
Abstract
Purpose
UK oncology services face increasing demand alongside workforce constraints. This study evaluated the impact of a pharmacist-led breast cancer clinic on consultant workload and clinic utilisation in a UK district general hospital.
Methods
This was a prospective service evaluation conducted over 11 months following implementation of an independent prescribing pharmacist-led breast cancer clinic. Data were collected on systemic anti-cancer therapy (SACT) prescribing, clinic overbooking rates, and pharmacist-led consultations, including requirement for consultant input.
Results
The pharmacist prescribed 420 of 3135 (13.4%) of all breast cancer systemic anti-cancer prescriptions (95% CI: 12.2%–14.6%). Pharmacist consultations were conducted independently in 81.5% (95% CI: 77.7%–85.3%) of cases, without requiring consultant input. Following implementation, clinic overbooking rates remained stable (19.6% vs 21.7%; χ2 = 1.783, p = 0.18), suggesting sustained utilisation of clinic capacity despite redistribution of patient care to pharmacist-led consultations. Requirement for medical input differed according to treatment type (χ2 = 11.8, p < 0.001), consistent with anticipated differences in treatment complexity and clinical oversight requirements.
Conclusion
The pharmacist-led breast cancer clinic absorbed a significant proportion of routine prescribing and reviews of breast cancer patients, with the majority of consultations managed independently. Broader adoption of this approach may support redistribution of workload and maintenance of clinic capacity within oncology services. Further work is required to evaluate safety outcomes and cost-effectiveness.
Keywords
Introduction
The increasing incidence of cancer, alongside workforce constraints, continues to challenge the sustainability of oncology services. 1 In the UK, breast cancer remains the most common malignancy, 2 with a growing number of patients receiving systemic anti-cancer therapy (SACT) due to advances in targeted and long-term treatment strategies. This expanding patient population, combined with increasing treatment complexity, places significant pressure on oncology consultants, contributing to clinic overbooking, delays in care, and workforce strain.
To address these pressures, alternative workforce models are being explored, including expanded roles for pharmacists. 3 In the UK, pharmacists can undertake additional training to become independent prescribers and contribute to patient management within defined governance frameworks. Previous studies have demonstrated the clinical competence of pharmacists in oncology settings4,5; however, there is limited real-world evidence evaluating their impact on consultant workload and service delivery.
This service evaluation examines the implementation of a pharmacist-led breast cancer clinic within a UK district general hospital. The primary aim was to assess the impact on consultant workload, with secondary objectives including clinic utilisation and patient experience. It was hypothesised that a pharmacist-led clinic could redistribute routine clinical activity without compromising service delivery.
Objectives
The primary objective was to evaluate pharmacist-led prescribing and consultation activity within a breast cancer clinic and its impact on consultant workload. Secondary objectives included assessment of clinic utilisation through overbooking rates and exploration of patient experience within a pharmacist-led clinic.
Methods
This was a prospective, single-site service evaluation assessing the impact of a pharmacist-led breast cancer clinic on consultant workload, clinic logistics and patient satisfaction. This project was conducted over an 11-month period between December 2023 and November 2024, in a district general hospital in the UK. Patient feedback was collected using a United Kingdom Royal Pharmaceutical Society validated tool. 6 This evaluation did not require ethical approval in accordance with NHS Health Research Authority Guidelines, as no identifiable patient data was collected.
Data collected during this period were compared with data from the 11-month period preceding pharmacist-led breast cancer clinic implementation. All data collections and analyses were performed in Microsoft Excel 365. A p-value < 0.05 was considered statistically significant.
Pharmacist-Led clinic model
A single independent prescribing pharmacist conducted weekly breast cancer clinics within established governance frameworks. The pharmacist was responsible for reviewing patients, prescribing systemic anti-cancer therapy (SACT), and escalating to medical staff where clinically appropriate.
Patients included those receiving adjuvant or palliative oral, subcutaneous, or intravenous therapies. Patient selection for pharmacist-led review was undertaken by the consultant oncology team, which may have introduced selection bias towards clinically stable or less complex cases.
Selection criteria
Inclusion criteria
Data was collected regarding all appointments seen in the pharmacist-led breast cancer clinic. Any intervention required from a medical colleague to support the NMP pharmacist was included in the data. Interventions required included: scan result interpretation, physical examination and management of complex toxicities or acutely unwell patients.
Any patient review as part of the breast cancer clinic was included. These included mid-cycle toxicity reviews, pre systemic anti-cancer therapy assessment appointments and end-of-treatment reviews.
Any systemic anti-cancer therapy for patients with breast cancer was included, irrespective of formulation such as IV or oral treatments.
Exclusion criteria
Non-breast cancer patients seen in the pharmacist-led cancer clinic.
Taking consent for systemic anticancer therapy does not form part of this analysis.
Data collection
Four data domains were captured
SACT prescribing workload: all prescriptions over the duration of this service evaluation were tracked via the local e-prescribing system. Each prescription was identified as either prescribed by a consultant or pharmacist.
Clinical overbooking: clinic slot data was collected from the trust's platform through manual counts, before and after the implementation of a pharmacist-led breast cancer clinic.
Pharmacist clinic characteristics: number of pharmacists led appointments, need for medical input, average appointment duration and reasons for escalation were recorded manually in an excel spreadsheet.
Patient satisfaction feedback (exploratory): a validated Royal Pharmaceutical Society patient feedback form was offered to all patients attending the pharmacist clinic in April 2024.
Statistical analysis
Descriptive statistics were used to summarise prescribing activity, overbooking rates and medical support frequency. All calculations were performed using Microsoft Excel.
95% confidence intervals (CIs) for proportions were calculated in excel using the standard normal approximation: CI = p ± 1.96 x √[p(1-p)/n]
Cohen's h was calculated to assess effect size between overbooking proportions pre- and post-intervention: h = 2 x [arcsin(√p1) - arcsin(√p2)], this was calculated in Excel using formula = ASIN(SQRT(B2)) and = ASIN(SQRT(B3)).
Chi-square tests were used to assess associations between treatment type and the need for medical input. A p-value < 0.05 was considered significant.
Results
Prescription workload
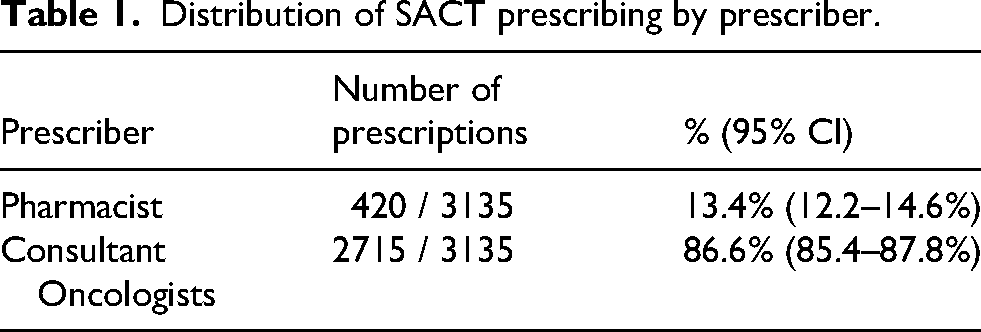
During the 11-month period, the pharmacist prescribed a total of 420 of 3135 SACT prescriptions, accounting for 13.4% of all breast cancer prescribing (95% CI: 12.2%–14.6%) (Table 1).
Distribution of SACT prescribing by prescriber.
Medical input
A total of 395 pharmacist-led consultations were conducted independently in 322 cases (81.5%, 95% CI: 77.7%–85.3%), without requiring consultant input. Escalation to consultant support occurred in 73 consultations (18.5%, 95% CI: 14.7%–22.3%).
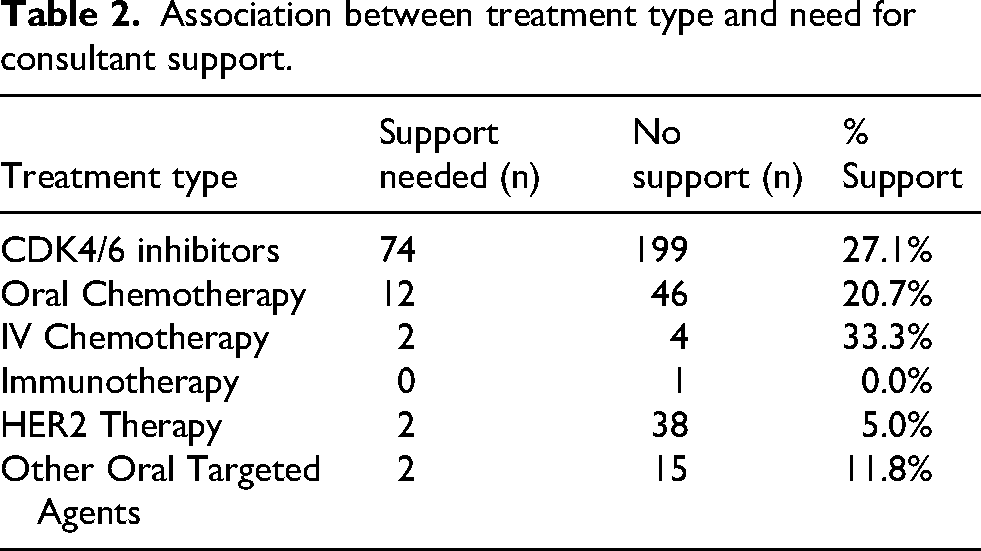
Reasons for escalation included scan interpretation, need for physical examination, management of complex toxicities, and acutely unwell patients (Table 2).
Association between treatment type and need for consultant support.
Clinic utilisation (overbooking rates)
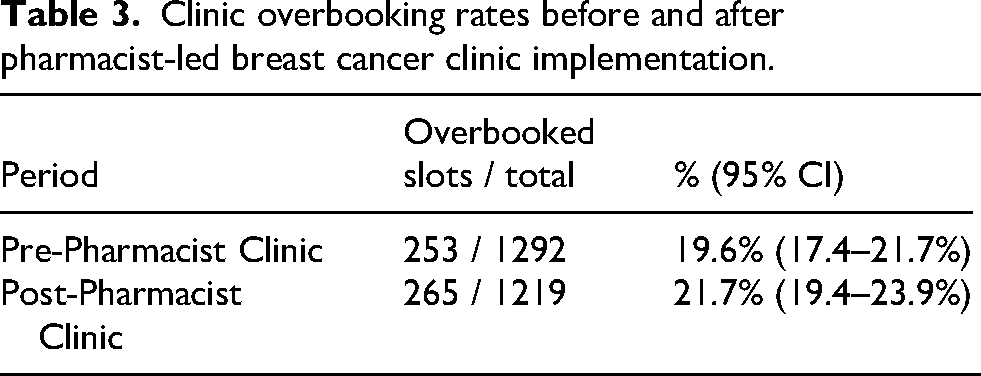
Pre-implementation overbooking rate: 253 of 1292 slots (19.6%), (95% CI: 17.4% to 21.7%) and post-implementation: 265 of 1219 slots (21.7%), (95% CI: 19.4% to 23.9%).
There was no statistically significant difference between periods (Chi-square X2 = 1.783, df = 1, p = 0.1819) with a negligible effect size (Cohen's h = 0.053) (Table 3).
Clinic overbooking rates before and after pharmacist-led breast cancer clinic implementation.
Treatment type and need for medical input
Requirement for medical input differed according to treatment type (χ2 = 11.8, df = 5, p < 0.001), consistent with anticipated differences in treatment complexity and clinical oversight requirements.
Patient feedback (exploratory)
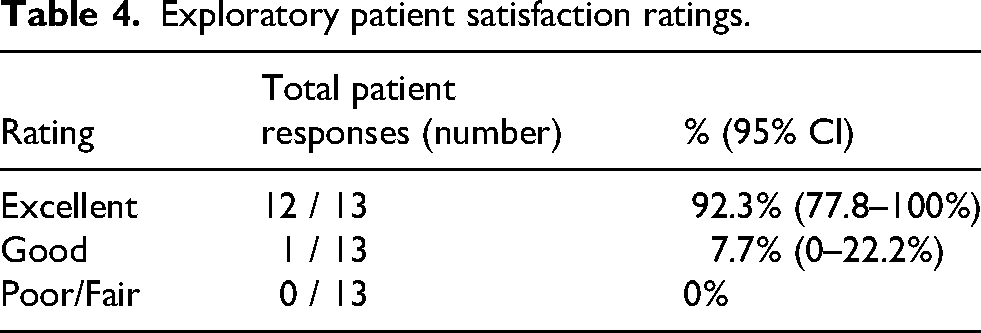
A total of 13 responses were received from 43 distributed questionnaires (30.2% response rate). Of respondents, 12 (92.3%) rated their experience as excellent.
Given the small sample size, limited collection period, and potential response bias, these findings should be interpreted as exploratory (Table 4).
Exploratory patient satisfaction ratings.
Discussion
This service evaluation demonstrates that a pharmacist-led breast cancer clinic can contribute to routine oncology service delivery, with over 80% of consultations managed independently and a measurable proportion of prescribing undertaken by the pharmacist. These findings suggest that redistribution of routine clinical activity to an independent prescribing pharmacist is feasible within a real-world NHS setting.
The high proportion of consultations not requiring consultant input highlights the potential for pharmacist-led models to reduce demand on medical staff by managing routine reviews and prescribing. This is particularly relevant in the context of increasing cancer incidence and workforce constraints.
Despite redistribution of a proportion of patient care to pharmacist-led consultations, clinic overbooking rates remained stable following implementation, suggesting sustained clinic utilisation and ongoing service demand.
The association between treatment type and need for consultant input suggests that certain therapies require greater medical involvement, likely reflecting differences in toxicity, monitoring, and complexity.
A concurrent GP-led clinic was introduced during the study period and may have contributed to clinic capacity, limiting the ability to isolate the independent effect of the pharmacist-led model.
Formal safety outcomes, including adverse events and hospitalisations, were not prospectively collected and therefore cannot be definitively assessed.
Patient feedback suggested high satisfaction among respondents; however, low response rates and potential bias limit interpretation.
Overall, these findings support the role of advanced practice pharmacists in contributing to oncology service delivery and workforce sustainability.
Future directions
Further work should aim to evaluate pharmacist-led oncology clinics across multiple centres and tumour types, using prospective study designs or matched controls to isolate their impact. Economic analyses would help establish cost-effectiveness, while patient-reported outcome measures (PROMs) could capture broader impacts on quality of care. Additionally, exploring the role of pharmacists in supporting complex regimens or managing treatment toxicities could further expand their scope and utility within cancer services.
Limitations
This study had several limitations. First, the evaluation was limited by its single-centre design and lack of patient-level clinical characteristics. Patient selection by consultants may have introduced selection bias, while the concurrent introduction of a GP-led clinic represented a potential confounder. Patient feedback findings were limited by low response rates, a short collection period, and potential response bias, meaning these findings should be interpreted as exploratory. No cost-effectiveness analysis was conducted, and formal safety outcomes were not prospectively assessed.
Conclusion
A pharmacist-led breast cancer clinic contributed to routine oncology care, with the majority of consultations managed independently and a measurable proportion of prescribing undertaken by the pharmacist. This model supports redistribution of workload within multidisciplinary teams and may help maintain service capacity in the context of increasing demand. Further work is required to evaluate safety outcomes and economic impact.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.