
Abstract
Objective
To evaluate current pharmacotherapeutic strategies for H3 K27M-mutant diffuse midline glioma (DMG), with emphasis on the clinical evidence for dordaviprone, its place in therapy, and its implications for oncology practice.
Study Selection and Data Extraction
A structured literature search was conducted using PubMed and ClinicalTrials.gov through November 1, 2025. The search terms “(ONC201 OR dordaviprone) AND (‘diffuse midline glioma’ OR DMG OR H3 K27 M OR H3K27-altered)” were applied using Boolean operators. Clinical trials, cohort studies, case reports, and relevant preclinical studies evaluating pharmacologic therapies in H3 K27 M DMG were included, with emphasis on clinical outcomes and safety. The review was informed by PRISMA principles and conducted as a narrative review given the limited evidence base. A full systematic review was not possible given the limited and heterogeneous evidence base.
Results
Dordaviprone received accelerated FDA approval based on the results of an integrative analysis of five phase 1 and 2 trials. The primary endpoint of overall response rate (ORR) was 20%, disease control rate 40%, and median duration of response (DOR) was 11.2 months. Fatigue, headache, vomiting, and nausea are the most common adverse effects.
Discussion
Dordaviprone is the only FDA approved medication for H3 K27 M DMG. It demonstrates long-lasting radiographic and symptomatic improvement. It is currently approved for recurrence following prior therapy, not as a substitute for radiation or surgery. The ACTION trial may provide guidance on its broader use in newly diagnosed H3 K27 M DMG. Pharmacists play a role in optimizing treatment, monitoring safety and drug interactions, and supporting patient adherence.
Conclusion
Dordaviprone is a novel treatment option with modest response rates and durable benefit in recurrent/progressive H3 K27 M DMG. Ongoing trials may further define its role in earlier lines of therapy.
Keywords
Introduction
H3 K27 M diffuse midline glioma (DMG) is an aggressive primary brain malignancy with limited therapeutic options and a poor prognosis, with reported 5-year survival rates of less than 1% despite standard-of-care treatment including radiation, chemotherapy, and, when feasible, surgical intervention. 1 The midline location of these tumors often precludes complete surgical resection, necessitating reliance on systemic and supportive pharmacologic therapies. However, treatment efficacy remains limited, in part due to the frequent absence of MGMT promoter methylation, which is associated with reduced responsiveness to alkylating agents such as temozolomide. 2
Diffuse midline gliomas are molecularly defined by the H3 K27 M mutation, characterized by substitution of a lysine residue with methionine in histone H3, leading to epigenetic dysregulation of chromatin structure and gene expression. These molecular and anatomic features may contribute to the aggressive clinical behavior, therapeutic resistance, and poor outcomes associated with the H3 K27 M genotype. They are a distinct subset of high-grade gliomas with especially poor outcomes and virtually no proven treatment options beyond radiation.
Dordaviprone is a novel small-molecule agent with a dual mechanism of action as an allosteric agonist of caseinolytic mitochondrial protease P (ClpP) and an antagonist of dopamine D2/D3 receptors. In August 2025, it received accelerated approval from the U.S. Food and Drug Administration for the treatment of H3 K27 M DMG in patients with disease progression following prior therapy. 3 This approval, based on objective response rate and duration of response observed in early-phase studies, represents the first targeted pharmacologic option for this disease and introduces new considerations for oncology pharmacists in medication selection, monitoring, and management of drug interactions. Dordaviprone is the only medication FDA-approved for H3 K27 M DMG and represents a novel, small molecule inhibitor in this rare disease.
The purpose of this review is to carefully define dordaviprone's role in oncology pharmacy practice. The review synthesizes current evidence on dordaviprone in H3 K27 M DMG to report clinical data, critically appraise its studies, and describe its clinical place in therapy. It also aims to discuss supportive care in DMG and where symptomatic treatment is used in relation to dordaviprone. Additionally, it describes a number of disease-altering drug interactions that are relevant to pharmacists and medicine teams monitoring patients on dordaviprone.
Methods
Search strategy
A structured literature search was conducted using PubMed and ClinicalTrials.gov to identify relevant studies published through November 1, 2025. This review was conducted as a narrative review informed by systematic principles 4 selected to balance the limited evidence base with transparency of methodology.
The primary search string “(ONC201 OR dordaviprone) AND (“diffuse midline glioma” OR DMG OR H3 K27 M OR H3K27-altered)” was entered into PubMed using Boolean operators and returned 53 results. One integrated analysis of five phase 1 and 2 studies 5 was identified as the primary source of clinical efficacy data for dordaviprone and served as the foundation for evaluating therapeutic outcomes. The FDA approval press release 6 and the dordaviprone package insert 3 were retrieved directly to identify labeled indications, accelerated approval conditions, and adverse effect data. A secondary PubMed search filtering for randomized controlled trials of “dordaviprone” returned 3 results: the ACTION trial design paper, 7 and two phase 1 pharmacokinetic studies,8,9 all of which are referenced in this review.
ClinicalTrials.gov was searched using “diffuse midline glioma” and “diffuse midline glioma H3 K27M” through November 1, 2025, returning 7 trials. Six were excluded because they were withdrawn, focused on DIPG, or used radiation as the sole primary intervention. The remaining trial evaluating GD2 CAR T-cell therapy is discussed as an emerging investigational therapy. A separate ClinicalTrials.gov search for “dordaviprone” or “ONC201” returned 9 results; the ACTION trial (NCT05580562) was identified in both searches, 3 trials (NCT02525692, NCT03416530, NCT03295396) were closed to defer enrollment to the ACTION trial, and the remainder studied dordaviprone in cancer types outside H3 K27 M DMG.
Additional searches in PubMed using “pentoxifylline radiation necrosis” (51 results) and “bevacizumab glioma” (87 results) were performed to identify supportive care evidence. Primary studies referenced within included clinical trials were also screened for relevance.
Inclusion and exclusion criteria
Studies were included if they: (1) enrolled patients with H3 K27M-altered diffuse midline glioma, (2) evaluated a pharmacologic intervention, and (3) reported clinically relevant outcomes such as overall survival (OS), progression-free survival (PFS), ORR, or functional measures including Karnofsky or Lansky performance scores. Priority was given to prospective clinical trials, particularly phase 1–3 studies evaluating dordaviprone. Studies focusing exclusively on DIPG, spinal cord tumors, or non-midline gliomas were excluded unless findings were considered directly translatable. For supportive care interventions, cohort studies, randomized controlled trials, and retrospective analyses with clinical overlap to H3 K27 M DMG were included. Investigational therapies are discussed narratively based on early-phase clinical and preclinical data; these were not subject to the same evidence threshold as the primary analysis of dordaviprone.
Limitations of the review
This review is limited by the scarcity of high-quality randomized controlled trials in H3 K27 M DMG, particularly for recurrent disease. The available evidence for dordaviprone is derived from early-phase, single-arm studies and a small integrated analysis. Reliance on surrogate endpoints such as radiographic response assessed by RANO criteria may limit interpretation of long-term clinical benefit. The narrative approach to investigational therapies introduces inherent selection bias in source selection. Ongoing studies, including the phase 3 ACTION trial, are expected to substantially expand the evidence base.
Results
Dordaviprone clinical evidence
Dordaviprone received accelerated approval based on an integrated analysis of 50 patients with recurrent H3 K27 M diffuse midline glioma from two phase 2 clinical studies (29 & 10 patients), an expanded access program (8 patients), a Phase 1 study (2 patients) and one patient who received drug through compassionate use approval.5,6 The median age of patients was 30 years, with the majority between 8 and 40 years of age. All patients had a Karnofsky or Lansky performance score of at least 60 and were required to have stable or decreasing corticosteroid use at baseline. Tumors were most commonly located in the thalamus, and most patients were enrolled following their first recurrence. Efficacy outcomes were assessed using Response Assessment in Neuro-Oncology (RANO) criteria. 10 The objective response rate (ORR) was 20%, with a disease control rate (DCR) of 40%. The median duration of response (DOR) was 11.2 months, and the median time to response was 8.3 months. When response was evaluated using either high- or low-grade RANO criteria, the ORR increased to 30% and the disease control rate to 44%. Symptomatic outcomes were also reported, including a corticosteroid response rate of 46.7%, defined as a reduction in corticosteroid use with stable or improved performance status. Improvement in performance scores was observed in 20.6% of evaluable patients, with a median time to response of 3.5 months. Survival outcomes demonstrated a median overall survival of 13.7 months, with 12- and 24-month overall survival rates of 57.3% and 34.7%, respectively. Progression-free survival at 6 months was 35.1%. The safety profile of dordaviprone was characterized primarily by fatigue, headache, nausea, vomiting, and musculoskeletal pain. Grade 3 or 4 laboratory abnormalities included lymphopenia, hypocalcemia, and elevated alanine aminotransferase. Reported serious adverse events included hydrocephalus, brain edema, encephalopathy, and pulmonary embolism.
Critical appraisal of integrative analysis
A major strength of this analysis was the rigorous selection of clinical studies to include. With the help of the United States Food and Drug Administration, the study leaders developed pre-specified inclusion criteria to achieve meaningful safety and efficacy data. The patients in this study were assessed using Blinded Independent Central Review (BICR) with objective response rate according to Response Assessment in Neuro-Oncology-HGG (RANO-HGG) criteria as a primary end point. A primary critique of this study used for approval by the FDA is there is no Phase III data. There is no way to quantify true survival benefit from this study. Based on the rare nature of this glioma subset, the population size for this study was small relative to other oncology trials. The study also included primarily young adult patients vs pediatric patients due to exclusion criteria (e.g., DIPG) and higher availability of studies in young adults. One subtle but potentially important consideration with the study's population is the predominance of immunohistochemistry (IHC) classification of H3 K27 M mutations. IHC does not discriminate between H3.3 or H3.1 genotypes which may be associated with relevant overall survival differences. There were considerable differences in time to imaging. Nearly all of the patients in this analysis had previously received temozolomide. Bevacizumab use is an additional confounder. The bevacizumab washout requirement was 42 days for inclusion, however, it could reasonably confound imaging-based results (PFS, response rate) by lowering peritumoral edema longer than 42 days. Other confounders could have been dopamine receptor antagonists (eg. olanzapine) used as supportive care for nausea.
Ongoing clinical trial
The ACTION trial is an ongoing phase 3 randomized, double-blind, multicenter study evaluating dordaviprone in patients with newly diagnosed H3 K27 M diffuse midline glioma. 7 Following completion of radiation therapy, patients are randomized to receive placebo, once-weekly dordaviprone, or a twice-weekly dosing regimen administered on consecutive days. The primary endpoints of this study are overall survival and progression-free survival, and the results are expected to further define the role of dordaviprone in earlier lines of therapy. The ACTION trial addresses the major gaps in evidence for the use of dordaviprone in H3 K27 M DMG. It is a phase III randomized controlled trial evaluating dordaviprone in the front-line setting. The imaging schedules in this study will be more consistent than previous data which will mitigate potential confounders when evaluating PFS, DOR, and ORR. The trial is also controlling for other pharmacotherapy interventions, requiring washout periods for temozolomide, DRD2 antagonists, and CYP3A4/5 inducers and inhibitors. It is excluding patients who have received bevacizumab at any time.
Pharmacokinetics and drug interactions
Dordaviprone is an orally administered imipridone with demonstrated penetration of the blood–brain barrier. It is primarily metabolized by cytochrome P450 3A4 (CYP3A4). The elimination half-life of dordaviprone is approximately 10.2 h, while its active metabolite, ONC207, has a longer half-life of approximately 27.4 h. The drug exhibits a large volume of distribution of approximately 450 liters and is highly protein bound, with 95% to 97% binding observed in vitro. Pharmacokinetic studies have demonstrated that coadministration with strong CYP3A4 inhibitors increases drug exposure, whereas CYP3A4 inducers, including certain anticonvulsants and corticosteroids, may reduce systemic concentrations. 3
Supportive and symptomatic pharmacotherapy
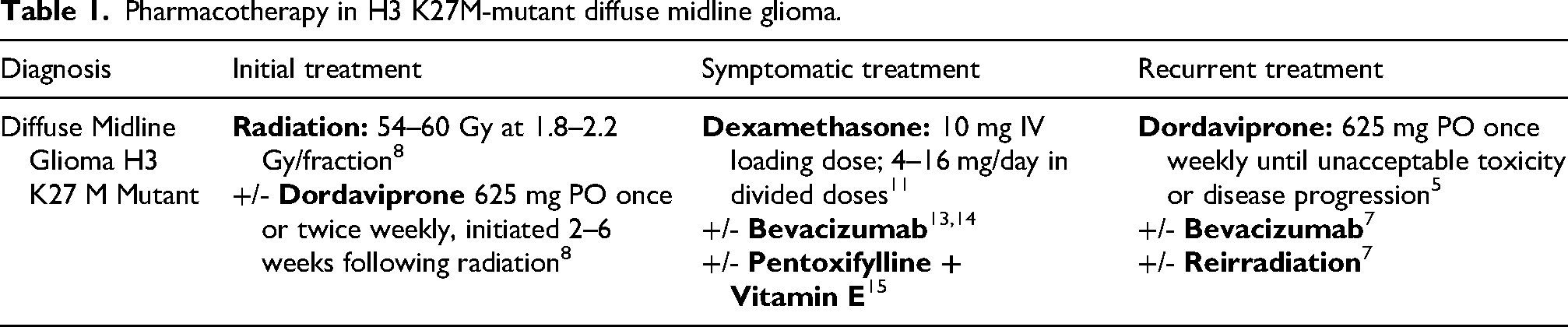
Supportive pharmacotherapy remains an important component of management in H3 K27 M diffuse midline glioma, particularly for the control of peritumoral edema and radiation-related complications. Glucocorticoids, including dexamethasone and betamethasone, are commonly used for symptomatic management. Dexamethasone is typically administered as a 10 mg intravenous loading dose followed by maintenance dosing ranging from 4 to 16 mg daily in divided doses. 11 Betamethasone is generally dosed at an equivalent ratio and may offer pharmacokinetic advantages in certain clinical scenarios. 12 Bevacizumab has been studied in managing edema in glioma.13,14 Additionally, pentoxifylline in combination with vitamin E has been studied in the context of radiation-induced necrosis, with dosing regimens of 400 mg twice daily for pentoxifylline and 1000 IU daily for vitamin E reported in retrospective analyses. 15
Other common therapies and investigational studies
Temozolomide remains a commonly used agent in high-grade gliomas and was administered to a majority of patients prior to treatment with dordaviprone in the integrated analysis used by the FDA for approval. Specifically, 88% of patients included in the analysis had previously received temozolomide as part of their treatment regimen. This is despite the lack of methylated MGMT promoters in H3 K27 M glioma,16,17 very limited efficacy data of temozolomide in H3 K27 M DMG, 18 and temozolomide resistance in H3 K27 M DMG. 19 Bevacizumab is commonly given in glioma patients with recurrent or progressive disease given its anti-angiogenesis properties through VEGF inhibition, including many patients in the ACTION trial. 7 Bevacizumab has also been evaluated for its role in managing radiation-associated edema and related symptoms in glioma.13,14 in case studies. However, like temozolomide, bevacizumab has limited data in H3 K27 M DMG in controlled trials and its role is still evolving. A number of investigational therapies are currently under evaluation for H3 K27 M diffuse midline glioma. These include GD2-targeted chimeric antigen receptor (CAR) T-cell therapies, which have demonstrated early signals of clinical activity, 20 as well as immunotherapeutic approaches such as immune checkpoint inhibitors and vaccine-based strategies. 21 Additional agents under investigation include combination therapies involving mebendazole, 22 as well as targeted approaches such as venetoclax 23 and CD99-directed therapies. 24 Anlotinib and olaparib have shown some observed clinical efficacy in combination with other therapies.25,26 These investigational treatments are primarily being evaluated in early-phase clinical trials and preclinical studies.
Collective critical appraisal of dordaviprone's evidence
The overall strength of evidence supporting dordaviprone is limited and consistent with its accelerated approval status. All primary studies were early-phase, single-arm trials with small sample sizes, creating risk of selection bias. The absence of randomized comparator groups prevents definitive assessment of treatment effect relative to standard care or historical controls. Heterogeneous prior treatments and disease courses complicate interpretation across studies. Reliance on surrogate endpoints, particularly RANO-based radiographic response and PFS, introduces uncertainty in the context of diffuse midline glioma where imaging changes may not fully correlate with clinical outcomes. Survival data, while encouraging, remain immature and may be influenced by subsequent therapies and supportive care. Taken together, current evidence suggests that dordaviprone has modest activity with a favorable safety profile in recurrent H3 K27 M DMG, but the magnitude of clinical benefit remains uncertain pending confirmatory RCT data.
Discussion
The treatment of H3 K27M-mutant diffuse midline glioma (DMG) remains a significant clinical challenge due to its aggressive biology, limited surgical accessibility, and resistance to conventional systemic therapies such as temozolomide. Developments in pharmacotherapy for this disease have unfortunately long been pursued with limited clinical translatability. The accelerated approval of dordaviprone by the United States FDA represents a meaningful milestone. As a new and unique pharmacotherapy option in this disease, dordaviprone represents an additional treatment modality to pair with surgical and radiotherapy options. This review synthesizes the available evidence and contextualizes dordaviprone's place in therapy from a clinical pharmacotherapy perspective.
Dordaviprone has demonstrated modest but durable radiographic responses and disease control in a subset of patients with recurrent H3 K27 M DMG, with an ORR of 20%, a median DOR of 11.2 months, and corticosteroid response in nearly half of evaluable patients. These findings are clinically meaningful in a setting where no alternative pharmacotherapy has been approved and where functional decline is a defining feature of disease progression. The corticosteroid response rate is particularly relevant: a reduction in corticosteroid burden has direct quality-of-life implications for patients managing the cumulative effects of long-term glucocorticoid use. Although radiographic changes assessed by RANO criteria may not uniformly reflect symptomatic benefit in all patients, the consistency of response across radiographic and functional measures supports the biological plausibility of dordaviprone's mechanism in this disease.
The evidence supporting dordaviprone must be interpreted within inherent limitations. The integrated analysis that formed the basis for FDA approval enrolled only 50 patients in a non-randomized, single-arm design, making it impossible to quantify survival benefit relative to a comparator. The accelerated approval appropriately acknowledges this limitation while recognizing the severity of unmet need. Until additional data from the ACTION trial is available, clinicians and pharmacists should interpret current evidence while recognizing that for patients with recurrent H3 K27 M DMG, no proven therapeutic alternative exists and the risk-benefit profile of dordaviprone remains favorable relative to supportive care alone. Participation in the ACTION trial or other clinical studies should be encouraged for eligible patients, as access to clinical trials in oncology remains a documented barrier for a substantial portion of the patient population. 27
Conventional cytotoxic chemotherapy, particularly temozolomide, appears to have limited utility in the specific H3 K27M-mutant diffuse midline glioma, although much of the data is theoretical or preclinical. Limited temozolomide efficacy could be attributable to underlying molecular resistance mechanisms, including low rates of MGMT promoter methylation. The available evidence supporting temozolomide in this disease remains limited if H3K27 M is molecularly confirmed. Its historical prevalence largely reflects use prior to mutation-specific genotyping, underscoring the importance of molecular characterization in guiding pharmacotherapy decisions. The ACTION trial's inclusion of a temozolomide washout requirement further signals its recognition as a potential confounder in this genotype.
Bevacizumab occupies a nuanced position in H3 K27 M DMG management. Its anti-VEGF mechanism may reduce vascular peritumoral edema and lower glucocorticoid requirements, supporting a symptomatic role. However, it also poses a significant imaging confounder: pseudoresponse, where apparent tumor shrinkage on MRI reflects reduced vascular permeability rather than true tumor regression, may confound radiographic response endpoints. This concern is reflected in the ACTION trial's exclusion of patients with any prior bevacizumab use, which may eventually provide more definitive guidance on its role in the H3 K27 M DMG treatment paradigm. Until such data emerge, its use should be reserved for symptomatic management with clear documentation of the imaging interpretation challenge it introduces.
Supportive pharmacotherapy, including corticosteroids, continues to play an important role in symptom management. These therapies may improve quality of life through reduction of associated neurologic symptoms but do not appear to significantly alter disease progression. Dexamethasone is a popular steroid used in H3 K27 M DMG due to its CNS penetration, potency relative to other steroids, long half life, and glucocorticoid selectivity. Dexamethasone is a heavily used steroid in CNS cancers. Betamethasone may be considered as an alternative when dexamethasone is unavailable or poorly tolerated, given its structural similarity and pharmacokinetic profile, though DMG-specific data are limited. Pentoxifylline with vitamin E represents a reasonable adjunct consideration for radiation-induced necrosis, though the evidence base is confined to retrospective cohort analyses and its use requires assessment of bleeding risk.
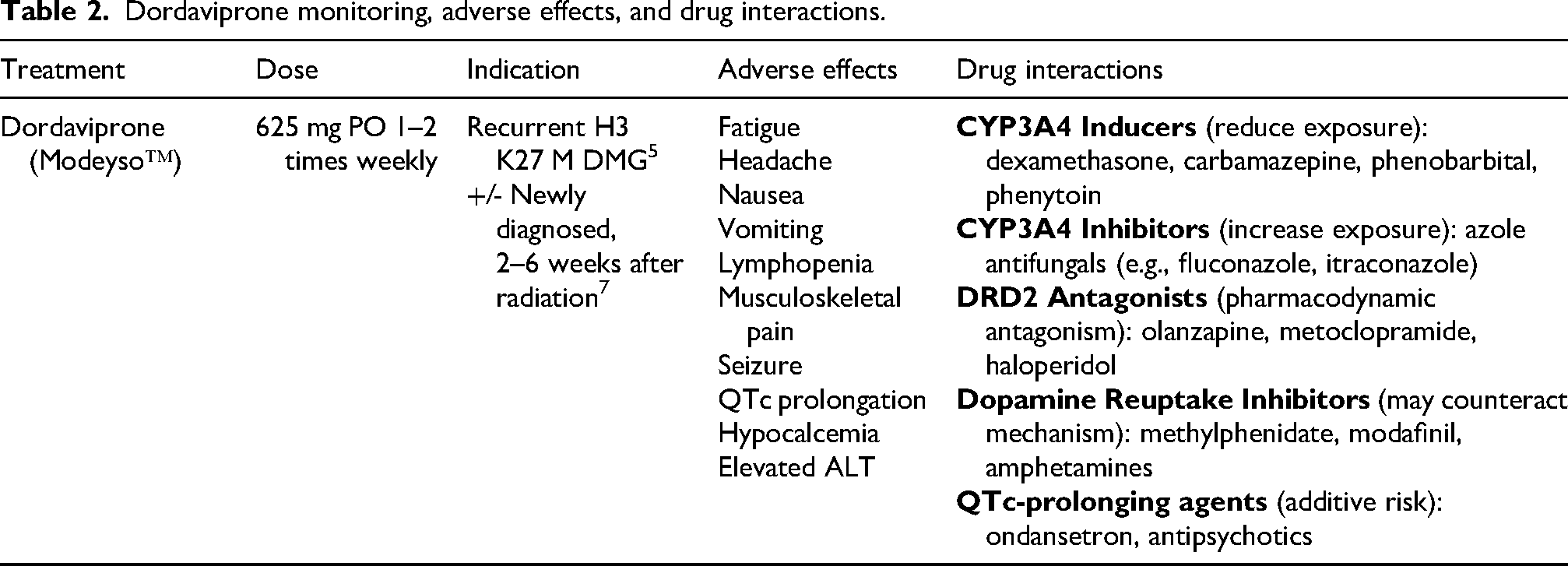
From a clinical pharmacotherapy perspective, dordaviprone's drug interaction profile warrants proactive and ongoing monitoring throughout the treatment course. Table 2 summarizes key interactions. Dexamethasone, which virtually all patients will receive for symptomatic management, is a dose-dependent CYP3A4 inducer. Significant escalations in dexamethasone dose may reduce dordaviprone exposure and attenuate therapeutic effect; in such circumstances, the twice-weekly dosing schedule may be preferred over once-weekly to compensate. Anticonvulsants including carbamazepine, phenobarbital, and phenytoin are strong CYP3A4 inducers and should be avoided where possible in favor of non-inducing alternatives such as levetiracetam. Azole antifungals (e.g., fluconazole, itraconazole) inhibit CYP3A4 and may increase dordaviprone exposure and toxicity risk, requiring clinical vigilance or dose modification considerations.
Because dordaviprone acts in part as a dopamine D2/D3 receptor antagonist, concurrent use of DRD2 antagonists such as olanzapine, metoclopramide, or haloperidol—commonly prescribed for nausea and vomiting in this setting—may theoretically produce pharmacodynamic redundancy or interference with efficacy. Serotonin 5-HT3 antagonists (e.g., ondansetron) are preferred antiemetics in this context, with attention to additive QTc prolongation risk when combined with other QTc-prolonging agents. Dopamine reuptake inhibitors including methylphenidate, modafinil, and amphetamines, which may be used for cancer-related fatigue, could theoretically counteract the dopamine antagonism central to dordaviprone's mechanism and should generally be avoided during treatment cycles.
The once-weekly oral dosing regimen of dordaviprone offers practical advantages in terms of patient burden but also introduces adherence considerations unique to a weekly rather than daily schedule. Pharmacists are positioned to provide targeted counseling around the importance of consistent weekly dosing, recognition and management of common adverse effects including fatigue and nausea, the impact of food on Cmax (reduced with high-fat meals), and the need for proactive communication about any new medications that may introduce drug interactions with dordaviprone. Medication reconciliation at each clinical encounter is especially important given the complexity of the concurrent medication regimen typical in this population.
Several limitations of the current evidence should be explicitly acknowledged. Available data are derived primarily from small, early-phase studies with heterogeneous patient populations and no comparator arms. Accelerated approval based on surrogate endpoints limits the ability to draw definitive conclusions regarding long-term clinical outcomes or true survival benefit. The ongoing phase 3 ACTION trial will be essential in confirming whether dordaviprone provides a measurable OS benefit in newly diagnosed disease and in resolving the confounders identified in the current approval dataset. Future research should also examine optimal sequencing with radiation, combination strategies, and the emerging investigational therapies including CAR T-cell and immunotherapeutic approaches that may complement or eventually challenge dordaviprone's role. Table 1 provides a summary of the current pharmacotherapy framework for H3 K27 M DMG across the disease course. Overall, dordaviprone represents a meaningful therapeutic advance in a disease historically lacking approved options, and its optimal positioning will continue to evolve as additional clinical data emerge.
Pharmacotherapy in H3 K27M-mutant diffuse midline glioma.
Dordaviprone monitoring, adverse effects, and drug interactions.
Conclusion
H3 K27 M DMG represents a challenging treatment landscape in pharmacotherapy. Dordaviprone (Modeyso™) is the first FDA approved therapeutic option for recurrent H3 K27 M DMG and represents a major milestone in drug development for this disease. Accelerated FDA approval was granted based on durable radiographic responses and survival outcomes observed across integrated Phase 1–2 studies and expanded access data. The evidence, while limited by its early-phase, non-randomized design, supports use in recurrent disease in the absence of any proven alternative. The ongoing phase 3 ACTION trial will further evaluate dordaviprone's efficacy in newly diagnosed H3 K27 M DMG and is expected to provide the data needed to firmly characterize its role in therapy. While participation in a clinical trial may still be a preferred treatment option for eligible patients, access to clinical trials in oncology remains a barrier for a substantial number of people. Symptomatic therapy for H3 K27 M DMG and radiation may include glucocorticoids, bevacizumab, and pentoxifylline with vitamin E. Pharmacotherapy is not a substitute for radiation, and neurosurgical consultation should be obtained at diagnosis regardless of glioma grade or H3 K27 M status. Pharmacists play a critical role in optimizing dordaviprone therapy through interaction screening, adverse effect monitoring, adherence counseling, and coordination of supportive care.
Footnotes
Author contributions
ZN: Conceptualization, Methodology, Investigation, Writing – Original Draft, Writing – Review & Editing, Project Administration.
CD: Investigation, Writing – Original Draft.
DG: Conceptualization, Methodology, Investigation, Supervision, Writing – Review & Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and informed consent
Ethics approval and informed consent were not required for this clinical review.
Data availability statement
All data supporting the findings of this study are available within the article and its supplementary materials.