
Abstract
Background
Manual chemotherapy compounding carries occupational hazards and requires high technical accuracy. Robotic automation has emerged as an important advancement to enhance personnel safety and improve dosing precision.
Objective
This study evaluated the impact of syringe size and compounding cycle number on accuracy, operational efficiency, and safety margins of a prototype two-arm robotic chemotherapy compounding system during its first year of clinical implementation at Maha Vajiralongkorn Thanyaburi Hospital, Pathum Thani, Thailand.
Methods
A retrospective analysis of 7,922 intravenous chemotherapy preparations was conducted. Preparation accuracy was assessed using percentage volume error determined by gravimetric verification, and efficiency was measured by total preparation time. The effects of syringe size (10, 30, and 50 ml) and compounding cycles (one to three) were analyzed. Bootstrap resampling was applied to generate 90% confidence intervals and evaluate safety margins.
Results
The system demonstrated high precision, with an overall mean percentage error of −1.19 ± 1.32% (median −1.14 ± 1.86%) and a mean preparation time of 11.86 ± 3.47 min (median 11.29 ± 3.06 min). Smaller syringe sizes and increased compounding cycles were associated with a consistent tendency toward slight under-delivery. However, all deviations remained within the clinically acceptable ±5% threshold. Bootstrap analysis confirmed stable and reproducible safety margins across hardware configurations.
Conclusion
Clinical implementation of the robotic compounding system demonstrated high accuracy, reproducibility, and operational safety, supporting its role in enhancing safety in high-throughput chemotherapy compounding practice.
Background
Chemotherapy remains a cornerstone of modern cancer treatment, yet its manual preparation is fraught with challenges that place both healthcare workers and patients at risk.1–4 The cytotoxic nature of these agents necessitates stringent handling protocols to prevent occupational exposure,5,6 while the narrow therapeutic windows of many drugs demand uncompromising precision in dosing.7–10 As the demand for cancer care continues to grow globally, automation has emerged as a critical area of innovation, offering a technological solution to enhance the safety, accuracy, and efficiency of pharmacy operations.11–14
The manual compounding of injectable chemotherapy presents a dual challenge. First, there are significant occupational hazards associated with handling cytotoxic agents. Previous studies have consistently confirmed environmental contamination in preparation areas and have detected cytotoxic residues in the urine of exposed personnel,15–24 highlighting the long-term health risks, including reproductive toxicity and genotoxicity.25–27 Second, patient safety is critically dependent on dose accuracy. Even minor deviations from the prescribed dose can compromise therapeutic efficacy or lead to severe toxicity, 28 directly impacting patient outcomes.
Robotic chemotherapy compounding systems have been developed to directly address these challenges. These sophisticated platforms integrate advanced functionalities such as gravimetric control for weight-based dose verification,29–34 barcode scanning to ensure the correct drug and diluent are used,29–36 and closed-system transfer devices to contain hazardous aerosols and vapors.37,38 Previous international studies have validated the reliability of these systems, consistently demonstrating dose deviations of less than ±5%, a benchmark for clinical acceptability.
Despite the growing body of evidence supporting robotic chemotherapy compounding, performance data from real-world clinical settings in Southeast Asia remain limited, particularly for newly implemented technologies. This study addresses this gap by providing a comprehensive performance evaluation of a robotic chemotherapy compounding system implemented at Maha Vajiralongkorn Thanyaburi Hospital, Pathum Thani, Thailand. The primary objectives were to assess the system's accuracy, measured by the percentage error between theoretical and prepared volumes, and its efficiency, measured by the total preparation time. The following sections detail the rigorous methodology employed to evaluate system performance and present the findings of this large-scale retrospective analysis. In addition, mechanical factors such as syringe size and the number of compounding cycles were examined, as they may influence dose accuracy and variability, thereby affecting the overall safety margin of robotic compounding systems.
Methods
Ensuring the validity and transparency of clinical research requires a robust and clearly defined methodology. This section outlines the retrospective study design, the technical specifications and workflow of the robotic compounding system, the data collection process, and the statistical techniques used to conduct a comprehensive performance evaluation.
Study design and setting
The study was conducted as a retrospective analysis of routinely collected clinical data. Ethics approval was obtained prior to data extraction and analysis (MTH 2025-17, December 11, 2025), with a waiver of informed consent granted due to the use of anonymized data. This study was conducted at the oncology pharmacy unit of Maha Vajiralongkorn Thanyaburi Hospital, a tertiary care institution that prepares approximately 35 cytotoxic doses daily for both inpatient and outpatient services. All robotic compounding was performed within a negative-pressure isolator, maintaining an ISO Class 5 environment within a Class 7 background area, in full compliance with USP <797 > and USP <800 > standards for sterile and hazardous drug preparation.39,40
Robotic system and workflow
The AYA robotic system is a prototype platform developed for institutional use and is not commercially distributed. The AYA system was developed through a collaborative effort between pharmacists at Udonthani Cancer Hospital (Udonthani, Thailand) and engineers at King Mongkut's Institute of Technology Ladkrabang (Bangkok, Thailand). The system is currently a non-commercial prototype platform designed for institutional clinical use rather than commercial distribution. As of late 2024, three AYA robotic units have been deployed in real-world clinical settings, including Udonthani Cancer Hospital, Maha Vajiralongkorn Thanyaburi Hospital (Pathum Thani, Thailand), and Ubonratchathani Cancer Hospital (Ubonratchathani, Thailand). None of the authors have financial or proprietary interests in the system. This study received no external industry funding. The system operated using AYA Pharma.tech software (version 05.2025), with daily calibration of the analytical balance and routine preventive maintenance performed monthly. No hardware or software modifications were introduced during the study period. The system operates within a closed ISO Class 5 environment and is designed to automate the entire compounding process. 41 Medication orders were entered by pharmacists into the AYA Pharmatech software, which generated QR codes containing drug identity, dose, diluent type, and final volume. The QR codes were scanned to initiate robotic compounding. Up to six compounding stations could be loaded simultaneously with drug vials, syringes, and diluents. Before compounding, all components were verified using an integrated barcode and computer vision system, which compared real-time data against a validated reference database. Drug preparation was then performed using dual robotic arms under aseptic conditions. Dose accuracy was ensured through gravimetric dose verification using an analytical balance with four-decimal-place precision, allowing real-time calculation of dose deviation. Upon completion, prepared infusion containers and deviation data were displayed in the AYA Pharmatech interface for pharmacist verification prior to release for patient administration.
Data collection
The study period was defined from October 1, 2023, to December 31, 2024. All intravenous chemotherapy preparations with complete gravimetric data were included for analysis. A total of 7,922 individual preparations were analyzed, encompassing twelve distinct cytotoxic drug preparations as follows: - 5-Fluorouracil 1000 mg/20 ml vial - Paclitaxel 100 mg/16.7 ml vial - Paclitaxel 300/50 ml mg vial - Oxaliplatin 50 mg/10 ml and 100 mg/20 ml vial - Cisplatin 50 mg/50 ml vial - Carboplatin 150 mg/15 ml vial - Carboplatin 450 mg/45 ml vial - Leucovorin 50 mg/50 ml vial - Leucovorin 300 mg/30 ml vial - Leucovorin 350 mg/35 ml vial - Etoposide 100 mg/5 ml vial - Irinotecan 100 mg/5 ml vial
Performance evaluation of a two-arm robotic chemotherapy compounding system
The study evaluated two primary performance metrics, i.e., gravimetric accuracy and preparation time.
- Gravimetric accuracy
The primary outcome was the percentage volume error, calculated as the difference between the measured volume (derived from weight) and the theoretical prescribed volume. The calculation used the following formula, with specific gravity values provided by the drug manufacturers:

An analytical balance (Mettler Toledo WMS6002C-L) was employed for all measurements. The instrument underwent daily internal calibration and its performance was routinely verified using traceable standard weights. According to the manufacturer's specifications, the balance has an expanded measurement uncertainty of ±0.01 g (k = 2). This level of uncertainty was considered negligible relative to the magnitude of the observed volumetric deviations and was therefore not propagated into the percentage error calculations.
- Preparation time definition
Preparation time was defined as the duration from initial barcode verification to completion of robotic compounding (final mixing step). This measure reflects robotic operational efficiency rather than total end-to-end workflow time. Future studies should evaluate full workflow duration, including pharmacist verification and handling steps.
- Inclusion/Exclusion criteria
Preparations were included if complete gravimetric data were available. Preparations with incomplete records, interrupted robotic runs, or system errors were excluded from analysis.
Effects of syringe size and compounding cycles
To evaluate the influence of mechanical factors on compounding precision, data were stratified based on the hardware configurations utilized during the preparation process. This analysis specifically examined two key variables: the nominal capacity of the syringes (10 ml, 30 ml, and 50 ml) and the number of fill cycles (1 cycle, 2 cycles, or 3 cycles) required to deliver the prescribed dose. Descriptive statistics, including mean error, median, and interquartile range (IQR), were calculated for each configuration to identify potential scale-dependent or cumulative biases. Furthermore, a bootstrap analysis was employed to estimate 90% confidence intervals (CI) for the mean deviation, ensuring robust safety margin estimation.
To differentiate inherent mechanical limitations from robotic operational performance, the observed deviations were interpreted with reference to the ISO 7886-1 standard. Specifically, system accuracy was evaluated against the Tolerance on Graduated Capacity (TOGC) defined for sterile single-use syringes. 42 According to ISO 7886-1, the allowable TOGC depends on both the nominal syringe capacity and the delivered volume. For delivered volumes less than half the nominal syringe capacity, TOGC was calculated as (1.5% × nominal capacity) + (1% × delivered volume). For delivered volumes equal to or greater than half the nominal syringe capacity, TOGC was calculated as 4% of the delivered volume. Using this framework, the magnitude of the observed deviations was assessed relative to the allowable syringe tolerance. The results indicated that the measured errors were within the expected variability associated with syringe graduated capacity, implying that a proportion of the deviation may arise from intrinsic syringe limitations rather than inaccuracies of the robotic system. By incorporating this comparison, the study further examined the scale effect across different syringe volumes and the cumulative impact of repeated preparation cycles.
Statistical analysis
Statistical analyses were conducted using Stata version 14.0. Descriptive statistics, including mean, standard deviation (SD), median, interquartile range (IQR), skewness, and kurtosis, were calculated to characterize the accuracy and distribution of percentage volume errors for the entire dataset and individual drug types.
Bootstrap resampling (10,000 iterations) was performed at the level of individual preparations to estimate confidence intervals for mean absolute deviation. Analyses were stratified by syringe size and compounding cycle where appropriate. A 90% confidence interval (CI) was selected to provide a pragmatic estimate of operational safety margins in line with process validation practices. Given evidence of non-normality (Shapiro-Wilk; p < 0.001), parametric assumptions were not relied upon, and resampling-based methods were prioritized.
The data supporting the findings of this study are available within the article and its supplementary materials. In addition, the data are not publicly available due to privacy/ethical restrictions but are available from the corresponding author upon reasonable request.
Results
This section presents the empirical evidence of the robotic compounding system's performance, derived from the analysis of 7922 preparations. The findings begin with an overview of the system's overall accuracy and efficiency, followed by more granular analyses examining performance variability across different drugs and the impact of mechanical factors such as syringe size and compounding cycles.
Performance evaluation of a two-arm robotic chemotherapy compounding system
Across the entire dataset of 7,922 preparations, the robotic system demonstrated a high degree of accuracy and consistency. The mean percentage error was −1.19 ± 1.32%, with a median of −1.14% (IQR 1.86). The slight negative skew of the error distribution (−0.26) indicates a consistent but minor underdispensing trend relative to the theoretical target volumes. In addition, the mean preparation time was 11.86 ± 3.47 min per dose, with a median of 11.29 ± 3.06 min, demonstrating standardized and efficient workflow across a high volume of preparations. Certain subgroups had limited sample sizes (e.g., Irinotecan n = 9, Leucovorin 50 mg n = 25, and 50 ml cycle 3 n = 37), which may reduce the precision of subgroup estimates. Findings from small subgroups should be interpreted with caution and warrant confirmation in larger datasets.
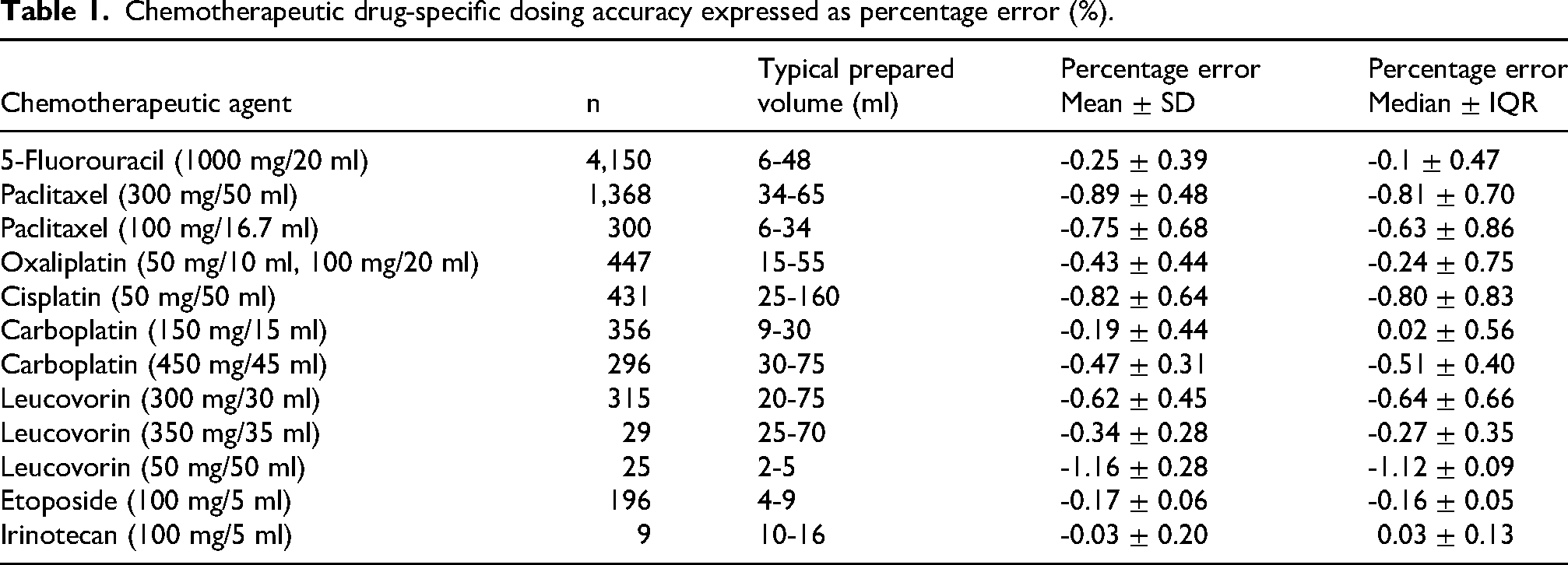
While overall performance was strong, analysis at the individual drug level revealed variability in precision, likely related to the physicochemical properties of each chemotherapeutic agent and its concentration. A summary of the accuracy for each chemotherapeutic agent is detailed in Table 1. Certain chemotherapeutic agents were compounded with exceptional accuracy. Etoposide (mean error −0.17 ± 0.06%, median error −0.16 ± 0.05%) and Irinotecan (mean error −0.03 ± 0.20%, median error 0.03 ± 0.13%) showed minimal deviation from their target volumes, indicating optimal performance with these drugs. In contrast, some chemotherapeutic drugs exhibited slightly larger, though still clinically acceptable, deviations. These included Leucovorin 50 mg (mean −1.16 ± 0.28%, median error −1.12 ± 0.09%) and Paclitaxel 300 mg (mean −0.89 ± 0.48%, median error −0.81 ± 0.70%). Additionally, for chemotherapeutic drugs prepared in multiple concentrations, accuracy sometimes varied. For instance, Carboplatin 150 mg preparations (mean error −0.19 ± 0.44%, median error 0.02 ± 0.56%) were more accurate than the 450 mg preparations (mean error −0.47 ± 0.31%, median error −0.51 ± 0.40%). Similarly, the mean error for Leucovorin varied across its 50 mg, 300 mg, and 350 mg formulations.
Chemotherapeutic drug-specific dosing accuracy expressed as percentage error (%).
Effects of syringe size and compounding cycles
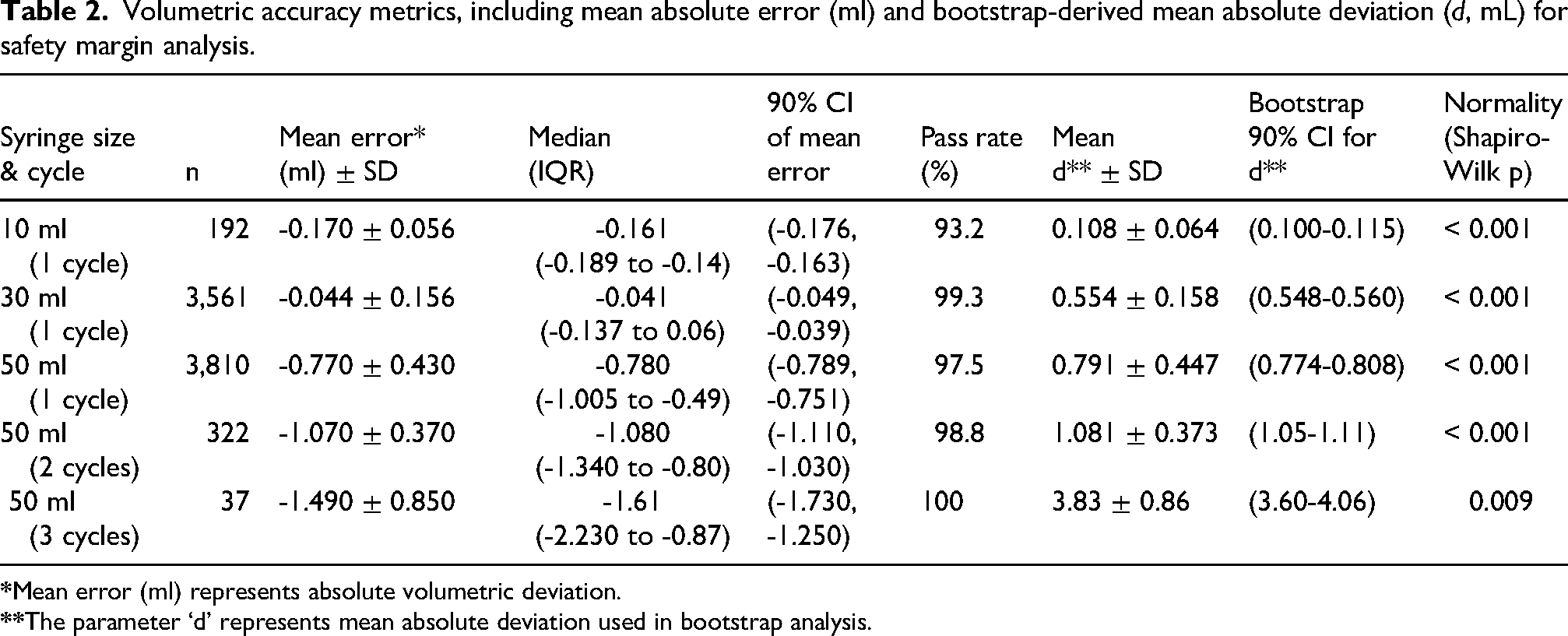
To understand how mechanical factors influence accuracy, further analysis was conducted based on syringe size and the number of fill cycles required for a single dose. The percentage error (%) represents relative deviation from the target volume and was used to assess relative clinical accuracy. The mean error (ml) represented the absolute volumetric deviation from the target value. In addition, d was defined as the absolute mean deviation, reflecting the magnitude of error for safety margin analysis. Manuscript revision includes a new clarification paragraph. This analysis, summarized in Table 2, revealed a systematic under-delivery bias across all hardware configurations.
Volumetric accuracy metrics, including mean absolute error (ml) and bootstrap-derived mean absolute deviation (d, mL) for safety margin analysis.
The data revealed two key trends as follows:
A scale effect Although the 10 ml syringe exhibited a larger proportional error (−0.170) relative to its nominal volume, bootstrap analysis based on absolute mean error demonstrated higher error and lower precision for the 30 ml syringe (0.554 ± 0.158; 90% CI, 0.548-0.560) compared with the 10 ml syringe (0.108 ± 0.064; 90% CI, 0.100-0.115). The absence of overlap between the 90% confidence intervals supports a substantially higher and less precise mean error for the 30 ml syringe as shown in Figure 1. A cumulative error effect For large-volume preparations requiring multiple 50 ml syringe cycles, the under-delivery bias increased with each cycle, growing from −0.770 ml in a single cycle to −1.490 ml in three cycles. Bootstrap distributions of the mean volumetric error (d) for the 50 ml syringe are shown across three operational cycles. Cycle 1 (n = 3810) demonstrated a low and precise mean error (0.791 ± 0.447; 90% CI, 0.774-0.808). Cycle 2 (n = 322) exhibited a rightward shift with increased mean error (1.081 ± 0.373; 90% CI, 1.05-1.11). Cycle 3 (n = 37) showed a markedly higher and more variable mean error (3.83 ± 0.86; 90% CI, 3.60-4.06). The narrow dashed vertical lines represent relatively small 90% confidence intervals of the mean error, indicating higher precision as shown in Figure 2. The non-overlapping confidence intervals indicate statistically distinct mean errors across cycles, suggesting progressive performance drift.
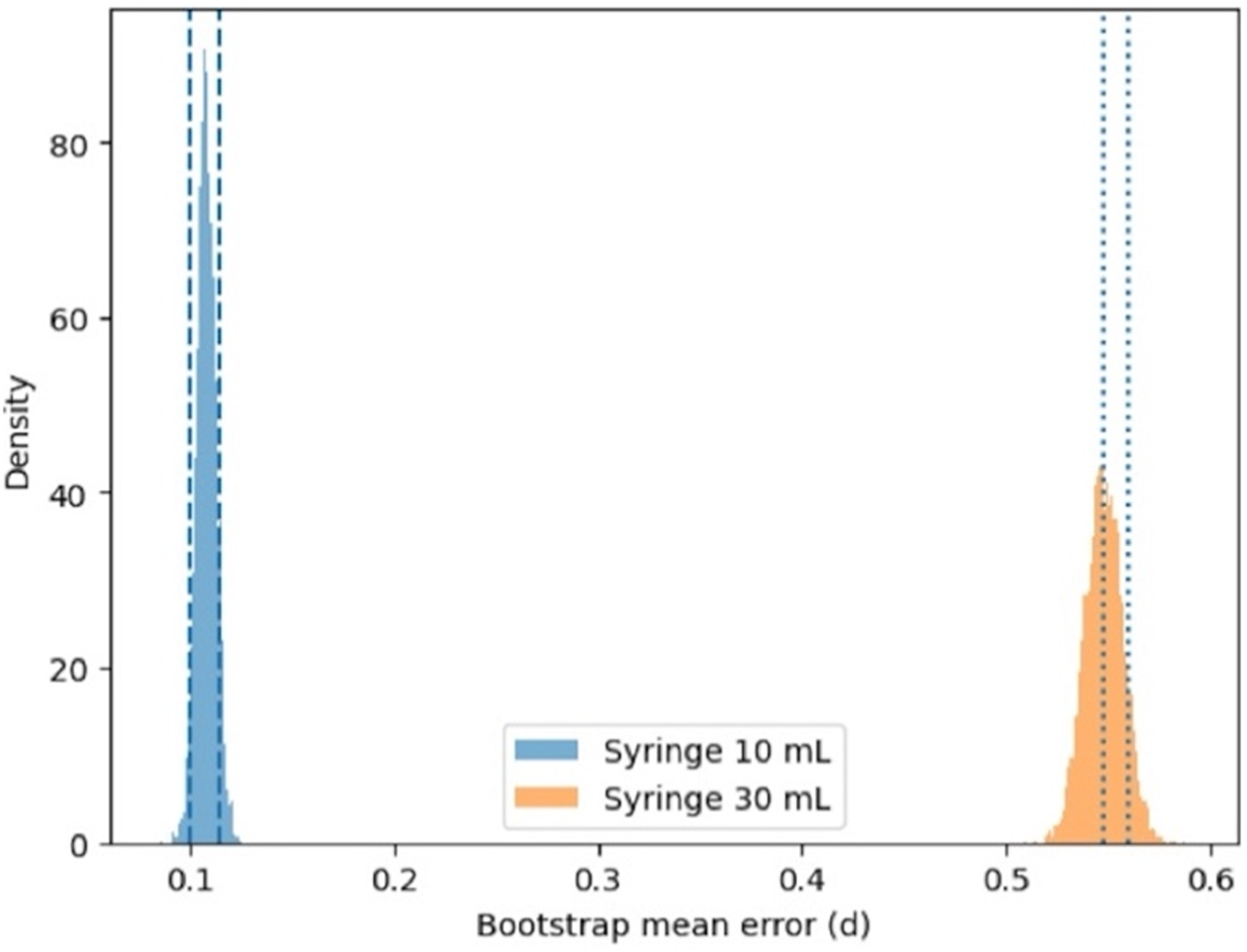
Comparison of bootstrap-estimated mean absolute deviation (d) between 10 ml and 30 ml syringes.
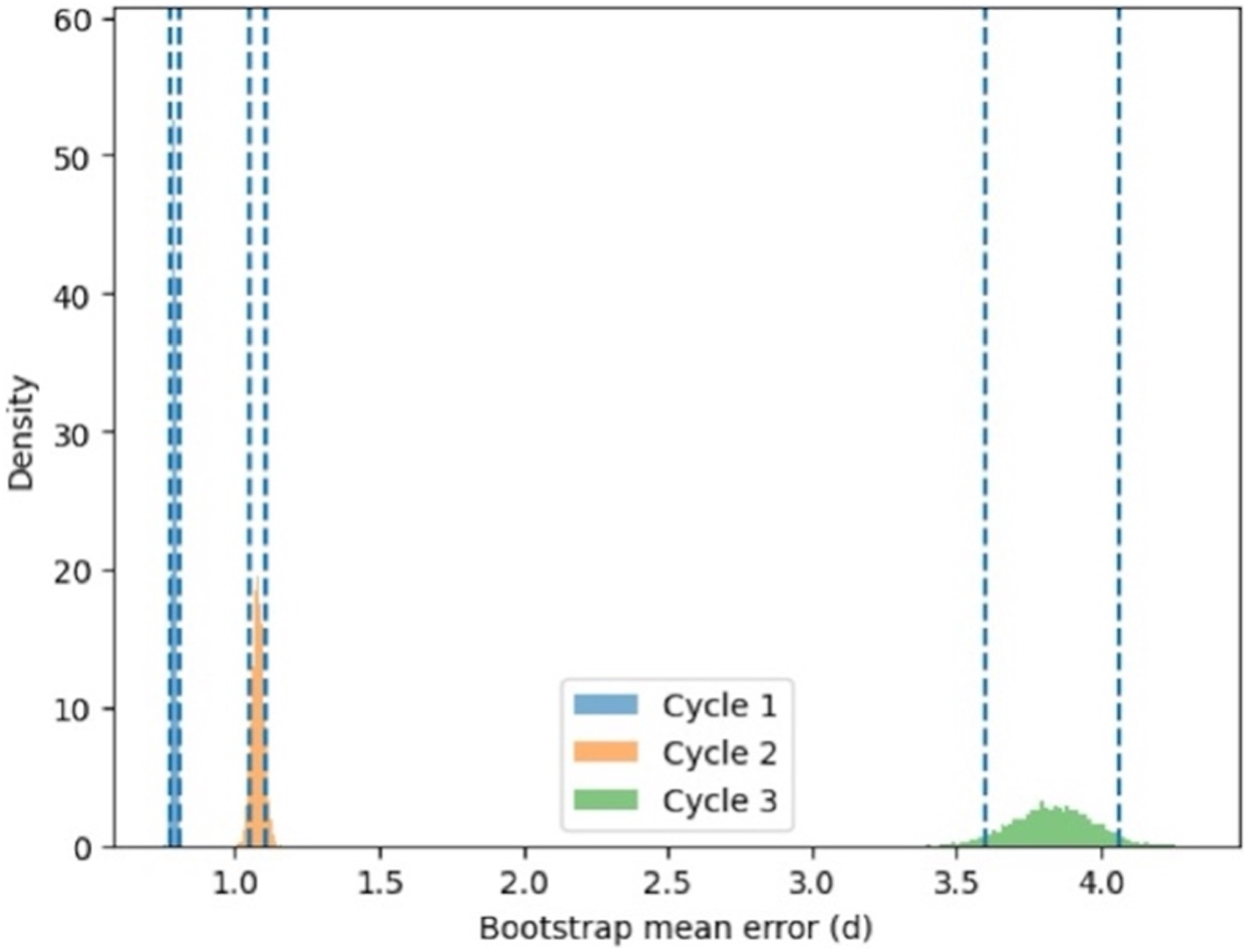
Bootstrap distributions of mean absolute deviation (d) for the 50 ml syringe across three compounding cycles.
Crucially, despite these observable biases, the compliance rates with the system's internal tolerance of gravimetric control remained exceptionally high, ranging from 93.2% to 100%. All observed deviations, regardless of drug, concentration, or syringe size, remained well within the clinically acceptable ±5% threshold, setting the stage for a discussion of their clinical and operational implications.
Discussion
This section moves beyond the presentation of data to interpret its meaning in a broader clinical and operational context. This study evaluates the study's findings in relation to existing literature, analyze the sources of performance variability, and assess the overall impact of the robotic system on oncology pharmacy practice.
Performance evaluation of a two-arm robotic chemotherapy compounding system
The primary finding of a −1.19 ± 1.32% overall mean percentage error with a median percentage error of −1.14% ± 1.86 confirm that this prototype robotic system achieves a high level of precision that is consistent with international data and established benchmarks from commercial systems like APOTECAchemo and RIVA.15,36 The data also revealed a slight but systematic under-dispensing bias. From a clinical safety perspective, this conservative bias is preferable to overdosing, particularly when compounding cytotoxic agents with narrow therapeutic windows. However, this must be balanced against the concurrent risk of underdosing, which could potentially impact therapeutic efficacy and lead to suboptimal patient outcomes.
Technical performance and sources of variability
The cytotoxic drug-specific accuracy analysis suggests that performance can be influenced by both physicochemical and mechanical factors.43,44 We hypothesize that the exceptional precision observed with Etoposide may be attributable to its stable formulation and optimal aspiration performance. Conversely, the larger deviations seen with agents like Paclitaxel could be linked to factors such as higher solution viscosity or greater vial residuals during withdrawal. It is plausible that such physicochemical properties interact with mechanical factors; for instance, a highly viscous drug may be more prone to under-delivery when drawn into smaller-volume syringes or during the rapid repetitions of a multi-cycle preparation. The presence of occasional outliers, suggested by high kurtosis values for certain drugs, may be attributed to intermittent mechanical issues like syringe friction or the retention of microscopic air bubbles during aspiration.
Effects of syringe size and compounding cycles
The analysis of mechanical factors demonstrated that both syringe size and the number of compounding cycles significantly influenced dosing precision, 42 resulting in a clear scale effect and cumulative error pattern. Smaller 10 ml syringes and multi-cycle preparations using 50 ml syringes showed a more pronounced but consistent tendency toward under-delivery. Despite these trends, system performance remained stable across all configurations. Bootstrap analysis confirmed that the variability of the mean deviation was tightly controlled, with narrow 90% confidence intervals indicating a high degree of predictability rather than random fluctuation. Notably, comparisons between syringe sizes revealed non-overlapping confidence intervals, suggesting meaningful differences in performance, with larger syringes exhibiting greater absolute deviation. In addition, the increased variability observed in the third cycle of the 50 ml syringe may indicate a potential accumulation of mechanical error or early signs of operational drift, which warrants further investigation. Future studies incorporating physicochemical parameters (e.g., viscosity, concentration) and multivariable modeling are warranted to better isolate independent contributors to compounding error. Outliers were retained in the analysis to reflect real-world system performance and were not excluded. Preparations exceeding the internal ±5% tolerance were classified as failures that may cause by syringe friction, air bublbles, and viscosity-reated aspiration variability. These were automatically flagged by the system and were not released for clinical use. All failed preparations were reprocessed prior to administration. No patient received a preparation outside predefined safety limits. Importantly, all measured deviations remained within the clinically accepted ±5% threshold, and compliance with internal gravimetric tolerance criteria was consistently high, reaching up to 100% even in more complex multi-cycle preparations. The observed deviations were interpreted in the context of ISO 7886-1 tolerance on graduated capacity (TOGC), which permits deviations of approximately ±5% for sterile syringes. This indicates that part of the observed variability may be attributable to inherent syringe limitations rather than robotic system inaccuracy. Overall, these findings demonstrate that the system maintains reliable and consistent performance under varying mechanical conditions. While these results provide important insight into the technical determinants of compounding accuracy, their clinical significance is addressed separately in the following section.
Clinical implications of systematic under-delivery
The study showed a small and consistent under-delivery bias (−1.19%), which is within the accepted ±5% range and is unlikely to affect treatment outcomes in most adult patients. However, its clinical relevance may vary depending on the treatment context, particularly for drugs with a narrow therapeutic index, where small dose differences can influence efficacy or toxicity. This is especially important in pediatric patients, where dosing is based on body weight or body surface area and margins are smaller. For example, a −1.19% deviation in a 500 mg dose such as carboplatin or 5-fluorouracil corresponds to a reduction of about 6 mg, which is generally not clinically significant for most standard regimens. Importantly, the slight under-delivery observed may offer a safety advantage, as overdosing of cytotoxic drugs poses a greater risk of severe toxicity. Overall, this level of deviation is unlikely to have meaningful clinical impact, but it highlights the need for ongoing system calibration and monitoring to maintain dosing accuracy. Simulation-based analyses evaluating clinically meaningful thresholds of under- or over-dosing would further strengthen understanding of real-world impact and should be explored in future studies.
Limitations
This study has several limitations. First, certain subgroups had small sample sizes, limiting statistical precision. Second, physicochemical variables such as drug viscosity were not systematically analyzed. Third, temporal trends in system performance were not evaluated. Future studies incorporating multivariable analysis and time-series evaluation are warranted. Furthermore, temporal performance trends (e.g., learning curve effects or maintenance-related variation) were not evaluated in this study but represent an important area for future investigation.
Conclusion
The implementation of the two-arm robotic compounding system at Maha Vajiralongkorn Thanyaburi Hospital has demonstrated excellent accuracy, reproducibility, and operational efficiency for a wide range of cytotoxic agents. With an overall mean deviation well within clinically accepted limits and a consistent, predictable preparation time, the system has proven to be a highly effective tool in a demanding clinical environment. This robotic platform provides a reliable, safe, and scalable solution for modern chemotherapy preparation, significantly enhancing operator safety and ensuring precise, traceable dosing for patients in high-volume healthcare settings.
Supplemental Material
sj-docx-1-opp-10.1177_10781552261462449 - Supplemental material for Performance evaluation of a two-arm robotic chemotherapy compounding system: Effects of syringe size and compounding cycles on accuracy, efficiency, and safety margins
Supplemental material, sj-docx-1-opp-10.1177_10781552261462449 for Performance evaluation of a two-arm robotic chemotherapy compounding system: Effects of syringe size and compounding cycles on accuracy, efficiency, and safety margins by Taweesak Kunjam, Nuchalinda Eiambutlop and Nuttakorn Baisaeng in Journal of Oncology Pharmacy Practice
Footnotes
Acknowledgments
The authors thank the pharmacy staff at Maha Vajiralongkorn Thanyaburi Hospital, Thailand for their collaboration and technical expertise in robotic compounding.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
The datasets generated and/or analyzed during the current study are not publicly available due to institutional and ethical restrictions, but these are available from the corresponding author on reasonable request and with permission from Maha Vajiralongkorn Thanyaburi Hospital, Thailand.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.