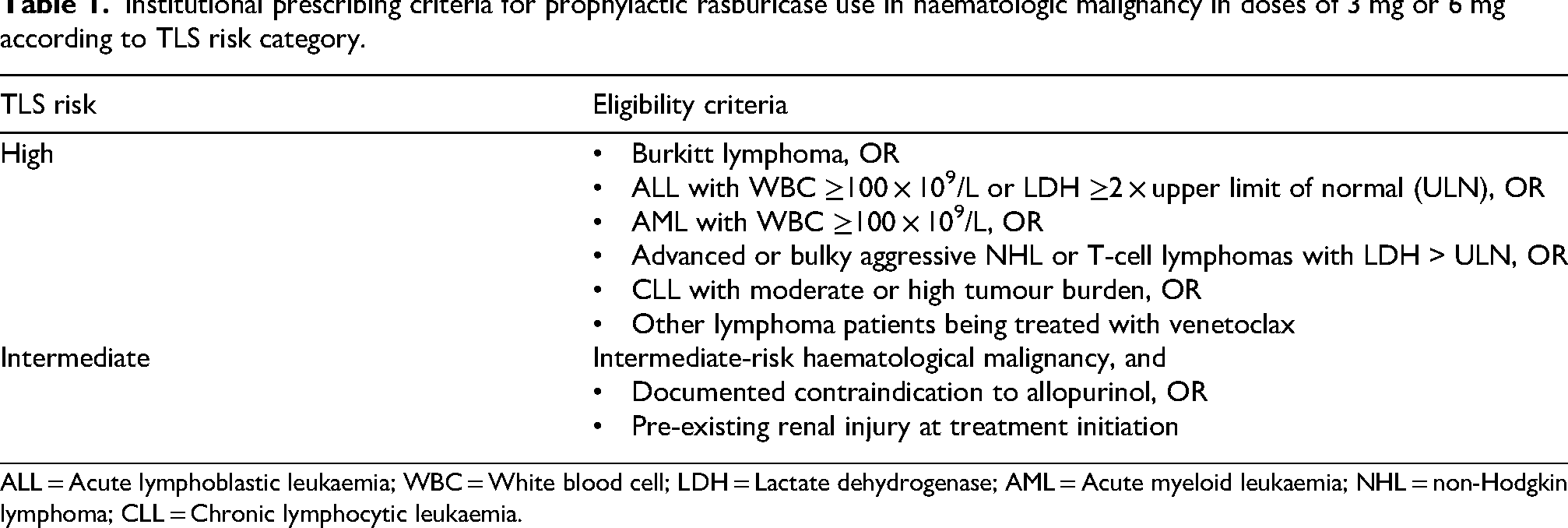
ALL = Acute lymphoblastic leukaemia; WBC = White blood cell; LDH = Lactate dehydrogenase; AML = Acute myeloid leukaemia; NHL = non-Hodgkin lymphoma; CLL = Chronic lymphocytic leukaemia.
Coiffier et al. established the efficacy of weight-based multiday rasburicase dosing (0.2 mg/kg/day for 3–7 days) in adults with aggressive NHL, demonstrating rapid and sustained urate normalisation. 8 A subsequent prospective study confirmed single-dose weight-based strategies could achieve biochemical control comparable to the approved multiday regimen in many patients at intermediate and high risk of TLS. 9 Other retrospective analyses have extended this evidence to fixed low-dose strategies, demonstrating no statistically significant difference between fixed low-dose groups and weight-based dosing groups, 10 and no clear dose-response relationship between weight adjusted dose and urate decline. 11
More recent comparative analyses have directly evaluated 3 mg versus 6 mg dosing and generally reported similar rates of urate normalisation.10–12 However, these studies frequently excluded prophylaxis patients, 12 included mixed malignancies10,11 or substantial proportions of low-risk patients, 11 and reported limited repeat dosing.10–12 As a result, uncertainty remains regarding the ability of fixed low-dose rasburicase to prevent progression to clinical TLS in a predominantly high-risk haematologic population.
This retrospective observational study aimed to evaluate the effectiveness of fixed low-dose rasburicase (3 mg and 6 mg) in high- and intermediate-risk TLS cohorts, including prophylaxis and treatment populations, at an Australian tertiary institution. The primary objective was to assess biochemical response, defined as normalisation of serum urate (≤0.476 mmol/L) within 24 h of rasburicase administration. Secondary objectives included evaluation of LTLS and CTLS incidence in patients receiving prophylactic doses of rasburicase, and description of repeat dose use, renal recovery, and clinical factors associated with progression to CTLS. Institutional adherence to local risk stratification criteria was examined as a contextual measure to characterise current prescribing practice. The findings from this study provide evidence to optimise the safe and cost-effective use of fixed low-dose rasburicase in high-risk patients and support continuing appropriate governance.
Methods
This study was granted exemption from requirement of ethical review by a Medicines Use Evaluation Subcommittee of the Medicines Management Committee under a protocol approved by a Human Research and Ethics Committee (CM22042501).
Study design and patient population
A retrospective observational study was conducted of all adult patients (≥18 years) with haematological malignancies who received at least one dose of rasburicase for the prophylaxis or treatment of TLS between March 1, 2017, and March 20, 2025, at a large tertiary metropolitan hospital in Brisbane. Patients were excluded if rasburicase was administered as part of a clinical trial protocol, or for non-haematological malignancy indications.
Participant identification and recruitment
Patients were identified through detailed review of multiple institutional databases to ensure complete case capture. The primary data source was the hospital pharmacy dispensing system, iPharmacy, which recorded all instances of rasburicase supply during the study period. 13 Each record identified was subsequently cross-checked using the electronic medical record to confirm administration. Two additional databases, the Oncology Information Management Solution system, CHARM, and the Intensive Care Unit clinical information system, Metavision, were reviewed to identify any doses not captured in the pharmacy dispensing system.14,15
Data collection
Data were collected through detailed review of electronic medical records using a project-specific data collection tool. Collected variables included patient demographics, malignancy type, prephase treatment, SACT protocol and initiation date, tumour bulk, WBC, LDH, and absolute lymphocyte count (ALC). Pre-existing kidney injury, defined as baseline eGFR <50 mL/min, was documented. Details of rasburicase administration were recorded, including indication, dose administered (mg), number of doses administered, and time of dose administration. Concurrent therapies relevant to TLS management, such as allopurinol use or contraindication and use of phosphate binder therapy, were also documented. Laboratory values were collected at defined time points: baseline (≤14 days before first rasburicase dose), and at 24, 48, 72 h, and 7 days after administration. When multiple measurements were available, the value closest to the specified timepoint (24, 48, or 72 h) was used for analysis. A peak serum urate concentration (Cmax), defined as the highest value within 24 h post SACT initiation with rasburicase, was also recorded.
Definitions and classifications
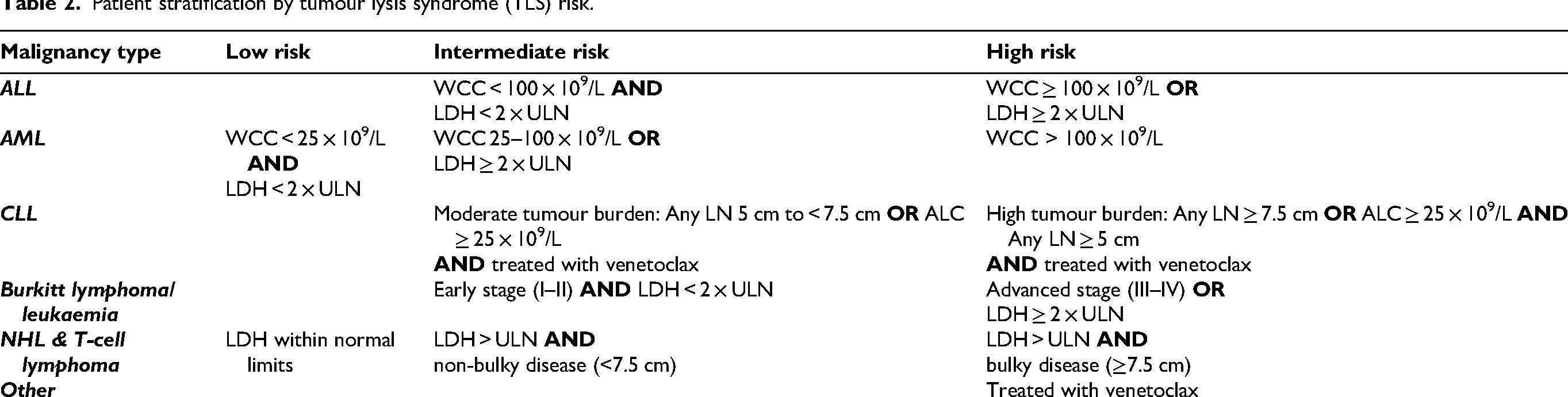
Patients were categorised by indication as either prophylaxis or treatment. Prophylaxis was defined as rasburicase administration in patients without evidence of LTLS or CTLS prior to initiation of SACT or prephase treatment, including corticosteroids or hydroxyurea. Treatment was defined as rasburicase administered for established LTLS or CTLS, occurring following prephase treatment, SACT initiation or spontaneous autolysis. All patients were stratified into low, intermediate, or high risk for TLS according to malignancy type and clinical risk factors (Table 2). Risk categories were adapted from the Cairo-Bishop and Coiffier classifications, incorporating institutional prescribing criteria. Evidence of LTLS or CTLS was classified using published Cairo-Bishop diagnostic criteria.1,3
Patient stratification by tumour lysis syndrome (TLS) risk.
Rasburicase dosing
During the study period, fixed low-dose rasburicase (3 mg or 6 mg) was the standard institutional approach for TLS prophylaxis and treatment. Dose selection was clinician-directed and based on individual patient characteristics, including baseline serum urate level, TLS risk category, kidney function, tumour burden, and overall clinical assessment, rather than directed by institutional prescribing criteria. Repeat dosing was permitted based on biochemical response and clinical judgement. The number of doses administered and the interval between doses were recorded.
Data analysis
All variables were summarised using descriptive statistics. Categorical variables were expressed as frequencies and percentages, while continuous variables were reported using medians and ranges or interquartile ranges for the study cohort.
Outcomes
The primary outcome was biochemical response, defined as normalisation of serum urate (≤0.476 mmol/L) within 24 h of rasburicase administration. Secondary outcomes were the incidence of LTLS and CTLS, repeat dosing requirements, renal recovery, and identification of clinical factors associated with CTLS progression among patients who received rasburicase for TLS prophylaxis. Institutional adherence to prescribing criteria based on risk stratification was assessed as an exploratory measure to characterise prescribing practice.
Results
A total of 161 patients received rasburicase between March 2017 and March 2025, of whom 144 met inclusion criteria. Reasons for exclusion included rasburicase administration as part of a clinical trial protocol (n = 14) or use for a non-haematologic malignancy indication (n = 3). Baseline patient characteristics are described in Table 3. The median age was 62.5 years (range 19–91 years), and 63.9% of patients were male. The most common haematologic malignancies were AML (33.3%) and NHL (26.4%). The majority of patients (79.2%) were classified as high-risk for TLS.
Baseline characteristics of the study patients.
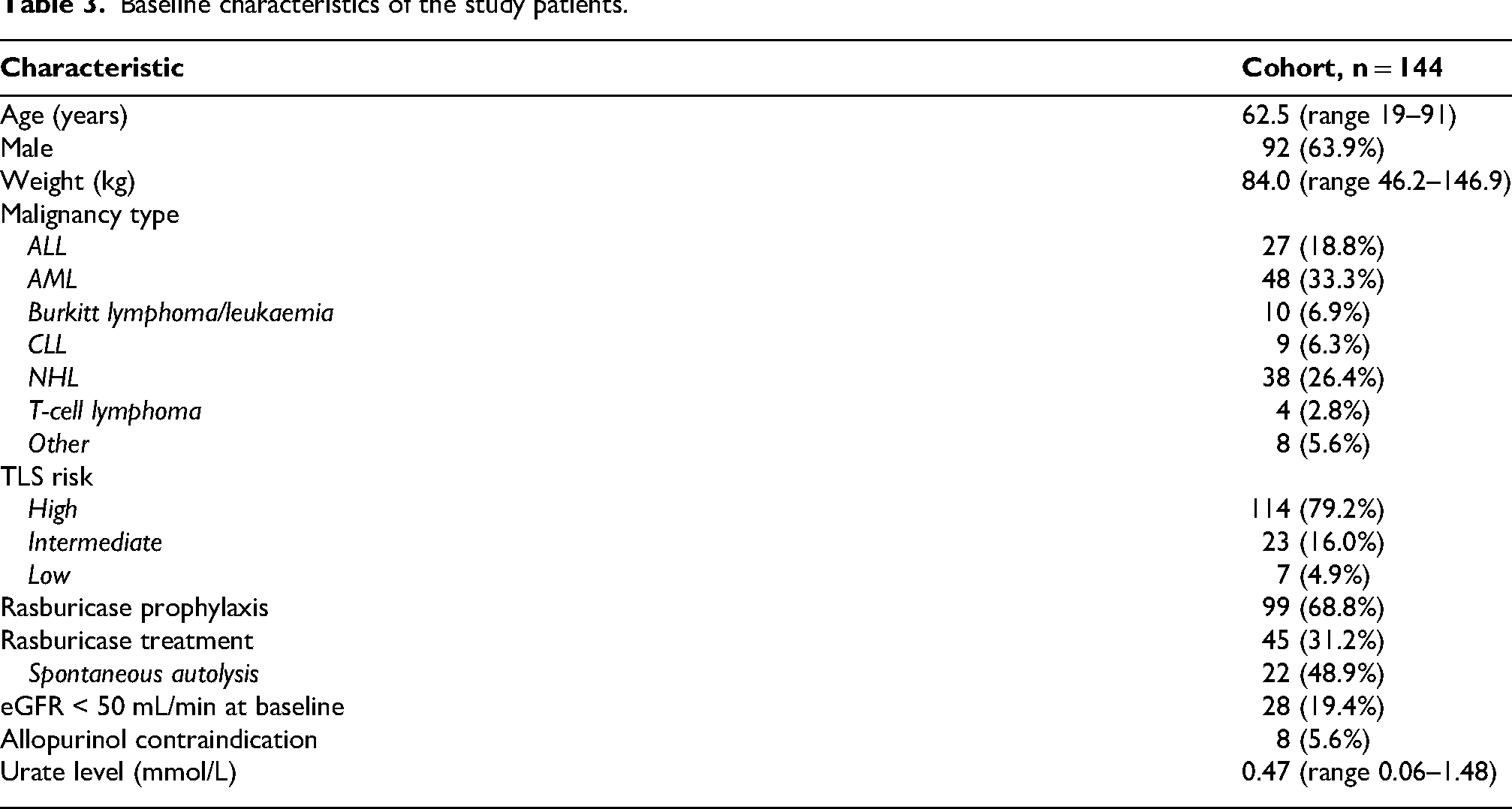
Rasburicase was used prophylactically in 99 (68.8%) cases, and for TLS treatment in 45 (31.2%) patients. Among patients receiving rasburicase for treatment, 22 out of 45 (48.9%) received rasburicase for spontaneous autolysis, 10 out of 45 (22.2%) for TLS potentiated by prephase treatment, and 13 out of 45 (28.9%) following SACT initiation. Pre-existing kidney injury was evident in 28 (19.4%) patients, and 8 (5.6%) patients had a documented contraindication to allopurinol. The median baseline serum urate level was 0.47 mmol/L (0.06 −1.48 mmol/L) across the study cohort.
Rasburicase dosing
Across the study period, a total of 254 rasburicase administrations were recorded, predominantly as prophylaxis (n = 149). Fixed-dose regimens were standard practice, with 61% of patients receiving a single dose, 22% receiving two doses, and 17% receiving more than two doses. Additional doses were typically administered in the context of aggressive and/or bulky disease, kidney injury, or ongoing LTLS or CTLS management. The median administered dose was 3 mg (3–6 mg). Among patients receiving more than one dose, the median dosing interval was 25 h (0.8 to 374 h). Relevant concurrent TLS therapies included allopurinol use in 94% of patients and phosphate binders in 28% of patients.
Primary outcome: biochemical response
Urate normalisation (≤0.476 mmol/L) within 24 h was achieved in 92% of all patients. Normalisation occurred in 97% of those receiving rasburicase for prophylaxis and 80% of those receiving rasburicase for treatment (Figure 1). Among patients prescribed rasburicase as prophylaxis, urate normalisation was maintained through to day 7 by 97.8%.
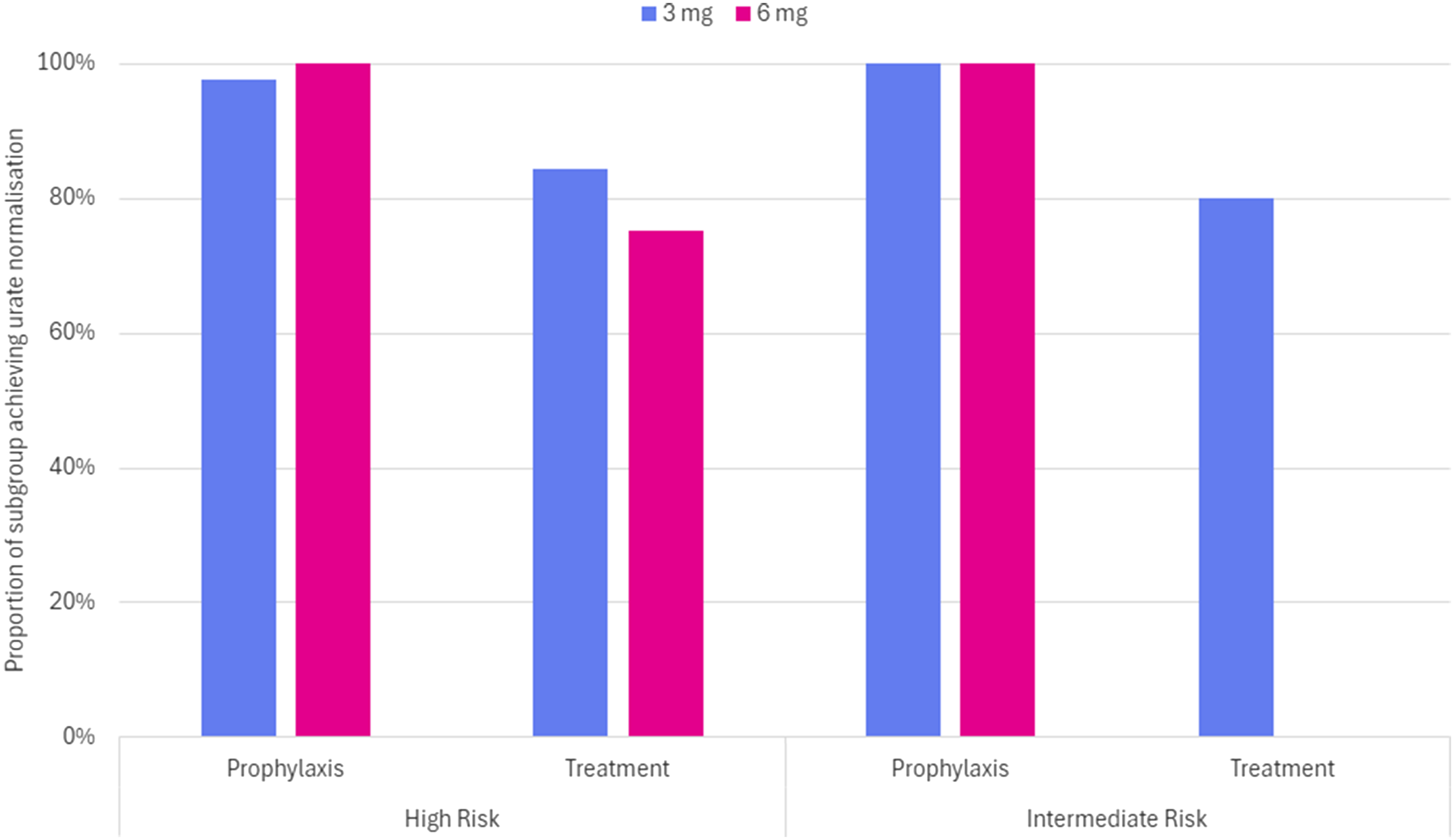
Proportion of urate normalisation (≤0.467 mmol/L) within 24 h by risk category, indication, and initial rasburicase dose.
The extent of serum urate reduction within 24 h varied across risk, dose and indication subgroups, with percentage reductions ranging from 23% to 87%. Patients classified as high-risk for TLS achieved the greatest absolute reductions in urate, with a median decrease of −0.37 mmol/L (IQR −0.49 to −0.14) from a median baseline of 0.50 mmol/L. In contrast, intermediate-risk patients demonstrated a smaller median decrease in urate of −0.14 mmol/L (IQR −0.27 to −0.06) from a median baseline of 0.29 mmol/L.
When analysed by dose, 3 mg and 6 mg regimens produced comparable biochemical responses across the study group, with median urate reductions of −0.26 mmol/L (IQR −0.39 to −0.11) and −0.38 mmol/L (IQR −0.52 to −0.21), respectively. High-risk patients were almost equally likely to receive 3 mg or 6 mg doses (50.9% vs 49.1%), whereas lower-risk patients predominantly received 3 mg doses (70.0%). Repeat dosing followed a similar pattern: 44.7% of high-risk patients required >1 dose, compared with 16.7% of lower-risk patients. Among high-risk patients, additional doses were required at similar rates for the 3 mg and 6 mg regimens (46.6% and 42.9%), respectively.
Further stratification by indication demonstrated that patients prescribed rasburicase as prophylaxis achieved a median urate reduction of −0.31 mmol/L (IQR −0.42 to −0.13), while those receiving rasburicase for treatment achieved median urate reductions of −0.37 mmol/L (IQR −0.58 to −0.10). Among high-risk patients receiving a 6 mg dose of rasburicase, median urate reductions were similar for prophylaxis and treatment indications (−0.41 mmol/L [IQR −0.49 to −0.33] and −0.42 mmol/L [IQR −0.66 to −0.07]), respectively). No intermediate-risk patients received 6 mg dosing for treatment (Figure 2).
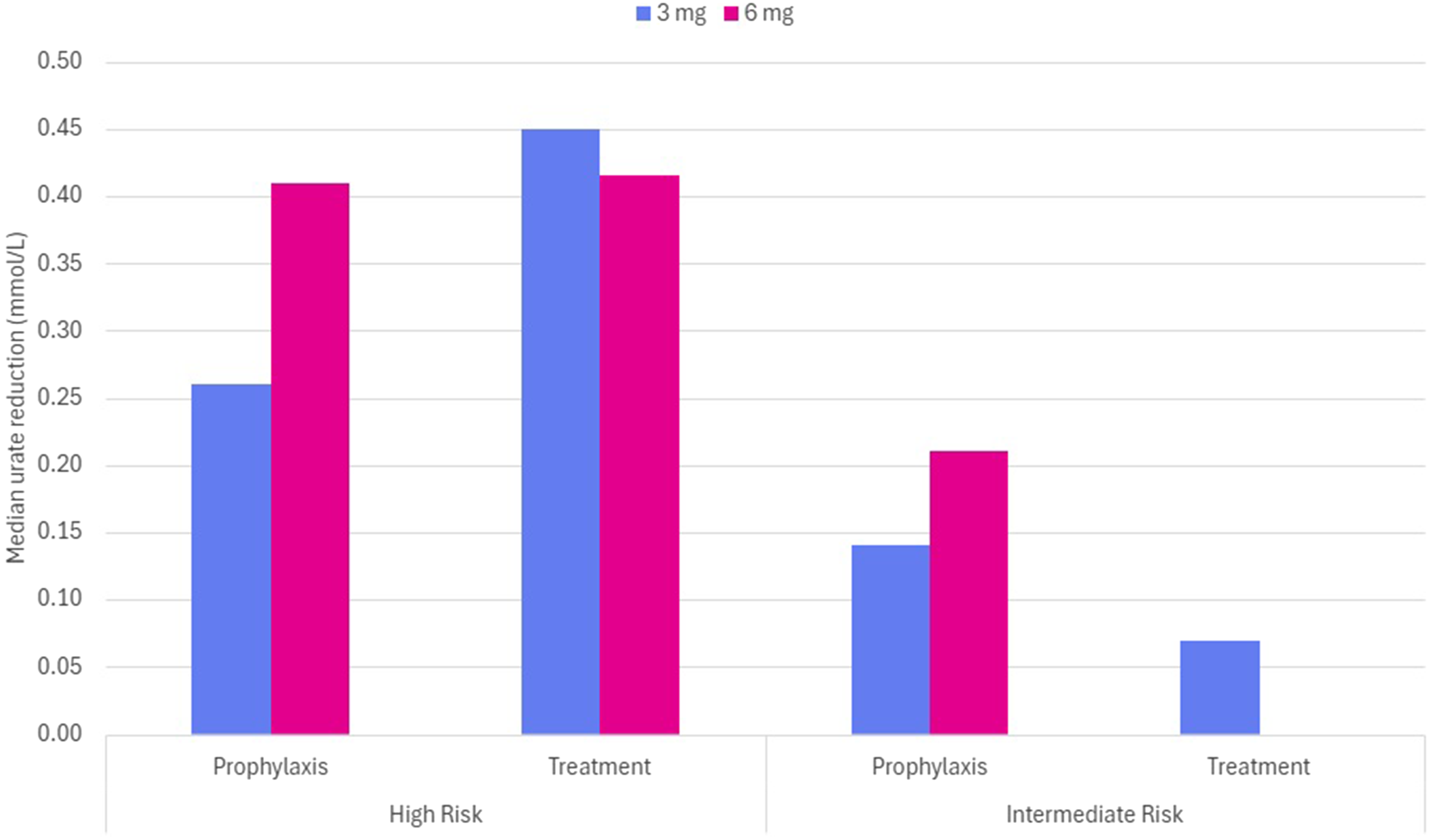
Median reduction in serum urate (mmol/L) within 24 h by risk category, indication, and initial rasburicase dose.
Secondary outcome
Laboratory and clinical TLS outcomes of prophylaxis patients
Among patients prescribed rasburicase for prophylaxis, 47 out of 99 (47%) demonstrated transient evidence of LTLS after SACT initiation, most driven by elevations in urate and phosphate (70%). Urate was normalised within 24 h in all cases, with rebound urate elevation evident in only 3 out of 99 (3%) patients between 48 h and day 7.
Of those with LTLS, 14 out of 47 (29.8%) progressed to CTLS, representing 14% of all patients prescribed rasburicase for prophylaxis. The majority of CTLS occurred in high-risk patients, 10 out of 14 (71%), compared to lower risk patients where there was 4 out of 14 (29%). All CTLS cases were associated with a creatinine level ≥1.5 x ULN, and 9 out of 14 (64.2%) patients had pre-existing kidney impairment at baseline. The severity of CTLS was moderate with a median grade of 2 (range 2–3) per Cairo-Bishop TLS grading. 1 Kidney function recovered to baseline by day 7 in 6/14 (43%) of patients.
Rasburicase use compliance with prescribing criteria
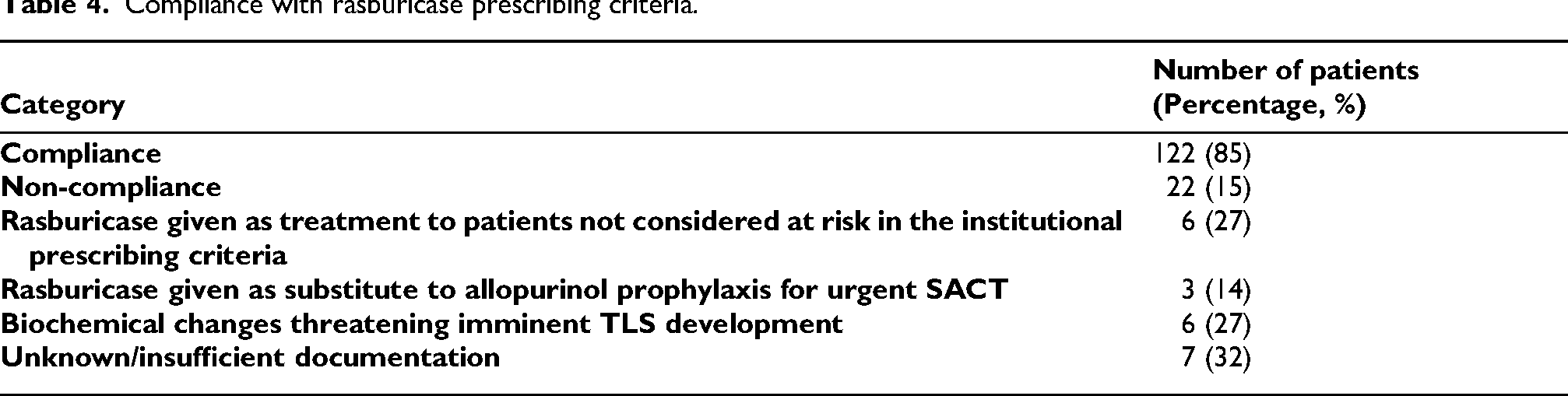
Overall compliance with institutional prescribing criteria was 85%. Non-compliance was 15% with documented reasons for non-compliance summarised in Table 4, where documentation was available.
Compliance with rasburicase prescribing criteria.
Discussion
This study delivers a detailed evaluation of fixed low-dose rasburicase use in a predominantly high-risk haematologic population. Doses of 3 mg or 6 mg demonstrated comparable biochemical responses in producing rapid and sustained urate normalisation in over 90% of patients, while revealing important limitations in preventing TLS progression. In contrast to prior fixed-dose studies that largely focused on short-term biochemical endpoints, our findings integrate biochemical response, repeat dosing needs, and CTLS outcomes within a cohort where 79% of patients were classified as high-risk. This distinction is valuable as the efficacy of fixed-dose strategies in lower-risk or mixed malignancy population may not reflect outcomes in more aggressive and/or bulky disease states. Despite near universal urate control, progression to CTLS occurred in a subset of patients, particularly those presenting with baseline kidney impairment. These findings extend the existing fixed-dose literature by demonstrating that while biochemical efficacy is preserved in a predominantly high-risk cohort, CTLS progression remains influenced by baseline kidney impairment and metabolic burden.
Biochemical outcomes
Consistent with existing literature, the results of this study show that low-fixed doses of rasburicase achieved urate normalisation in 92% of patients at high- or intermediate-risk for TLS. Response rates were comparable to those observed by Trifilo et al. and McBride et al., with a 3 mg dose (72% and 92.2%, respectively), however, our study showed greater median urate reductions within the high-risk treatment group possibly reflecting lower baseline urate levels in this study's cohort, as well as early identification and management of high-risk patients through the institutional prescribing criteria.
Importantly, we did not observe a clinically meaningful dose-response relationship between 3 mg and 6 mg dosing strategies. While some studies suggest higher doses may provide greater absolute urate reduction, such findings frequently involve cohorts with higher baseline urate levels or a greater proportion of established TLS treatment cases.16,17
Surprisingly, in the high-risk treatment group, a 3 mg dose provided greater median urate reduction (0.45 mmol/L) compared to those treated with 6 mg (0.42 mmol/L). This larger reduction is despite the 6 mg group having a higher median baseline urate level (0.74 mmol/L) versus the 3 mg group (0.64 mmol/L). This finding possibly demonstrates once sufficient enzymatic activity is achieved to rapidly degrade circulating urate, additional drug exposure may not proportionally enhance biochemical response. Therefore, this reinforces the rationale for a 3 mg default strategy, with dose escalation reserved for selected high-risk or biochemically unstable patients.
Approximately 39% of patients required more than one rasburicase dose, predominately those with high disease burden and/or kidney impairment. This pattern suggests repeat dosing reflects ongoing tumour lysis burden or impaired clearance of metabolites rather than inadequate initial dosing. The comparable rates of repeat dosing between 3 mg and 6 mg doses in high-risk patients further support this interpretation.
These observations support the concept that rasburicase mitigates hyperuricaemia but does not directly modify phosphate-mediated kidney injury, which may explain persistent CTLS in susceptible patients. Thus, fixed-dose rasburicase appears biochemically robust, but its clinical impact is modulated by patient-specific disease states and renal reserve.
Clinical outcomes
The most important finding of this study is that TLS progression occurred despite effective urate control. Nearly half of the prophylaxis cohort met criteria for LTLS and 14% progressed to CTLS. This highlights an important limitation that while rasburicase effectively controls hyperuricaemia, it does not eliminate the progression to CTLS, particularly where additional metabolic disturbances are present as a result of aggressive disease or impaired kidney function.
Most CTLS cases occurred in high-risk patients (71%) and were associated with renal insufficiency, consistent with the pathophysiology of TLS and the influence of baseline kidney impairment on disease severity. 1 The majority of affected patients had moderate-grade CTLS (median grade 2) and many demonstrated renal recovery within one week, suggesting that early rasburicase use may have mitigated severity and promoted renal recovery, even where TLS developed.
The observed incidence of TLS was higher than that of previously reported rates, likely due to the higher proportion of high-risk patients in this cohort or the inclusion of a peak urate measurement recorded between rasburicase administration and 24 h.17,18 As 97% patients achieved normalisation by 24 h and rebound urate elevation was only observed in three patients, this peak measurement may have inflated the true incidence of TLS in our TLS prophylaxis patient cohort. This difference could also be due to variation in reporting TLS outcomes, as many studies focus on hyperuricaemia outcomes rather than clinical outcomes associated with TLS, making comparison challenging.
Adherence to institutional prescribing criteria
Rasburicase use was consistent with the institutional prescribing criteria in 85% of cases, reflecting that institution-led governance is a strategy that can be used to successfully influence clinical practice. Majority of use was indicated for prophylaxis in patients at intermediate- or high-risk of TLS, consistent with proactive management of TLS risk in haematological malignancies. Instances of non-compliance were infrequent and primarily reflected appropriate clinical discretion in scenarios not explicitly covered in the prescribing criteria, including emerging biochemical changes suggesting imminent TLS or the need for urgent SACT before effective prophylaxis with allopurinol could be achieved. These findings suggest that prescribers exercised appropriate clinical judgement in balancing prompt intervention against local policy constraints, likely preventing further biochemical deterioration or more severe TLS presentations.
While the prescribing criteria does not currently provide explicit criteria for treatment dosing, most treatment with rasburicase was administered to high-risk patients who would have otherwise met the defined institutional prescribing criteria indications for prophylactic use. In contrast, treatment dosing in lower-risk patients, though infrequent, represented the primary source of non-compliance and may reflect ambiguity of risk stratification within the prescribing criteria and/or cautious clinical escalation outside of formal criteria. This distinction indicates that the current prescribing criteria may not fully capture the complexity of TLS progression and supports consideration of clearer guidance for both risk stratification and treatment dosing.
The higher prescribing criteria compliance rate observed among 6 mg doses compared with 3 mg doses (94% versus 77%) further suggests that clinicians appropriately reserved higher doses for patients with clear risk, and biochemical or clinical evidence of TLS. Collectively, these findings reveal that rasburicase was used primarily within the intended population, guided by both protocol adherence and contextual clinical reasoning.
The clinical relevance of these findings extends beyond biochemical efficacy. Effective urate control remains central to preventing TLS complications. In this study, urate normalisation occurred rapidly in both prophylaxis and treatment groups, suggesting early intervention guided by the prescribing criteria successfully mitigated clinical progression. Although cost analysis was not the primary objective, the fixed-dose approach resulted in an estimated 92.5% reduction in rasburicase therapy costs within our study group compared to the TGA approved regimen, highlighting the economic sustainability of evidence-based local governance without compromising efficacy.
Limitations
Several limitations of this study must be acknowledged. The retrospective observational design limits the ability to control for confounders or assess causality. Incomplete records, while limited, may have impacted outcome analysis and TLS risk classification. The single-centre design may also limit generalisability to health services with differing governance structures or patient populations. Additionally, clinical outcomes such as progression to dialysis and mortality were not recorded, potentially underestimating the broader benefits of early rasburicase use.
Implications for practice
Despite these limitations, these findings support the use of low fixed-dose rasburicase as an effective and resource-efficient strategy for the management of TLS in patients with haematologic malignancies. A 3 mg dosing approach achieved comparable biochemical outcomes to 6 mg dosing, supporting its use as a standard initial strategy in many patients.
From a health systems perspective, simplified fixed dose rasburicase may improve access by reducing cost without compromising biochemical efficacy. At the study institution, an application is planned for rasburicase to be added to the state-wide formulary to facilitate broader access in place of directorate-only temporary prescribing criteria. With this application, it is recommended the criteria be reviewed to include treatment dosing and better-defined intermediate risk stratification. Several questions remain unanswered at present, including determining which clinical factors (e.g., bulky and/or aggressive disease, baseline urate level) cause the need for further rasburicase doses after the initial dose.
Conclusion
This study confirmed the clinical and economic validity of low fixed dosing of 3 mg or 6 mg for TLS prophylaxis in high- and intermediate-risk patients and TLS treatment, which may improve access to this medicine globally from a reduced cost burden perspective. It also demonstrated high compliance with institutional rasburicase prescribing criteria. Further research is warranted to identify predictors of TLS progression which necessitate dose escalation, additional doses, and the optimal interval between additional doses.
Footnotes
Authorship statement
Conceptualisation: MR; Research question: TM, MR; Methodology: TM, MR, VC, MW, EL, KW, JD, JT; Data collection: TM, VC, MW, EL. Analysis of data TM, MR, VC, MW, EL, KW, JD, JT; Writing (original draft): TM. Writing (reviewing and editing): TM, MR, VC, MW, EL, KW, JD, JT.
Ethical considerations
This study was granted exemption from the requirement for ethical review by the Princess Alexandra Hospital Medicines Use Evaluation Subcommittee of the Medicine Management Committee under a protocol approved by the Metro South Human Research and Ethics Committee (CM22042501).
Consent to participate
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The de-identified data that support the findings of this study are available from the corresponding author upon reasonable request.