
Abstract
Introduction
Pharmacokinetic monitoring of busulfan allows individualized dosing in patients, which is essential due to its high interindividual variability and narrow therapeutic range. Non-compartmental and compartmental methods are used in clinical practice to analyze busulfan exposure by area under the curve (AUC), which differ in their estimates. We aimed to compare both methods in pediatric patients and to evaluate their implications on dose recommendations.
Methods
A retrospective, observational study including 16 pediatric patients treated with busulfan as preconditioning for hematopoietic stem cell transplantation (HSCT). Trapezoidal method was used to estimate the non-compartmental AUC and the Shukla population model to estimate the compartmental AUC with NONMEM®. Statistical analysis was performed with R® software using the Wilcoxon test of paired data.
Results
No significant differences were observed in the estimation of AUC between the non-compartmental and compartmental methods, although the non-compartmental method showed greater variability and lower drug exposure, with a median of 14.985 mg/L*h vs 16.873 mg/L*h, respectively. In addition, the proportion of patients who reached the therapeutic target was similar, only 12.5% in both methods, while the majority were below it. Therefore, the dose adjustment recommendations would be similar, although quantitatively higher in non-compartmental method due to lower exposure.
Conclusions
There is good agreement between the two estimation methods. Most patients were below therapeutic target, indicating that the initial dose used is often lower than necessary and a dose increase is generally required. Bayesian models are more complex, but may provide more precise exposure estimates than the trapezoidal method.
Introduction
Busulfan is an antineoplastic agent that acts as a bifunctional DNA alkylating agent, inhibiting DNA replication and producing a potent cytotoxic effect. It is used as a conditioning treatment prior to HSCT in adult and pediatric patients, in combination with other drugs (such as cyclophosphamide, fludarabine or melphalan), for the treatment of hematologic malignancies such as leukemia, lymphoma, and myelodysplastic syndromes, as well as non-malignant conditions including inborn errors of immunity and hemoglobinopathies.1–4
Busulfan is characterized by a narrow therapeutic index, associated with low exposures leading to lack of efficacy, a higher incidence of relapses and graft rejection, and high exposures leading to toxicity of different organs, such as hepatic veno-occlusive disease, neurological toxicity (tonic-clonic seizures) and respiratory toxicity.3,5,6 In addition, it presents a high interindividual variability, especially in small pediatric patients (<9 kg) and newborns, and greater if administered orally than intravenously.4,7–10
For these reasons, the Guidelines for Conditioning for Hematopoietic Transplantation in Pediatrics, of the Spanish Group for Hematopoietic Transplantation and Cellular Therapy (GETH-TC) recommend monitoring busulfan levels in pediatric patients undergoing HSCT. 11 Currently, therapeutic drug monitoring (TDM) of busulfan is performed as part of routine clinical practice, due to the good exposure-response relationship described in several studies. This allows individualized dose adjustment after the first dose to achieve concentrations within the therapeutic range, thus optimizing efficacy and reducing toxicity, improving patient response.6,12,13
Several indices are used to determine busulfan exposure, such as estimation of AUC from concentration-time values or mean steady-state concentration (Css). Css can be estimated by dividing AUC by the dosing frequency.2,5,6,13 The European Society for Blood and Marrow Transplantation (EBMT)/European Society for Immunodeficiencies (ESID) Inborn Errors Working Party (IEWP) guidelines, as well as the GETH-TC guidelines, recommend a target AUC of 90 (85–95) mg/L*h for busulfan treatment in myeloablative conditioning and 65 (60–70) mg/L*h for reduced-intensity conditioning, for both adult and pediatric patients.1,11
AUC can be estimated by non-compartmental and compartmental methods.
Non-compartmental methods make no assumptions about the distribution of the drug in the organism and assume first-order kinetics. Thus, the AUC is calculated using trapezoids for the sampled concentration range, and for the final part of the curve from the last sample a linear regression is performed, extrapolating to the time of the next dose or to infinity in case of no further dosing.14,15
Compartmental methods based on Bayesian models assume a distribution of the drug in specific compartments in the body, other relationships describing distribution and elimination, and also consider interindividual and residual variability. For this purpose, validated population pharmacokinetic models are used, from which the individual pharmacokinetic parameters are estimated and then the AUC.13,15
Non-compartmental methods are widely used in clinical practice for busulfan dosing in pediatric patients, although with the increasing availability of precision dosing software, as well as numerous population pharmacokinetic models published for this patient group in recent years, compartmental methods are increasingly being adopted.13,15–17
For this reason, because these two methods vary in how they perform their analysis and estimates, differences in the results could affect the selection and recommendation of busulfan doses for patients. Consequently, this could have a significant clinical impact by varying patient outcomes, both in terms of efficacy and toxicity.15,16
Therefore, the main objective of this study was to compare the AUC values estimated in our population using non-compartmental versus compartmental analysis, and to evaluate the results obtained and the practical implications that the use of one or the other method may have on busulfan dosing.
Methods
A retrospective and observational study that included all pediatric patients (<18 years) treated and monitored with busulfan as a conditioning regimen prior to HSCT in a tertiary hospital from October 2022 to May 2024. No exclusion criteria were considered.
The study was submitted to and approved by the Drug Research Ethics Committee of the hospital (code 2024-0616-1; approved 21 Jun 2024). A waiver of informed consent for patients was granted due to the retrospective nature of the study. No funding was received for conducting this study.
Study variables were collected from the medical records and the electronic prescribing system for oncohematological drugs. Demographic and anthropometric variables collected were sex, age, weight, height and body mass index (BMI). In addition, clinical variables such as diagnosis, type of HSCT (autologous/allogeneic), conditioning protocol (myeloablative/reduced-intensity) and initial dose were collected, as well as pharmacokinetic variables such as plasma busulfan concentration at different times and estimated AUC with compartmental and non-compartmental methods.
Patients received intravenous busulfan administered once daily by three-hour infusion, initially dosed by body weight. Once-daily doses were derived from the European Medicines Agency recommendations for four-times-daily dosing, as described by Palmer et al.; 18 except for one patient with reduced-intensity conditioning, where dosing was according to EBMT/ESID guidelines. 1 A four-day consecutive busulfan treatment regimen was followed for myeloablative conditioning and a three-day regimen for reduced-intensity conditioning. 1
To analyze busulfan exposure, TDM was performed. Blood samples were drawn from patients after administration of the first dose at three (end of infusion), four, five and six hours after the start of infusion. This was used to estimate the AUC of the first day of treatment (AUC0−24h).
A target AUC0−24h of 21.25–23.75 mg/L*h was considered for myeloablative conditioning and 20–23.33 mg/L*h in reduced-intensity, in accordance with the aforementioned EBMT/ESID recommendations. 1 These targets correspond to the daily AUC0−24h on the first day of treatment, which is used to guide dose adjustment for subsequent days in order to achieve the recommended total course AUC targets of 90 (85–95) mg/L*h (myeloablative, 4-day regimen) and 65 (60–70) mg/L*h (reduced-intensity, 3-day regimen).
Samples were centrifuged and plasma concentrations were subsequently determined using the homogeneous nanoparticle agglutination immunoassay technique on the Architect® analyzer of the Clinical Pharmacokinetics Unit of the hospital Pharmacy Service.
Based on the plasma concentrations obtained, the AUC0−24h was estimated using the non-compartmental trapezoidal method, and this result was used to make dose adjustment recommendations for patients. Subsequently, individual pharmacokinetic parameters were estimated using the compartmental method, introducing a population pharmacokinetic model into the NONMEM® software and then the AUC0−24h was calculated for each patient as dose/clearance.
The population model used was the Shukla one-compartment model, published in 2020, which was developed in pediatric patients and young adults. 19 This model employs age, treatment day, conditioning regimen, and fat-free mass (FFM) as covariates that influence busulfan exposure. FFM was calculated using the Al-Sallami equation. 20
Categorical variables were expressed as frequency and percentage and quantitative variables as median and interquartile range (IQR).
Statistical analysis was performed using R® software. AUC0−24h data obtained by non-compartmental and compartmental methods were compared using the non-parametric Wilcoxon paired data statistical test. A p-value ≤0.05 was considered statistically significant.
To reduce potential bias, all consecutive pediatric patients treated with busulfan during the study period were included and pharmacokinetic sampling and analytical procedures were performed according to the standard clinical protocol in all cases. Because both AUC estimation methods were applied to the same patients, a paired analysis was performed. This approach reduces the influence of interindividual pharmacokinetic variability and allows a direct comparison between methods within the same subject.
Results
A total of 16 patients treated with busulfan were included in the study, and no patients were excluded. Their demographic, anthropometric and clinical data are described in Table 1.
Characteristics of patients treated with busulfan (n = 16).
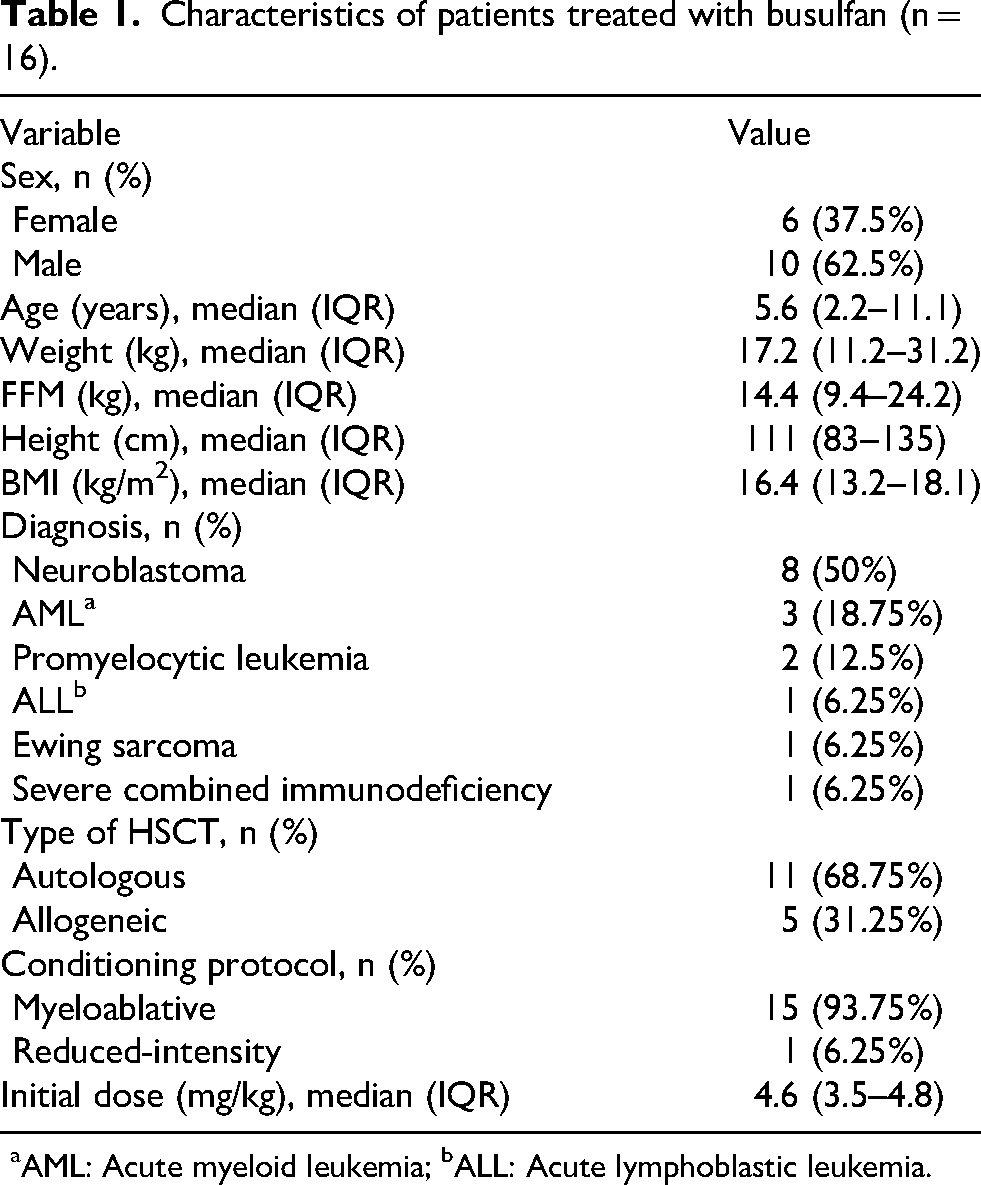
aAML: Acute myeloid leukemia; bALL: Acute lymphoblastic leukemia.
Patient age ranged from 0.6 to 15.5 years. 15 patients received myeloablative conditioning and one patient reduced-intensity conditioning. Busulfan treatment lasted four days for myeloablative conditioning and three days for reduced-intensity conditioning.
Table 2 shows the AUC0−24h values for each patient estimated by non-compartmental and compartmental methods, from busulfan plasma concentrations obtained at the sampling times of the first day of treatment. No missing data were present for any of the variables used in the analysis.
Estimated AUC0−24h values by non-compartmental and compartmental methods.
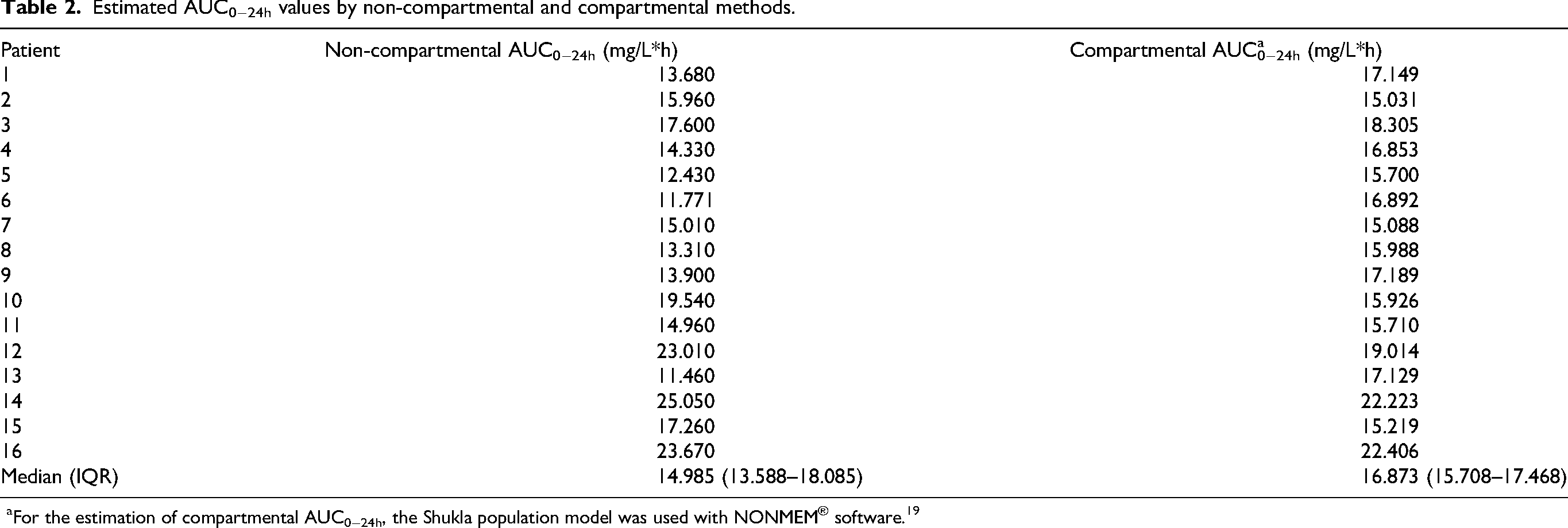
For the estimation of compartmental AUC0−24h, the Shukla population model was used with NONMEM® software. 19
The distribution of the data obtained by both methods can be observed in the box plots in Figure 1. The non-compartmental method showed a greater dispersion of the data, with a greater range, from values lower than 12 mg/L*h to higher than 24 mg/L*h, and a higher IQR compared to the compartmental method (13.588–18.085 mg/L*h vs 15.708–17.468 mg/L*h, respectively). On the other hand, the compartmental method showed a lower variability of values, which were distributed around the median, except for two outliers with a higher value. The median obtained by the non-compartmental method was lower than with the compartmental method (14.985 mg/L*h vs 16.873 mg/L*h, respectively).
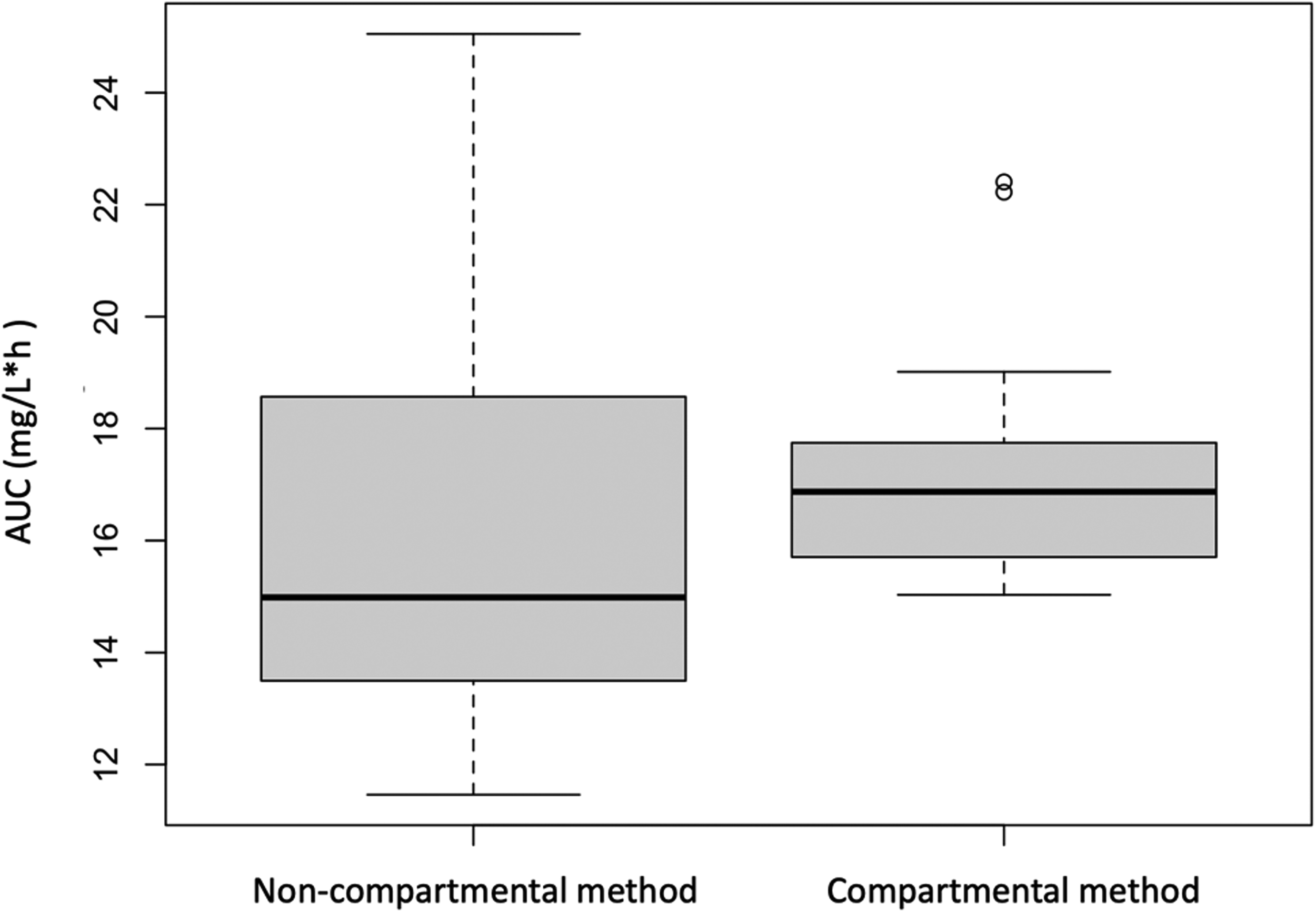
Distribution of AUC0−24h values estimated by non-compartmental and compartmental methods.
Given the small sample size (n = 16) and the skewness observed (mainly in the box plot of the non-compartmental method), a non-parametric statistical approach was used.
Therefore, to compare the AUC0−24h results estimated by both methods, the non-parametric Wilcoxon paired data statistical test was performed. A p-value of 0.4037 indicated that no statistically significant differences were observed in the estimation of AUC0−24h between the trapezoidal non-compartmental method and the compartmental method using the Shukla model.
Subsequently, the relationship between the estimated AUC0−24h results and the AUC0−24h target therapeutic range was analyzed. Table 3 shows the number of patients reaching the target interval with each AUC estimation method, as well as those below or above it, taking into account that the target is different depending on whether the conditioning is myeloablative or reduced-intensity. The results were quite similar, reaching the target AUC0−24h on the first day of treatment in only two patients (12.5%) with both methods, while most of them were below it, 13 patients with the non-compartmental method and 14 with the compartmental method, except for one patient with the non-compartmental method who exceeded it.
Distribution of estimated AUC0−24h values of patients with respect to the target therapeutic range.
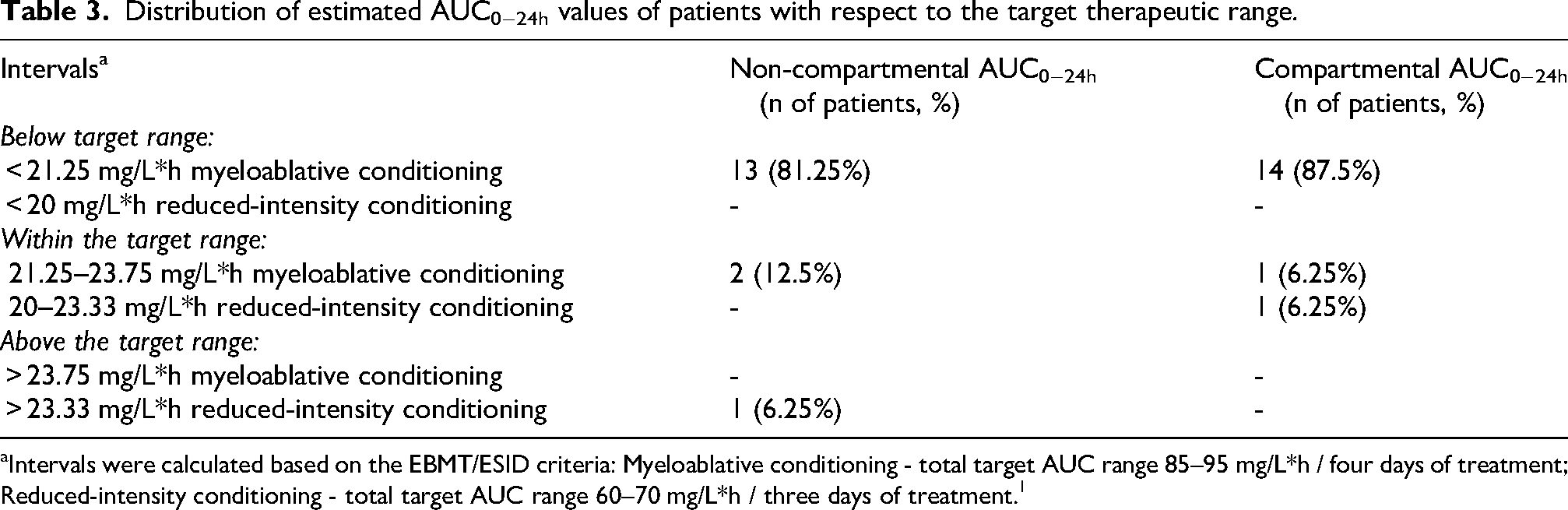
Intervals were calculated based on the EBMT/ESID criteria: Myeloablative conditioning - total target AUC range 85–95 mg/L*h / four days of treatment; Reduced-intensity conditioning - total target AUC range 60–70 mg/L*h / three days of treatment. 1
These results are shown in Figure 2, which shows the values graphically represented with respect to the target range of AUC0−24h according to the type of conditioning, with both estimation methods.
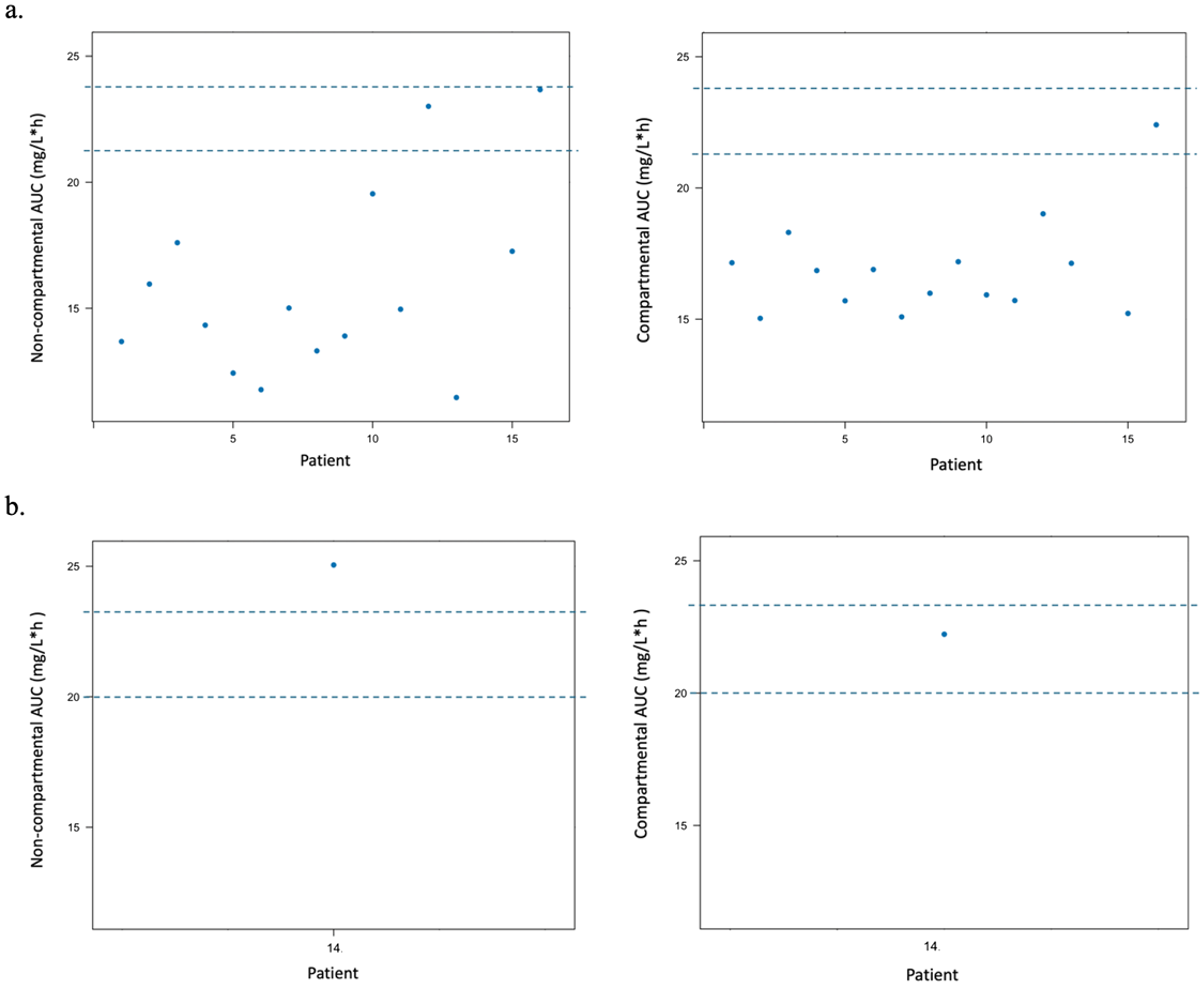
Scatter plots showing the target therapeutic range according to type of conditioning, a) Myeloablative conditioning b) Reduced-intensity conditioning. Each point represents the estimated AUC0−24h of each patient, both by the non-compartmental method (left) and by the compartmental method (right).
The estimated AUC0−24h/target AUC0−24h ratio was calculated for each patient and a median of 0.666 (0.604–0.804) was obtained for the non-compartmental method and 0.750 (0.698–0.776) for the compartmental method. Since values closer to 1 indicate closer agreement with the target AUC0–24h, this indicates that the results obtained with the compartmental method were generally closer to the therapeutic target than those obtained with the non-compartmental method.
Discussion
Non-compartmental and compartmental methods are currently being used in clinical practice to estimate the AUC of busulfan, but it is not established which method is the most appropriate and best fits the real data. This leads to variability in the results that may have a significant impact on drug dosing in clinical practice and therefore on patient response.
The population model used to estimate the AUC compartmentally in our sample was the Shukla model. 19 This model was chosen because it employs four covariates that affect busulfan pharmacokinetics (specifically clearance (CL)), which as mentioned above are age, treatment day, conditioning regimen and FFM. In turn, FFM is calculated from the sex, age, weight, and BMI of patients. 20 By taking all these factors into account, it was considered a model that could better fit the characteristics of each patient and predict AUC, compared to other published models that used only one or two covariates, mainly body weight and/or age. 13
Numerous studies have shown that different factors can influence busulfan CL such as age, day of treatment, GSTA1 genotype, BMI, body surface area, FFM or liver function, among others, so it is important to take them into account in individualized busulfan dosing, as this may help to achieve better clinical objectives.13,19,21
Due to the high interindividual variability of busulfan in pediatric patients, the narrow therapeutic index, and the good exposure-response relationship described, it is important to perform TDM in order to improve drug exposure.
In our cohort, the non-compartmental method tended to produce slightly lower AUC estimates and greater variability than the compartmental approach. However, no significant differences were observed between the two methods, suggesting that both methods provide similar estimates in terms of drug exposure, so using either method would be appropriate and would not result in significant differences in results.
Furthermore, with respect to the target therapeutic range of AUC0−24h, with both methods it was achieved in only 12.5% of patients, while the majority were below it, 81.25% with the non-compartmental method and 87.5% with the compartmental method, except for 6.25% with the non-compartmental method, who exceeded it. This suggests that, in general, the initial dose used on the first day of treatment is lower than necessary and results in underexposure to the drug, which could lead to a risk of relapse and graft failure. However, it should be noted that this underexposure refers specifically to the AUC0−24h on the first day of treatment. Since dose adjustments are made for subsequent treatment days based on TDM results, under- or overexposure on day 1 is corrected, being compensated across the full treatment course. For this reason, TDM is essential to optimize busulfan dosing on subsequent days of treatment.
On the other hand, the median estimated AUC0−24h/target AUC0−24h ratio was lower with the non-compartmental method than with the compartmental method, indicating that using the former to estimate AUC0−24h results in lower busulfan exposure. Therefore, the compartmental method led to a greater achievement of the therapeutic target in terms of AUC, although in terms of the number of patients reaching it, the result was similar.
The study by Shukla et al. 19 also showed a median estimated AUC/target AUC closer to one with the compartmental method, i.e., greater target attainment with the use of the compartmental versus non-compartmental method, as well as a higher number of patients achieving the target, however, it should be noted that in this case the initial doses were different depending on the method used. Patients who were outside the therapeutic range had mainly subtherapeutic exposure as well.
Based on the estimated AUC0−24h on the first day of treatment, a dose adjustment is made to achieve an AUC throughout treatment of 90 mg/L*h in myeloablative conditioning and 65 mg/L*h in reduced-intensity.
In patients who are within the therapeutic range, the same dose would be maintained for the second day of treatment, while for those who are below it, the dose would be increased proportional to AUC, and in those who exceed it, it would be necessary to reduce it to avoid toxicity.
In our sample of patients, recommendations for both methods would be similar: the same dose would be maintained in two patients, and in the non-compartmental method the dose would be increased in thirteen patients and reduced in one, while in the compartmental method it would be increased in fourteen patients. However, there would be differences in the proportion of dose increase between both methods, since in general, given that with the compartmental method results are closer to the therapeutic objective, the dose increase would be lower than with the non-compartmental method.
Our results are consistent with those described by Hughes et al. in whose study non-compartmental method also estimated lower exposures than compartmental methods, with the main difference being in the estimation of AUC during infusion. 15 The mean AUC estimated after the first dose by the non-compartmental method was 17.6 mg/L*h, whereas with the Shukla one-compartment model it was 18.3 mg/L*h, 19 compared to an actual mean AUC of 19.7 mg/L*h (considered from McCune bicompartmental model). 2 Similar results were described in other studies, with lower estimated AUC for the non-compartmental than the compartmental method.16,22 Notably, a recent study by Kawedia et al. using a new immunoassay based method and standard liquid chromatography coupled mass spectrometry based method, reported that non-compartmental AUC estimates were slightly higher than one-compartmental AUC estimates. However, despite these variations, the overall agreement between the two methods remains acceptable, and both approaches provide clinically comparable estimates of busulfan exposure in different populations and contexts, regardless of the method used. 23
As we have mentioned, some studies have shown that busulfan CL may decrease over time during treatment.10,13,15 The Shukla population model takes this factor into account when estimating clearance, incorporating the day of treatment as a covariate; however, the non-compartmental method does not consider this. Therefore, caution should be taken when increasing the dose on subsequent days, especially when using the non-compartmental method, since a reduction in CL could lead to a risk of overdose and too high exposure. In addition, according to our results, by obtaining lower exposure with this method, the dose increase would be higher to achieve the therapeutic objective, which could contribute to an increased risk of overdosing.
It is therefore essential to perform busulfan TDM again on subsequent days and analyze drug exposure, to verify whether the therapeutic target is reached or whether further dose adjustments are necessary during the rest of the treatment. 10 In addition, it would be interesting to conduct long-term studies to assess the response and toxicity of our patients according to the total AUC achieved and the estimation method used.
Therefore, the estimation of AUC using Bayesian models is more complex, but at the same time offers greater individualization and precision in estimates than the non-compartmental method, as it considers patient covariates that significantly affect busulfan pharmacokinetics. Nevertheless, the non-compartmental method remains an important tool for estimating drug exposure, due to its simplicity and wide applicability, as it allows dosing in patients who do not fit a specific population model or when a model is required that is not available. Thus, having both methods available allows using the most appropriate one at any given time, although it would be convenient to standardize the method between centers for better comparison of the results, which would help to optimize dosing strategies in patients.15,16,19
The main limitation of our study is that the sample size is small, so further studies with a larger population would be needed to confirm our results. Furthermore, compared to the Shukla compartmental model used, there are many other published models in which the results could be different due to the incorporation of other covariates that influence busulfan pharmacokinetics differently.13,19 Overall, these limitations may introduce some uncertainty in the magnitude of differences between non-compartmental and compartmental methods, but the direction of the bias is likely minimal since both methods were applied to the same, reducing interindividual variability.
The generalizability of our findings is limited by the single-center design and the small sample size, which may not be representative of all pediatric patients undergoing hematopoietic stem cell transplantation in other settings. Therefore, caution should be exercised when extrapolating these results to broader pediatric populations or to centers using different dosing protocols or population models. Furthermore, clinical outcome data (toxicity and treatment response) were not systematically collected in this study due to its retrospective nature, the heterogeneity of diagnoses among the 16 patients included and the analysis of the AUC on the first day of treatment rather than the entire treatment, which precluded robust conclusions about the clinical impact of AUC variability between methods. Future prospective studies with larger cohorts, longer follow-up, and systematic toxicity and response monitoring are needed to fully assess the clinical significance of differences in AUC estimation methods.
In conclusion, in our patient sample, no significant differences were observed in the estimation of AUC0-24 h between the non-compartmental trapezoidal method and the compartmental method using the Shukla model, although greater variability and lower drug exposure were obtained with the non-compartmental model. Furthermore, similar results were obtained regarding the distribution of patients who reached the therapeutic target, with most of them below it using both methods, indicating that the dose used on the first day is generally lower than necessary, making it essential to adjust and monitor busulfan in subsequent days.
Both methods are valid for estimating AUC, however, the Bayesian models are more complex but may provide more precise exposure estimates than the trapezoidal method because they take into account patient covariates that are not considered in the non-compartmental method. Furthermore, regardless of the method used, the study demonstrates the importance of TDM in clinical practice for busulfan, as it allows for individual optimization of treatment, thus improving patient response.
Footnotes
ORCID iDs
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Drug Research Ethics Committee of Hospital Universitari i Politècnic La Fe (code 2024-0616-1; approved 21 Jun 2024).
Consent to participate
Informed consent waiver of patients was granted due to the retrospective nature of the study.
Consent for publication
Not applicable
Author contributions
SGC and MRMM contributed to the study conception and design; SGC and MRMM contributed to the data collection and analysis and wrote the paper; CFS, PEC, VBR, JGP and JLPA reviewed the manuscript and contributed to the editing and validation of the final draft. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data generated and analyzed during the study are available in the corresponding tables and figures of the article.