
Abstract
Background
Leptomeningeal disease is a complication of advanced solid tumors, and treatment options are limited by inadequate central nervous system penetration. Intrathecal pemetrexed has emerged as an off-label therapeutic option. However, data describing its hematologic toxicity, particularly neutropenia, are limited.
Objective
To evaluate the incidence, timing, and severity of neutropenia associated with intrathecal pemetrexed and to assess differences in neutropenia risk among clinically relevant subgroups, such as concomitant osimertinib use, vitamin supplementation, and exposure to other bone marrow suppressing medications.
Methods
A retrospective analysis was conducted of adult patients who received at least one dose of intrathecal pemetrexed over a four-year period. Patient demographics, treatment characteristics, laboratory values, concomitant therapies, and history of prior craniospinal irradiation were extracted from the electronic health record. The primary outcome was incidence of neutropenia, defined as an absolute neutrophil count <1.0 × 109/L. Exploratory subgroup analyses evaluated neutropenia incidence and severity based on concomitant osimertinib therapy, vitamin supplementation status, and use of other medications with bone marrow suppressing potential.
Results
Sixteen patients who received 138 doses were included. Neutropenia occurred in approximately one-third of patients, most commonly after loading doses. Higher neutropenia incidence and earlier onset were observed in patients receiving concomitant osimertinib and those not receiving vitamin B12 and folic acid supplementation. No consistent increase in neutropenia was observed with other marrow-suppressing medications.
Conclusion
Intrathecal pemetrexed is associated with clinically meaningful neutropenia. Subgroup findings highlight the importance of vitamin supplementation, careful regimen assessment, and close hematologic monitoring to optimize safety and patient outcomes.
Introduction
Leptomeningeal disease (LMD) remains a challenging complication of advanced malignancies, particularly non–small cell lung cancer (NSCLC) and breast cancer. Therapeutic options are limited by poor central nervous system penetration of systemic agents.
Intrathecal chemotherapy allows for direct drug delivery into the cerebrospinal fluid. While methotrexate and cytarabine remain the standard, 1 intrathecal pemetrexed has emerged as an off-label option, particularly in EGFR-mutated NSCLC. Published intrathecal pemetrexed regimens vary in both dosage and frequency (see Appendix 1). A common dosing schedule used is described in the expanded Phase II trial by Fan et al., which consists of 50 mg twice weekly (load) for one week, followed by 50 mg every three weeks for four cycles, then once monthly. 2 However, overall data describing its systemic toxicities, especially hematologic effects, are limited.
Although pemetrexed is associated with myelosuppression when administered systemically, 3 the extent to which intrathecal administration contributes to cytopenias is unclear. Additionally, patients with LMD frequently receive concurrent therapies and may have prior exposure to treatments such as craniospinal irradiation (CSI), further complicating attribution.
This study evaluated the incidence of neutropenia in patients receiving IT pemetrexed and explored potential contributing factors, including concomitant therapies, vitamin supplementation, and prior CSI.
Methods
Study design and population
This retrospective study included adult patients who received ≥ 1 dose of IT pemetrexed at a single academic medical center between November 12, 2021, and October 22, 2025. The dosing schedule used was 50 mg twice weekly for one week (loading doses) followed by 50 mg approximately every three weeks. Patients also received dexamethasone 5 mg intrathecally with each IT pemetrexed dose to reduce the incidence of chemical myelitis.
Data collection
Data extracted from the electronic health record included: Demographics and disease characteristics, IT pemetrexed dosing and schedule, laboratory values (ANC, hemoglobin, platelets), concomitant therapies, vitamin B12 and folic acid supplementation, use and timing of craniospinal irradiation (CSI) relative to IT pemetrexed (Table 1).
Baseline characteristics.
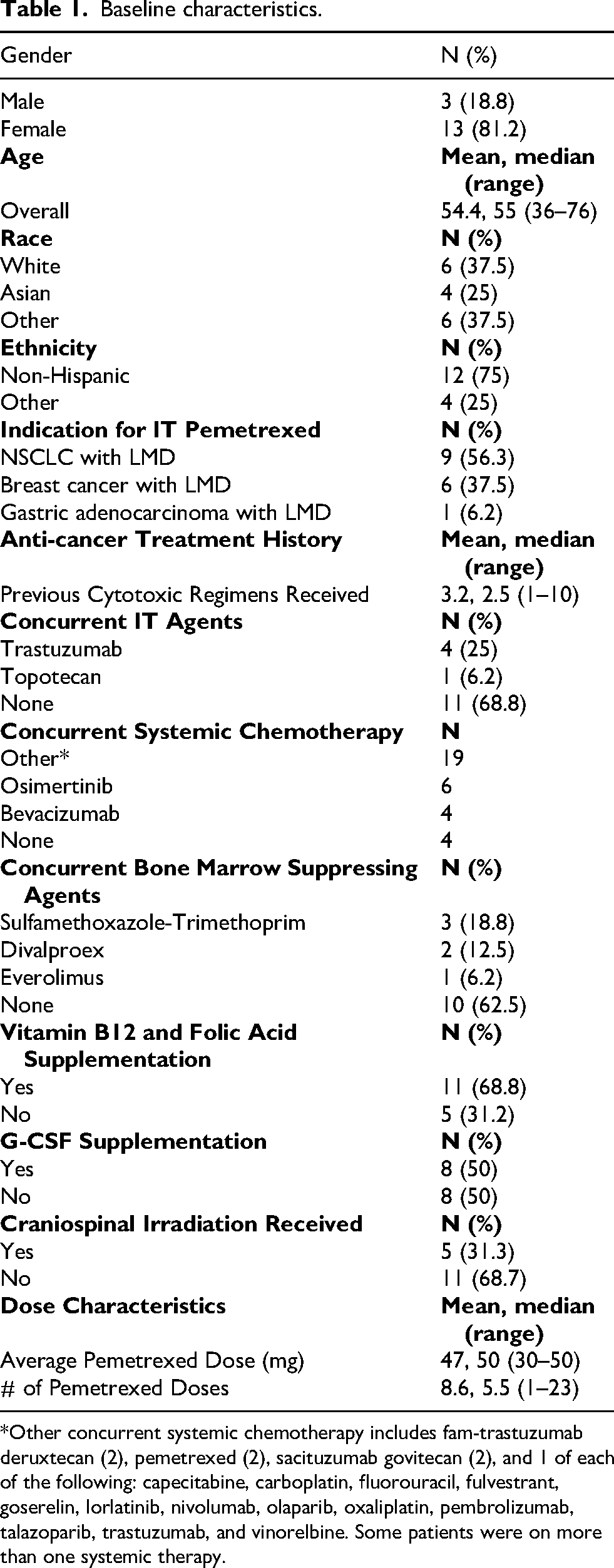
*Other concurrent systemic chemotherapy includes fam-trastuzumab deruxtecan (2), pemetrexed (2), sacituzumab govitecan (2), and 1 of each of the following: capecitabine, carboplatin, fluorouracil, fulvestrant, goserelin, lorlatinib, nivolumab, olaparib, oxaliplatin, pembrolizumab, talazoparib, trastuzumab, and vinorelbine. Some patients were on more than one systemic therapy.
Outcomes
The primary outcome was incidence of neutropenia (ANC <1.0 × 109/L). Secondary analyses evaluated timing, severity, and associations with clinical variables.
Statistical analysis
The analysis was descriptive. Subgroup comparisons were exploratory.
Results
Patient and treatment characteristics
Sixteen patients received 138 doses of IT pemetrexed. The median age was 55 years, and most patients were female (81.2%). The most common indications were NSCLC (56.3%) and breast cancer (37.5%). No patients were chemotherapy-naïve with a median of 2.5 prior lines of anti-cancer treatment.
The median number of IT pemetrexed doses was 5.5 (range, 1–23), with a median dose of 50 mg. A majority of patients (62.5%) tolerated six doses or fewer. Six patients (37.5%) received concomitant osimertinib, five (31.3%) received other concurrent IT therapy, mostly trastuzumab, and 68.8% received vitamin B12 and folic acid supplementation. Furthermore, five patients (31.3%) received craniospinal irradiation. Of these, four initiated IT pemetrexed 2 to 10 months after CSI, while one received IT pemetrexed prior to CSI.
Neutropenia
The overall incidence of neutropenia was 32.5%. Among affected patients, the mean ANC nadir was 0.53 × 109/L with a mean time to nadir of 8.3 days. Most neutropenia events occurred following initial loading doses (Table 2). Seven patients required granulocyte-colony stimulating factors (G-CSF) in response to IT pemetrexed related neutropenia. One patient received prophylactic G-CSF as part of their systemic chemotherapy regimen. Additionally, there were two patients with bone marrow involvement who both developed significant neutropenia. Given the potential for prolonged marrow suppression following CSI, prior radiation was evaluated as a contributor. However, heterogeneity in timing relative to IT pemetrexed limited interpretation.
Overall neutropenia characteristics.
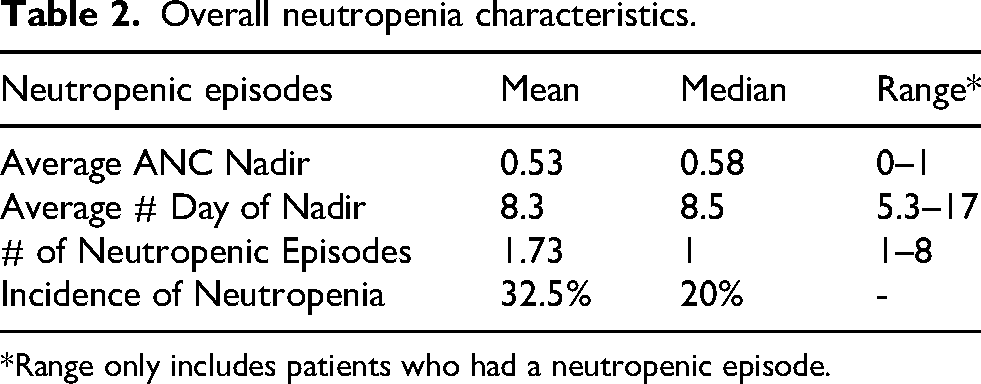
*Range only includes patients who had a neutropenic episode.
Subgroup analyses (Table 3)
Osimertinib
Neutropenia incidence was higher in patients receiving osimertinib compared with those who did not (63.3% vs 16.5%), with earlier onset and greater declines in hematologic parameters.
Subgroup analysis.
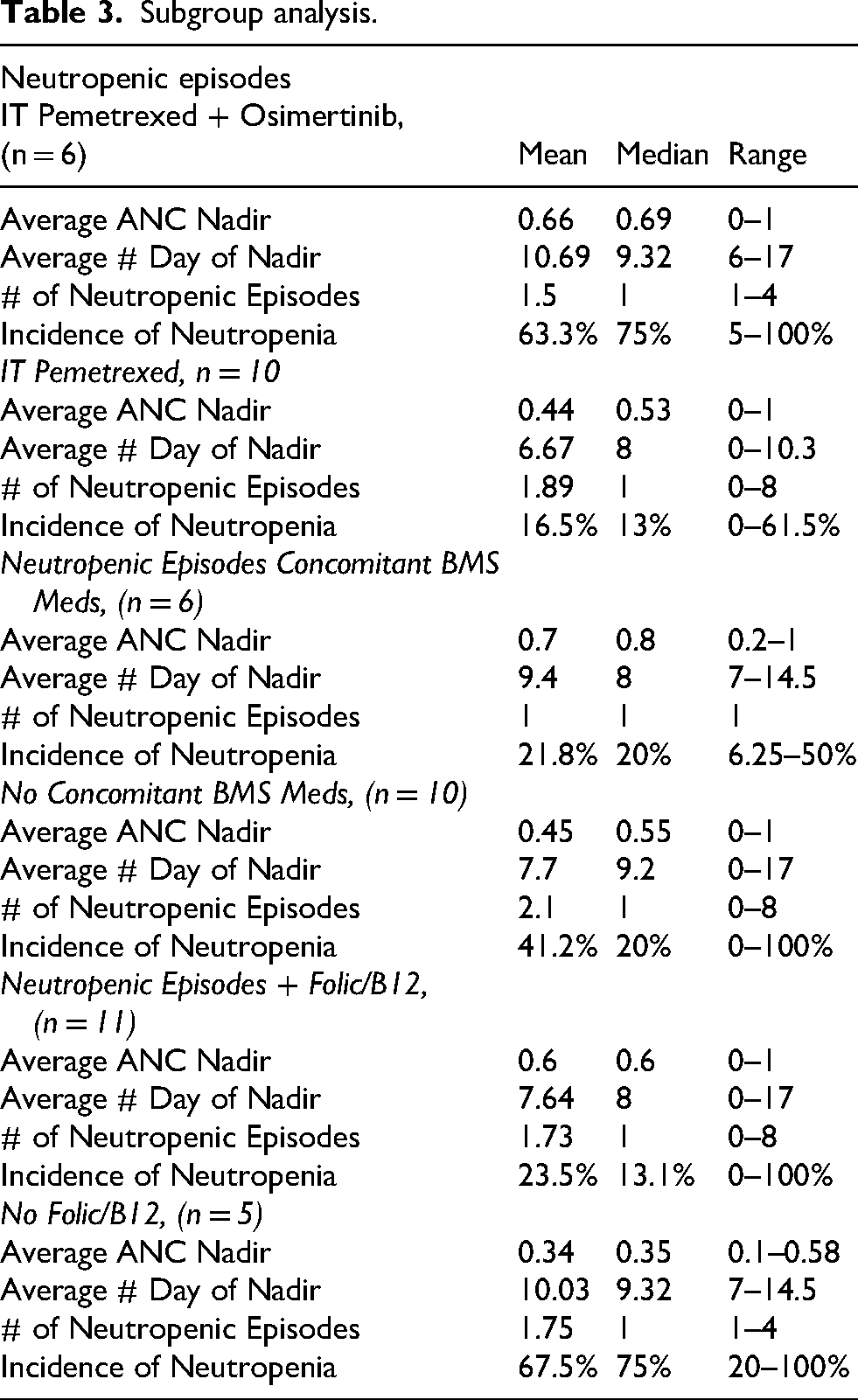
Bone marrow–suppressing medications
No consistent increase in neutropenia was observed with other marrow-suppressive agents.
Vitamin B12 and folic acid supplementation
Supplementation was associated with a lower neutropenia incidence (23.5% vs 67.5%), higher ANC nadirs, and greater treatment exposure.
Discussion
This study provides real-world data on hematologic toxicity associated with intrathecal pemetrexed. The observed neutropenia incidence (32.5%) suggests that clinically meaningful myelosuppression may occur despite intrathecal administration. Concomitant osimertinib was associated with substantially higher rates of neutropenia, raising concern for additive or synergistic myelosuppressive effects (Figure 1 and 2). This finding is notable given the relatively low incidence of severe neutropenia reported with osimertinib monotherapy. 4
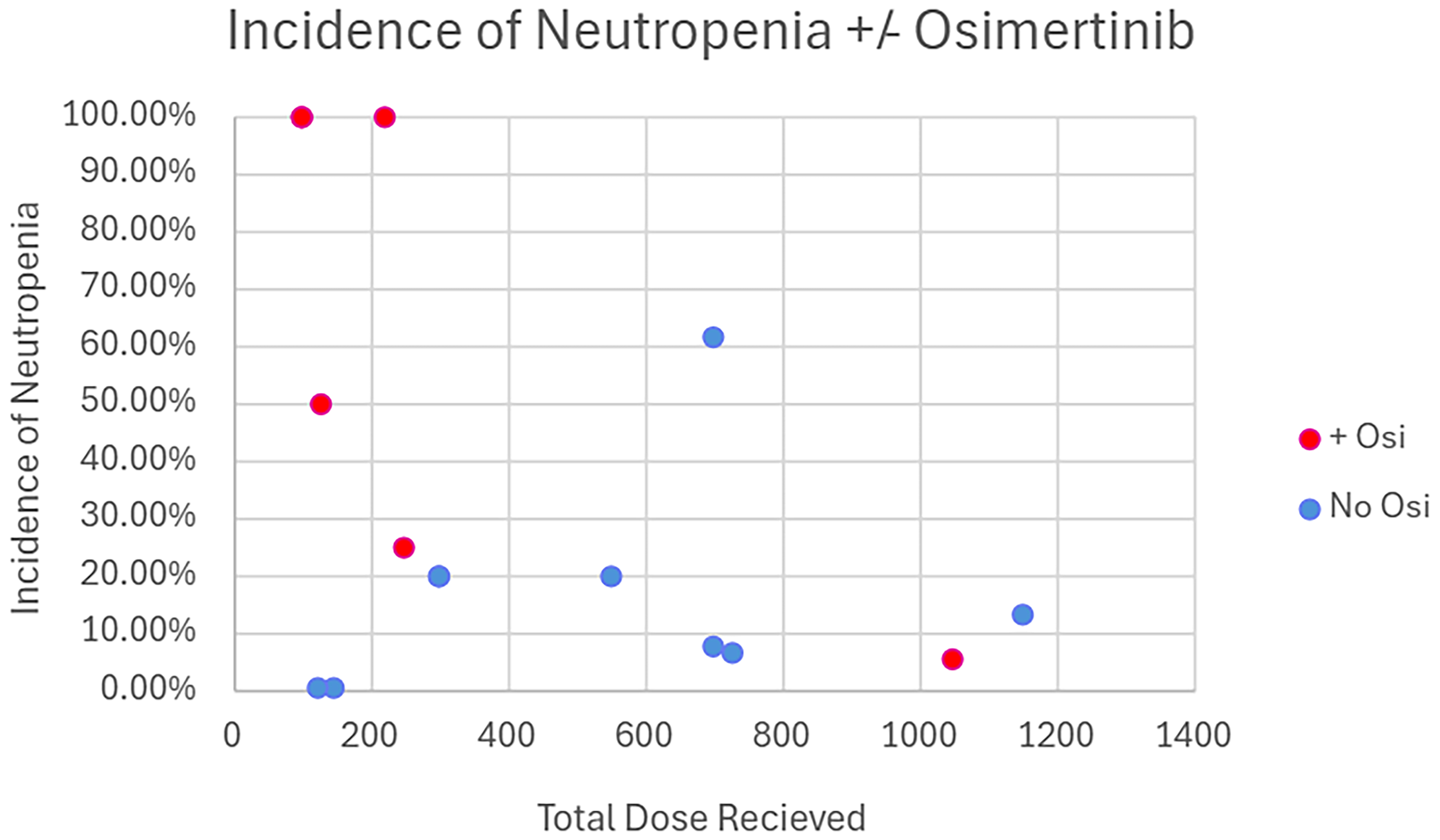
It pemetrexed ± osimertinib: incidence of neutropenia.
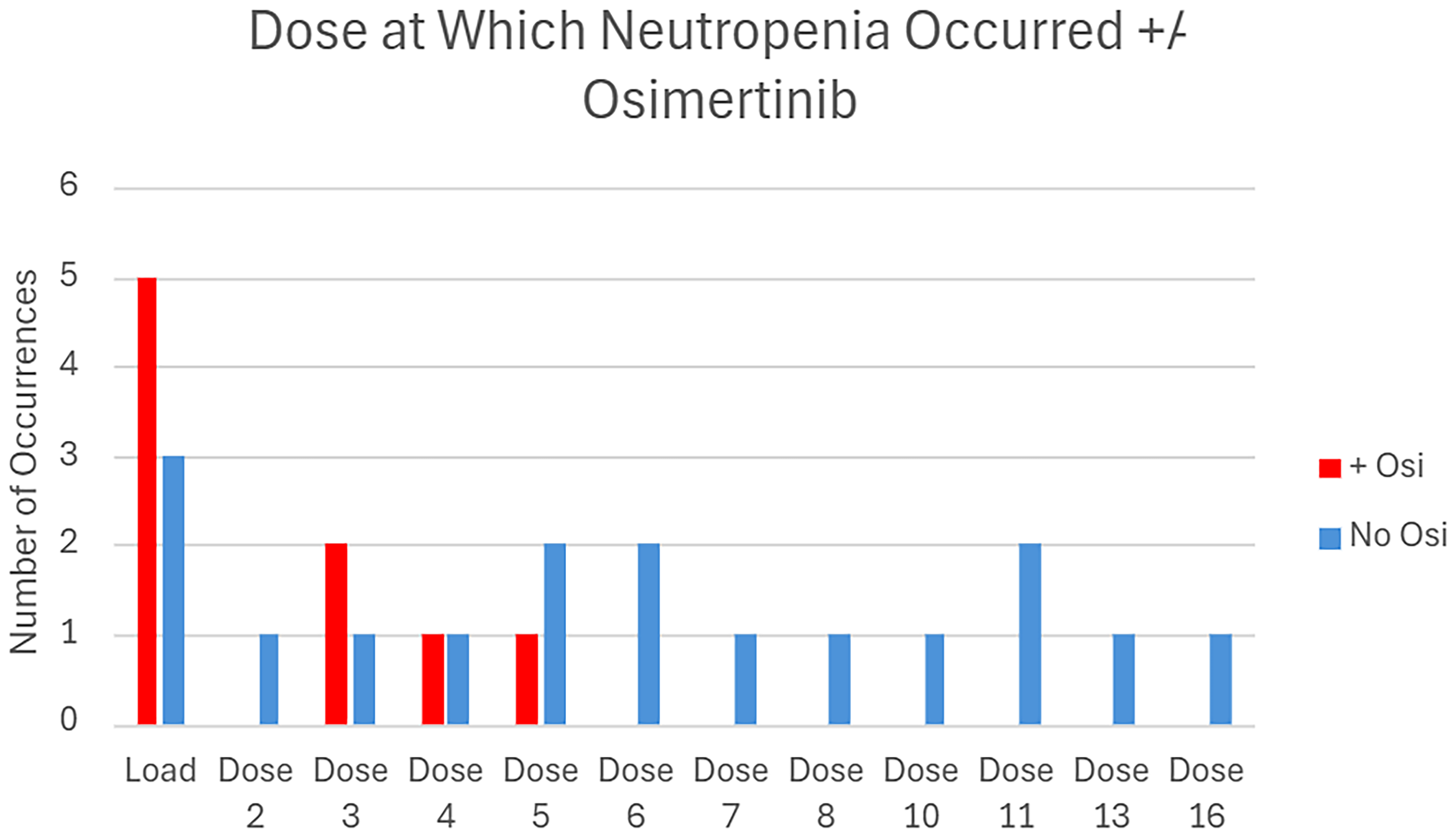
It pemetrexed ± osimertinib: dose when neutropenia occurred.
Vitamin B12 and folic acid supplementation demonstrated a protective association, consistent with established data for systemic pemetrexed. These findings reinforce the importance of adherence to supplementation protocols even in the intrathecal setting.
Craniospinal irradiation represents an additional, clinically relevant confounder. Four of five patients received IT pemetrexed within months of CSI, a period during which delayed or persistent marrow suppression may occur. While this temporal relationship suggests a potential contribution, the variability in timing and small sample size preclude definitive conclusions. Importantly, one patient received IT pemetrexed prior to CSI, supporting that neutropenia may occur independent of radiation exposure.
Unexpectedly, other marrow-suppressive medications were not associated with increased neutropenia, though this possibly reflects limited power.
Limitations
This study is limited by small sample size, retrospective design, and variability in laboratory monitoring. Multiple confounders, including concomitant therapies, limit causal inference. Additionally, prior craniospinal irradiation may have contributed to cytopenias, but its independent effect could not be isolated.
Conclusion
Intrathecal pemetrexed was associated with moderate rates of neutropenia in this cohort. Concomitant osimertinib and absence of vitamin supplementation may increase risk, while prior CSI represents an additional confounding factor. Further prospective studies are needed to better characterize hematologic toxicity and optimize supportive care strategies.
Footnotes
Acknowledgements
The corresponding author would like to acknowledge his co-authors for their expertise and guidance.
Ethical approval and informed consent statements
Ethical approval was not required.
Written consent
The study was conducted in accordance and was approved by the ACQUIRE Committee at UC San Diego Health (no. 1604), with the need for written informed consent waived.
Author contribution
NN: investigation, data curation, formal analysis, writing – original draft, visualization; AS: validation, writing – review & editing, supervision; SH: validation, writing – review & editing, supervision; DP: methodology; SP: conceptualization, methodology
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data is confidential and cannot be shared as it is from an internal database and contains patient information.
Appendix 1. Published intrathecal pemetrexed dosing regimens
Study
Dosing
Fan C, Jiang Z, Teng C, et al.: Efficacy and safety of intrathecal pemetrexed for TKI-failed leptomeningeal metastases from EGFR-positive non–small-cell lung cancer: An expanded, single-arm, phase II clinical trial. ESMO Open 9:102384, 2024
2
50 mg twice per week (day 1, 5) for 1 week, then every 3 weeks for 4 cycles, and then once monthly
Fan C, Zhao Q, Li L, et al.: Efficacy and safety of intrathecal pemetrexed combined with dexamethasone for treating tyrosine kinase inhibitor–failed leptomeningeal metastases from EGFR-mutant non–small-cell lung cancer: A prospective, open-label, single-arm phase 1/2 clinical trial. J Thorac Oncol 16:1359–1368, 2021
5
50 mg twice per week (day 1, 5) for one week, then once per 3 weeks (total, 4 weeks) then once monthly
Pan Z, Yang G, Cui J, et al.: A pilot phase 1 study of intrathecal pemetrexed for refractory leptomeningeal metastases from non–small-cell lung cancer. Front Oncol 9:838, 2019
6
10–20 mg twice weekly for 2 weeks then once weekly for 4 weeks
Li H, Zheng S, Lin Y, et al.: Safety, pharmacokinetic and clinical activity of intrathecal chemotherapy with pemetrexed via the Ommaya reservoir for leptomeningeal metastases from lung adenocarcinoma: A prospective phase I study. Clin Lung Cancer 24:e94-e104, 2023
7
30–50 mg days 1 and 8 every 3 weeks
Noronha V, Patil V, Peelay Z, et al.: Intrathecal pemetrexed in non–small-cell lung cancer patients with leptomeningeal metastasis. Ecancermedicalscience 18:1792, 2024
8
50 mg, frequency unspecified
Zhao Y, Gao X, Han Y, Wang T: The efficacy and safety of intrathecal pemetrexed for leptomeningeal metastasis from non–small-cell lung cancer: A single-arm meta-analysis of Chinese patients. Front Oncol 15:1543416, 2025
9
Meta-analysis reviewing various dosages and frequencies
Chen J, Pan L, Liu Y, et al.: Intrathecal pemetrexed administration and myelosuppression in patients with leptomeningeal metastases from lung adenocarcinoma: A retrospective study. Oncol Res 33:2107–2121, 2025
10
Induction therapy: 10 mg twice weekly for 2 weeks
Consolidation therapy: 10–30 mg, with some doses at 50 mg, administered weekly for 4 weeks
Maintenance therapy: 10–30 mg administered every 4 weeks.