
Abstract
Background
Cancer cachexia is a complex metabolic syndrome that causes a gradual loss of skeletal muscle mass that cannot be fully reversed by normal nutritional support. It has considerable impact on patient's health, but it is still not well-known and well-managed in most cancer care settings. This study sought to investigate healthcare professionals (HCPs) perceptive of cachexia in cancer patients.
Methods
An exploratory qualitative study design was employed. Semi-structured face-to-face interviews were conducted with physicians, pharmacists and nurses working at a specialized cancer care hospital in Lahore. Audio-recorded interviews were transcribed verbatim, and data were analyzed using deductive thematic analysis to identify key themes and sub-themes.
Results
A total of 10 HCPs participated in this study (n = 3 doctors, n = 3 nurses and n = 4 pharmacists). Five main themes were identified: Understanding cachexia, management of cachexia, inter-professional collaboration, needs of patients and families, and quality care of cachexia. Participants generally perceived cachexia as a form of expected or disease-related weight loss, reflecting limited differentiation between pathological cachexia and normal clinical decline. Management approaches were predominantly symptom-driven and largely focused on nutritional interventions. Multi-professional collaboration was described as effective strategy to support patient care. The needs of patients and families were reported to be addressed with sensitivity and structured support. Furthermore, quality management practices demonstrated a proactive orientation, emphasizing organized care processes.
Conclusion
The study concluded that strengthening education, establishing structured care pathways, integrating palliative and supportive care principles can enhance clinician's confidence. Moreover, mitigating conceptual and therapeutic gaps can improve the quality of cachexia care in cancer patients.
Introduction
Traditionally, cachexia has been understood as a symptom rather than a syndrome. However, there is no widely recognized definition of cachexia, and the mechanisms underlying it are poorly understood. 1 Cachexia is a complex metabolic syndrome linked to an underlying illness, characterized by muscle loss, with or without the loss of fat mass. 2 Patients are classified as having cachexia if they exhibit more than 5% loss of stable body weight over six months, or have a body mass index (BMI) below 20 kg/m2 with ongoing weight loss exceeding 2%, or show signs of sarcopenia with ongoing weight loss exceeding 2%. 3 It frequently co-exists with differential diagnoses like malnutrition, anorexia, and sarcopenia. Pre-cachexia, cachexia, and refractory cachexia are the three stages of cancer cachexia (CC) progression. The stage in which it seems impossible to reverse weight loss is known as refractory cachexia. 4 Although the research on CC 5 is increasing, little is known about its underlying mechanisms, and there are only few effective treatment options available. 6
Cancer is the leading cause of death globally, with an estimated 12 million cancer-related deaths expected by 2028. 2 Reports indicate that between 10% and 50% of patients with cancer suffer with cachexia. 7 Reduced tolerance to current cancer treatments, increased treatment-related toxicity, and frequent therapy delays are all associated with CC. Additionally, it is an independent predictor of patient survival.8,9
Beyond its physiological impact, CC also produces significant psychological and social consequences for patients and their families.10–12 Physically, progressive muscle wasting results in severe weakness, fatigue, and a marked reduction in physical functioning, which limits the patient's ability to perform daily activities and reduces quality of life (QOL).3,13 In addition, the visible weight loss and physical deterioration associated with cachexia may negatively affect a patient's body image and emotional well-being, often leading to social withdrawal and psychological distress.12,14 Furthermore, patients’ QOL is greatly reduced by the ensuing decline in physical, social, and psychological functioning, 5 and caregivers experience emotional distress because they frequently interpret this as a sign of impending death. 15 Although CC is a prevalent and crippling condition, 16 for many cancer patients, their evaluation and treatment are still largely unmet. Such circumstances may lead to emotional conflict during an already difficult period of illness, indicating that the burden of cachexia extends beyond the patient and affects the entire family.17,18 Despite increasing awareness of its clinical significance, effective management of CC remains challenging, and multiple therapeutic strategies continue to be explored to reduce its impact on patient outcomes. 19
Literature have indicated that enhanced knowledge can increase healthcare professionals (HCPs) confidence in discussing CC with patients and their families. 20 The adoption of a holistic approach to CC care is influenced by cultural factors and available resources. 12 Several qualitative studies have described the experiences of patients and their family caregivers. 21 Although these studies highlight the need for more focus on CC, little is known about how HCPs view the management of CC, and no such studies have been conducted in Asia. Thus, this study aimed to investigate the perception of HCPs regarding CC, making a significant contribution to the understanding and development of context-specific strategies for CC management in Pakistan, where such research is currently lacking.
Methodology
Ethical approval
The study approval was taken by the institutional review board (IRB) of specialized cancer care hospital, Lahore, Pakistan (IRB#25-49). The IRB review process of hospital complies with International Council for Harmonization - Good Clinical Practice (ICH-GCP) guidelines.
Study design
An exploratory qualitative study design was adopted to understand and explore participant's perception and their subjective experiences about CC. A face to face semi- structured interviews were taken by Principle investigator who was the hospital pharmacist with relevant clinical and research experience in oncology practice between September 1st 2025-December 30th, 2025. The reporting of the results follows the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist. 22
Study centre and population
Participants were recruited from cancer speciality hospital of Lahore. It includes doctors from medical oncology and internal medicine, nursing staff from palliative and inpatient adult care, and pharmacists, including senior and managerial staff responsible for cancer care with more than one year of clinical experience in managing cachexia.
Participants sampling and inclusion criteria
HCPs who were actively involved in oncology care units of hospital such as doctors, nurses, and pharmacists with at least one year experience were included. Participants having no direct experience in oncology patient care, administrative and other non-clinical staff were excluded. A purposive sampling technique was employed to recruit the participants. Interviews were continued until the point of data saturation was reached. Saturation was attained at tenth interview. Among ten HCPs interviewed, there were four pharmacist while there were three physicians and three nurses. The uneven distribution among participants reflected that pharmacists were more readily accessible and available for participation during the study period. Despite this imbalance, all professional groups contributed to all major themes, and their perspectives demonstrated considerable convergence on key aspects of CC management.
Data collection
A pre-designed validated interview guide was adapted with permission from prior research. 20 The interview questions focused on CC, such as interpreting cachexia, managing cachexia, multi-professional working, needs of patients and families, and perspectives on quality care of cachexia. Potential participants were contacted via appointment and verbally invited to participate in the study. Written informed consent was obtained from participants before interviews, and their names were coded to ensure confidentiality. All interviews were conducted in English language and each interview lasted between 15 and 35 min. Probing questions were used and they were encouraged to freely share their thoughts. Interviews were conducted in a private office to ensure confidentiality and were recorded before transcription for analysis.
Data analysis
The recorded interviews were transcribed verbatim and, where needed also transcribed in English. Minor grammatical changes were made while preserving the integrity of the original content. Initially data coding and deductive thematic content analysis were carried out using Braun and Clarke's method. 23 The analysis was conducted independently by three researchers. Transcripts were read repeatedly to achieve familiarization with the data. Meaningful segments of text were then systematically coded in alignment with the research objectives. Codes with conceptual similarities were grouped into themes, and sub-themes through an iterative analytical process manually. During the analytical process, overlapping concepts were refined and reorganized to improve thematic clarity and interpretive depth. The analysis focused on identifying recurring patterns, perspectives, and experiences related to CC management among HCPs. Reflexivity was maintained throughout the data collection, whereby researchers continuously reflected on their assumptions, professional background, and potential influence on data interpretation. To minimize subjective bias, researchers independently coded a subset of transcripts and held regular peer debriefing sessions to discuss code definitions, resolve discrepancies, and reach a consensus which further enhances analytical rigor. This strategy supported the credibility and trustworthiness of the analysis by ensuring that interpretations were grounded in participants’ accounts rather than the researcher's prior assumptions.
Results
Basic demographics of participants
Basic demographic characteristics of HCPsare shown in the Table 1.
Participants basic demographics.
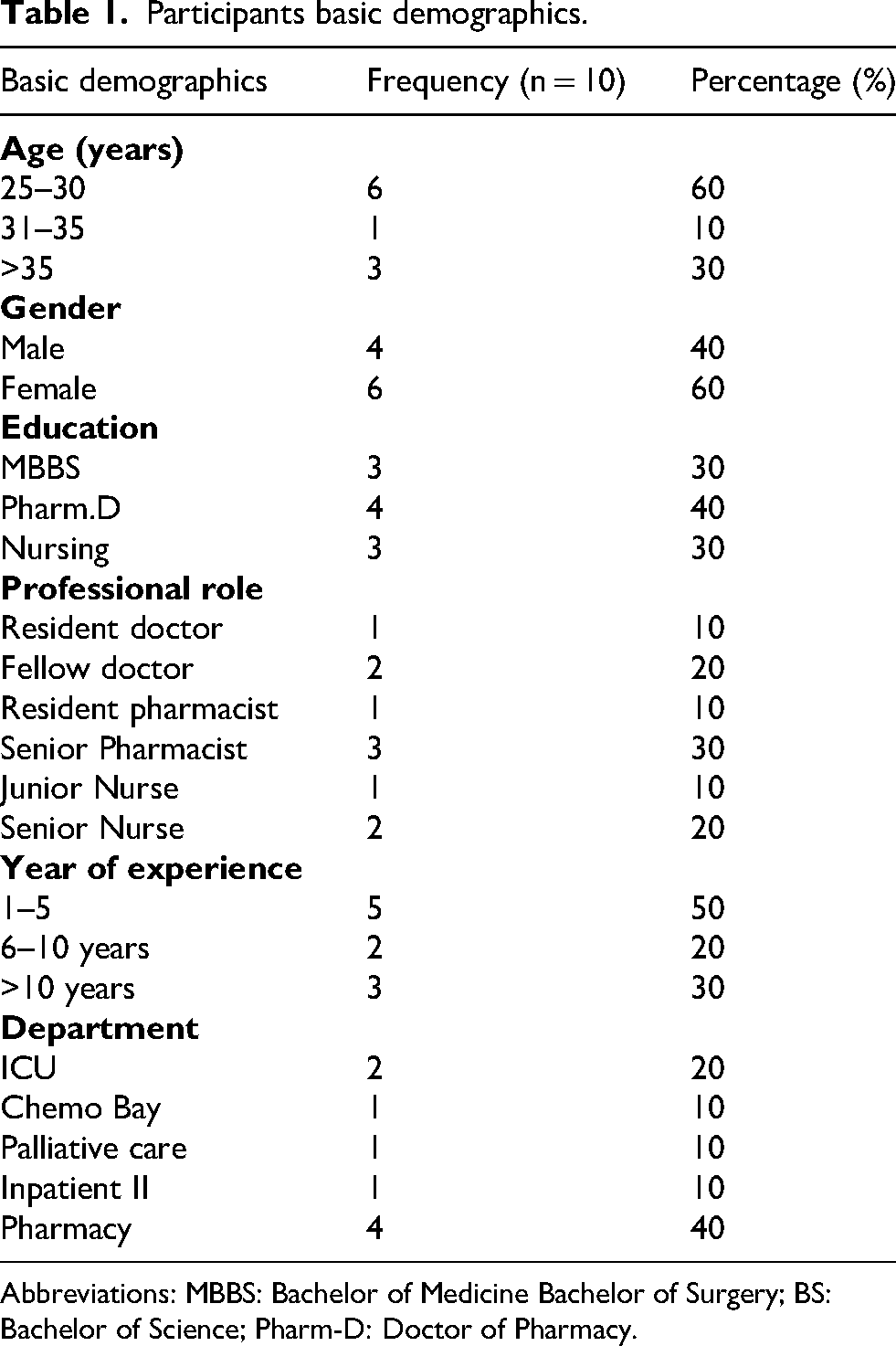
Abbreviations: MBBS: Bachelor of Medicine Bachelor of Surgery; BS: Bachelor of Science; Pharm-D: Doctor of Pharmacy.
Thematic content analysis
The 5 main themes including understanding of cachexia, management of cachexia, inter-professional collaboration, needs of patients and families and quality care of cachexia were divided into subthemes for detailed investigation.
Understanding of cachexia
HCPs demonstrated shared pattern of understanding about cachexia as a syndrome that is characterized by progressive physical decline and weight loss. Although a common perspective described by HCPs was that cachexia represent both physical deterioration and a marker for disease worsening status.
Weight loss and wasting
Respondents described cachexia through an observable physical manifestations and their daily clinical experiences. Oncologists referred to a diagnostic criteria and clinical definition, whereas nurses and pharmacists focused on functional decline and visible weight loss.
“It reminds me of its definition, which is more than 10 percent of weight loss in 6 months of duration”. (D2)
“When I hear the term cachexia, I immediately think of severe unintentional weight loss combined with muscle wasting.” (N3)
The pharmacist additionally highlighted a broader understanding that goes beyond nutritional deficiency alone.
“It is an unintentional weight loss, occurs in terminally ill patients. It is a metabolic syndrome associated with underlying disease and weight loss is not only attributable to anorexia and malnutrition.’’ (P2)
Poor prognosis
Beyond physical deformation, cachexia was viewed as an indicator of disease progression and declining survival prospect.
“ In advanced cancer, when I think about cachexia, I see a weak patient with poor prognosis having dehydrated skin, who has difficulty in moving, wrinkles all over his body due to dehydration and lack of fluids.’’ (N1)
“Poor prognosis, impaired life, short duration of life expectancy, and then he needs support.” (P1)
Management of cachexia
Participants responded that complete reversal of cachexia is difficult in cancer patients therefore management strategies are directed towards symptom control, supportive care and nutritional optimization.
Nutrition and symptom management
Participants viewed cachexia management as a shared responsibility requiring input from multiple healthcare disciplines.
“We provide comfort care management, which involves relieving the patient's symptoms so they can pass away without feeling much pain and maintaining quality of life rather than reversing weight loss. We collaborate closely with the dieticians, physicians, and families to support the patient.”(N1)
“If a patient with significant weight loss is admitted, we observe him and do consultation with clinical nutritionist and a psychologist. That provides them with both emotional and nutritional support.” (D1)
“First, we focus on nutritional support. As we cannot reverse the condition, but we can provide enteral feeding, TPNs, oral supplementation, and anything else that can improve it.’’ (P4)
Awareness of interventions
Nutritional support was emerged as a frequently reported intervention for patient with cachexia. Participants emphasized on enteral feeding, appetite stimulants and dietary consultations.
“As part of my profession, I am responsible for verifying prescriptions, and most are weight-based. For cachectic patients, the medication should be optimised through appropriate dosing, to ensure that patients with cancer and weight loss receive appropriate weight based dosing.’’ (P4)
Respondents stated that they actively managed their cachexia while acknowledging the complexity and limitations of the interventions that were available.
“In the assessment, there are some criteria mentioned that we can use to identify cachexia including BMI, or weight recording for the previous 6-month duration. And for interventions, referrals to a clinical psychologist and a nutritionist, as well as a PEG tube to support nutrition in advanced cancer patients.” (D1)
Interprofessional collaboration
Respondent valued interdisciplinary support in the cachexia management by working together to improve patient care. Although each professional identified a distinct responsibility by keeping in view the importance of teamwork and coordinated care in patients with cachexia.
Professional responsibility
Participants emphasized that providing patient care is their core responsibility on an individual level and also when working in Multi-disciplinary teams.
“I think early identification of a patient who has cachexia, identifying the complications that arise from cachexia, and starting nutrition and managing it vigorously and referring to a specialist who is dealing with these kinds of problems, is important.”(D2)
“As a pharmacist, it's basically related to medication, and the most essential thing in supporting the patient with cachexia is definitely the need for optimised therapy, which absolutely reflects my profession and not to harm the patient further in terms of overdosing.”(P3)
Collaborative approach
Respondents described cachexia management as a collaborative process focused on achieving shared therapeutic goals, which guided the planning and delivery of patient care.
“We work with multi-disciplinary team, which includes physicians, dieticians, physiotherapists, psychologists and other social workers. The dietician helps create individualised food plans, while psychologists support patients coping with body image changes, depression, and family meetings with the entire team help align the goal and reduce unrealistic expectations.”(N3)
Collaborative working was perceived as essential for addressing the multifaceted challenges associated with cachexia and ensuring comprehensive patient care.
“As part of the multidisciplinary healthcare team, I collaborated with physicians and nutritionists to develop a nutritional chart that helped pharmacists optimize interventions, support dose-related decisions, and provide effective counselling on nutritional supplement use.” (P1)
Needs of patients and families
Disease burden on patient
Respondents highlighted that with cachexia, patients experience substantial psychological, physical, and emotional burden.
“It is an issue, a problem in advanced-stage cancer because there is a massive disease burden. Patient is emaciated, so it is difficult to give them treatment, and most patients are not able to afford it. So it has become a significant setback for treatment and management” (D3)
Respondents also emphasized that patients not only carry disease burden but also face additional treatment and medication-related side effects, as this condition involves multiple interactions, not limited to disease but also to drug as well.
“This is a problematic because cancer patients are already immunocompromised and struggling with multiple medications that have significant side effects. With weight loss, their bodies become weaker and less able to tolerate high-potency treatments. This ultimately compromises their lifestyle and overall quality of life.’’ (P1)
Assessment of patient's family needs
Respondents highlighted a clear need for patients and their families to receive accurate information about cachexia that is tailored to their level of understanding, as misconceptions are often related to heightened anxiety for both patients and their families.
“Informing them and updating them on what cachexia is as it is a part of the big picture of underlying illness not only a consequence of reduced appetite.” (D3)
“Families often believe that increasing intake will resolve the problem, and they feel guilty when the patient cannot eat. Helping them understand cachexia as a medical condition, not neglect, reduces emotional distress. Managing symptoms, ensuring dignity, and maintaining patients’ comfort are central to my job.” (N3)
Families find it challenging to deal with the emotional effects of continuing weight loss and functional impairment.
“I am continually engaged in verification processes, so I am well aware of the medication process, proper dosing, and nutritional support. If I know how to counsel a patient properly, I will be better able to advise him on how to take them, and I know indeed it would, in turn, benefit the patient more.”(P1)
Quality care of cachexia
Quality of life of patients
Respondents emphasized that multidisciplinary coordination is essential to the successful integration of palliative and supportive care. The availability of specialized supportive services combined with interventions that preserve comfort, dignity, and quality of life.
“Ultimately, quality cachexia management is about comfort, dignity, education, and maintaining the best possible quality of life for patients.” (N1)
Follow up care of patients
Doctors, nurses and pharmacist consistently highlighted the importance of nutritionist as central member of cachexia care pathway. To facilitate wider implementation, participants acknowledged that this approach was not consistently available across other services and emphasized the need for more structured education and system-level support.
“Nutritionists regularly review patients during hospital stays, provide follow-up care through outpatient clinics, and offer telemedicine consultations. This ensures ongoing nutritional support and guidance, allowing patients to discuss their needs from home and continue appropriate supplement use between hospital visits.”(D3)
Theoretical framework illustrating factors influencing the cachexia perception among healthcare provider
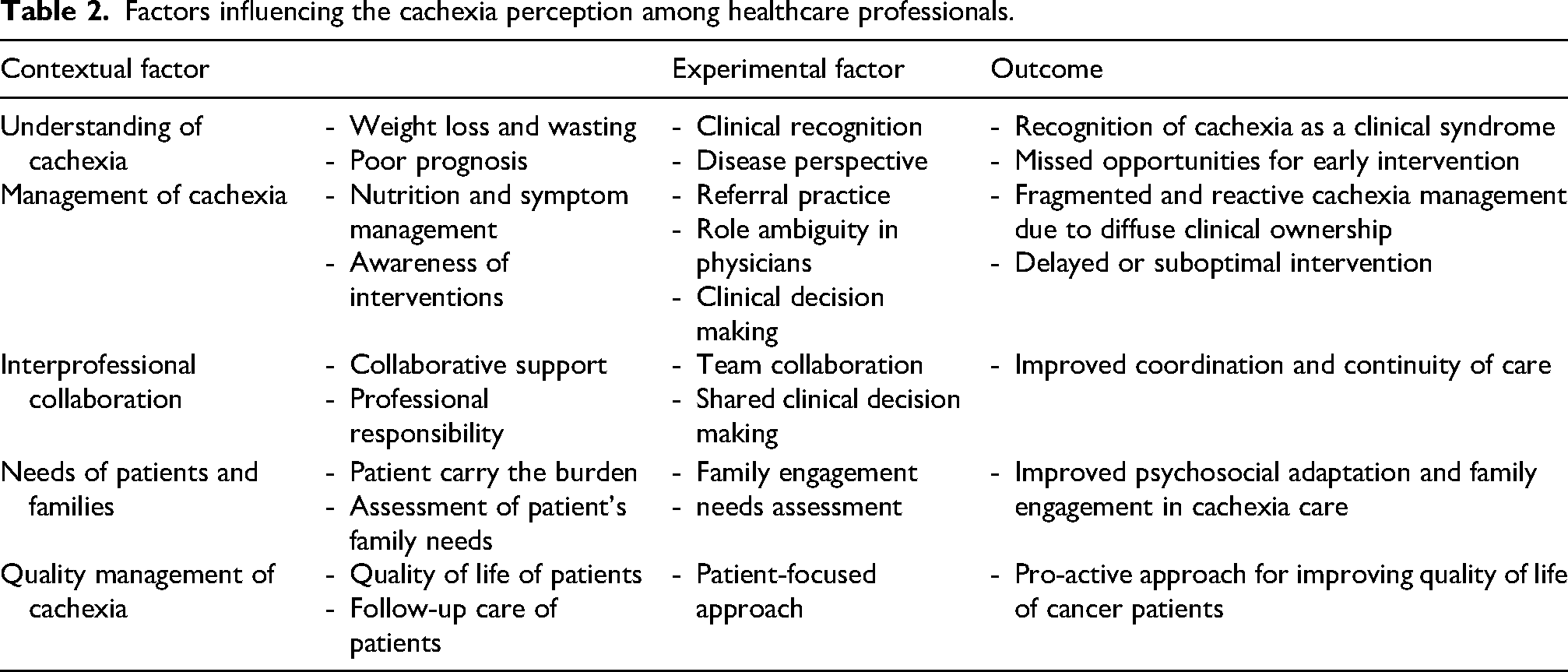
Table 2 shows the conceptual framework developed from the reflexive thematic analysis of the perspectives of HCP's regarding CC and reflects the progression from participant narratives to codes, sub-themes, and final themes. The framework illustrates the interconnected relationships among these themes and demonstrates how they collectively influence CC management. The contextual factors are the major perspective that influences cachexia care, and the experimental factors are the processes, actions and professional practices adopted in clinical setting. The outcomes represents perceived effect of these practices on patient care and service delivery.
Factors influencing the cachexia perception among healthcare professionals.
Recommendations by health care professionals for managing cancer cachexia
Overall recommendations provided by HCPs regarding management of CC are shown in Figure 1.
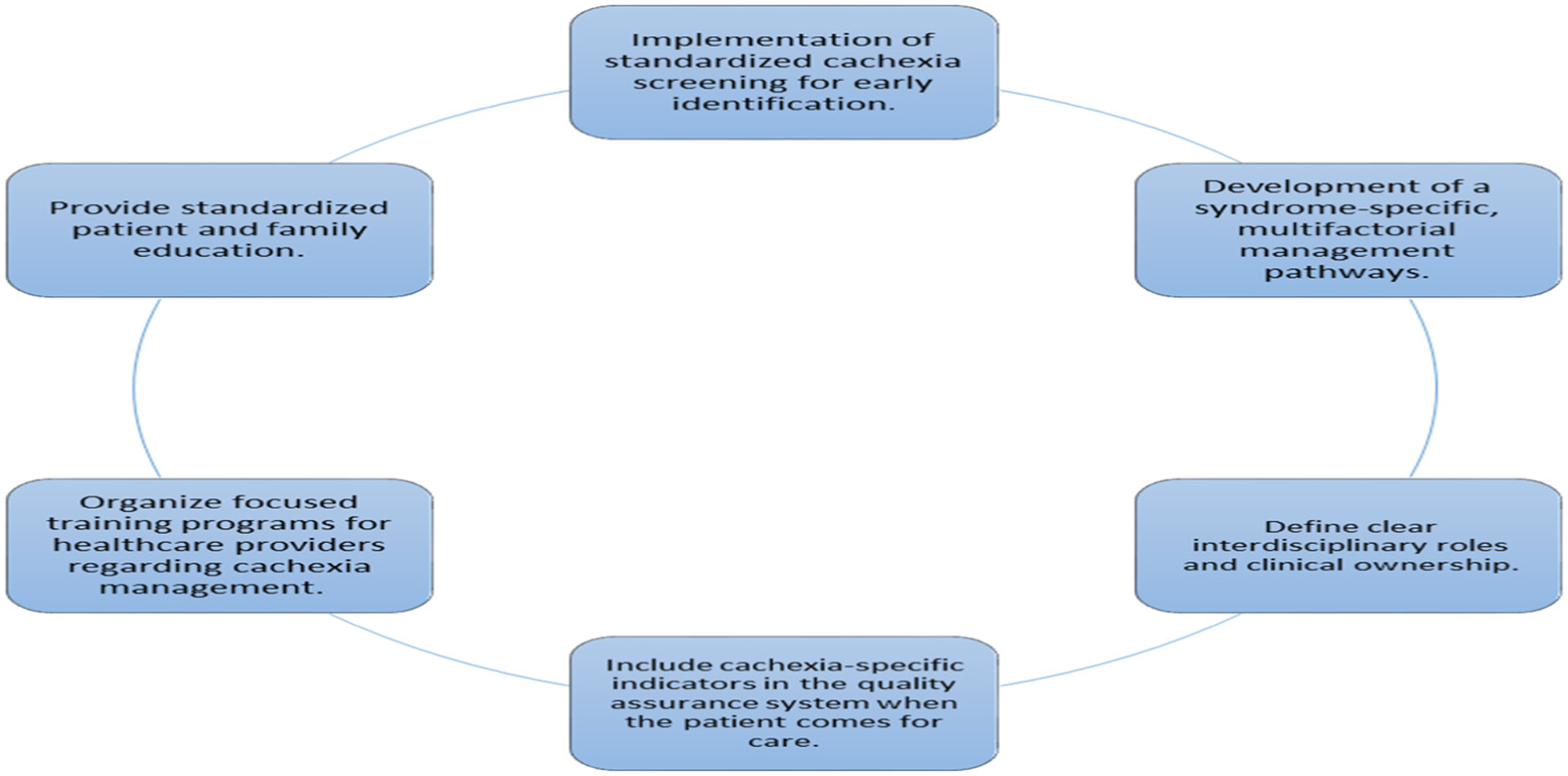
Recommendations for managing cancer cachexia.
Discussion
The present study highlights the influence of educational opportunities, clinical culture, and organizational context on the care of patients with advanced cancer. Despite limited formal education in cachexia management, participants in this study demonstrated an ability to address the condition through experiential learning gained in clinical practice. The results are in line with previous research 20 that examined the benefits of a cachexia clinic in an Australian hospital. Both studies show that knowledge, clinical culture, access to specialized support, and organizational structures influence how HCPs respond to cachexia, despite the differences in the contexts. The extent of knowledge of the causes and treatment of cachexia in advanced cancer was different among participants in this study. Physicians most frequently described cachexia in terms of diagnostic and clinical criteria, especially percentage weight loss and nutritional decline. Such observations have been reported previously 24 that physicians frequently identify cachexia only when clinically significant weight loss occurs. Nurses emphasized functional consequences such as weakness and decreased mobility, consistent with findings that nurses often recognize cachexia through daily observations of the patient and functional impairment. This finding is consistent with previously reported 25 that nurses often identify cachexia through long-term observation of physical and functional decline of their patients during routine care. Pharmacists recognized that cachexia had a metabolic basis and can be distinguished from simple starvation or anorexia. This finding is concordant with proposed international consensus definition 3 that CC is a multifactorial syndrome characterized by ongoing loss of skeletal muscle mass with or without loss of fat mass that is not fully reversible by conventional nutritional support. 3 Previous study, 24 have also reported that cachexia was mainly recognized by HCPs based on visible weight loss and physical deterioration instead of its metabolic pathophysiology.
Regarding management of cachexia participants recognized that cachexia is challenging to reverse in advanced cancer and therefore requires coordinated interventions aimed at minimizing functional decline and improving patient comfort. A key component of this was holistic assessment, as it was recognized that patients with cachexia need a multidisciplinary approach to their care that considers the complex bio-psychosocial impact of the syndrome. 25 The HCPs holistic assessment is necessary as reported previously, 26 which suggested that patients and families only discuss psychosocial concerns if these issues are raised by their HCPs. Hence, the absence of holistic assessment could result in under-recognition of the full multidimensional impact of cachexia. Physicians frequently described referring patients to nutritionists and psychologists, reflecting recognition that cachexia requires expertise beyond tumour-directed treatment. Similar findings were reported in literture, 27 that multidisciplinary involvement is essential for addressing the complex nutritional, psychological, and social consequences of cachexia. International guidelines from the European Society for Clinical Nutrition and Metabolism (ESPEN) also recommend multidisciplinary management involving physicians, dieticians, nurses, psychologists, and palliative care specialists. 28
Nurses emphasized continuous patient monitoring, skin care, symptom assessment, and family support. The experiences reported by nurses are particularly important because symptoms such as mucositis, nausea, pain, and fatigue are well-established contributors to reduced nutritional intake and progressive weight loss among patients with advanced cancer. 28 Pharmacists described their contribution through medication review, weight-based dose adjustment, and participation in multidisciplinary discussions. Previous studies have similarly highlighted the expanding role of oncology pharmacists in supportive cancer care and optimization of pharmacotherapy among nutritionally compromised patients. 29 Participants acknowledged the need for collaborative care models, which is consistent with current recommendations advocating integrated supportive care pathways for patients with CC. 3 The predominance of weight loss and wasting in patients related data suggest that cachexia continues to be recognized primarily at later stages, when physical manifestations are clinically apparent. This observation is relevant as early metabolic changes often precede visible weight loss and delayed recognition may reduce opportunitiess for timely intervention. 28
In order to support patients and caregivers, a multidisciplinary approach to CC is encouraged. The effectiveness of this approach depends on the active participation of all clinical disciplines. 30 The study participants signifies working with other allied HCPs to treat the psychological and physical aspects of cachexia. This result is in strong agreement with previous finding 20 that described multidisciplinary approach as an essential measure to the cachexia clinic's success. Furthermore, the importance of delivering coordinated, patient-centred care is reflected in another study, 31 where respondents reported increased awareness of the beneficial impact of supportive care measures. Participants believed that increased awareness facilitated a more inclusive and multidisciplinary approach to communication with patients and carers. From this perspective, such findings underscore the value of integrating supportive care within collaborative clinical frameworks to enhance patient and caregiver engagement.
Previous research indicated that many HCPs find communicating with patients and their families about cachexia difficult32–34 and could lead to uncomfortable discussions about end-of-life issues. Literature have consistently reported the importance of open conversations with patients and families about end-of-life concerns to allow time to prepare for impending death. The best evidence suggests that a comprehensive, patient-centered approach that takes into account all aspects of care is necessary to effectively address the needs of this patient group.20,35 To help patients and families understand cachexia and lessen feelings of guilt, conflict, and helplessness, it is important for medical professionals to provide sensitive and clear information. 36
Overall, the findings of this study support and extend existing research by reinforcing the critical role of education, experiential learning, and multi-professional collaboration in shaping HCPs responses to cachexia. The findings suggest that although HCPs may recognize weight loss and loss of appetite as consequences of cancer, there is a failure to recognize CC as a negative prognostic factor. Patients are diagnosed late in their history of disease, and at this time, the impact of CC on both QOL and treatment outcomes may already be profound. Another factor that contributes to sub-optimal CC management is the lack of awareness of simple tools to identify patients with CC symptoms (e.g., standardized tools for body weight loss and appetite). A recent study 29 has shown the urgent need for a standardized symptom assessment tool to identify patients at risk earlier in the course of the condition. 37 Moreover, the persistence of challenges across different healthcare settings suggests that reliance on specialist clinics alone may not be sufficient. Integrating cachexia education into undergraduate and postgraduate training, alongside system-level support for collaborative practice, may be necessary to ensure consistent, high-quality care for patients with cachexia and their families. Consistent CC management practices across institutions may be supported by the creation of locally tailored clinical guidelines.
Conclusion
This study demonstrates that CC is a common and clinically significant syndrome among patients undergoing cancer treatment, with important implications for patient outcomes and quality of care. The findings indicate that limited awareness and understanding of cachexia among HCPs may hinder timely recognition and effective management. Addressing CC requires a coordinated, multidisciplinary approach supported by appropriate training and clear communication with patients and their families. Strengthening education, integrating supportive care, and developing locally relevant management strategies may enhance the quality of cancer care for patients affected by cachexia.
Study limitation
This study has few limitations. A relatively small sample recruited from a single specialized oncology setting may limit the transferability of the findings to other healthcare contexts. Furthermore, participant representation across professional disciplines was uneven. However, the study aimed to obtain in-depth exploratory perspective regarding HCP perspectives on cancer cachexia within a resource-limited clinical setting.
Impact statement
The study highlights critical gaps in the recognition and management of cancer cachexia among healthcare professionals and emphasize the need for standardized assessment and care pathways.
The results favor the incorporation of multidisciplinary and supportive care models to enhance patient outcomes and quality of life in oncology settings.
Footnotes
Acknowledgements
The author would like to extend sincere thanks to all participants and for their cooperation and support and to the Institutional Research Board of Hospital for allowing the conduct of this study.
Author's contribution statement
ZA and SK conceptualized study, MK collected data. OUS, ZA, SK, SM and OAB interpreted results. MK wrote initial draft of manuscript. All authors reviewed and approved the final draft of manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.