
Abstract
Background
Hazardous drugs preparation is a high-risk process requiring strict control of aseptic conditions to ensure product sterility and to protect healthcare workers. Isolators and laminar airflow cabinets are widely used in hospital pharmacies for the preparation of hazardous drugs. Structured assessments of process-related risks associated with routine handling practices remain limited.
Objectives
This study aimed to apply Failure Mode and Effects Analysis (FMEA) to identify and prioritize high-risk handling steps in hazardous drugs preparation workflows using isolators and to evaluate risk profiles associated with laminar airflow cabinets.
Methods
An observational FMEA-based risk assessment was conducted in a hospital pharmacy during routine hazardous drugs preparation. Six critical handling steps were evaluated: glove installation, surface cleaning, material transfer, documentation, waste removal, and glove removal. For isolator-based preparation, 100 routine preparations were directly observed to quantify failure frequencies and to assign occurrence scores. For laminar airflow cabinets, failure modes and occurrence levels were evaluated using observational insights combined with structured expert consensus. Severity and detection scores were assigned by an interdisciplinary expert panel. Risk Priority Numbers (RPNs) were calculated to prioritize critical failure modes.
Results
FMEA identified surface cleaning, material transfer, and glove handling as the most critical steps in hazardous drugs preparation workflows. In isolator-based preparation, the highest initial RPNs were observed for surface cleaning (RPN = 240), material transfer (RPN = 210), and glove installation (RPN = 144). Risk assessment highlighted different underlying drivers of failure across workflows. In isolators, elevated risks were mainly associated with handling complexity and limited detectability of failures within a closed system. In laminar airflow cabinets, risks were primarily related to open-system exposure and greater dependance on operator technique and environmental control.
Conclusion
FMEA proved to be a practical tool for systematically identifying and prioritizing risks in hazardous drugs preparation workflows. The analysis highlighted critical handling steps requiring targeted risk mitigation strategies and demonstrated the importance of workflow design, operator training, and adherence to standard operating procedures. The proposed FMEA-based approach provides a transferable framework to support continuous quality improvement and enhance safety in oncology pharmacy practice.
Keywords
Introduction
Hazardous drugs preparation is a high-risk activity that requires strict control of aseptic conditions to ensure product sterility while simultaneously protecting healthcare workers from occupational exposure. Hazardous drugs, including antineoplastic agents used in hazardous drugs, are associated with carcinogenic, teratogenic, and genotoxic risks, and unsafe handling may result in serious health consequences for exposed staff.1,2 Failures during hazardous drugs compounding may lead to microbial contamination, medication errors, and hazardous drug exposure, with potentially severe consequences for both patients and pharmacy personnel.3,4 International guidelines emphasize the need for robust risk management strategies and the use of appropriate engineering controls in oncology pharmacy practice.1,5 Laminar airflow systems, typically in the form of Class II biological safety cabinets, and isolators are the two main technologies used for aseptic hazardous drugs preparation in hospital pharmacies. Biological safety cabinets rely on unidirectional airflow to maintain a clean environment but remain open systems that are highly dependent on operator technique, environmental control, and strict adherence to aseptic procedures.5,6 Isolators provide a physical barrier between the operator and the compounding area, reducing occupational exposure and potentially enhancing sterility assurance.7,8 Isolators introduce additional handling complexity, including glove systems, material transfer ports, and internal decontamination procedures, which may themselves become sources of failure if not adequately controlled.8,9 With the widespread use of both systems, understanding workflow-related risks under routine practice conditions is essential, particularly in hospital settings with constrained resources. Previous studies have primarily focused on microbiological monitoring, surface contamination, and compliance with guidelines, while fewer investigations have addressed process-related risks associated with daily handling steps in hazardous drugs preparation.6,10 Structured risk assessment approaches are increasingly recommended in healthcare to support quality improvement and patient safety, including in sterile compounding practices. Failure Mode and Effects Analysis (FMEA) is a proactive risk management tool that enables systematic identification of potential failures, evaluation of their severity, likelihood of occurrence, and detectability, and prioritization of corrective actions.3,4 FMEA has been successfully applied in various healthcare processes, including medication safety and sterile compounding workflows.3,4,15 Further application of structured FMEA approaches is needed to better characterize workflow-related risks in hazardous drugs preparation and support continuous quality improvement. The present study aimed to apply FMEA to hazardous drugs preparation workflows in a hospital pharmacy setting, with a focus on isolator-based compounding supported by a contextual evaluation of laminar airflow cabinet workflows. The objectives were to identify and prioritize high-risk handling steps and to propose targeted risk mitigation strategies. By providing a practical and transferable FMEA-based framework, this study seeks to support safer and more standardized hazardous drugs preparation practices in oncology pharmacy.
Materials and methods
Study Design: This study was a prospective, observational risk assessment conducted using FMEA to evaluate critical handling steps during hazardous drugs preparation performed in isolators and laminar airflow (LAF) cabinets in a hospital pharmacy setting.3,4,14,15
Study Setting: The study was carried out in the oncology pharmacy unit of a tertiary hospital where hazardous drugs are routinely prepared in compliance with institutional standard operating procedures (SOPs) and international recommendations for hazardous drug handling.1,2,5,6 The unit is equipped with closed-system cytotoxic drug preparation isolators (ISOCYT®, FREIA, a Getinge Group company, France), while laminar airflow cabinets (LN 090, Nüve, Ankara, Turkey; biological safety cabinets, Class II) are not routinely used during the study period to prepare hazardous drugs due to occupational safety policies but remain used for other preparations.7–10
Process Mapping: A detailed process mapping of the hazardous drugs preparation workflow was performed. The complete workflow was documented and is presented as a process map (Figure 1). Six critical handling steps common to both isolator-based and LAF-based preparation were selected based on their potential impact on product sterility, operator safety, and process reliability: glove installation, surface cleaning, material transfer, logbook entry, waste removal, and glove removal. These steps were selected to allow standardized evaluation of key risk-prone activities across compounding workflows.1,5,8,11,12
Observational Assessment: An observational checklist was developed to document deviations and failures occurring during routine hazardous drugs preparations. For the isolator system, a total of 100 routine preparations were directly observed. Failures were recorded for each handling step, and failure frequencies per 100 preparations were used to quantify occurrence. Laminar airflow cabinet workflows were not directly observed in routine hazardous drugs preparation during the study period due to institutional policies prioritizing isolator use for hazardous drug compounding. Therefore, a mixed-method approach was adopted. While occurrence scores for isolator-based workflows were derived from direct observational data, the evaluation of laminar airflow cabinet workflows relied on structured expert consensus supported by workflow analysis and observational insights from comparable hospital pharmacy practices. This approach is consistent with FMEA applications in healthcare when direct observational data are limited and allows for a contextual comparative assessment of risk profiles between closed and open compounding systems. Observed and anticipated deviations were categorized according to predefined failure modes.8,11–13,17
Failure Mode and Effects Analysis: FMEA was applied to evaluate hazardous drugs preparation workflows.3,4,14,15 For each identified failure mode, three parameters were evaluated: Severity (S): the potential impact of the failure on product sterility and/or operator safety. Occurrence (O): the likelihood of the failure occurring. Detection (D): the likelihood that the failure would be detected before resulting in harm. Each parameter was scored on a numerical scale from 1 (lowest risk) to 10 (highest risk) according to predefined scoring criteria.3,4,14,15
Scoring Methodology: Occurrence scores (O) for isolators were calculated based on observed failure frequencies per 100 preparations. For laminar airflow cabinets, occurrence scores were determined using structured expert consensus supported by workflow analysis and observational insights. This approach is consistent with FMEA applications in healthcare where direct failure frequency data are limited. Severity (S) and Detection (D) scores for both workflows were assigned by expert consensus, considering the potential consequences of each failure mode and the effectiveness of existing preventive and monitoring measures.3,4,14,15
Expert Panel: FMEA scoring was performed by an interdisciplinary expert panel composed of pharmacists, pharmacy technicians involved in hazardous drugs preparation, and quality assurance personnel. Consensus was reached through structured discussions conducted in two iterative rounds, based on observed practices, institutional SOPs, and professional experience.1,7,11,12
Risk Priority Number (RPN): For each failure mode, a Risk Priority Number (RPN) was calculated using the following formula:

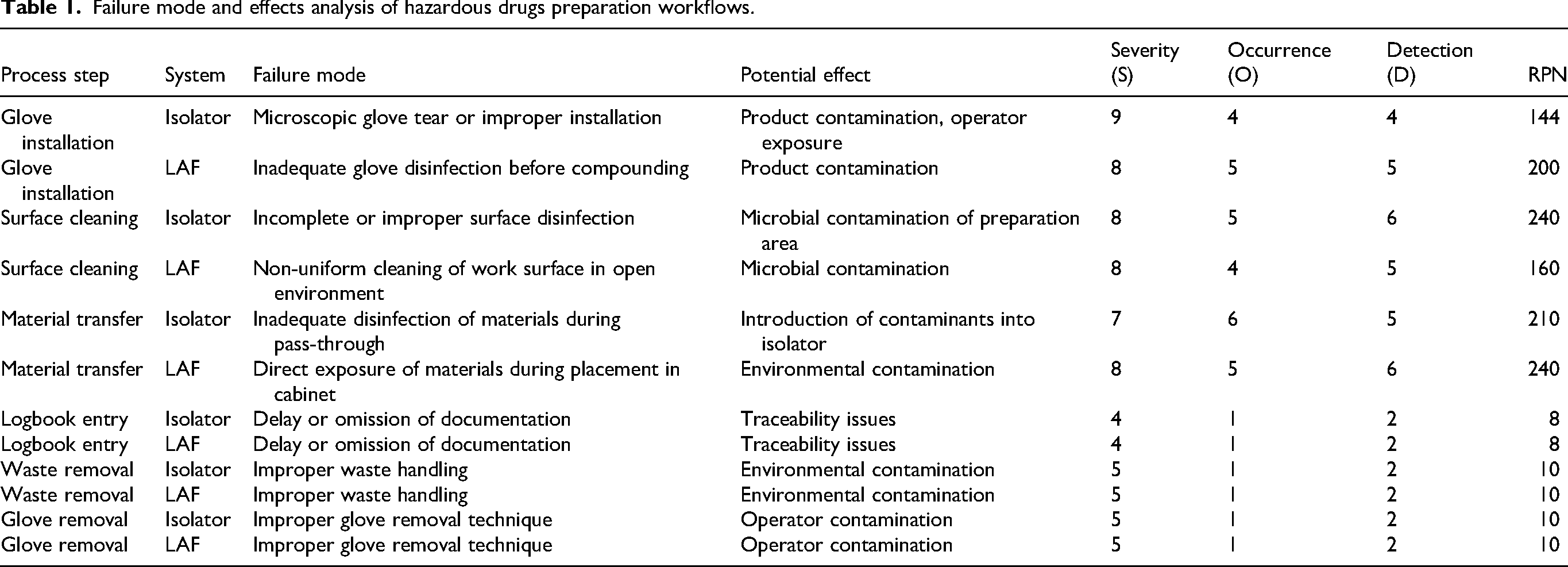
Failure modes were classified according to their RPN values as: High risk: RPN ≥ 100, Moderate risk: RPN 50–99, Low risk: RPN < 50.3,4,14,15 A detailed summary of identified failure modes, FMEA scores, and RPN values for both systems is provided in Table 1.
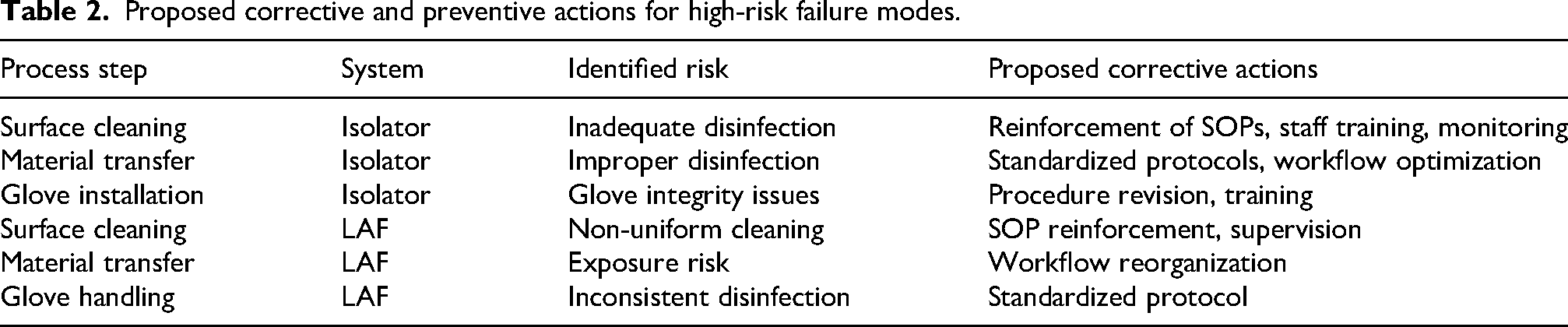
Corrective and Preventive Actions: For failure modes classified as high risk, corrective and preventive actions were proposed (Table 2), including reinforcement or revision of standard operating procedures, targeted staff training, and implementation of monitoring and documentation tools. These actions were aligned with international recommendations for sterile compounding quality improvement and hazardous drug handling.1,5,10–12 The proposed actions were not implemented during the study period, and no post-intervention observational validation was performed. Ethical Considerations: The study involved observation of routine professional practice without the collection of patient-specific data. All observations were conducted anonymously and exclusively for quality improvement purposes.
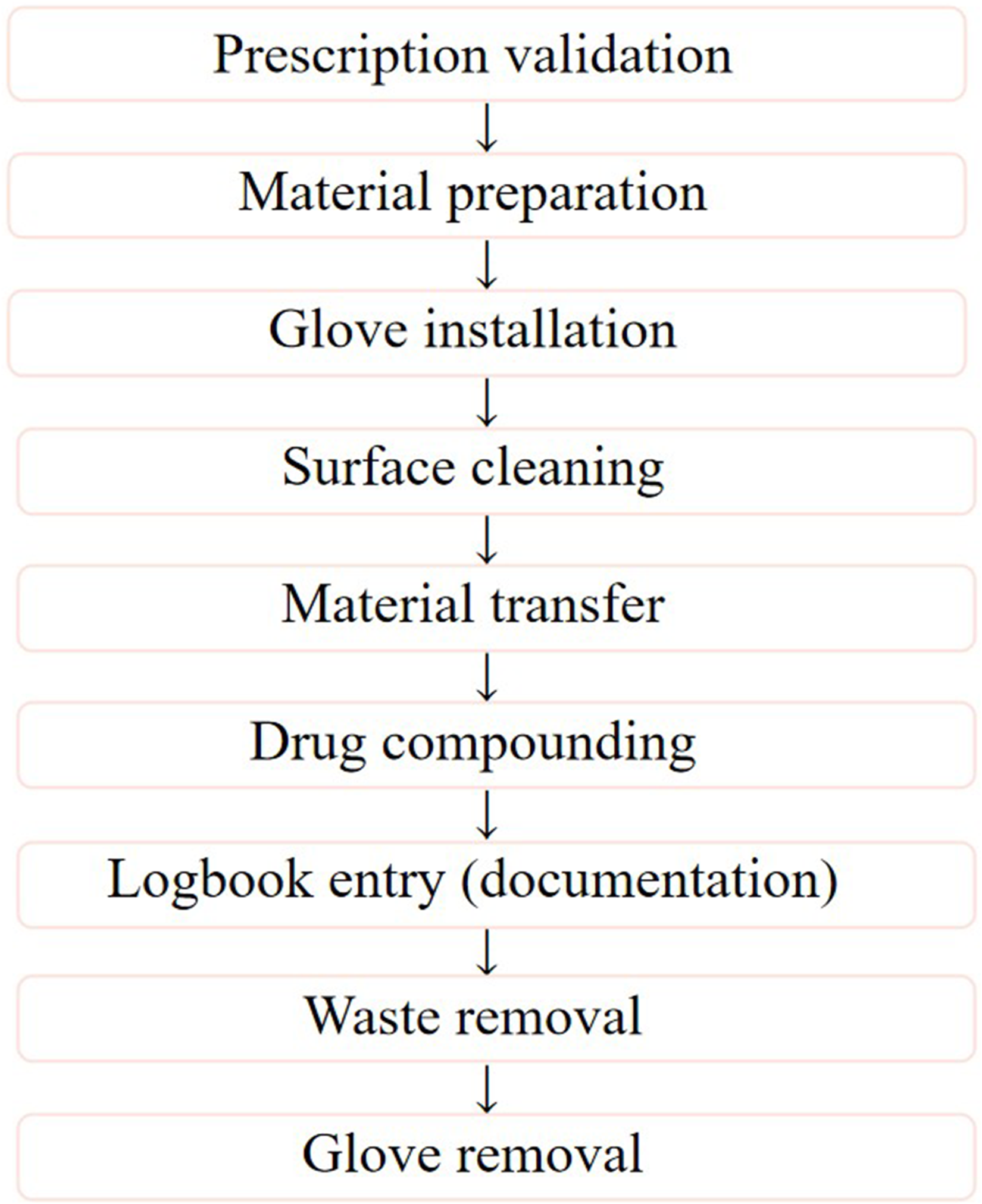
Process map of chemotherapy preparation workflow in hospital pharmacy.
Failure mode and effects analysis of hazardous drugs preparation workflows.
Proposed corrective and preventive actions for high-risk failure modes.
Results
Observational Findings and Failure Frequencies: A total of 100 routine hazardous drugs preparations performed using isolators were observed. Failures were identified in three of the six evaluated handling steps. The highest failure frequency was observed during material transfer (7 failures per 100 preparations), followed by surface cleaning (3/100) and glove installation (1/100). No failures were observed during logbook entry, waste removal, or glove removal. For laminar airflow cabinets, failure modes were identified based on workflow analysis and expert panel evaluation, supported by observational insights from comparable practice settings. Identified deviations included inconsistent glove disinfection, variability in surface cleaning practices, and potential environmental exposure during material handling. These findings were used to inform occurrence scoring within the FMEA framework.
Failure Mode and Effects Analysis of Isolator-Based Preparation: Initial FMEA of isolator-based hazardous drugs preparation identified three high-risk handling steps (Table 1). Surface cleaning demonstrated the highest Risk Priority Number (RPN = 240), followed by material transfer (RPN = 210) and glove installation (RPN = 144). These elevated RPN values reflected a combination of moderate-to-high severity, observed failure frequencies, and limited detectability prior to potential contamination or occupational exposure. The remaining steps - logbook entry, waste removal, and glove removal - showed low RPN values and were not considered critical contributors to process risk under routine practice conditions.
FMEA-Based Risk Profile of Laminar Airflow Cabinet Workflows: FMEA applied to laminar airflow cabinet workflows identified similar critical handling steps, including surface cleaning, material transfer, and glove handling (Table 1) The calculated RPN values for laminar airflow cabinet workflows are presented in Table 1, with the highest values observed for material transfer (RPN = 240), glove handling (RPN = 200), and surface cleaning (RPN = 160). Occurrence scores were derived from expert consensus supported by workflow analysis. Elevated RPN values in these steps reflected increased susceptibility to environmental exposure, variability in operator technique, and challenges in maintaining consistent aseptic conditions in an open-system setting. Unlike isolator-based preparation, where failure frequencies were directly observed, these results represent an expert-informed assessment of risk-prone steps within laminar airflow workflows.
Risk Profile Interpretation: Analysis of FMEA results highlighted distinct underlying risk drivers associated with each workflow. In isolators, high RPN values were primarily associated with handling complexity, pass-through disinfection procedures, and limited detectability of failures within a closed system. laminar airflow cabinet workflows were characterized by increased operator-dependent risks, including direct environmental exposure and potential disruption of airflow during manipulation. Steps related to documentation, waste removal, and glove removal demonstrated low-risk profiles and did not significantly contribute to overall process risk.
Summary of Key Findings: Three critical handling steps were identified in isolator-based hazardous drugs preparation: surface cleaning, material transfer, and glove installation. FMEA-based assessment of laminar airflow workflows identified similar high-risk steps, with differences in the underlying mechanisms contributing to failure. Closed-system isolators were mainly associated with complexity-related risks, whereas open-system workflows were associated with greater dependance on operator technique and environmental control. These findings support the use of FMEA as a structured approach to identify and prioritize risk-prone steps in hazardous drugs preparation workflows.
Discussion
Interpretation of Key Findings: This study applied FMEA to systematically identify and characterize risks associated with hazardous drugs preparation workflows performed using isolators and laminar airflow cabinets in a hospital pharmacy setting. The findings demonstrate that, although both systems are designed to ensure aseptic compounding and operator safety, they present distinct risk profiles driven primarily by differences in system design and workflow characteristics.1,5,11,18 FMEA identified surface cleaning, material transfer, and glove handling as the most critical steps in hazardous drugs preparation. In isolator-based preparation, surface cleaning emerged as the highest-risk step, reflected by the highest RPN values. This finding underscores that isolators, despite their closed design, are not inherently risk-free. Inadequate cleaning or disinfection within an enclosed environment may allow contaminants to persist and compromise sterility, particularly when detection mechanisms are limited.5,8,11,12 Material transfer was identified as a critical step across workflows. In isolators, elevated RPN values were mainly associated with handling complexity, multiple disinfection steps, and pass-through procedures. 18 Laminar airflow cabinet workflows exhibited increased vulnerability to environmental exposure and airflow disruption during material handling, reflecting the inherent characteristics of open-system compounding.5,11,13 Glove handling also demonstrated system-specific risk patterns. In isolators, risks were primarily linked to glove integrity and installation, whereas in laminar airflow workflows, higher risk levels were associated with variability in glove disinfection practices and unrestricted hand movement within the compounding area.5,11,12 These findings reinforce the critical role of operator technique and adherence to aseptic practices.
Comparison with Published Guidance and Literature: The results of this study are consistent with international guidelines and previous reports emphasizing that aseptic compounding safety depends not only on equipment selection but also on workflow design, staff training, and adherence to standard operating procedures.1,5,10,11,17 While isolators are widely recognized for reducing occupational exposure, their effectiveness relies heavily on proper handling and maintenance.1,2,9,16 Biological safety cabinets operating with laminar airflow, when used correctly, can provide adequate sterility assurance but require strict compliance with aseptic techniques due to the absence of a physical barrier.5,11,13 A limited number of studies have applied FMEA in sterile compounding and medication safety processes, and further work is needed to better characterize workflow-related risks in different compounding environments.3,4,14,15,20
Practical Implications for Risk Management: A key strength of this study is the application of FMEA as a structured tool to identify and prioritize failure modes within hazardous drugs preparation workflows. The findings highlight that risk reduction strategies should focus on critical handling steps, including surface cleaning, material transfer, and glove handling. The proposed corrective and preventive actions (Table 2), including reinforcement of standard operating procedures, targeted staff training, and improved monitoring tools, represent practical interventions to enhance process safety. These measures can be implemented without major technological changes, making them particularly relevant for hospital pharmacies operating in resource-constrained settings.6,7,15,19
Strengths: This study has several strengths, including the use of real-life observational data for isolator-based preparation, a structured FMEA methodology, and the involvement of an interdisciplinary expert panel.3,4,20
Implications for Hospital Pharmacy Practice: The findings of this study emphasize that the safety of hazardous drugs preparation depends on workflow design, operator training, and adherence to aseptic practices, rather than equipment selection alone.1,6,7,11,18 FMEA provides hospital pharmacies with a structured framework to identify vulnerabilities, prioritize interventions, and support continuous quality improvement in sterile compounding processes.3,4,15,20 The proposed FMEA-based model can be adapted to different hospital settings to enhance safety, improve process standardization, and support harmonization of oncology pharmacy practices.
Limitations: This study has several limitations that should be considered when interpreting the findings. The study was conducted in a single hospital pharmacy setting, which may limit the generalizability of the results to other institutions with different organizational structures, resources, and workflow practices. The number of observed hazardous drugs preparations in isolator-based compounding, although sufficient to identify common failure modes, may not capture rare or infrequent events. While occurrence scores for isolator-based preparation were derived from direct observation, the evaluation of laminar airflow cabinet workflows relied partly on expert consensus, which may introduce a degree of subjectivity. The use of an interdisciplinary expert panel and structured discussions helped to enhance the consistency and robustness of the scoring process. The FMEA methodology inherently involves semi-quantitative assessment based on expert judgment, which may vary between institutions. Corrective and preventive actions proposed in this study were not validated through post-implementation measurements, and their impact on risk reduction should be confirmed in future prospective studies.
Conclusion
This study demonstrates that FMEA is a practical and effective tool for systematically identifying and prioritizing risks in hazardous drugs preparation workflows. The analysis highlighted surface cleaning, material transfer, and glove handling as the most critical steps requiring targeted risk mitigation. Findings from isolator-based preparation showed that, despite the advantages of closed systems, significant risks persist and are mainly related to handling complexity and limited detectability of failures. The evaluation of laminar airflow cabinet workflows emphasized the importance of operator-dependent factors and environmental control in maintaining aseptic conditions. These results underline that the safety of hazardous drugs compounding is strongly influenced by workflow design, operator technique, and adherence to standard operating procedures, rather than equipment selection alone. The proposed FMEA-based approach provides a structured and transferable framework to support continuous quality improvement, enhance process safety, and promote harmonization of oncology pharmacy practices across different healthcare settings.
Footnotes
Ethics approval
This study involved the observation of routine professional practices without the collection of patient-specific or identifiable data. All observations were conducted anonymously and exclusively for quality improvement purposes. Therefore, formal ethical approval was not required according to institutional guidelines.
Author contributions
Conceptualization: SED, IB, ACC; Methodology: SED, KA; Data curation: SED; Investigation: SED Clinical and technical input: IB, ACC, IT, SED, BM, SEM, FZB, YH, AEK; Writing – original draft: SED; Writing – review and editing: IB, ACC; Supervision: IB, AEK; Validation: All authors. Final approval of the manuscript: All authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.