
Abstract
Introduction
Delayed methotrexate clearance can result in life-threatening toxicities including renal failure. Treatment includes vigorous hydration, urine alkalinization, leucovorin rescue, and glucarpidase. While traditional glucarpidase dosing is weight-based, its pharmacokinetic properties support possible use of non-weight-based dosing strategies. We evaluated clinical outcomes after transition from weight-based to fixed-dose glucarpidase for high-dose methotrexate (HDMTX) toxicity at a large academic medical center.
Methods
Adult patients requiring inpatient glucarpidase for HDMTX-associated renal insufficiency between October 2014 and June 2025 were retrospectively reviewed. Patients receiving weight-based glucarpidase prior to implementation of a fixed 2000-unit dosing strategy were included for comparison. The primary objective was to compare time to renal recovery. Secondary outcomes were exploratory and included time to glucarpidase administration, peak serum creatinine (Scr) fold-change, dialysis requirement, and hospital length of stay (LOS).
Results
Fourteen patients were included for analysis. Time to renal recovery was nearly identical between groups. The fixed-dose group received glucarpidase significantly sooner after HDMTX compared to the weight-based group (median 45.1 h vs. 71.5 h, p = 0.015) and had significantly lower max fold change in Scr (median 2.8-fold vs 3.8-fold, p = 0.034). The need for dialysis and median LOS trended towards fewer patients requiring dialysis (n = 0 vs n = 4, p = 0.070) and shorter LOS (19.1 days vs 39.3 days, p = 0.074) for the fixed-dose group.
Conclusions
Transitioning from a weight-based to 2000-unit fixed-dose for glucarpidase at our institution resulted in sustained efficacy and safety. Further research is necessary to define optimal glucarpidase dosing.
Introduction
High-dose methotrexate (HDMTX) is a chemotherapeutic agent utilized in treating both solid tumor and hematologic malignancies. Its ability to cross the blood-brain barrier makes it particularly effective for patients with central nervous system (CNS) malignancies, such as leukemias and lymphomas. 1 While many institutions have established protocols to ensure the safe administration and monitoring of HDMTX, its use can still lead to serious toxicities. One of the most concerning is acute kidney injury, which, if not promptly recognized and managed, can progress to renal failure. Even with institutional protocols utilizing vigorous hydration, urine alkalinization, and leucovorin rescue, renal dysfunction has been reported in 2–12% of patients receiving HDMTX.2,3 Following HDMTX administration, 80–90% of the parent drug and metabolites are excreted renally by glomerular filtration and tubular secretion.3,4 In addition to nephrotoxicity caused by methotrexate crystallization in the renal tubules, impaired clearance can prolong high methotrexate concentrations, leading to other significant adverse effects such as myelosuppression, gastrointestinal toxicity, and hepatotoxicity.
Glucarpidase is a recombinant carboxypeptidase enzyme that rapidly hydrolyzes methotrexate into two inactive metabolites, 4-deoxy-4-amino-N10-methylpteroic acid (DAMPA) and glutamate.1,5 It has been shown to reduce serum methotrexate levels by ≥ 97% within 15 min of intravenous administration.2,5 Following its FDA approval in 2012, it became the only commercially available non-renal modality for methotrexate elimination in the setting of methotrexate induced renal toxicity. 5 While hemodialysis remains a potential option for methotrexate removal, its efficacy is limited, in part by the high protein binding capacity of methotrexate. 4 Glucarpidase is indicated as a single, weight-based dose of 50 units/kg for the treatment of toxic plasma methotrexate concentrations exceeding 1 µmol/L.5,6 Widely cited consensus guidelines outline recommendations for glucarpidase use per a set of criteria related to renal dysfunction and methotrexate levels at specified time points based on methotrexate infusion duration. 1 Due to its high molecular weight, glucarpidase is primarily confined to the intravascular compartment and is most effective when administered within 60 h of methotrexate infusion. 1 As of early 2026, the average wholesale price of a 1000-unit vial of glucarpidase was reported to be $51,879.60. 7 Recent literature has increasingly explored glucarpidase dose optimization strategies, including dose capping and fixed-dosing, highlighting the need for real world data to inform safe and operationally feasible alternatives to standard weight-based dosing. Owing to its high cost and infrequent use, many hospitals are unable to routinely stock sufficient inventory to meet weight-based dosing requirements. As a result, many centers have implemented a “fixed-dose” strategy for glucarpidase based on its low volume of distribution. A small, published case series outlined processes and procedures for the use of a single 1000-unit vial followed by repeat dosing if 30-min High Performance Liquid Chromatography (HPLC) serum methotrexate levels were above a certain threshold after glucarpidase administration. 4 Because our institution does not have access to in-house HPLC testing to determine need for repeat glucarpidase dosing, we utilize a 2000-unit fixed-dose strategy. We aimed to describe our institutional experience following the transition from weight-based to a fixed 2000-unit glucarpidase dosing strategy at UPMC Shadyside Hospital.
Materials and methods
This was a single-center, retrospective chart review of all adult patients who required glucarpidase for HDMTX related renal insufficiency at UPMC Shadyside Hospital between October 2014 and June 2025. Approval was authorized by the University of Pittsburgh Institutional Review Board (IRB STUDY25080015) with a waiver of informed consent. All patients admitted to UPMC Shadyside Hospital for HDMTX who had received a dose of glucarpidase were included. Patients received standard supportive care measures including leucovorin, aggressive hydration with alkalinized intravenous fluid to maintain a urine pH ≥ 7 and urine output of 1200 mL/8 h nursing shift, and monitoring of methotrexate levels, serum creatinine (Scr), serum bicarbonate levels, and liver function tests. The institutional HDMTX supportive care protocol, including IV fluid composition and rate targets, remained unchanged throughout the study period. Intravenous bicarbonate fluids were started on admission (prior to the start of HDMTX) for all patients and adjusted based on serum bicarbonate levels, fluid volume status, and urine pH throughout the methotrexate clearance process. Patients who received weight-based glucarpidase (rounded to vial size) prior to the implementation of the fixed 2000-unit dosing strategy in 2023 were included for comparison.
The primary objective was to compare time to renal recovery between dosing strategies. Time to renal recovery was defined as time from glucarpidase administration to return of Scr to ≤ 1.5 times baseline and no longer requiring dialysis. Patients who did not recover prior to discharge were excluded. Secondary outcomes were exploratory and included time to glucarpidase administration, peak creatinine fold-change, dialysis requirement, and hospital length of stay (LOS).
It should be noted that early glucarpidase administration is independently associated with better outcomes. 2 The fixed-dose strategy for glucarpidase inherently results in a quicker turnaround time for drug dispensing and administration due to two vials being routinely stocked in our hospital inpatient pharmacy. As a result, we cannot adequately control for outcomes associated with this variable.
The study cohort was characterized by descriptive statistics. Categorical variables were compared for statistical significance using the Fisher's exact test. Continuous non-normally distributed variables were compared using the Mann-Whitney U test. No test was performed where all values were identical across both groups. All p-values were two-sided and considered statistically significant if p < 0.05. Statistical analysis was performed with R version 4.4.2.
Results
The medical records of patients requiring glucarpidase rescue for HDMTX toxicity between October 10, 2014 and June 30, 2025 at UPMC Shadyside Hospital were evaluated. A total of 14 patients were included for review after confirming documented receipt of glucarpidase and all data were collected retrospectively from the electronic health record. Seven patients (50%) received weight-based glucarpidase (50 units/kg rounded to vial size) and 7 patients (50%) received fixed-dose glucarpidase (2000 units) as shown in Table 1. For patients in the fixed-dose group, 6 patients received 2000 units once, while 1 patient received 1000 units x 2 doses separated by approximately 8 h. The median glucarpidase dose in the weight-based group was 46.8 units/kg (range 37.6–53 units/kg) versus 20.2 units/kg (range 18.6–31.7 units/kg) in the fixed-dose group.
Baseline characteristics.
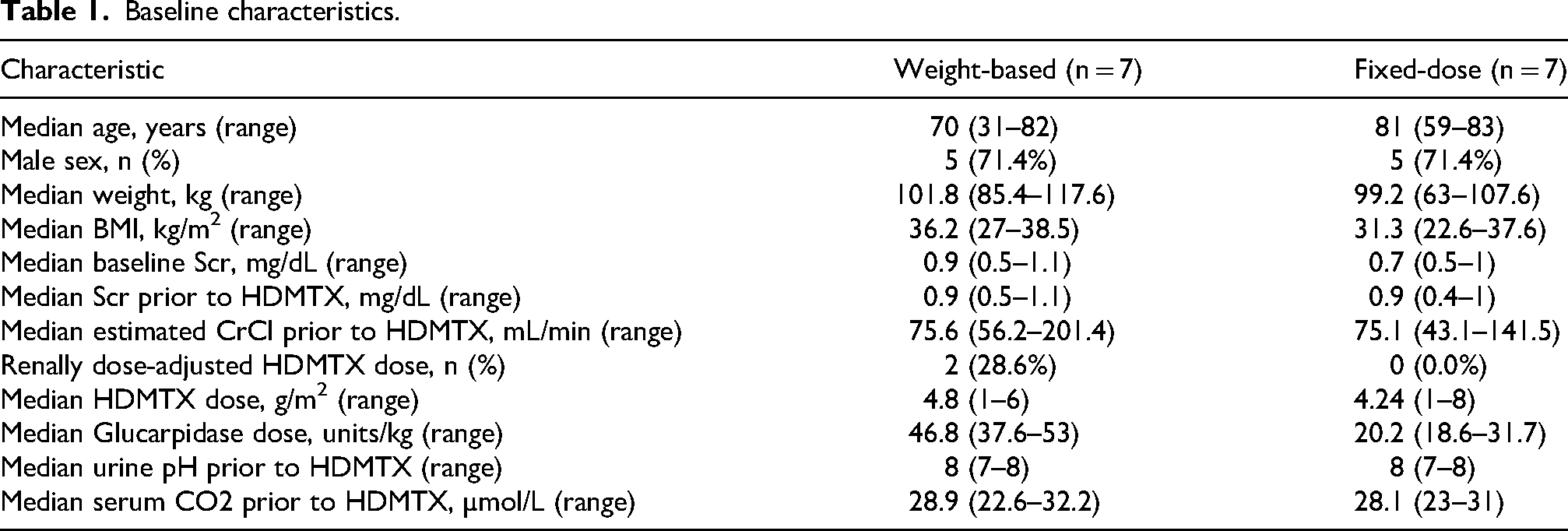
Among the 14 cases reviewed, 7 patients had a diagnosis of primary CNS lymphoma, 3 patients had secondary CNS lymphoma, and 4 patients had B- cell acute lymphoblastic leukemia (B-ALL). As shown in Table 1, a majority of patients were elderly (median age 73.5 years), male (71.4%), and had a larger body mass index (median body mass index (BMI) 34.7 kg/m2). A majority of patients received HDMTX monotherapy as a bolus over 4 h (n = 9), and more than half of these patients were undergoing their first cycle (n = 5). Three patients received HDMTX as a bolus over 2 h followed by a subsequent continuous infusion over 24 h as part of the “B” cycle of the Hyper-CVAD regimen. One patient received HDMTX as part of the EWALL-Ph-01 consolidation protocol as a continuous infusion over 24 h, and another patient received HDMTX as part of a clinical trial as a bolus over 4 h along with temozolomide, rituximab, and tirabrutinib.
Patient specific and admission specific risk factors for HDMTX toxicity were evaluated as shown in Table 2. As previously stated, the majority of our cohort was obese (defined as a BMI ≥ 30), but median BMI did not differ significantly between groups. There were also no significant differences between groups regarding median baseline Scr, median Scr prior to HDMTX, median estimated creatinine clearance (CrCl) prior to HDMTX, renal dose adjustment for HDMTX, median HDMTX dose, median urine pH prior to starting HDMTX, and median serum CO2 prior to starting HDMTX. Relevant comorbidities such as cirrhosis with ascites, chronic kidney disease (CKD), and heart failure were not statistically different between groups. Potentially interacting medications, lack of urine pH checks every 8 h after HDMTX administration per protocol, inadequate urine output during clearance, and documentation of acidic urine during clearance were also not significantly different between groups (Table 2).
Patient and admission risk factors for HDMTX toxicity.
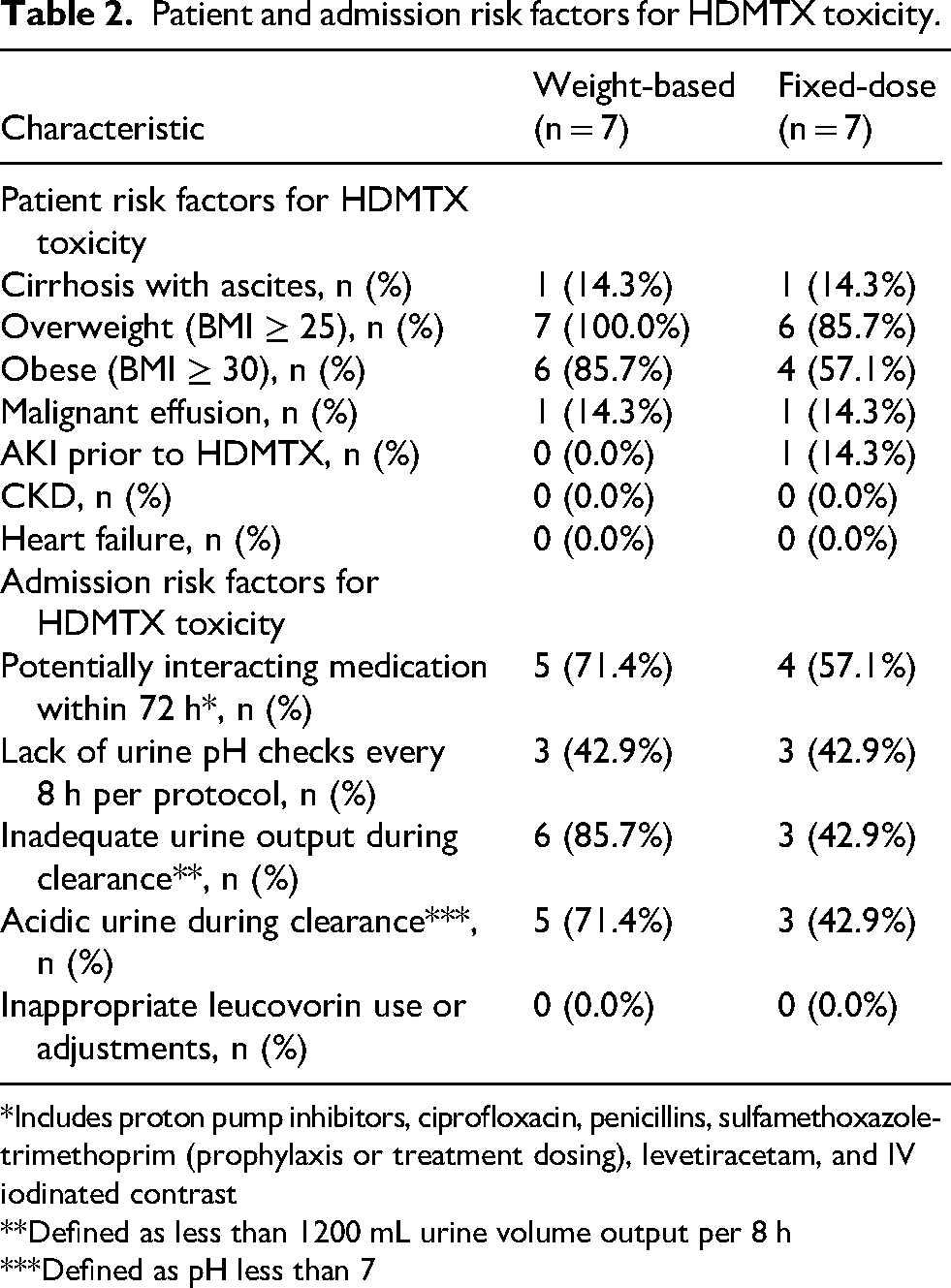
*Includes proton pump inhibitors, ciprofloxacin, penicillins, sulfamethoxazole-trimethoprim (prophylaxis or treatment dosing), levetiracetam, and IV iodinated contrast
**Defined as less than 1200 mL urine volume output per 8 h
***Defined as pH less than 7
Comparison of outcomes between glucarpidase dosing strategies.
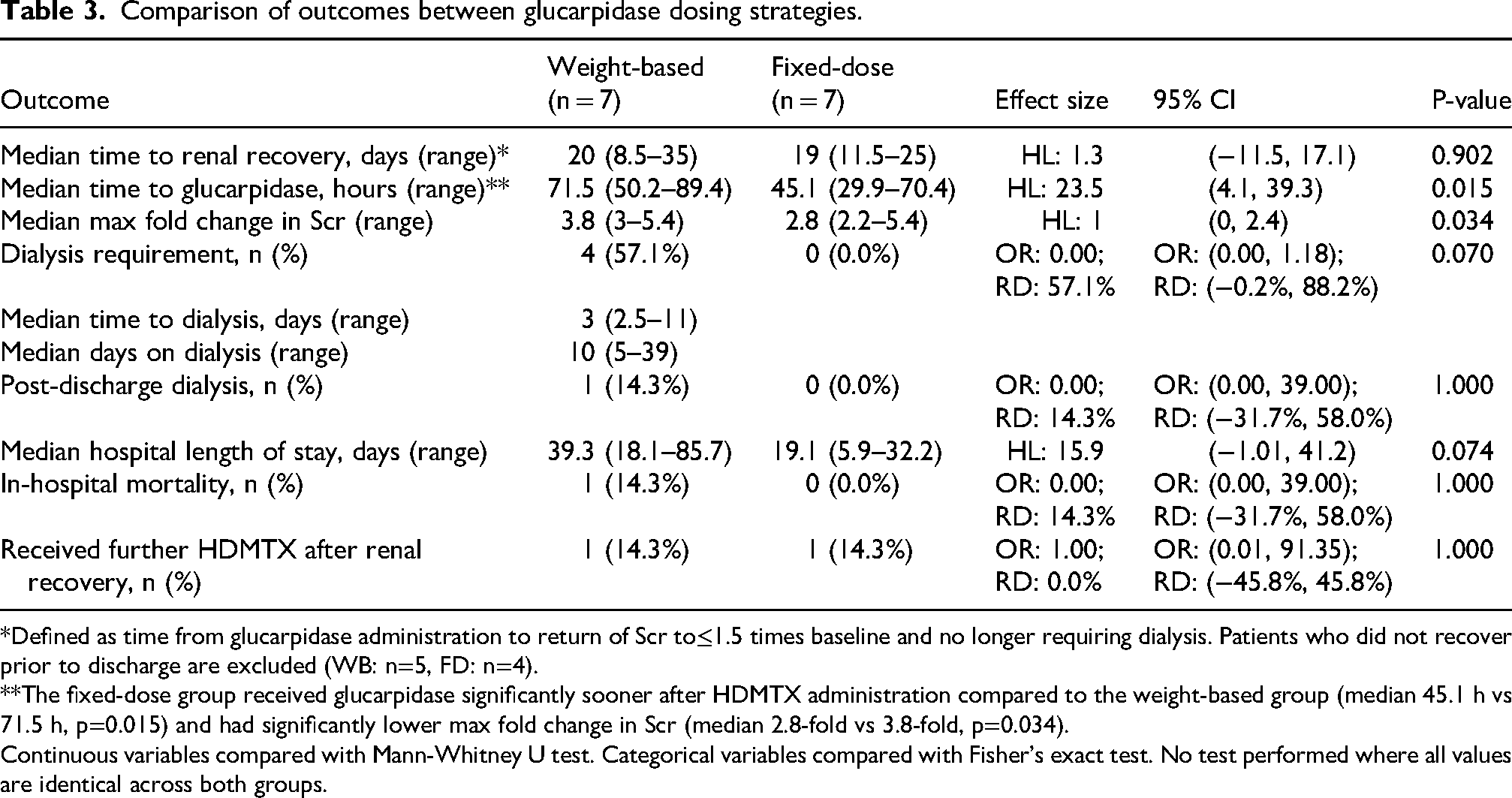
*Defined as time from glucarpidase administration to return of Scr to≤1.5 times baseline and no longer requiring dialysis. Patients who did not recover prior to discharge are excluded (WB: n=5, FD: n=4).**The fixed-dose group received glucarpidase significantly sooner after HDMTX administration compared to the weight-based group (median 45.1 h vs 71.5 h, p=0.015) and had significantly lower max fold change in Scr (median 2.8-fold vs 3.8-fold, p=0.034).
Continuous variables compared with Mann-Whitney U test. Categorical variables compared with Fisher's exact test. No test performed where all values are identical across both groups.
Our primary outcome, median time to renal recovery, was nearly identical between groups (19 days vs 20 days, p=0.902) as shown in Table 3. The fixed-dose group received glucarpidase significantly sooner after HDMTX administration compared to the weight-based group (median 45.1 h vs 71.5 h, p = 0.015) and had significantly lower max fold change in Scr (median 2.8-fold vs 3.8-fold, p = 0.034). While the need for dialysis and median LOS were not statistically significant between groups, there was a trend towards fewer patients requiring dialysis (n = 0 vs n 4, p = 0.070) and a shorter LOS (19.1 days vs 39.3 days, p = 0.074) for patients in the fixed-dose group as compared to those in the weight-based group. The risk difference just barely contained 0 for need for dialysis, and although statistical significance was not achieved, the point estimate suggested a substantial potential effect (57.1%). It is possible that our study was underpowered to detect a significant change in need for dialysis and median LOS based on the small sample size included.
We retrospectively reviewed serum methotrexate level results via HPLC testing for this cohort as shown in Table 4. Of the 7 patients who received the 2000-unit fixed-dose strategy, 4 patients had undergone a post-glucarpidase serum methotrexate level using HPLC testing via send-out to an outside laboratory to differentiate active drug from inactive metabolite. All 4 patients had >98% reduction in active metabolite after receipt of 2000-unit fixed-dose glucarpidase.
High-performance liquid chromatography (HPLC) levels analysis.
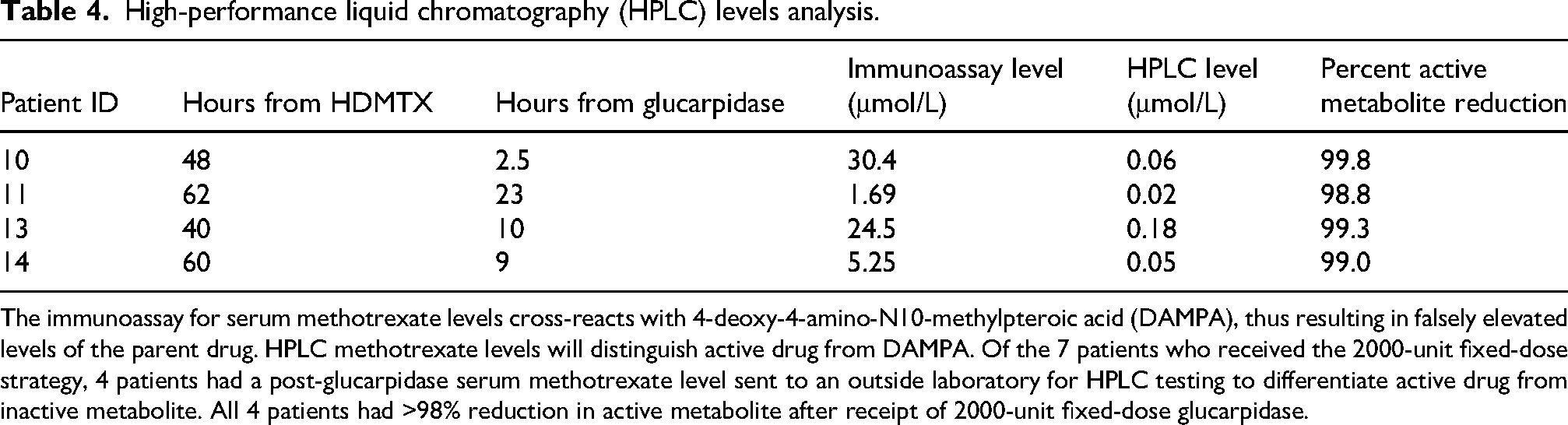
The immunoassay for serum methotrexate levels cross-reacts with 4-deoxy-4-amino-N10-methylpteroic acid (DAMPA), thus resulting in falsely elevated levels of the parent drug. HPLC methotrexate levels will distinguish active drug from DAMPA. Of the 7 patients who received the 2000-unit fixed-dose strategy, 4 patients had a post-glucarpidase serum methotrexate level sent to an outside laboratory for HPLC testing to differentiate active drug from inactive metabolite. All 4 patients had >98% reduction in active metabolite after receipt of 2000-unit fixed-dose glucarpidase.
Discussion
To our knowledge, this is the largest published comparison of weight-based versus fixed-dose glucarpidase dosing strategies for HDMTX toxicity. While a few larger publications have included patients who have received smaller glucarpidase doses for a variety of reasons (i.e., supply shortages, obesity, etc.), our study is the first to directly compare outcomes between patients receiving weight-based vs a 2000-unit fixed-dose strategy.
While our primary outcome, median time to renal recovery, was not statistically significant between groups, we believe this shows safety and efficacy of the fixed-dose approach as compared with the weight-based dosing approach. Although formal non-inferiority testing was not performed, outcomes were comparable between dosing strategies. Baseline characteristics were balanced between groups. As previously stated, median time to glucarpidase administration was significantly shorter, while median hospital LOS trended towards significance for the fixed-dose glucarpidase group. Although the trend towards overall shorter LOS cannot directly be attributed to a shorter time to glucarpidase administration, it is well established that glucarpidase efficacy is greater the sooner that it is administered. While we acknowledge that shorter time to glucarpidase administration for the fixed-dose group may have been driven by a change in institutional policy to routinely stock two vials of glucarpidase in the inpatient pharmacy, we would not have been capable of providing full weight-based dosing within a comparable timeframe. Weight-based dosing would have required ordering of additional vials, thus delaying glucarpidase administration. In addition, there are significant potential cost savings associated with this fixed-dose strategy. The median weight-based dose would have required 5 vials per patient at $51,879.60 per vial, compared with 2 vials per patient, yielding an estimated savings of approximately $1.1 million across 7 patients. Potential additional savings from reduced LOS and avoidance of dialysis were not quantified but may be substantial.
As previously mentioned, the fixed-dose strategy takes advantage of the pharmacokinetic properties of glucarpidase. Given its larger size (83 kDa) and low volume of distribution (3.6 L), it is primarily confined to the intravascular space and does not distribute to tissues or intracellular compartments. 1 After HDMTX administration, the drug is transported intracellularly via reduced folate carriers. As a result, early administration of glucarpidase limits the additional accumulation of intracellular polyglutamated methotrexate, thus reducing the degree of cellular methotrexate toxicity. Thus, many experts in the field have advocated for development of dosing strategies more dependent on pre-glucarpidase methotrexate levels as opposed to larger body habitus. 3 Pharmacokinetic and pharmacodynamic modeling studies have supported this, as a study by Kimura et al. reported both glucarpidase 20 units/kg and 50 units/kg reduced a plasma methotrexate concentration of 100 μM to less than 0.1 μM 70 h after administration. 8 Therefore, weight-based dosing of glucarpidase may be unnecessary, as it leads to the potential for overdosing of obese patients and avoidable financial toxicity.
While limited, other publications explore the use of lower doses of glucarpidase for HDMTX toxicity. Studies leading to FDA and EMA approval of glucarpidase reported some patients receiving lower than the recommended dosage.3,5,6,9 A case report published by Trifilio et al. detailed a case of a 59 yo male with pre-T acute lymphoblastic lymphoma who became anuric after a HyperCVAD B cycle. After two hemodialysis sessions, the patient received a single 1000 unit dose of glucarpidase (approximately 7.7 units/kg) with improvement in renal function. 10 In a study by Schwartz et al., 43 patients receiving > 1 g/m2 HDMTX were given glucarpidase if serum MTX levels were >5 μmol/l at ≥ 42 h after the start of HDMTX or had renal failure if <42 h after the start of HDMTX. Eleven of the 43 patients received lower doses (10–31 units/kg) due to a glucarpidase supply shortage. A second glucarpidase dose was allowed in patients with serum MTX >0.1 μmol/l ≥ 24 h after the first dose. A specific efficacy analysis based on this subset of 11 patients was not discussed, although it was noted that survival and HDMTX related toxicities did not correlate with variables such as glucarpidase dose. 11 In a later study by Heuschkel et al., 7 patients with toxic HDMTX levels received “half-dose” glucarpidase (mean 25 units/kg, range 17–32 units/kg) resulting in effective MTX concentration reduction to levels < 10 µmol/L. 12 A study by Krüger et al. evaluated glucarpidase dosed based on ideal body weight in 3 obese patients for delayed MTX clearance (2 of the 3 patients had acute kidney injury (AKI)). After administration of a single 4000 unit dose (23–40 units/kg), all patients achieved a rapid reduction in MTX level resulting in improvements in clinical status and renal function. 13 Truong et al. published a case series of 5 patients who received 1000-unit fixed-dose glucarpidase. As per their institutional protocol, repeat dosing with a second 1000-unit fixed-dose was allowed if 30-min HPLC serum MTX levels were > 1 μmol/L or if rebound toxicity occurred (defined as HPLC serum MTX level of > 1 μmol/L within 72 h of glucarpidase). All patients were reported to have undetectable MTX levels within 24 h of glucarpidase receipt and no patients developed additional MTX dose limiting toxicities (aside from reversible AKI) or death during hospitalization. 4 In a study by Gupta et al., a small subset of patients received glucarpidase dosed at <50 units/kg, but unfortunately analysis of this subgroup is not readily available. 14 More recently, a case series by Ertz and colleagues describe their institutional experience with 6 patients who received glucarpidase capped at a single 1000-unit vial dose. While 4 of the 6 patients (66.7%) achieved a serum methotrexate level < 0.05 at 24 h post-glucarpidase administration, 4 patients (66.7%) required renal replacement therapy and 2 patients (33.3%) died from preexisting complications and organ dysfunction. No patients received repeat glucarpidase doses. 15 Lastly, Scott et al. evaluated 26 pediatric patients who received glucarpidase at St Jude Children's Research Hospital. Glucarpidase doses ranged from 13–90 units/kg (doses < 50 units/kg were due to dose capping at a full vial size; doses >50 units/kg were due to rounding up to the next full vial size). A multivariable analysis did not show a significant relationship between glucarpidase dosing and percent decrease in MTX levels. 16
There are several limitations associated with our study including the retrospective nature of the study, small sample size, and various treatment regimens and disease states of patients included. As previously stated, early glucarpidase administration is independently associated with better outcomes. 2 Because the fixed-dose strategy for glucarpidase inherently results in a quicker turnaround time for drug dispensing and administration, we could not adequately control for outcomes associated with this variable. Lastly, as described above, the case series by Truong et al. detailed outcomes of 5 patients who received one dose of 1000-unit fixed-dose glucarpidase followed by a post-glucarpidase serum methotrexate level using HPLC testing to determine the need for a repeat dose. 4 As our institution only has access to HPLC testing as a send-out lab, we cannot make decisions about glucarpidase repeat dosing in real time due to lengthy turnaround times and thus why this strategy was not implemented. While only 4 of the 7 patients in the fixed-dose group had a post-glucarpidase serum methotrexate level sent to an outside laboratory for HPLC testing, all 4 patients had a > 98% reduction in active metabolite after receipt of 2000-unit fixed-dose glucarpidase, thus demonstrating efficacy of this dosing strategy.
Conclusions
For patients with severe methotrexate toxicity, transitioning from a weight-based to a 2000-unit fixed dosing strategy for glucarpidase at our institution resulted in sustained efficacy and safety. Further research is necessary to define the optimal dose of glucarpidase, but recently published data infers that doses lower than 50 units/kg may be non-inferior. In addition, this fixed-dosing strategy may lead to potential substantial cost savings, especially in the treatment of obese patients and for larger cancer centers who treat higher volumes of HDMTX patients.
Footnotes
Acknowledgments
We acknowledge the UPMC Shadyside Hospital Hematology/Oncology Clinical Pharmacy Department (Timothy Brenner, PharmD, BCOP; Timothy George, PharmD, BCOP; Jason Steele, PharmD, BCOP; Amanda Agnew, PharmD, BCOP; Diana Mansour, PharmD, BCOP, and Jessica Sieg, PharmD, BCOP) for their work that contributed to the development, implementation, and maintenance of a 2000-unit fixed-dose glucarpidase protocol at UPMC Shadyside Hospital.
Ethical considerations
Approval of this study was authorized by the University of Pittsburgh Institutional Review Board (IRB STUDY25080015) with a waiver of informed consent.
Authorship comments
First author (Melissa L Bastacky) and senior author (Megan M Mantica)
Authorship
Study design: MLB, MM, SD, GL, JD, MMM. Data collection: MLB and MM. Statistical analysis: HT, MLB, MM. Manuscript writing and review: MLB, MM, MMM. Final version review and approval: All authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JD reports research support from Servier, AstraZeneca, and Novartis; and stockholder/equity interests in Pfizer and Gilead. SD reports UpToDate (contributing author), Incyte (speakers bureau/advisory board), Merck (advisory board), and Syndax (speakers bureau). None are relevant to this project.
All other authors do not have anything to disclose.
Data availability statement
The data collected and analyzed in this study are available upon reasonable request and approval by the University of Pittsburgh Institutional Review Board.