
Abstract
Introduction
Cancer is a growing public health crisis in Nepal, with an estimated 22,008 new cases and 14,704 deaths reported annually. 1 The risk is also rising in low- and middle-income countries (LMICs) such as Nepal, where a population-based cancer registry recorded 3295 new cases and 1427 deaths, though current figures are likely higher. 2 The majority of patients present at advanced stages, when the pain management becomes paramount, requiring the administration or consumption of opioids. Yet Nepal's per capita morphine consumption is just 0.88 mg, roughly one-seventh of the global average of 6.15 mg. 3 This limited supply is further undermined by geographic inequities as opioids remain concentrated in a handful of urban tertiary centers, while rural healthcare facilities, serving most of the population, rarely stock morphine in any formulation.
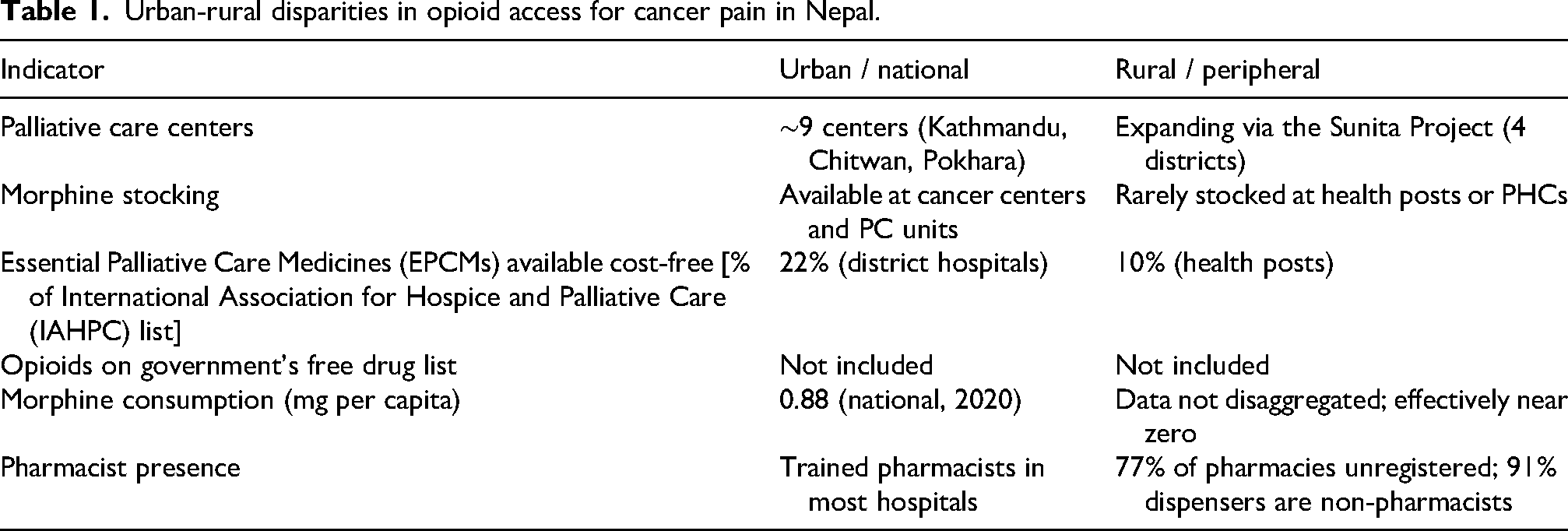
The urban-rural gap in opioid access is well-documented. Morphine and other opioids (including fentanyl and codeine) are primarily available in tertiary hospitals, cancer centers, and the few palliative care units clustered in urban areas like Kathmandu Valley, Chitwan, and Pokhara.3,4 A recent cross-sectional study found that while 22% of essential palliative care medicines (EPCMs) listed by the International Association for Hospice and Palliative Care are available free of charge at district hospitals, as such, this drops to just 10% at health posts, the primary point of care in rural Nepal. 5 This inequity is compounded by the government policy of not including opioids from both the government free drug list and the fixed-price medicine list, compelling patients to pay out-of-pocket for medicines that many cannot afford. Nepal's entire morphine supply depends on a single private manufacturer that imports raw materials from Europe, creating a supply chain that is fragile and disproportionately affects peripheral facilities. 5 These structural barriers persist despite a policy environment that permits all medical practitioners to prescribe morphine and a National Strategy for Palliative Care (2017) that envisions universal access. Table 1 summarises key urban-rural disparities in opioid access in Nepal.
Urban-rural disparities in opioid access for cancer pain in Nepal.
Out of the healthcare workforce, pharmacists represent a critical, yet largely untapped, workforce to bridge gaps in safe and accessible use of opioids. A 2022 systematic review on opioid stewardship revealed that pharmacists’ interventions, including pain assessment, dose adjustment, adverse effect monitoring, and patient education, improved prescribing quality and patient safety without worsening pain management outcomes across all evaluated settings. 6 However, all contributing studies were from high-income settings, with none from LMICs, exposing a critical evidence gap. A Nepal-specific qualitative study illustrates why this gap is critical: patients discharged with opioid prescriptions from a tertiary hospital in western Nepal had no shared follow-up plan, and knowledge of adverse effects, dependence risks, and tapering protocols was uniformly poor, highlighting the need to strengthen pharmacist-led counseling. 7 An accompanying commentary on opioid stewardship in LMICs has positioned pharmacists as holding pivotal roles in prescription monitoring, safe disposal programs, patient education, and community collaboration. 8
International precedent further supports an expanded role for pharmacy professionals. In Uganda, specially trained nurses and clinical officers were authorized to prescribe morphine since 2004, with a heavy reliance on pharmacists to ensure safe use and uninterrupted supply. 9 Adapting this task-shifting model for Nepal's pharmacy workforce, comprising over 8355 registered pharmacists and 16,977 pharmacy assistants, 10 could address rural access barriers when paired with targeted training and regulatory support. In Nepal, the Sunita Project (2022–2025), implemented by INF Nepal and EMMS International across four districts in western Nepal, demonstrated that rural palliative care models can facilitate access to essential pain-relief medicines, including opioids, for patients living outside major urban centers through linked specialist support and supervised care pathways. Together with the National Palliative Care Formulary launched in February 2025, these experiences provide a practical foundation for developing pharmacist-supported opioid services in rural health facilities. 5
The Lancet Commission on Palliative Care estimated that closing the global morphine access gap would cost approximately US$145 million, while providing an essential palliative care package that includes morphine would require only about US$3 per capita in low-income countries. 11 These estimates demonstrate that improving access to morphine is highly affordable and that the finanical resources required are modest relative to the burden of untreated pain. In Nepal, this is especially important because oral morphine is the most affordable option for chronic cancer pain, whereas fentanyl patches are substantially more expensive and often unaffordable for many patients. Addressing this affordability gap is therefore essential to ensuring equitable access to effective pain relief, particularly for patients in rural and resource-limited settings. Three steps are needed. First, the Government of Nepal should include at least oral morphine on the free essential drug list and other opioids on the health insurance formulary to remove financial barriers at the point of care. Second, pharmacist-led opioid counseling and stewardship protocols should be developed for rural health facilities, building on the evidence from the Sunita Project and emerging Nepal-specific pharmacy research. Third, pilot programs enabling pharmacists or trained health workers to dispense oral morphine in rural districts should be evaluated, drawing on Uganda's proven task-shifting model. Without deliberate action to decentralize opioid access and leverage the pharmacy workforce, cancer patients in rural Nepal will continue to suffer and die from preventable pain.
Conclusion
Cancer-related pain remains undertreated in rural Nepal, not because effective medicines are unavailable, but because structural, regulatory, and workforce barriers have prevented their equitable distribution within the country. The evidence presented here points to a convergence of opportunity: a growing pharmacy workforce, an emerging palliative care policy framework, and international models of task-shifting that have already demonstrated feasibility in comparable settings. Realizing this opportunity will require coordinated action across government, regulatory bodies, professional pharmacy associations, and civil society to integrate opioid stewardship into routine pharmacy practice and to remove the financial and logistical barriers that keep morphine out of reach for rural patients. The cost of inaction is measurable in preventable suffering; the cost of action is modest, and the path is clear.
Footnotes
Ethical approval
Not applicable. This manuscript is a commentary/perspective piece and did not involve the collection of primary human data.
Informed consent
Not applicable.
Author contributions
Sunil Shrestha: Conceptualization, Methodology, Writing—Original Draft, Writing – Review & Editing, Supervision, Project Administration.
Rajeev Shrestha: Investigation, Data Curation, Writing – Review & Editing.
Sundus Shukar: Writing – Review & Editing.
Nabin Pathak: Investigation, Data Curation, Writing – Review & Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this manuscript, the authors used artificial intelligence-assisted language tool solely for proofreading and language editing purposes. The authors reviewed and edited the output as necessary and take full responsibility for the content of the manuscript. No AI-generated scientific content, data analysis, interpretations, or conclusions were used.
Data availability statement
No new data were generated or analysed in support of this research.