
Abstract
Background
Sacituzumab govitecan (SG) has shown clinical activity in hormone receptor-positive/human epidermal growth factor receptor 2-negative metastatic breast cancer (HR+/HER2− MBC), although evidence remains limited and heterogeneous. We performed a systematic review and meta-analysis to evaluate its efficacy and safety.
Methods
Studies assessing SG in HR+/HER2− MBC were systematically identified. Outcomes included objective response rate (ORR), disease control rate (DCR), progression-free survival (PFS), overall survival (OS), and safety. Random-effects models were used for pooled analyses.
Results
Twelve studies including 2431 patients (5 clinical trials, 7 real-world studies) were analyzed. The pooled ORR was 23% (95% CI, 17%–31%) and DCR was 68% (95% CI, 52%–80%). Median PFS and OS were 5.35 months (95% CI, 3.96–7.22) and 12.66 months (95% CI, 10.68–15.01), respectively. No significant differences in ORR were observed according to prior cyclin-dependent kinase 4/6 (CDK4/6) inhibitor exposure, number of prior treatment lines, or study design. Grade ≥3 neutropenia, febrile neutropenia, and diarrhea occurred in 46%, 5%, and 8% of patients, respectively.
Conclusions
SG demonstrates clinically meaningful antitumor activity in heavily pretreated patients with HR+/HER2− MBC. No statistically significant differences in ORR were detected according to prior CDK4/6 inhibitor exposure, number of prior treatment lines, or study design; however, these findings should be interpreted cautiously given the limited number of studies and substantial heterogeneity. Within a continuously evolving treatment landscape, further prospective studies are warranted to better define the optimal positioning of SG.
Introduction
Hormone receptor-positive/human epidermal growth factor receptor 2-negative metastatic breast cancer (HR+/HER2− MBC) is the most common subtype of breast cancer. 1 Despite advancements in treatment options, the prognosis may deteriorate significantly as the disease progresses. Particularly despite the gains achieved with cyclin-dependent kinase 4/6 (CDK4/6) inhibitors, selecting the optimal treatment for patients who develop resistance to these agents remains a significant clinical challenge.2–4 Consequently, there is an urgent need for effective and tolerable new therapeutic options in this patient population.
Sacituzumab govitecan (SG) is a trophoblast cell-surface antigen 2 (Trop-2) targeted antibody-drug conjugate (ADC) that has demonstrated efficacy in heavily pretreated patients with metastatic breast cancer.5–7 Specifically, the phase III TROPiCS-02 study showed that SG provided significant improvements in progression-free survival (PFS) and overall survival (OS) compared to chemotherapy in patients with HR+/HER2− MBC. 8 However, the results of that study are based on specific patient populations, and it remains unclear how treatment efficacy varies across different clinical subgroups as well as in real-world settings. Moreover, recent efforts to evaluate SG in earlier treatment lines, such as the ASCENT-07 study, reflect ongoing attempts to redefine its optimal place, further highlighting the complexity of treatment sequencing in this disease. 9
Studies evaluating the efficacy of SG in the HR + patient group are limited in the existing literature, often featuring small sample sizes and heterogeneous patient populations.10–19 Furthermore, factors that may influence treatment response—such as prior CDK4/6 inhibitor use, the number of previous therapy lines, or discrepancies between real-world data and clinical trial results—have not been sufficiently elucidated.
Therefore, we conducted this meta-analysis to systematically evaluate the efficacy and safety of SG in patients with HR+/HER2− MBC. Additionally, potential clinical and study-related factors that may influence treatment response were examined using subgroup analyses and meta-regression methods.
Materials and methods
Literature search and study selection
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. 20 PubMed/MEDLINE, Embase, Cochrane Library, and Google Scholar databases were systematically searched from inception to March 1, 2026. The search strategy was developed using a combination of Medical Subject Headings (MeSH) terms and relevant keywords, including: (‘Metastatic Breast Cancer’) AND (‘Sacituzumab Govitecan’ OR ‘IMMU-132’ OR ‘Trodelvy’) AND (‘Hormone Receptor Positive’ OR ‘HR+’ OR ‘HER2-negative’). Boolean operators (AND, OR) were applied to maximize the sensitivity and specificity of the search. Additionally, reference lists of relevant articles were manually screened to identify additional studies.
Inclusion criteria were defined as: (i) studies involving patients with HR+/HER2− MBC, (ii) administration of SG treatment, and (iii) reporting of at least one efficacy (survival and/or response rates) or safety outcome. Editorials, case reports, and studies with insufficient data were excluded. The detailed study selection process, from initial identification to final inclusion, is illustrated in the PRISMA flow diagram (Figure 1).
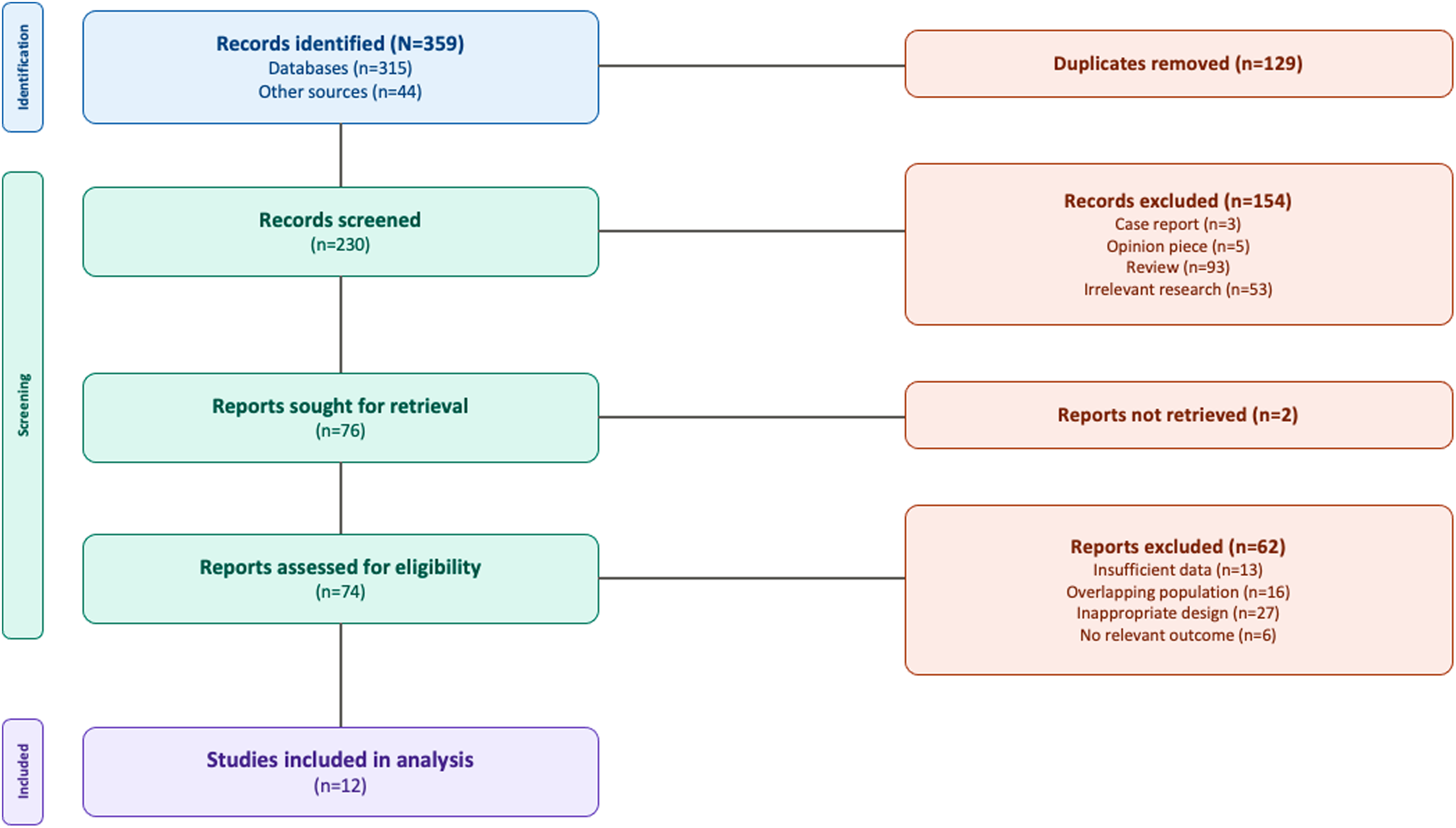
PRISMA flow diagram illustrating the study selection process for the systematic review and meta-analysis.
Data extraction and quality assessment
Study characteristics and outcome data were extracted by two independent researchers (A.K.G. and M.F.K.) using a standardized data collection form. Extracted data included study design, patient count, demographic characteristics, number of prior treatment lines, CDK4/6 inhibitor exposure, and clinical outcomes. Discrepancies were resolved through consensus with a third researcher (N.C.D.).
Outcome measures and statistical analysis
Primary outcomes were defined as objective response rate (ORR) and disease control rate (DCR). Secondary outcomes included median PFS, median OS, and the incidence of treatment-related adverse events (AEs), specifically grade ≥3 neutropenia, febrile neutropenia, grade ≥3 diarrhea, dose reductions, and treatment discontinuations.
For single-arm studies, ORR, DCR, and AE rates were pooled using a random-effects model with logit transformation (PLOGIT). In PFS and OS analyses, median survival values and 95% confidence intervals (CIs) were log-transformed, and standard errors (SE) were calculated using the formula: $SE = \frac{\log(\text{upper limit}) - \log(\text{lower limit})}{3.92}$. The resulting values were analyzed using a random-effects model, and results were back-transformed and reported in months. Heterogeneity was assessed using the I2 statistic and Cochran's Q test.
Subgroup analyses were performed based on clinically relevant variables. Studies were categorized according to prior CDK4/6 inhibitor exposure (≥80% vs. < 80%) to distinguish cohorts predominantly consisting of CDK4/6 inhibitor-pretreated patients from more heterogeneous study populations. This threshold was selected to improve comparability between studies while preserving an adequate number of studies within each subgroup for meaningful analysis. The number of prior treatment lines was categorized as 1–2 and ≥3 to represent early and late lines of therapy in clinical practice. Furthermore, real-world data (RWD) were compared with clinical trials according to study design.
Univariable meta-regression analyses were conducted to evaluate potential effects on ORR. Multivariable meta-regression was not performed due to the limited number of included studies, missing data for certain variables, and the absence of significant associations in univariable analyses. Publication bias was assessed visually using funnel plots. The methodological quality of the included studies was assessed using the Newcastle–Ottawa Scale (NOS). All statistical analyses were performed using R software (version 4.3.1, R Foundation for Statistical Computing).
Results
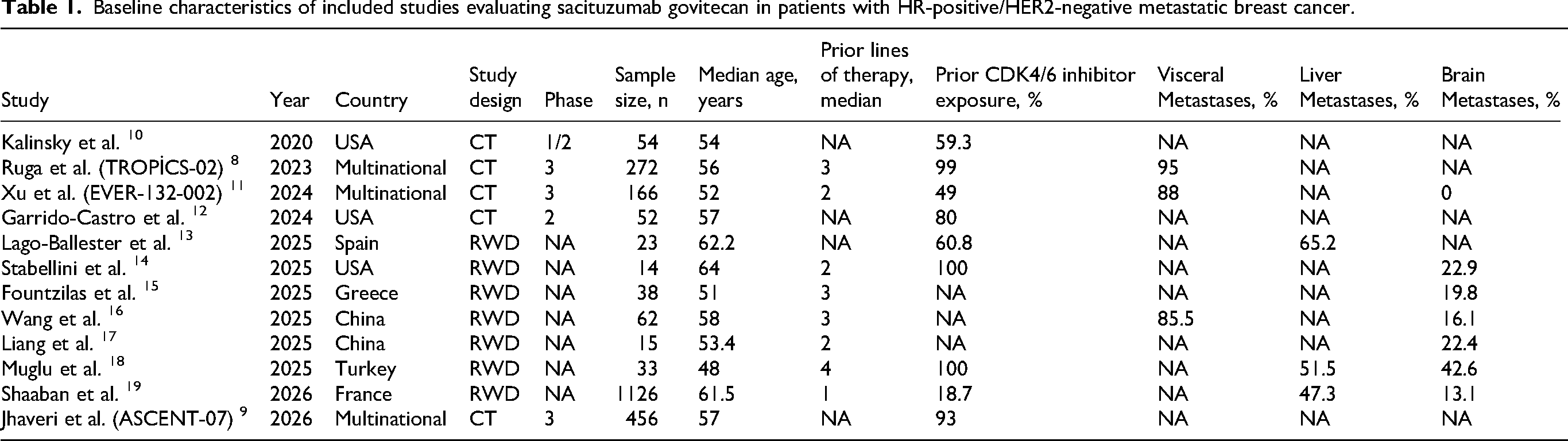
A total of 12 studies comprising 2431 patients were included in the analysis, including 5 clinical trials and 7 real-world studies. The median age across studies ranged from 27 to 81 years, with a median of medians being 56 years. The proportion of patients with prior CDK4/6 inhibitor exposure varied substantially across studies, ranging from 18% to 100%, while the median number of prior treatment lines ranged from 1 to 4. The overall characteristics of the included studies are summarized in Table 1.
Baseline characteristics of included studies evaluating sacituzumab govitecan in patients with HR-positive/HER2-negative metastatic breast cancer.
Pooled analysis of 8 studies including 1091 patients demonstrated an ORR of 23% (95% CI, 17%–31%), with considerable between-study heterogeneity (I2 = 84%), as shown in Figure 2. Similarly, pooled analysis of 5 studies comprising 569 patients yielded a DCR of 68% (95% CI, 52%–80%), again with substantial heterogeneity (I2 = 86%, Figure 3).
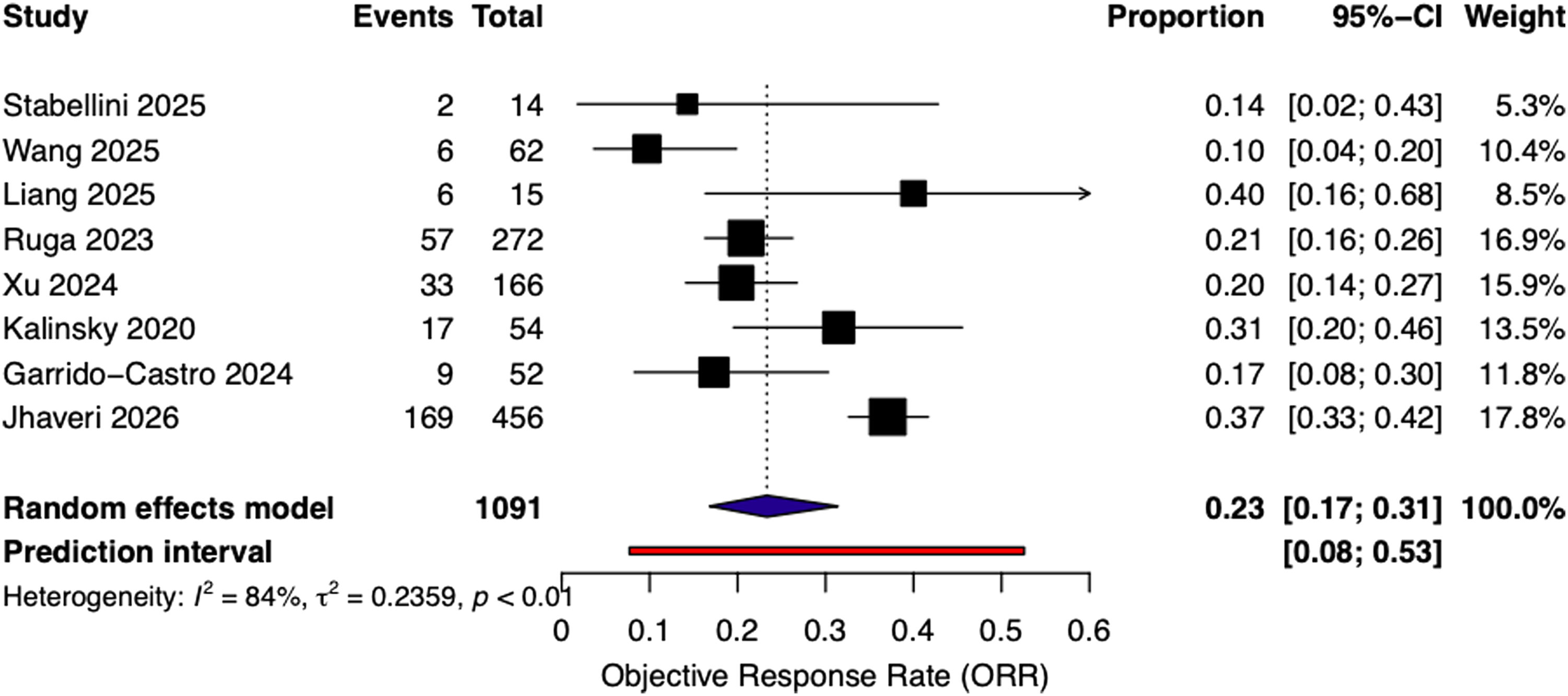
Forest plot of pooled objective response rate (ORR) across included studies using a random-effects model.
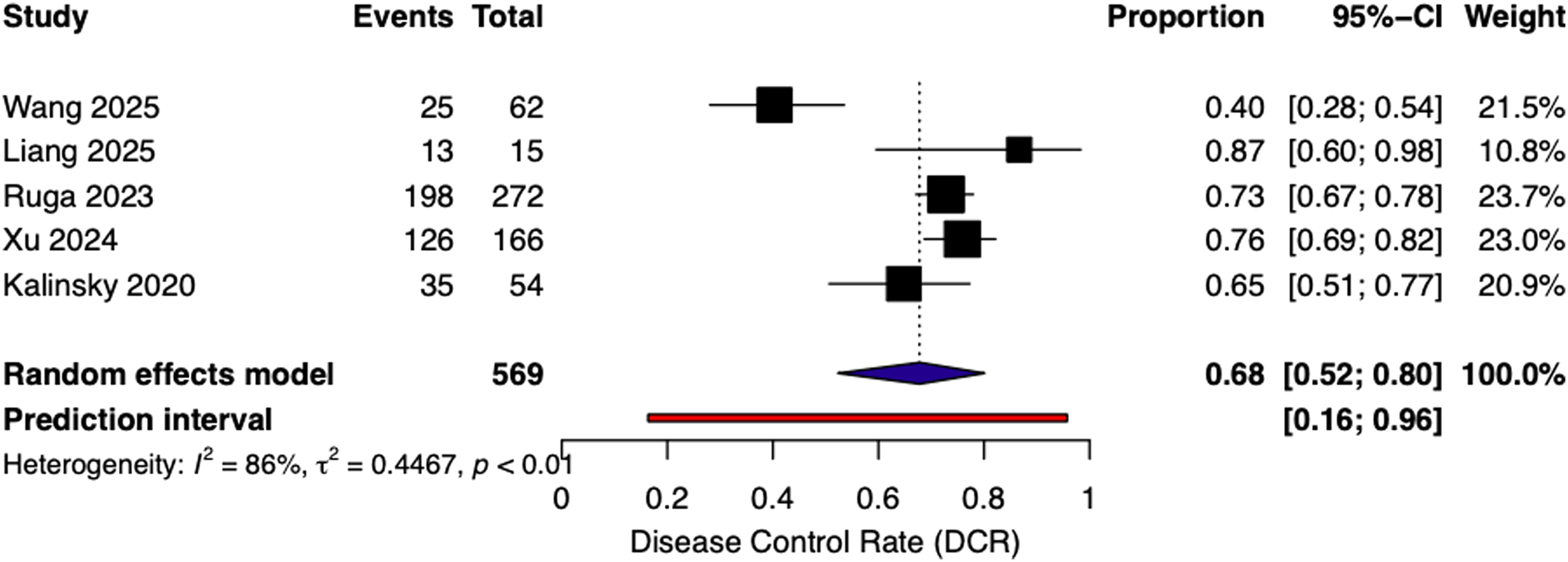
Forest plot of pooled disease control rate (DCR) across included studies using a random-effects model.
Pooled analysis of 7 studies comprising 808 patients evaluating PFS demonstrated a median PFS of 5.35 months (95% CI, 3.96–7.22), with substantial heterogeneity (I2 = 91%), as shown in Figure 4. Although 8 studies reported OS outcomes, only 5 provided sufficient data for quantitative synthesis. Pooled analysis of 5 studies reporting OS included 1508 patients and yielded a median OS of 12.66 months (95% CI, 10.68–15.01), with moderate-to-high heterogeneity (I2 = 72%, Figure 5). Exclusion of the largest study (n = 1126) resulted in an increased pooled OS of 14.16 months (95% CI, 12.95–15.48) with no observed heterogeneity (I2 = 0%), suggesting a substantial influence of this study on the overall estimate.
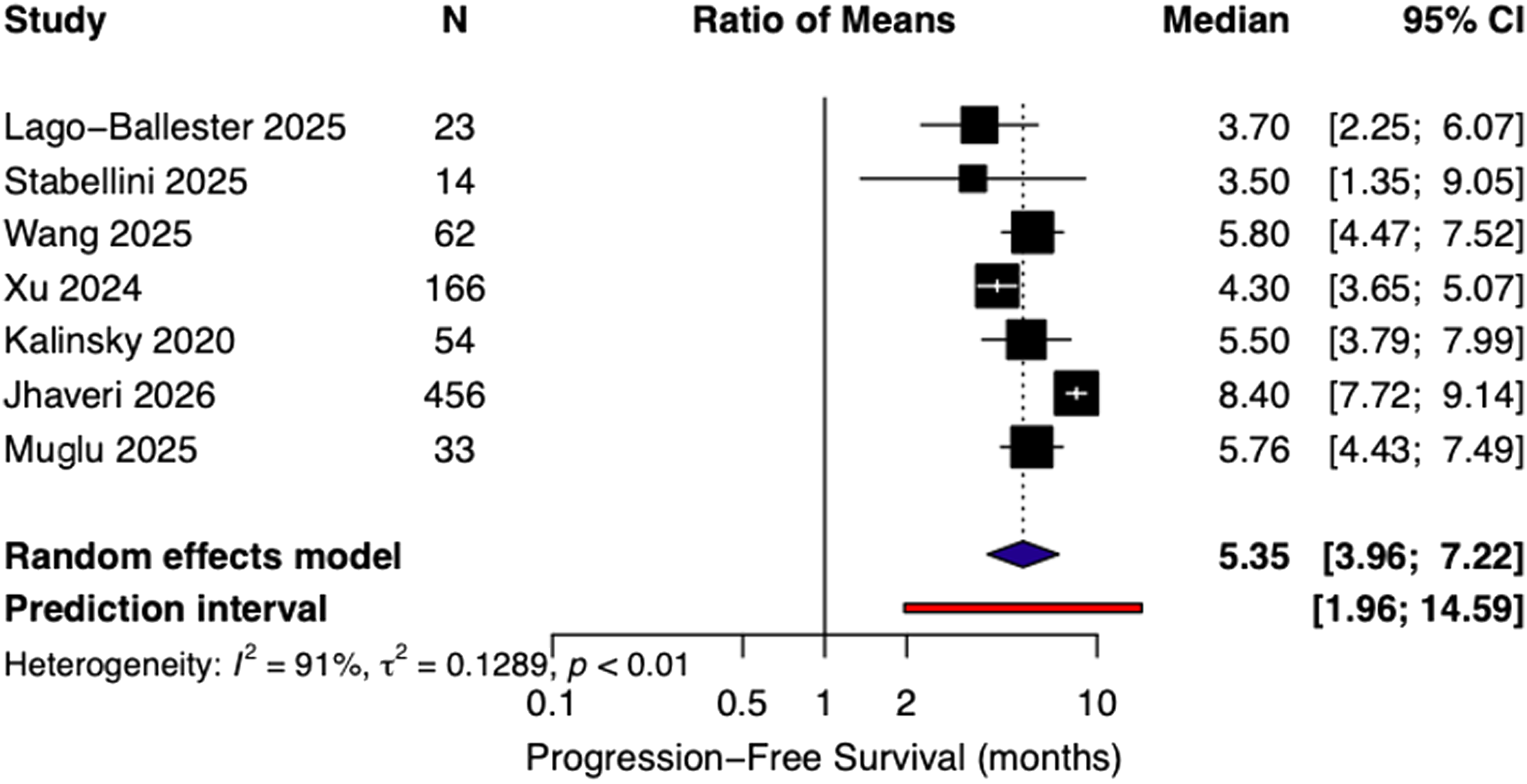
Forest plot of pooled median progression-free survival (PFS) across included studies using a random-effects model based on log-transformed estimates.
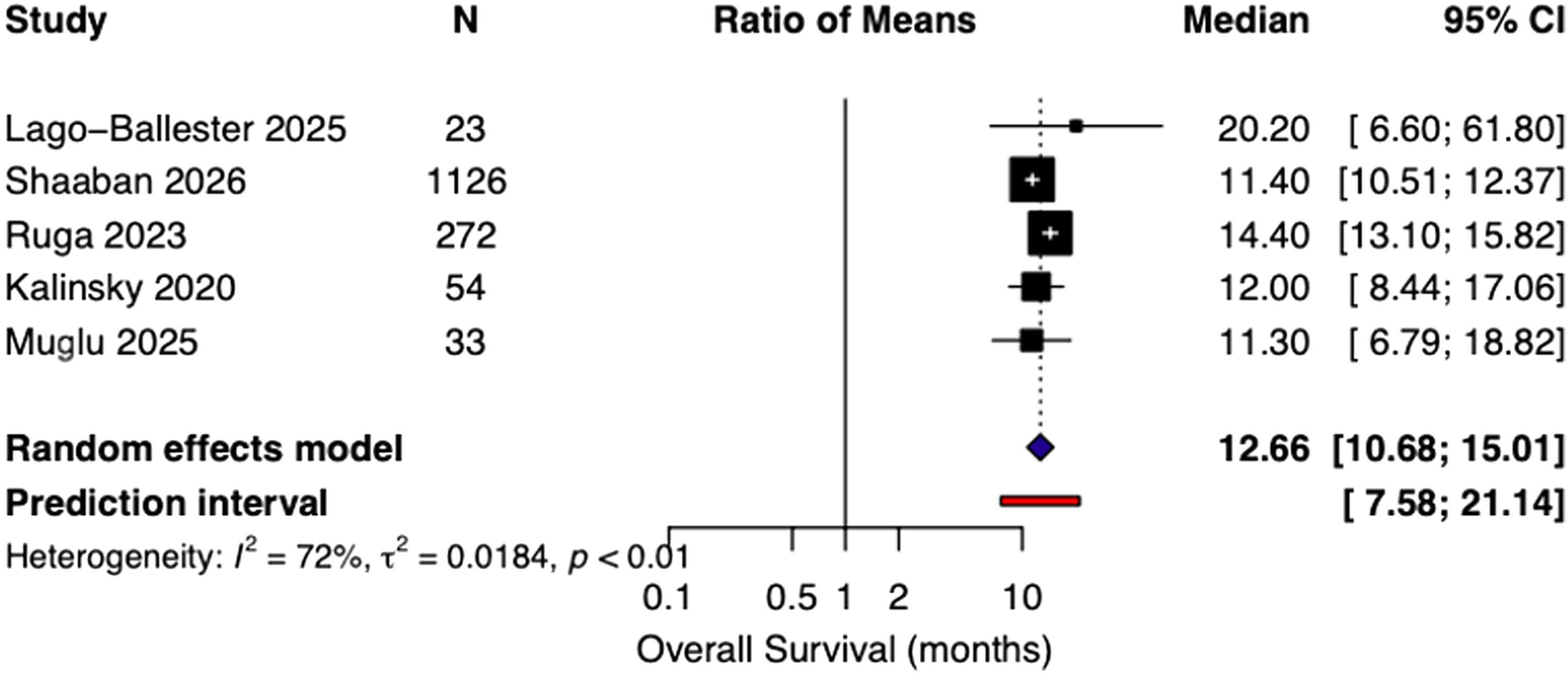
Forest plot of pooled median overall survival (OS) across included studies using a random-effects model based on log-transformed estimates.
Subgroup analyses based on prior CDK4/6 inhibitor exposure (≥80% vs <80%), study design (RWD vs clinical trials), and number of prior treatment lines (1–2 vs ≥3) demonstrated no statistically significant differences in ORR across any of the evaluated subgroups (p = 0.94, p = 0.53, and p = 0.38, respectively). Subgroup analyses are presented in Supplementary Figures S1-S3.
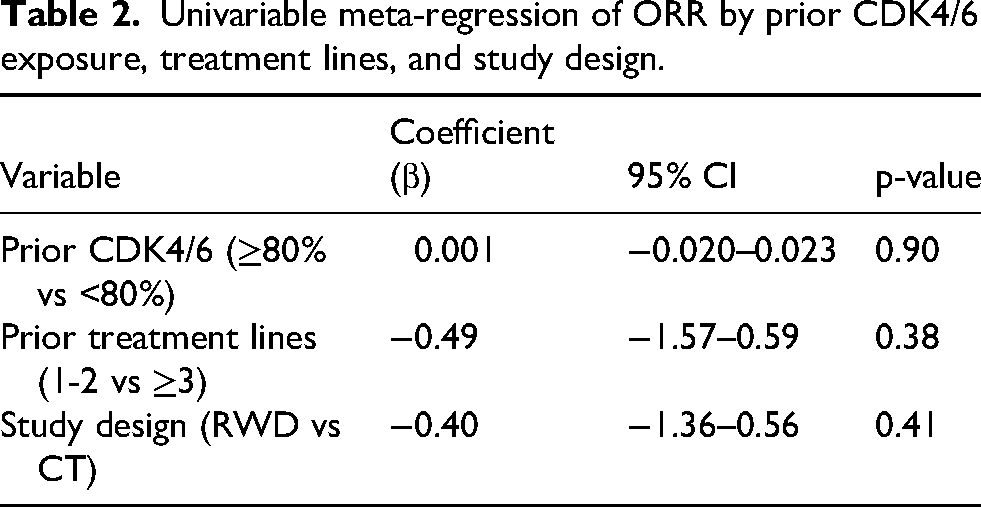
Univariable meta-regression analyses demonstrated no significant association between ORR and prior CDK4/6 inhibitor exposure (β = 0.001, p = 0.90), number of prior treatment lines (β = −0.49, p = 0.38), or study design (RWD vs clinical trials; β = −0.40, p = 0.41), indicating that none of these variables significantly influenced treatment response. Due to the limited number of included studies and missing covariate data across studies, multivariable meta-regression analysis was not performed to avoid overfitting. Table 2 summarizes the findings of the analysis.
Univariable meta-regression of ORR by prior CDK4/6 exposure, treatment lines, and study design.
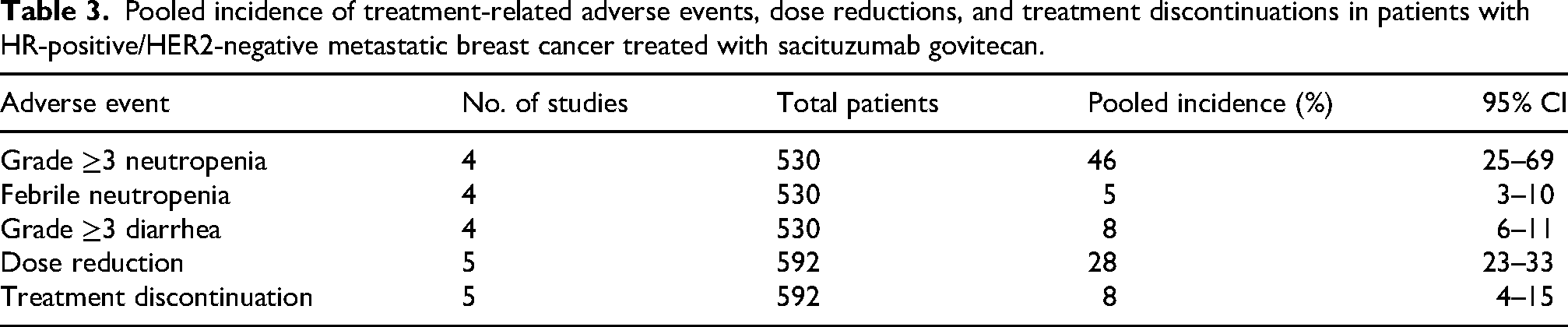
Safety analyses were based on 4 studies including 530 patients for grade ≥3 neutropenia, febrile neutropenia, and grade ≥3 diarrhea, and on 5 studies including 592 patients for dose reduction and treatment discontinuation. The pooled incidence of grade ≥3 neutropenia was 46% (95% CI, 25%–69%), while febrile neutropenia occurred in 5% of patients (95% CI, 3%–7%
Pooled incidence of treatment-related adverse events, dose reductions, and treatment discontinuations in patients with HR-positive/HER2-negative metastatic breast cancer treated with sacituzumab govitecan.
The funnel plot is provided in Supplementary Figure S6. Visual inspection did not demonstrate clear asymmetry; however, interpretation was limited by the small number of included studies (k = 8). Therefore, Egger's regression test was not performed. According to the NOS assessment, most included studies were of moderate-to-high methodological quality; however, the retrospective and heterogeneous nature of several included studies should still be considered when interpreting the pooled estimates
Discussion
This meta-analysis demonstrates that SG provides clinically meaningful antitumor activity in pretreated patients with HR+/HER2− MBC. In pooled analyses, the ORR was 23% and the DCR was 68%, while the median PFS and OS were 5.35 months and 12.66 months, respectively. Subgroup and meta-regression analyses did not detect statistically significant differences in ORR according to prior CDK4/6 inhibitor exposure, number of prior treatment lines, or study design. However, these findings should be interpreted cautiously given the limited number of included studies and the substantial heterogeneity observed across analyses. Overall, the results suggest that SG may retain clinical activity in heavily pretreated patient populations.
In the phase I/II basket study, an ORR of 31.5%, a median PFS of 5.5 months, and a median OS of 12 months were reported with SG in heavily pretreated patients with HR+/HER2− MBC. 10 Similarly, the phase III TROPiCS-02 study demonstrated an ORR of 21%, a median PFS of 5.5 months, and a median OS of 14.4 months, thereby establishing a significant clinical benefit compared to standard chemotherapy. 8 In contrast, the ASCENT-07 study, which evaluated the use of SG in earlier lines of therapy, found no statistically significant difference in PFS according to blinded independent central review (BICR) (HR 0.85; 95% CI, 0.69–1.05; p = 0.130), although a numerical improvement was observed in investigator assessment (HR 0.78; 95% CI, 0.64–0.93; nominal p = 0.008). While OS data were immature at the primary analysis (27% maturity), an early benefit signal in favor of SG was observed (HR 0.72; 95% CI, 0.54–0.97; nominal p = 0.029). 9 These divergent results suggest that while a more pronounced efficacy is observed in heavily pretreated populations (such as in TROPiCS-02), the role of therapy in earlier lines remains to be clarified and outcomes may be more heterogeneous.8–9 In our study, obtaining significant results for PFS and OS in pooled analyses—where diverse patient groups were evaluated together—provides a positive signal regarding the efficacy of SG, yet highlights the need for further prospective data for the optimal positioning of this treatment.
In our study, no significant difference was observed in ORR based on prior CDK4/6 inhibitor use, the number of prior lines of therapy, or study design (clinical trials vs. RWD). Similarly, univariable meta-regression analyses demonstrated that these variables were not significantly associated with treatment response. However, given the limited sample sizes and heterogeneity among included studies, these findings should be interpreted cautiously.
Importantly, the therapeutic landscape of HR-positive/HER2-negative metastatic breast cancer has evolved substantially in the post-CDK4/6 inhibitor era.3–4 Novel targeted therapies including elacestrant for ESR1-mutated disease, alpelisib for PIK3CA-mutated tumors, capivasertib for AKT/PTEN/PIK3CA-altered disease, and PARP inhibitors for germline BRCA-mutated patients have expanded available treatment options and further complicated treatment sequencing strategies.21–25 Since many studies included in our analysis were conducted before the widespread integration of these agents into routine clinical practice, the applicability of our pooled findings to contemporary treatment algorithms may be limited. Prior treatment lines in most included studies were primarily defined according to therapies administered after endocrine resistance, without detailed molecular stratification. Therefore, future studies evaluating sacituzumab govitecan within biomarker-driven and contemporary sequencing approaches are warranted. In addition, the increasing use of antibody-drug conjugates such as trastuzumab deruxtecan in HER2-low and HER2-ultralow breast cancer further complicates treatment sequencing strategies in contemporary clinical practice.26–27 Recent real-world and comparative analyses evaluating trastuzumab deruxtecan and sacituzumab govitecan also highlight the growing need to better define the optimal positioning of these ADCs in biomarker-selected patient populations.28–29
SG primarily causes hematological toxicities (particularly neutropenia and anemia) and gastrointestinal adverse events (particularly diarrhea and nausea).30–32 In our study, the safety data obtained for the HR+/HER2− MBC group are consistent with the literature and demonstrate a similar toxicity profile. Considering that the entire patient population had received multiple prior lines of therapy, these adverse events are generally manageable and acceptable. These findings, in alignment with current literature, support that SG can be safely administered with appropriate patient selection and close monitoring in this late-line setting.
Previous studies have also demonstrated that efficacy and safety outcomes may differ between clinical trial populations and real-world cohorts due to differences in patient selection, comorbidity burden, treatment patterns, and follow-up practices.33–34 Therefore, significant heterogeneity was observed across pooled efficacy outcomes, including ORR, DCR, and survival analyses (ORR I2=84%, DCR I2=86%, PFS I2=91%). This heterogeneity likely reflects differences in study design, patient selection, disease burden, endocrine sensitivity, prior treatment exposure, molecular characteristics, follow-up duration, and the inclusion of both clinical trial and real-world populations. In addition, pooled analyses of median PFS and OS should be interpreted cautiously, as survival estimates may be influenced by differences in patient populations, follow-up durations, and censoring patterns across studies. Although subgroup and univariable meta-regression analyses were performed, substantial residual heterogeneity remained, which may limit the interpretation and generalisability of the pooled estimates. Future studies with more homogeneous and biomarker-driven patient populations may further clarify the factors contributing to variability in treatment outcomes.
The most significant strength of this study is that it provides a comprehensive overview by consolidating data that are scattered and mostly based on small sample sizes in the literature. Furthermore, subgroup and meta-regression analyses did not detect statistically significant differences according to prior CDK4/6 inhibitor exposure or treatment intensity, although these findings should be interpreted cautiously given the limited number of studies and substantial heterogeneity.
This study has several limitations. First, most of the included studies were single-arm with small sample sizes, which may limit the generalizability of the findings. Furthermore, there is notable heterogeneity across studies regarding patient characteristics, prior treatment exposures, and reporting formats. Specifically, pooled analyses of median PFS and OS should be interpreted cautiously, as survival estimates may be influenced by differences in patient populations, follow-up durations, and censoring patterns across studies. These factors may limit the generalisability and robustness of the pooled estimates. As survival data were not standardized across all studies, some analyses could only be performed with a limited number of trials. Additionally, the relatively small number of studies included in the meta-analysis and the lack of data for certain clinical variables restricted the scope of meta-regression and precluded multivariable analysis. Although publication bias was evaluated using funnel plot analysis, the limited number of included studies restricts the robustness of this assessment. Finally, the potential influence of a single large-scale study on the overall pooled results should be considered.
In conclusion, this meta-analysis demonstrates that SG provides clinically meaningful antitumor activity in heavily pretreated patients with HR+/HER2− MBC. Subgroup and meta-regression analyses did not detect statistically significant differences according to prior CDK4/6 inhibitor exposure or treatment intensity; however, these findings should be interpreted cautiously given the limited number of studies and substantial heterogeneity. Within an increasingly complex treatment landscape—including PIK3CA- and ESR1-targeted therapies as well as novel SERDs—the optimal positioning of SG remains to be defined. Further large, prospective studies are warranted to clarify its role in treatment sequencing.
Supplemental Material
sj-docx-1-opp-10.1177_10781552261462434 - Supplemental material for Efficacy and safety of sacituzumab govitecan in hormone receptor–positive metastatic breast cancer: A systematic review and meta-analysis
Supplemental material, sj-docx-1-opp-10.1177_10781552261462434 for Efficacy and safety of sacituzumab govitecan in hormone receptor–positive metastatic breast cancer: A systematic review and meta-analysis by Ali Kaan Güren, Muhammed Fatih Kırcalı, Murat Sarı, Osman Köstek, İbrahim Vedat Bayoğlu and Nazım Can Demircan in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-docx-2-opp-10.1177_10781552261462434 - Supplemental material for Efficacy and safety of sacituzumab govitecan in hormone receptor–positive metastatic breast cancer: A systematic review and meta-analysis
Supplemental material, sj-docx-2-opp-10.1177_10781552261462434 for Efficacy and safety of sacituzumab govitecan in hormone receptor–positive metastatic breast cancer: A systematic review and meta-analysis by Ali Kaan Güren, Muhammed Fatih Kırcalı, Murat Sarı, Osman Köstek, İbrahim Vedat Bayoğlu and Nazım Can Demircan in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-docx-8-opp-10.1177_10781552261462434 - Supplemental material for Efficacy and safety of sacituzumab govitecan in hormone receptor–positive metastatic breast cancer: A systematic review and meta-analysis
Supplemental material, sj-docx-8-opp-10.1177_10781552261462434 for Efficacy and safety of sacituzumab govitecan in hormone receptor–positive metastatic breast cancer: A systematic review and meta-analysis by Ali Kaan Güren, Muhammed Fatih Kırcalı, Murat Sarı, Osman Köstek, İbrahim Vedat Bayoğlu and Nazım Can Demircan in Journal of Oncology Pharmacy Practice
Footnotes
Acknowledgements
The authors have no acknowledgements to declare.
Author contributions
A.K.G.: Writing - Original Draft, Writing - Review & Editing, Project administration, M.F.K.: Conceptualization, Software, Investigation, Resources, M.S.: Validation, Data Curation Writing - Review & Editing, O.K.: Supervision, Writing - Review & Editing, Software, I.V.B.: Supervision, Writing - Review & Editing, N.C.D.: Supervision, Project administration, Writing - Review & Editing
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.