
Abstract
Objective
This study aimed to evaluate the prevalence of polypharmacy and its association with clinically significant adverse events in geriatric patients (≥65 years) with metastatic hormone-sensitive prostate cancer (mHSPC) receiving androgen receptor pathway inhibitors (ARPis) in routine clinical practice.
Methods
This retrospective observational study included 186 male patients with mHSPC who received ARPi therapy between March 2024 and January 2026. Patient data were obtained from electronic health records. Polypharmacy was defined as the concurrent use of five or more medications, including ARPi. Adverse events were graded based on Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0.
Results
97.3% of 186 patients were using at least one medicine simultaneously with an ARPi, with a median of seven concomitant medicines. The prevalence of polypharmacy was found to be 55.4%. The most commonly prescribed drug classes included analgesics, antihypertensives, lipid-lowering agents, and antidiabetics. The most frequent Grade 3–4 adverse events were anemia (11.8%), fatigue (10.2%), and hypokalemia (9.1%). Liver enzyme elevations were observed more frequently in patients receiving enzalutamide whereas those treated with abiraterone acetate were more likely to develop metabolic and electrolyte abnormalities, including anemia, hypokalemia, and elevated creatinine kinase levels.
Conclusions
Polypharmacy is highly prevalent among geriatric patients receiving ARPi for mHSPC and may contribute to the development of clinically significant toxicities and adverse events.
Keywords
Introduction
In previous studies, new-generation androgen receptor pathway inhibitors (ARPis) enzalutamide, and abiraterone acetate have been shown to significantly improve treatment outcomes in patients with metastatic hormone-sensitive prostate cancer (mHSPC).1,2 These oral agents, however, are often prescribed to patients who require multiple concomitant medications for comorbidities or cancer-related symptoms. This clinical context raises concerns regarding polypharmacy, a phenomenon that has become increasingly prevalent in oncology practice. 3
Polypharmacy may lead to adverse clinical outcomes by altering pharmacokinetic and pharmacodynamic properties of drugs used concomitantly. 4 This may reduce benefits expected from ARPis or lead to serious toxicities. Similarly, ARPis may interact with the metabolism and elimination of concomitant medications and modify their effectiveness and safety profiles. These potential effects may reduce treatment efficacy and/or intensify adverse reactions associated with concomitant medications. 5
Given these considerations, systematic review of polypharmacy in patients treated with ARPis is warranted. The aim of the present study was to determine the prevalence of polypharmacy in patients with mHSPC who were on ARPis and assess its association with clinically significant adverse events in routine clinical practice.
Material and methods
Study population
This study included male patients diagnosed with mHSPC and treated with ARPis at Basaksehir Cam and Sakura City Hospital between March 2024 and January 2026. Data were obtained retrospectively from electronic health records of study patients. Data collected from patient files included oncologic diagnosis, prescribed ARPi, age, laboratory parameters, electrocardiogram (ECG) findings, corrected QT interval prolongation risk, comorbidities, and treatment-related side effects and their severity, excluding those observed during the first month after initiating treatment with ARPis. Any medications prescribed by oncologists or other healthcare providers during treatment with ARP inhibitors, were retrieved from the national electronic prescription system.
Inclusion criteria
✓ Patients aged ≥65 years
✓ Histologically or clinically confirmed mHSPC
✓ Treatment with enzalutamide or abiraterone acetate
✓ Availability of electronic medical records including
Exclusion criteria
✓ Age <65 years
✓ Diagnosis of castration-resistant prostate cancer
✓ ARPi use for indications other than mHSPC
✓ Evidence of bone marrow involvement at baseline
✓ Incomplete or missing medical records
Calculation and classification of corrected QT interval (QTc) in patients using ARBi
The Bazett's formula (QTc = QT / √RR) was used to calculate QTc and Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0 was used to classify QTc prolongations.
Normal QTc interval <450 ms
Grade 1: QTc 450–480 ms
Grade 2: QTc 481–500 ms
Grade 3: QTc ≥501
Grade 4: Torsades de pointes; polymorphic ventricular tachycardia
Statistical analysis
The SPSS 27.0 software package was used for statistical analysis of the data. The Kolmogorov-Smirnov test was used to test whether data were normally distributed. Data that were assumed to be normally distributed such as age were presented as the mean ± standard deviation. Non-normally distributed data such as total number of concomitant medications were presented as median, minimum, and maximum values. Adverse events, however, were presented as counts and percentages.
Results
Baseline patient characteristics
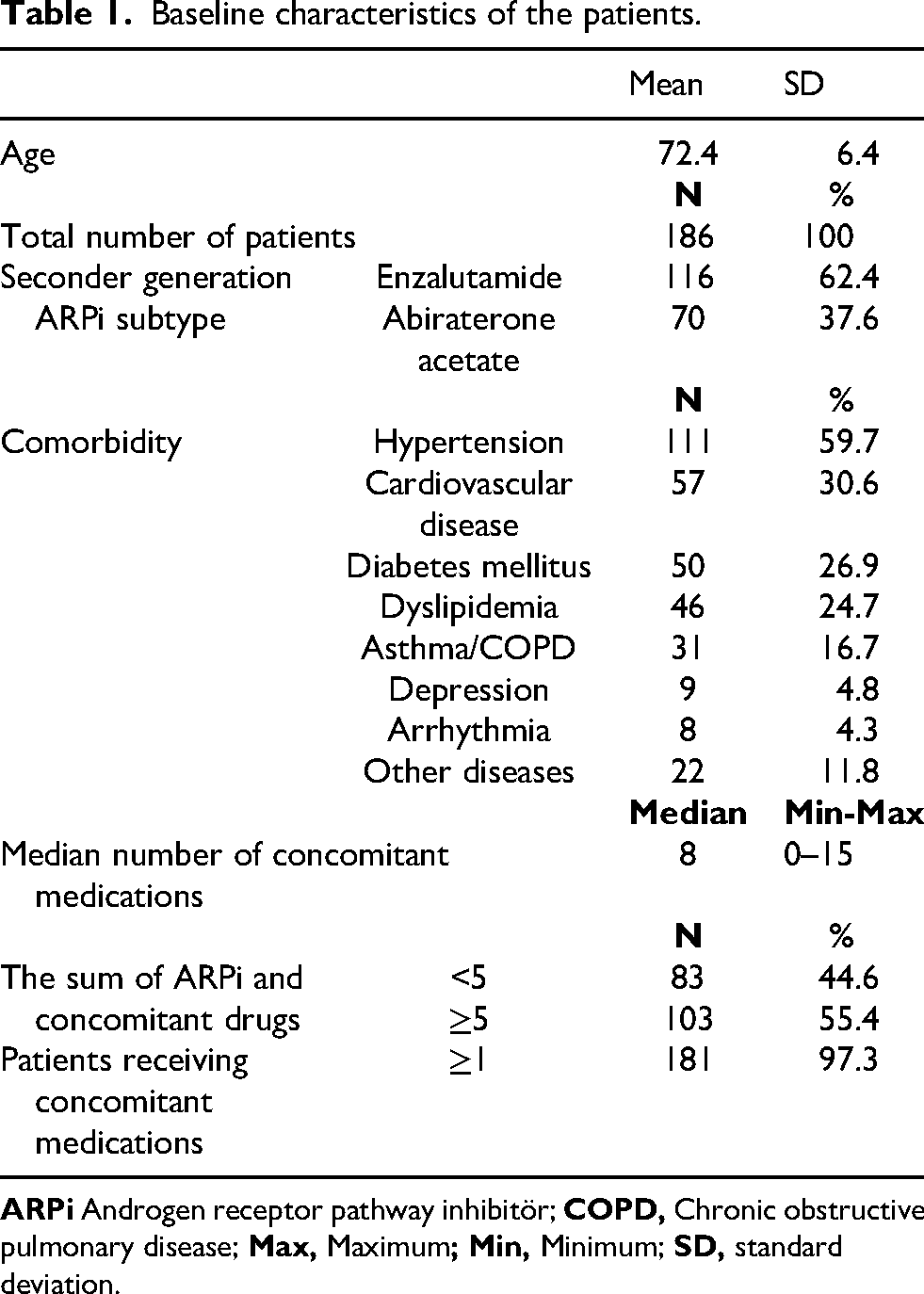
The mean age in the overall study population was 72.4 ± 6.4 (65–86) years. 116 (62.4%) patients were on enzalutamide and 70 (37.6%) were on abiraterone acetate. The median number of medications used in the overall study group was 8 (min-max, 0–15). The prevalence rate of polypharmacy was found to be 55.4%. The most common comorbidities in the study population were hypertension in 111 patients (59.7%), cardiovascular disease in 57 (30.6%), diabetes mellitus in 50 (26.9%), and dyslipidemia in 46 (24.7%) (Table 1).
Baseline characteristics of the patients.
Distribution of concomitant medications
Most of the 186 patients receiving ARPi therapy were taking multiple medications simultaneously. The most common concomitantly used medicines were analgesics, including tramadol (28.5%), codeine (22.6%), and diclofenac (18.8%). Cardiovascular and lipid-lowering drugs, such as atorvastatin (16.1%) and amlodipine (15.6%), were also frequently used (Table 2).
Distribution of concomitant medicines in patients receiving enzalutamide or Abiraterone acetate.
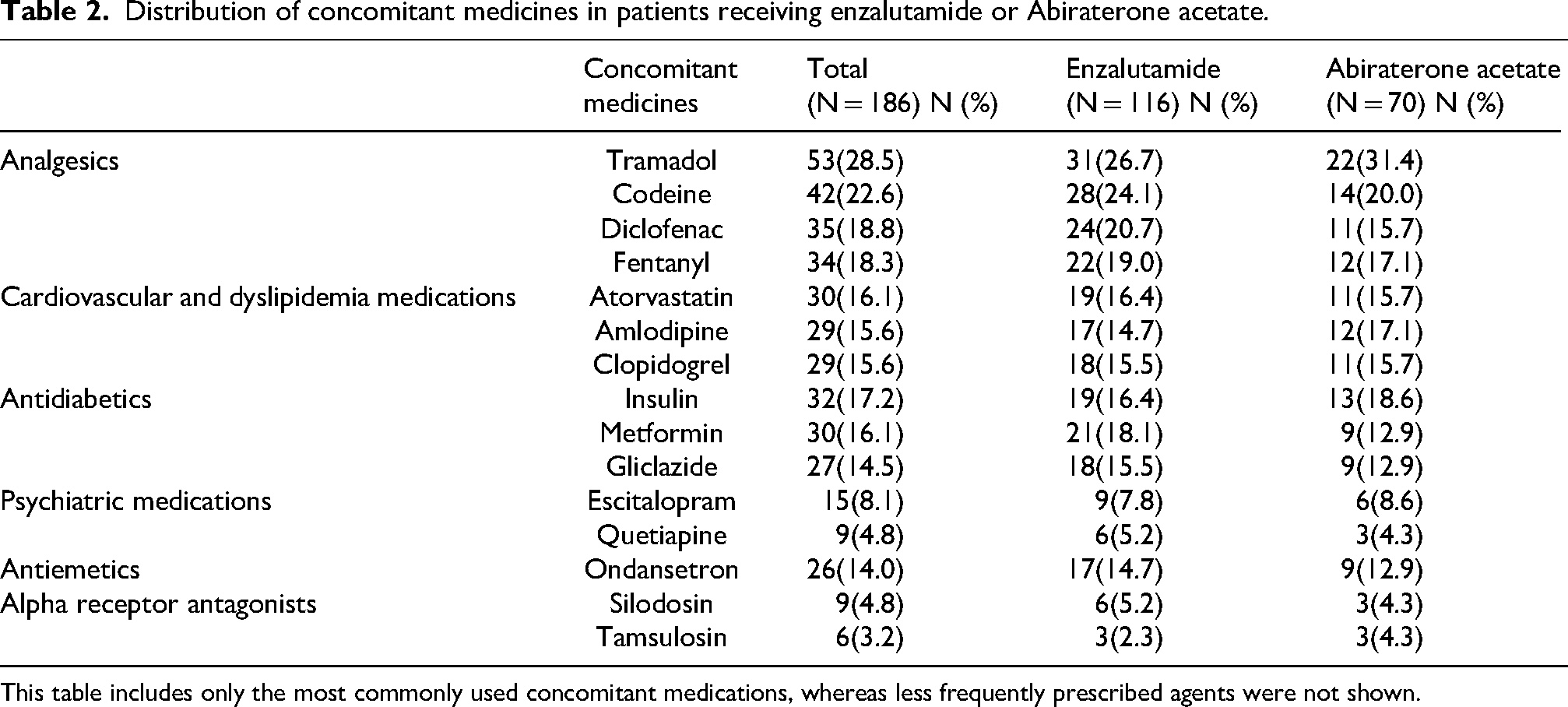
This table includes only the most commonly used concomitant medications, whereas less frequently prescribed agents were not shown.
Adverse events associated with ARBi
The incidence of grade 3–4 adverse events in patients on ARBi was relatively low compared to grade 1–2 events. Specifically, in the enzalutamide group, grade 3–4 fatigue and anemia were observed in 9 (7.8%) patients each, while grade 3–4 headache and QTc prolongation occurred in 7 (6.0%) and 5 (4.3%) patients, respectively within this treatment subgroup. Among patients treated with abiraterone acetate, grade 3–4 fatigue and anemia were more frequent, occurring in 10 (14.3%) and 13 (18.6%) patients, respectively, whereas grade 3–4 headache and QTc prolongation were observed in 5 (7.1%) and 3 (4.3%) patients (Table 3).
Comparison of adverse events and clinical outcomes between enzalutamide and Abiraterone acetate.
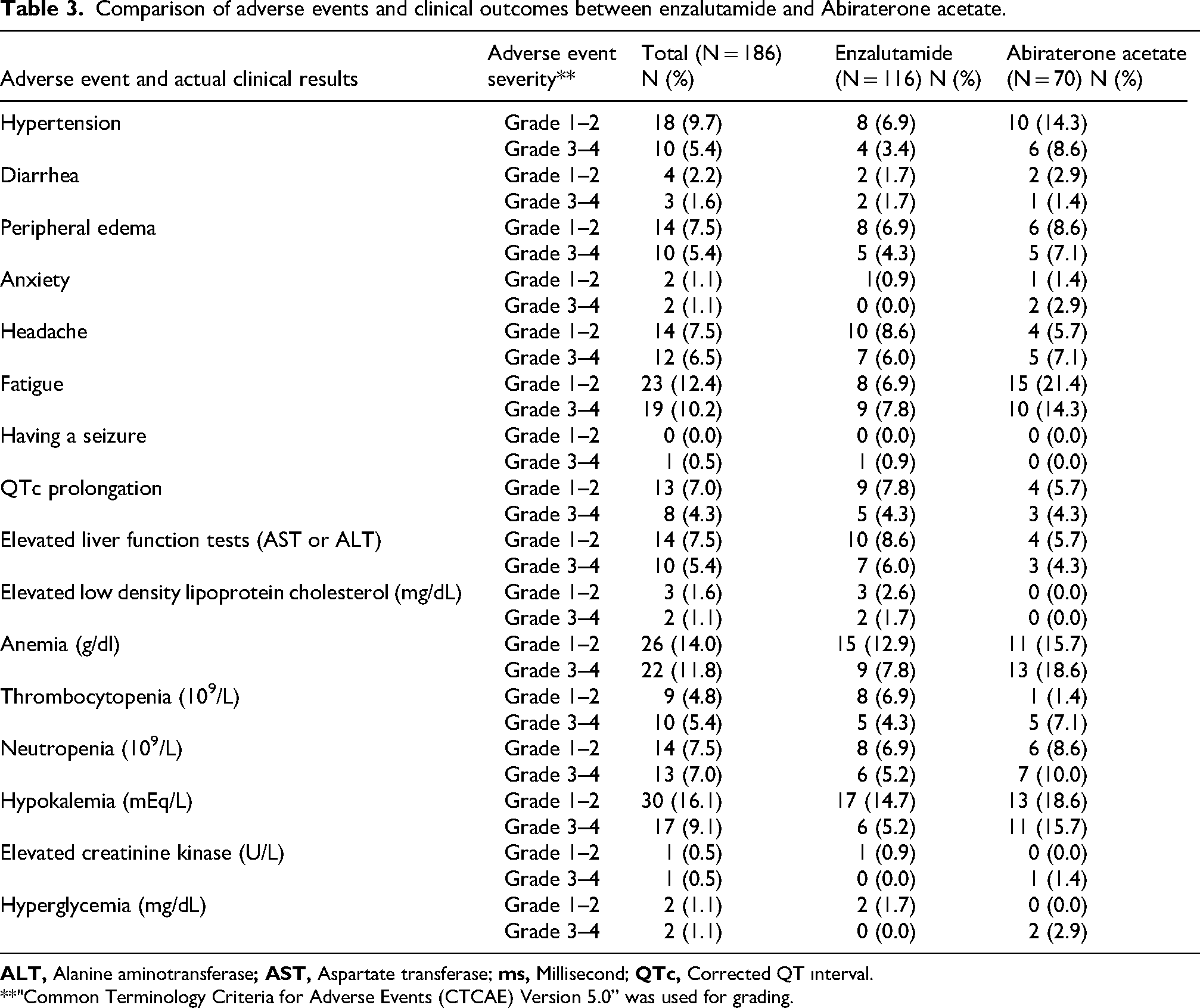
**"Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0” was used for grading.
Discussion
Polypharmacy may compromise treatment efficacy and increase the risk of adverse events, particularly in geriatric and comorbid patients. In this study, the use of other medications concurrently with ARPi was associated with an increased frequency of neurological, cardiovascular, and metabolic adverse events5,6; however, given the observational design of the study, these findings should be interpreted descriptively rather than as evidence of an independent association.
The prevalence of polypharmacy in our study was found to be 55.4%. This rate is higher than the prevalence rate reported by Krustev et al. (41%) in overall elderly population, and similar to that observed by Chen et al. (54.7%) in a large cohort of older patients with colorectal cancer. Overall, the prevalence observed in our cohort was higher than that reported in the general elderly population and similar to that observed in older patients with colorectal cancer.
In the present study, polypharmacy was defined as the concurrent use of five or more medications, including ARPi therapy, in accordance with the most commonly accepted definition in geriatric and pharmacoepidemiologic research.7,8 Although inclusion of ARPi in the total medication count may have contributed to a higher estimated prevalence, this approach was intentionally adopted to reflect the overall treatment burden encountered in routine oncology practice. Nevertheless, this definition does not distinguish between appropriate and potentially inappropriate prescribing, nor does it account for the clinical necessity of individual medications, which should be considered when interpreting the reported prevalence of polypharmacy.
Considering that polypharmacy is associated with an increased risk of adverse effects and reduced treatment efficacy, our findings underscore the necessity of regular and comprehensive medication reviews to optimize pharmacotherapy management.9,10
In the subgroup of patients who were on analgesic medication, 53 patients (28.5%) were on tramadol, making it the most commonly used and the most frequently prescribed analgesic in our cohort
Enzalutamide monotherapy has been associated with seizures at an incidence rate of 0.6 to 1.0%, as reported in prominent randomized trials such as AFFIRM and PREVAIL.12,13 Concomitant administration of tramadol and enzalutamide has been demonstrated to augment the risk of seizures. 14 In our cohort, one seizure event was observed among patients receiving concomitant tramadol and enzalutamide, corresponding to 0.5% of the overall study population and 3.2% (1 out of 31) of patients exposed to this combination. Given that this observation is based on a single event, no causal inference or definitive association can be established. Rather, this finding should be interpreted as a clinically relevant safety signal requiring confirmation in larger prospective studies.
QTc prolongation has been identified as an adverse effect associated with various anticancer agents, including androgen receptor pathway (ARP) inhibitors. 15
However, major randomized controlled trials investigating enzalutamide and abiraterone acetate in prostate cancer have not reported significant QTc prolongation as a frequent or prominent adverse event.16–19 Furthermore, to date, no published studies have provided precise incidence rates of QTc prolongation specifically attributable to these ARPi.
Nevertheless, the interpretation of QTc prolongation in our study is limited by the absence of baseline QTc measurements and the inability to adjust for concomitant use of QT-prolonging medications. Therefore, QTc changes observed in our cohort cannot be attributed to ARPi therapy alone with sufficient certainty, and should be interpreted within the context of multiple potential pharmacological contributors.
In contrast, tramadol, a frequently prescribed analgesic, has been associated with QTc prolongation in approximately 1.5% of patients when used at therapeutic doses. 20 However, in our patient group, grade 3–4 QTc prolongation was detected in 5 patients using enzalutamide and 3 patients using abiraterone acetate. In the context of the use of additional medications, it is noteworthy that 8 patients with grade 3–4 QTc prolongation in our cohort were also taking tramadol. Based on our literature search, there are studies that support our study data and emphasize that tramadol prolongs QTc. 21 Moreover, prior studies have shown that escitalopram and ondansetron also have the potential to induce QTc prolongation.14,22 Indeed, in our study, one of the patients with grade 3–4 QTc prolongation was using escitalopram and tramadol concurrently, and one was using ondansetron and tramadol, concurrently. Given the limited number of events and the presence of multiple concomitant medications with known QT-prolonging potential, these observations should be interpreted cautiously and should not be considered evidence of a direct association with ARPi therapy. Rather, they may represent safety signals requiring further investigation.
In addition, comparisons with pivotal clinical trials such as ARCHES and LATITUDE should be interpreted with caution, as substantial differences in patient characteristics, comorbidity burden, concomitant medication use, and real-world treatment patterns may limit the validity of direct comparisons between study populations.17,19 These methodological differences should be taken into account when interpreting the observed variations in adverse event rates.
In our cohort, the most frequently preferred drug for cardiovascular and dyslipidemia management was atorvastatin. Concomitant use with enzalutamide may reduce plasma concentrations of atorvastatin and its effectiveness in lowering cholesterol levels. 5 Concomitant use of atorvastatin with abiraterone acetate has been associated with myopathy or rhabdomyolysis, accompanied by an increase in plasma concentrations of atorvastatin. Concurrent use of abiraterone acetate and statins has been associated with rhabdomyolysis and renal failure. 23 Grade 3 LDL cholesterol elevation was detected in our 2 patients who received atorvastatin concomitantly with enzalutamide. One patient who used atorvastatin in combination with abiraterone acetate exhibited signs consistent with myopathy and elevated serum creatine kinase levels (2505 U/L) consistent with rhabdomyolysis. As this observation is based on a single case, no definitive association can be inferred, and this finding should be considered hypothesis-generating. Amlodipine ranked sixth among the most commonly used concomitant medications in our study patients. Plasma concentration of amlodipine may decrease when used simultaneously with enzalutamide. 24 Studies have also shown that both enzalutamide and abiraterone acetate can cause hypertension in patients with advanced prostate cancer.25,26 In particular, concomitant use of enzalutamide with amlodipine further increases the risk of blood pressure elevations. In the ARCHES and LATITUDE studies, grade 3 ≥ hypertension was reported in 3.3% and 20% with enzalutamide and abiraterone acetate, respectively.17,19 Although overall incidence of hypertension was lower than that reported in the literature, patients receiving enzalutamide had a lower incidence of grade 3–4 hypertension (3.4%) compared to those receiving abiraterone acetate (8.6%). Two out of three patients who developed hypertension were on amlodipine concomitantly with enzalutamide, and one patient was on amlodipine concomitantly with abiraterone acetate. Large- scale randomized studies of enzalutamide have not highlighted adverse events related to hyperglycemia.16,19
In the ARCHES study, grade 3 ≥ adverse effects included hypertension in 3.3% of patients, and fatigue in 1.7%. 19 In our study, grade 3–4 adverse effects in patients receiving enzalutamide included hypertension with a prevalence of 3.4% and fatigue with a prevalence of 7.8%. In our study, the incidence of grade 3–4 adverse effects was notably higher compared to the ARCHES trial, this difference may be attributed to the differences in patient populations or concomitant medications.
In the LATITUDE study, grade 3 ≥ adverse effects were hypertension with a prevalence rate of 20%, and hypokalemia with a prevalence rate of 10.3%. 17 In our study, grade 3 ≥ hypertension occurred in 8.6%, and hypokalemia occurred in 15.7% in patients receiving abiraterone acetate. Additionally, the rates of anemia and fatigue were found to be higher in our study group, with prevalence rates of 18.6% and 14.3%, respectively. Furthermore, advanced age, presence of comorbidities, polypharmacy, and small subgroup sizes may have contributed to this discrepancy.
Importantly, several adverse events described in this study, including seizure, severe QTc prolongation, and rhabdomyolysis, were observed in isolated or very limited numbers. Therefore, these observations should be interpreted as descriptive safety signals rather than evidence of a causal association, and require confirmation in larger prospective cohorts.
This study has several limitations. First, single-center, retrospective design of the study may limit the generalizability of the findings. In addition, the absence of multivariable analyses due to limited sample size and low event rates precludes assessment of independent associations and causal inferences. The exclusion of adverse events occurring within the first month of treatment may have led to underestimation of early-onset and clinically relevant toxicities. This decision was made to minimize confounding from baseline clinical status and treatment initiation effects; however, this approach should be considered when interpreting the reported safety outcomes. Nonetheless, one of its strengths is that it represents the first investigation to quantify the prevalence of polypharmacy among patients receiving ARPis and to evaluate its potential impact on adverse clinical outcomes in a real-world setting.
Conclusion
Polypharmacy is highly prevalent among geriatric patients with mHSPC receiving ARPIs and may increase the risk of clinically significant neurological, cardiovascular, and metabolic adverse events. These findings highlight the need for comprehensive medication reviews and individualized risk assessment in routine clinical practice. Further prospective studies are needed to clarify the impact of polypharmacy on treatment safety and outcomes in geriatric oncology. The present findings should therefore be interpreted as descriptive and hypothesis-generating rather than demonstrating an independent causal relationship.
Footnotes
Ethical Considerations
The protocol for sample collection was approved by the Basaksehir Cam and Sakura City Hospital Ethics Committee (KAEK/17.01.2024.10) and was carried out according to the principles of the Declaration of Helsinki.
Author contributions
TK and NB researched literature and conceived the study. UO and GUE wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.