
Abstract
Background
Acetylsalicylic acid (aspirin) is a widely used medication with antipyretic, anti-inflammatory, and antiplatelet effects. It also exhibits antitumor properties by enhancing immune responses, downregulating proinflammatory cytokines, and interfering with platelet–tumor cell interactions that promote metastatic dissemination. Identifying effective, safe interventions for brain metastases (BMs) remains a major clinical challenge.
Objectives
This narrative review synthesizes mechanistic, preclinical, clinical, and safety evidence on aspirin's potential role in preventing or modulating brain metastasis and proposes possible preventive and adjuvant strategies for future investigation.
Discussion
The development of BMs involves tumor-derived factors, extracellular vesicles, and recruited host cells that remodel the brain microenvironment into a premetastatic niche. Platelet activation and the COX-1/TXA2 axis promote platelet–tumor cell aggregates, immune evasion, and endothelial adhesion—key steps in metastatic seeding. Aspirin may inhibit these processes by (1) irreversibly blocking platelet COX-1 (reducing TXA2 and aggregation), (2) lowering prostaglandin E2 (PGE2)–mediated immunosuppression, and (3) preserving blood–brain barrier (BBB) integrity. Preclinical and retrospective clinical studies provide supportive but heterogeneous evidence across cancer types. Combination strategies—aspirin with radiotherapy, antioxidants (e.g., ascorbic acid), or immunotherapy—are biologically plausible and supported by limited data. Major safety concerns remain, particularly bleeding risk and intracranial hemorrhage in patients with intracranial disease.
Conclusion
Aspirin is a low-cost, biologically plausible adjunct for metastasis prevention. However, direct evidence in brain-metastasis settings is limited. Prospective trials with mechanistic biomarkers and careful safety monitoring are required to determine optimal dosing, timing, patient selection, and combination strategies.
Background
Brain metastases are the most common neoplastic lesions in the adult central nervous system, with rising incidence driven by improved imaging and prolonged survival among cancer patients. 1 BMs affect nearly 20% of patients with cancer and impose substantial physical and economic burdens. Several malignancies commonly metastasize to the brain, including lung, breast, colorectal, kidney cancers, and melanoma—lung cancer accounting for 39–50% of BMs, while melanoma demonstrates a particularly high propensity for brain colonization. Brain metastases reflect advanced disease and are associated with poor prognosis, significant neurological morbidity, and limited systemic therapeutic options. Consequently, identifying high-risk individuals and optimizing surveillance and preventive strategies are important clinical priorities. 2 The current ASCO–SNO–ASTRO guideline (2021/2022) recommends local treatments—surgery, stereotactic radiosurgery, and/or whole brain radiotherapy—for symptomatic brain metastases; targeted agents such as osimertinib or alectinib may be used for selected asymptomatic patients with driver mutations. 3
Aspirin (acetylsalicylic acid) is one of the most widely used medications globally, applied for pain, fever, inflammation, and antiplatelet prophylaxis. 4 Its antitumor effects are thought to arise from inhibition of prostaglandin synthesis, production of aspirin-triggered specialized pro-resolving mediators (AT-SPMs), reduced platelet activation, and modulation of immune responses.5,6 Moreover, angiogenesis plays a vital role in tumor metastasis and growth and demonstrates the potential of aspirin's antiangiogenic effects as a therapeutic strategy. 7 Low-dose aspirin inhibits COX-2 in lung and colon adenocarcinoma cells and suppresses PGE2 biosynthesis in metastasizing tumor cells, in addition to its effect on platelet COX-1. 8 This, in return, prevents the stem cell mimicry of cancer cells and the enhanced proaggregatory effects induced by platelet–tumor cell interactions. 9 The chemopreventive effect of aspirin aligns with its inhibition of platelet COX-1, which exhibits prolonged action and high potency at low doses. 10 This narrative review examines mechanistic rationale, preclinical findings, clinical evidence, combination strategies, and safety considerations for aspirin use in the context of brain metastasis. Existing data on aspirin for brain metastasis prevention are predominantly preliminary and hypothesis-generating, with overall confidence in the findings remaining modest at best. Therefore, this review draws predominantly from studies on systemic primary cancers (e.g., lung, breast, melanoma) and extrapolates their biological and therapeutic implications to the setting of brain metastasis.
Discussion
The biology of brain metastasis
Brain metastases condition the brain microenvironment before overt invasion, forming a premetastatic niche that permits later colonization. 11 In 1889, Steven Paget published the “seed and soil” concept: tumor cells (the “seed”) require a permissive organ microenvironment (the “soil”) to establish metastases. Primary tumors can condition distant sites through soluble factors, exosomes, and mobilization of bone marrow–derived cells, forming a premetastatic niche that facilitates later colonization. 12
The blood–brain barrier (endothelial cells, pericytes, astrocyte end-feet, basement membrane) becomes more permissive under tumor-derived soluble factors, chemokines, exosomes, and angiogenic signals, causing immunosuppression (macrophage inhibition, reduced cytotoxic/effector T cells), increased release of TNF-α, TGF-β, VEGF, VWF, CECR1-driven PDGF-B upregulation, and platelet COX-1/TXA2 activation that enhances tumor–endothelial adhesion and recruits metastasis-promoting monocytes/macrophages. 11 The primary tumor significantly influences the establishment of premetastatic niches by releasing soluble factors to these sites. 12
Tumor exosomes also reprogram astrocytes and microglia, raising vascular permeability and immunosuppressive signaling. Ye et al. (Mar 2023) showed H1299-derived exosomes induce apoptosis in SVG P12 astrocytes, increase cytokines (GROα/CXCL1, IFN-γ, IL-3, IL-5, IL-15, LIF, M-CSF, NGF, PDGF, VEGF), decrease IL-7, and elevate apoptosis/metabolism-related proteins (MAP2K1, TUBA1C, RELA, CASP6), indicating lung cancer remodels the brain microenvironment to build a premetastatic niche. 13
Metastatic cells reach the brain via blood, lymphatic, or hematogenous routes and must extravasate, survive, and colonize—classically: local invasion, intravascular survival, BBB invasion, then brain colonization and replication.14–16 Platelet–tumor interactions drive hypercoagulability—DTCs bound to platelets generate thrombin, activate platelets, and receive growth factors and TGF-β that promote EMT and invasion; coagulation and platelet activation have been linked to both parenchymal and leptomeningeal colonization.17,18 Similarly, in breast cancer CTCs cluster with platelets, secrete TGF-β to evade NK/IFN-γ, express CD47 and TrkB, and co-express SEMA4D and MYC to aid extravasation and brain colonization. 14 Figure 1 illustrates the mechanism by which brain metastasis develop.
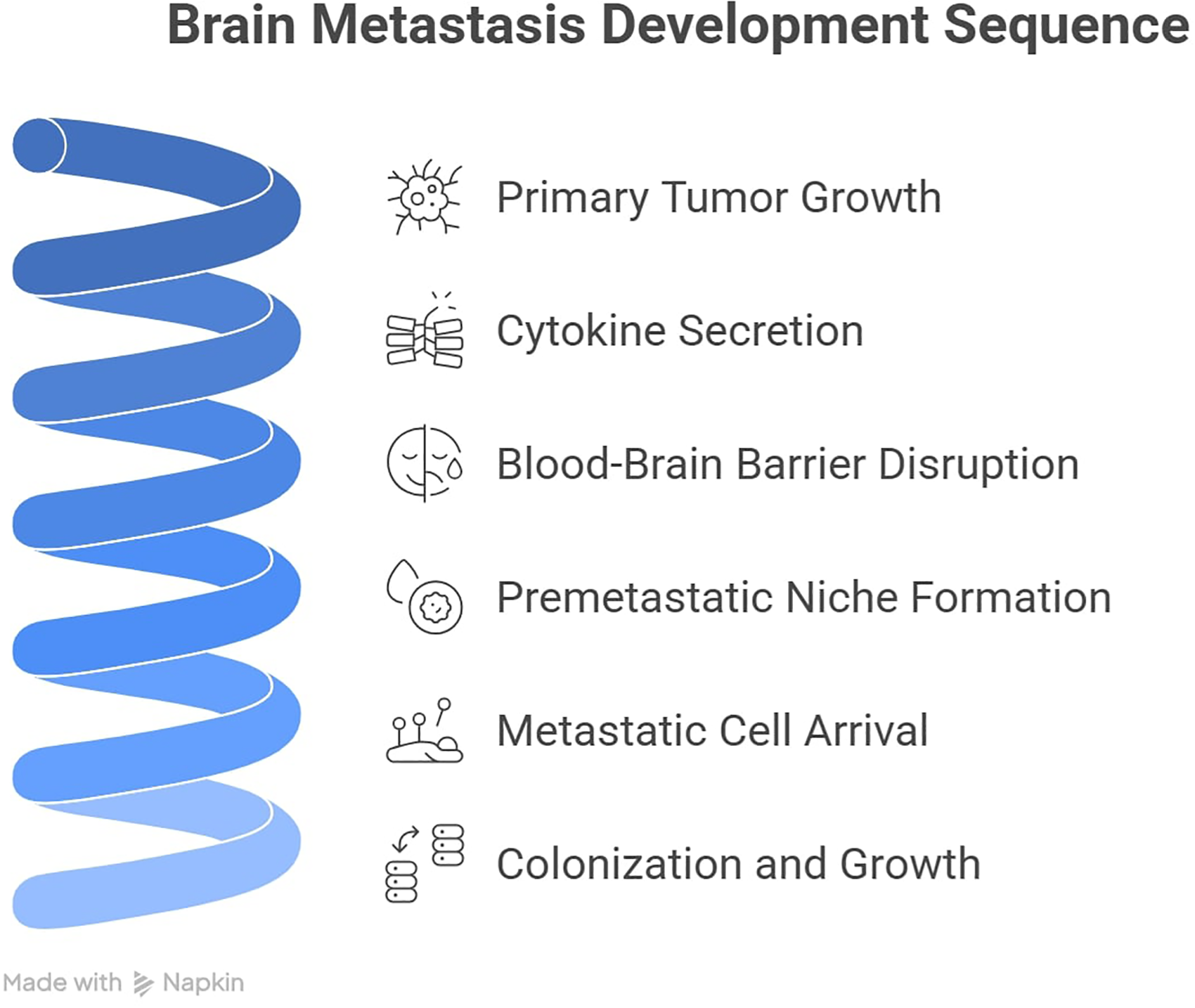
Sequential stages of brain metastasis development: from primary tumor to clinically detectable lesions: (a) primary tumor growth leads to secretion of cytokines (e.g., TNF-α, IL-6, TGF-β) and soluble mediators (e.g., VEGF, MMPs). (b) These factors alter systemic immunity and disrupt blood–brain barrier (BBB) integrity by downregulating tight junction proteins (claudin-5, occludin). (c) A pre-metastatic niche is established in the brain, characterized by activated astrocytes, microglia, and recruited myeloid cells. (d) Circulating tumor cells (CTCs) arrest in brain microvessels, extravasate through the disrupted BBB, and invade the parenchyma. (e) Colonization, proliferative expansion, and co-option of existing brain vasculature lead to (f) clinically detectable brain metastases.
Aspirin pharmacology
Despite more than a century of clinical use, aspirin's pharmacology continues to reveal new insights, particularly regarding its potential in metastatic brain disease. At low doses (typically 75–100 mg daily), aspirin irreversibly acetylates a serine residue at position 529 of the cyclooxygenase-1 (COX-1) enzyme in platelets, effectively blocking thromboxane A2 (TXA2) synthesis for the entire platelet lifespan of about 10 days. 19 This mechanism is not only central to aspirin's antithrombotic efficacy in cardiovascular patients but also appears relevant to cancer biology, as platelet-derived TXA2 has been shown to promote the formation of metastatic intravascular niches. 20 Pharmacokinetically, aspirin is rapidly absorbed from the stomach and upper small intestine, reaching peak plasma levels within 30 min, with an oral bioavailability of approximately 46–51 percent and a short plasma half-life of only about 24 min. 21 Because platelets are anucleated and cannot synthesize new COX-1, even this brief exposure yields sustained antiplatelet coverage, explaining why once-daily dosing suffices despite the drug's rapid clearance. 22 However, enteric-coated formulations — widely used to reduce gastric irritation — delay absorption and may lead to incomplete platelet COX-1 inhibition, particularly in patients with higher body weight. 23
From a clinical application standpoint, the role of aspirin in secondary prevention of cardiovascular events (75–100 mg daily after myocardial infarction, stroke, or peripheral arterial disease) is firmly established. For primary prevention, however, current ACC/AHA guidelines restrict aspirin use to select individuals aged 40–70 years with a 10-year cardiovascular risk of 10 percent or greater, while European guidelines generally discourage its routine use. 24 Major trials such as ASPREE and ARRIVE have shown that the bleeding risk (gastrointestinal and intracranial) often equals or exceeds the modest cardiovascular benefit, especially in older adults. 25 In patients at high bleeding risk — such as those with prior gastrointestinal ulcers or those taking concomitant anticoagulants — adding a proton-pump inhibitor can reduce the risk of upper gastrointestinal bleeding by about 61 percent without adversely affecting major cardiovascular outcomes. 26
Aspirin's mechanisms relevant to metastasis
Aspirin is emerging as an all-round blocker of cancer metastasis to the brain, exerting anti-tumor functions through platelet-dependent, immune, and vascular mechanisms. CTCs activate platelets and adhere to microthrombi; platelet-tumor microthrombi serve as a physical and biochemical barrier. Platelets release proteins like transforming growth factor-β (TGF-β) and platelet-derived growth factors. These proteins suppress cytotoxic lymphocytes and induce an epithelial-mesenchymal transition in tumor cells, enhancing invasive capability. Platelets also release pro-angiogenic and permeability factors (e.g., VEGF, MMPs) to facilitate extravasation of tumors through vascular endothelium into brain parenchyma. 27
Aspirin irreversibly inhibits platelet COX-1, reducing TXA2 synthesis and platelet aggregation. This reduces platelet shielding of CTCs, diminishing survival and adhesion of tumor cells in the circulation.27,28 Preclinical models have shown that aspirin or other COX-1 inhibitors substantially reduce the development of metastatic foci, as would be expected by blockade of “metastatic thrombosis” and cancer cell seeding mediated by platelets. 28
Apart from these anti-platelet effects, aspirin possesses another immune-mediated effect relevant to micrometastatic control by inhibiting TXA2 production. A recent study by Yang et al. demonstrated that platelet-derived TXA2 directly suppresses anti-tumor immunity by triggering a suppressive signal pathway in T-cells. Aspirin treatment in metastasis models in mice led to enhanced T-cell activation and immune-mediated rejection of tumor cells in the lungs and liver. This effect was abrogated when T-cells lacked ARHGEF1 or when TXA2 signaling was maintained. 28
These findings show a novel immunosuppressive pathway acting through platelet TXA2 and T cells that offers a mechanistic rationale for aspirin's pro-immune, anti-metastatic effect. Effectively, aspirin reinstates the body's inherent tumor vigilance: platelets inactivated, cytotoxic T cells (and most likely NK cells) can identify and kill tumor cells more easily prior to their establishment as brain metastasis.28,29
In addition, aspirin has the ability to improve the anatomical and physiological barriers to brain metastasis. Tumor-secreted inflammatory cytokines have the potential to impair BBB integrity and facilitate tumor extravasation. Aspirin preserves BBB integrity by upregulating tight junction proteins in the cerebral microvasculature. Several in vitro studies using brain microvascular endothelial cells, suggested that aspirin increases the expression of tight junction proteins such as zonula occludens-1 (ZO-1) and occludin, thereby, decreasing endothelial monolayer permeability. This effect is correlated with reduced transit of cancer cells across the barrier. 30 These findings suggest that aspirin's protective action in the brain could be partly due to its anti-inflammatory actions on the endothelium.
In general, aspirin has an overall anti-metastatic effect that directly relates to cancer spreading to the brain. It disrupts platelet-tumor cell communication that sustains metastatic survival, transport, and seeding. Moreover, it eliminates platelet-mediated colonization-induced immune suppression, thus giving T-cells the capacity to eliminate nascent metastasis.27,28 At the same time, aspirin fortifies vascular barriers, making the brain a less permissive “soil” for cancer “seeds” in circulation. 31 Figure 2 represents the anti-metastatic effects of aspirin.
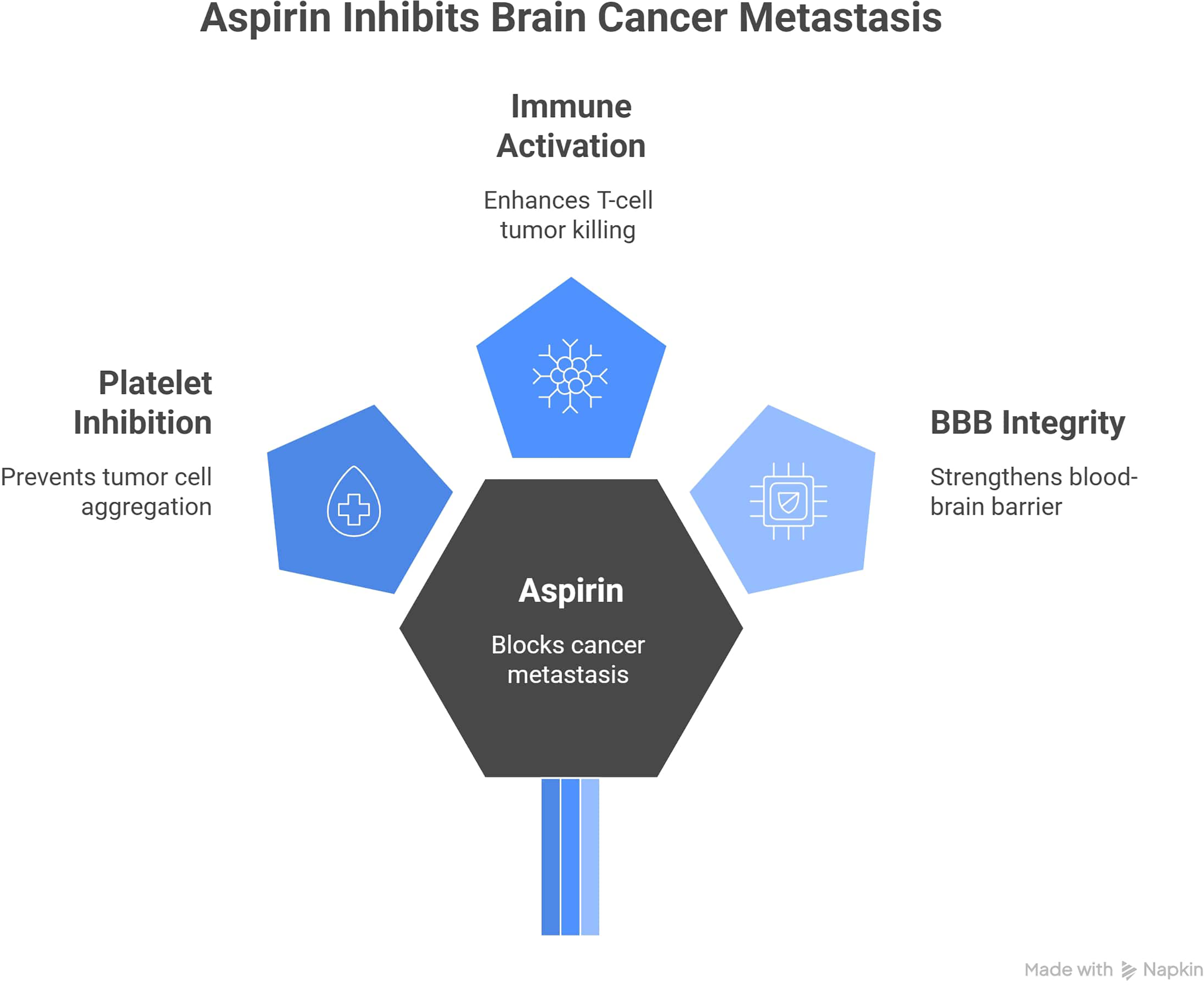
Proposed anti-metastatic mechanisms of aspirin in the brain metastatic niche.
Evidence linking aspirin to metastasis
Recently, there has been emerging evidence suggesting the anti-metastatic role of aspirin, primarily through selective cyclooxygenase (COX)-1 and COX-2 inhibition and prevention of platelet activation. 32 This evidence is supported by several preclinical and clinical studies across several types of cancer.
Colorectal cancer
M. Kane et al. conducted a preclinical study published in 2021, which aimed to assess aspirin's preventive effect in a murine model of BRAf mutant serrated colorectal neoplasia. They fed BrafV637E/+ and Villin-CreERT2/+ mice either a control diet or an aspirin-supplemented diet (equivalent to low-dose human aspirin). As a result, aspirin did not lower the incidence of serrated lesions or carcinomas, but it significantly reduced the size of the lesions. However, among mice that developed carcinoma, metastasis occurred in 35% of controls compared to 5% of aspirin-treated mice (RR 0.69, 95% CI 0.48–0.90, P = 0.0134). Moreover, metastatic carcinomas frequently expressed upregulation of NOTCH, FGFR, and PI3K/AKT signaling, which were downregulated among aspirin-treated mice. These results suggest that the main benefit of aspirin lies in reducing the incidence of metastasis rather than preventing Braf-mutant carcinoma. 33
Additionally, in a Danish nationwide retrospective cohort study, including 32,195 patients with incident colorectal cancer (CRC), Agustsson et al. reported lower cancer-related mortality rates among aspirin users (HR 0.88; 95% CI 0.83–0.94). Moreover, this effect was more pronounced in localized tumors, which further supports the underlying antimetastatic mechanism of aspirin. However, researchers did not assess the duration of aspirin use or collect data on former aspirin use before the diagnosis, which may mistakenly place former users in the non-user group. 34
A non-randomized controlled trial conducted by Novin et al. assigned 90 patients to receive standard neoadjuvant CRT either with (n = 45) or without (n = 45) daily 100 mg aspirin. The primary outcome was the pathological complete response (pCR) rate. Additional outcomes included tumor regression grade (TRG) and tumor down-staging, which are critical surrogates of reduced metastatic formation. The aspirin group showed a significantly higher rate of tumor down-staging (47%) compared to the control group (24%) (P < 0.001). Nevertheless, the authors observed a significantly higher pCR rate among aspirin users (26.6% vs. 17.7%, P < 0.001). These effects are thought to result from the inhibition of COX-2. However, the fact that this study was conducted in only two centers, with a small sample size, and a non-randomized, non-blinded design, may introduce bias and limit the generalizability of the findings. 35
These findings do not align with the results reported in the large retrospective observational study conducted by Giorli et al. and published in The British Pharmacological Society journal in 2020. They identified 7478 patients newly diagnosed with non-metastatic CRC between 2000 and 2013 using Italian primary care data. Among them, 1509 used aspirin prior to diagnosis. Patients were followed-up for a mean of 4 years, and Cox models were used to compare the risk of death or metastatic formation. The adjusted analysis found no evidence of decreased metastatic formation with prediagnostic aspirin use (adjusted HR 0.88; 95% CI 0.63–1.22). There was no significant trend showing that longer use was associated with a lower metastasis risk (P-trend = 0.22). Furthermore, the authors suggest that the potential survival benefit among aspirin users may be attributed to bleeding events caused by aspirin, which lead to an earlier diagnosis of the cancer. Although this study lacked data on the initial tumor stage, which is a critical prognostic factor that could confound the results, it highlights a crucial distinction: pre-diagnostic aspirin use may not impact metastasis risk, while post-diagnostic use might. 36
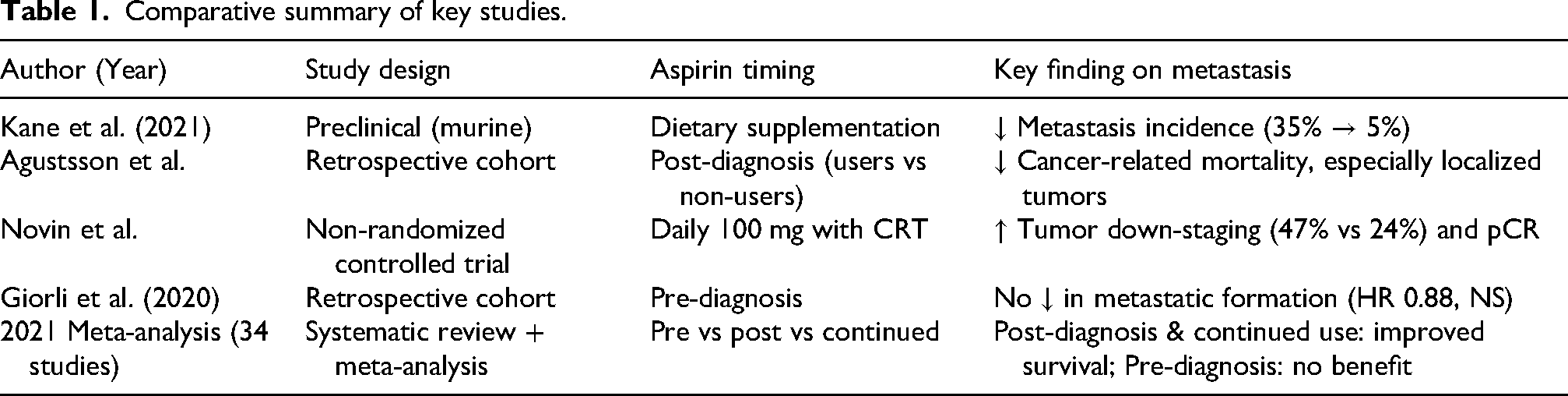
In colorectal cancer (CRC), a systematic review and meta-analysis study published in 2021 divided 950,365 patients from 34 studies into three groups according to the time of aspirin use, which are pre-diagnosis use, post-diagnosis use and continued use. The study showed that aspirin post-prognosis users had an improvement in all-cause mortality and not only CRC-specific mortality, whereas pre-diagnosis users had no improvement in CRC-specific mortality or all-cause mortality. In contrast, continued users had improvements in both CRC-specific mortality and all-cause mortality. The improvements in all-cause mortality probably return to aspirin's effect on the cardiovascular system since cancer increases the risk of some cardiovascular diseases (eg, thromboembolism). The positive influence of aspirin on mortality seemed to be more obvious in tumors with PIK3CA mutation or COX2 overexpression. 37 Collectively, these studies reveal a recurring pattern: aspirin's primary antimetastatic effect may be more consistently observed with post-diagnosis or continued use rather than pre-diagnostic use. However, major limitations across studies — including non-randomized designs (Novin et al.), lack of dosing duration data (Agustsson et al.), absence of tumor staging (Giorli et al.), and predominantly colorectal cancer focus — limit direct extrapolation to brain metastasis. Future studies specifically in brain metastatic models are urgently needed. Table 1 represent a summary of the studies mentioned and their key findings.
Comparative summary of key studies.
Lung cancer
Wei et al. conducted an in-vitro study using a co-culture model of rat brain microvascular endothelial cells (rBMECs) and astrocytes. The study aimed to investigate the mechanism by which aspirin may inhibit brain metastasis in lung cancer, with a specific focus on its effect on the BBB. They reported that aspirin could inhibit brain metastasis of lung cancer through the upregulation of tight junction protein expression of BBB endothelial cells, particularly heat shock protein 70 (HSP 70), zonula occludens-1 (ZO-1), and occludin. They also indicated that aspirin could inhibit the migration of lung cancer cells and reduce the permeability of the BBB in a time-dependent manner. Despite this, their findings may not be generalizable to other cancer types because they are based only on one type of cancer cell. 30
Similarly, a nationwide, population-based retrospective cohort study was conducted in Taiwan by Chuang et al., to investigate the influence of aspirin use on overall survival among inoperable non-small cell lung cancer (NSCLC). The authors used propensity score matching (1:1) to create a balanced cohort of 4932 aspirin users and 4932 non-users. The study reported that aspirin use was associated with a statistically significant 21% reduction in the risk of death (adjusted HR: 0.79; 95% CI: 0.75–0.83) and a longer median overall survival compared to non-users, indirectly indicating a potential role of aspirin in preventing disease progression and metastatic spread. However, the study did not include cancer-specific staging and histology data, which are important factors that affect survival. 38
Aiad et al., conducted a single-center retrospective study that analyzed 500 NSCLC patients treated with PD-1 or PD-L1 inhibitors. Patients were categorized based on their aspirin use. Notably, the combination of aspirin and PD-L1 inhibitors (e.g., durvalumab, atezolizumab) was independently associated with a 56% reduction in the odds of disease progression (adjusted OR: 0.44; 95% CI: 0.27–0.71; p < 0.001) compared to PD-1 inhibitors with ASA. However, no significant benefit regarding 18-month survival was observed between the ASA and non-ASA groups (50.3% vs. 49.7%, p = 0.79). The findings suggest that the benefit of ASA is not universal but may be contingent on the type of immunotherapy used, highlighting a potential strategy for improving outcomes in patients on PD-L1 blockade therapy. 39
Martín-Abreu et al., studied 650 patients with non-small cell lung cancer and concluded that antiplatelet users (predominantly low-dose aspirin) had a significantly reduced risk of late brain metastasis when compared with non-users. Only ∼7% of aspirin users developed brain metastasis, in contrast to ∼20% of unexposed controls, despite the aspirin group being older and with increased comorbidities. This translated into a longer interval to brain metastasis: median 77.5 months with aspirin versus 62.6 months in controls, and improved progression-free survival. On another perspective, patients who initiated aspirin upon diagnosis virtually had no cases of brain metastatic dissemination in the follow-up period, suggesting a window of opportunity for prevention of early metastatic seeding. The study determined that aspirin (and antiplatelet drugs in general) can disrupt key stages of the metastatic cascade, with fewer brain lesions. Moreover, long-term aspirin did not increase the rate of intracranial hemorrhage in these patients, alleviating an issue that otherwise would be present when using blood-thinning therapy for cancer. 31
One of the very few studies addressing the effect of aspirin on brain metastasis is the retrospective study conducted by Abreu et al. and recently published in 2025, which suggested a potential association between antiplatelet therapy (including aspirin) and a lower incidence of brain metastasis among non-small cell lung cancer (NSCLC). Moreover, they linked antiplatelet therapy with a longer mean time to metastasis development and a longer progression-free survival (PFS) time. Additionally, this effect was more notable among patients who were at advanced stages and who initiated antiplatelet therapy after diagnosis. However, this was a single-center study on one type of cancer and analyzed the effect of antiplatelets as a composite without providing data about aspirin alone, which may undermine the findings. 31
Across the studies presented, a consistent signal emerges that aspirin may reduce brain metastasis risk in non-small cell lung cancer (NSCLC), though the proposed mechanisms and clinical contexts vary. A critical gap remains: none of these studies prospectively assessed brain metastasis as a primary endpoint, and the Abreu et al. study grouped aspirin with other antiplatelets, limiting specificity. Nevertheless, the convergence of preclinical mechanistic evidence and retrospective clinical data supports further prospective investigation of aspirin specifically for brain metastasis prevention in NSCLC.
Breast cancer
Miller et al. conducted a preclinical study investigating the effect of pretreatment aspirin administration on the biology of breast cancer and metastasis. They used specific models, such as HER2 + and triple-negative breast cancer (TNBC). Although high-dose aspirin significantly delayed the time to develop metastasis in the HER2+ MDA-MB-231/LN2-4/H2N model, it did not improve the overall survival rates in other models, such as trastuzumab-resistant HER2+ (HCC1954) and TNBC patient-derived xenograft (PDX) models. The mechanism of action is thought to be the reduction of angiogenic and lymphangiogenic factor secretion from mesenchymal stromal cells (MSCs), preventing endothelial tubule formation in vitro and inhibiting metastatic formation. 32
Feinauer et al. found opposite results in their preclinical study on the JIMT-1 breast cancer cell line, a HER2 + and trastuzumab-resistant type. Antiplatelet therapy (including aspirin) was not associated with lower metastatic incidence, whereas anticoagulants were. These observations can be attributed to the mechanism by which cancer cells spread. Tumor cells highly express tissue factor (TF), triggering the coagulation cascade and facilitating extravasation. Therefore, clot formation was an indispensable prerequisite for brain colonization, and the influence of antiplatelet therapy against this mechanism was not significant. 40
Additionally, Chen et al. reported in their phase III, randomized, placebo-controlled trial involving 3020 patients a 27% higher risk of recurrence or death in the aspirin group, though this was not statistically significant. The hazard ratio (HR) for invasive disease-free survival (IDFS) events was 1.27 (95% CI, 0.99–1.63; P = .06). Moreover, 77 distant metastatic events were reported in the aspirin group, compared to the placebo group that had 67 events. These results crossed the prespecified threshold of futility (HR > 1.03), which led to early termination of the trial without completing the prespecified follow-up period (5 years). The early termination of the trial, combined with the overrepresentation of patients with hormone receptor-positive (88.6%) and node-positive (88.9%) disease, may affect the credibility and generalizability of the findings. Overall, this study suggests that aspirin should not be recommended as an adjuvant therapy for patients diagnosed with high-risk, ERBB2-negative, nonmetastatic breast cancer. 41
Unlike the consistent antimetastatic signals observed in colorectal and lung cancers, evidence for aspirin in breast cancer is discordant and largely negative. Collectively, findings indicate that aspirin's antimetastatic effects are cancer-type dependent.
Other types of cancers
The 2021 study by Zou et al. investigates the mechanism by which aspirin (acetylsalicylic acid, ASA) enhances the efficacy of chemotherapy and acts as a chemopreventive agent in oesophageal squamous cell carcinoma (ESCC), with a specific focus on targeting cancer stem cells (CSCs), which are key drivers of therapy resistance and recurrence. The authors discovered a synergistic therapeutic effect between aspirin and cisplatin in inducing tumour regression in xenograft mouse models, which was not achieved by either drug alone. Moreover, ASA caused extensive chromatin remodelling, particularly in putative CSCs (pCSCs), leading to altered gene accessibility. This was linked to increased histone acetylation. In the NMBzA-induced rat ESCC model, ASA treatment significantly reduced tumour incidence, multiplicity, and volume and delayed the progression from precancerous lesions to carcinoma. This preclinical study suggests that ASA therapy sensitizes CSCs to chemotherapy. Further research is required to assess if these specific mechanisms operate in cancers that metastasize to the brain. 42
On the other hand, Patel et al., conducted a national retrospective cohort study and investigated the relationship between aspirin use and the incidence of metastasis among esophageal cancer patients. They used multivariate logistic regression to calculate adjusted odds ratios (aORs). They found that aspirin users had significantly lower rates of metastatic disease at hospitalization than the non-user group. This antimetastatic effect remained consistent across different types of metastasis (GI-related and non-GI-related). However, no significant reduction in lymphoid metastasis was observed. The authors did not provide data regarding specific subtypes of esophageal cancer (adenocarcinoma vs. squamous cell carcinoma) and did not discuss the time at which aspirin was initiated (pre- vs. post-diagnosis). These limitations may confound the results; thus, they must be interpreted as a strong association but not as evidence of efficacy. 43
Similarly, Perlow et al. conducted a multicentric, retrospective cohort study including 237 patients diagnosed with high- or very high-risk prostate cancer and treated with definitive radiotherapy. They observed no association between aspirin and higher 4-year progression-free survival (PFS) rates compared to the non-user group. These findings indicate that aspirin is not linked to reduced distant metastasis or prevention of disease progression. However, the use of aspirin could be an indication of cardiovascular diseases that could influence the outcomes. Moreover, the study included only high-risk patients, which limits the generalizability of the results. 44
Despite robust preclinical rationale, the clinical certainty that aspirin reduces brain metastatic burden remains low-to-moderate, with current studies largely restricted to generating rather than validating definitive hypotheses. Where available, trials and cohort analyses should be interpreted in light of selection bias, dose differences, concomitant therapies, and bleeding risk.
Comparative strength of evidence across cancer types
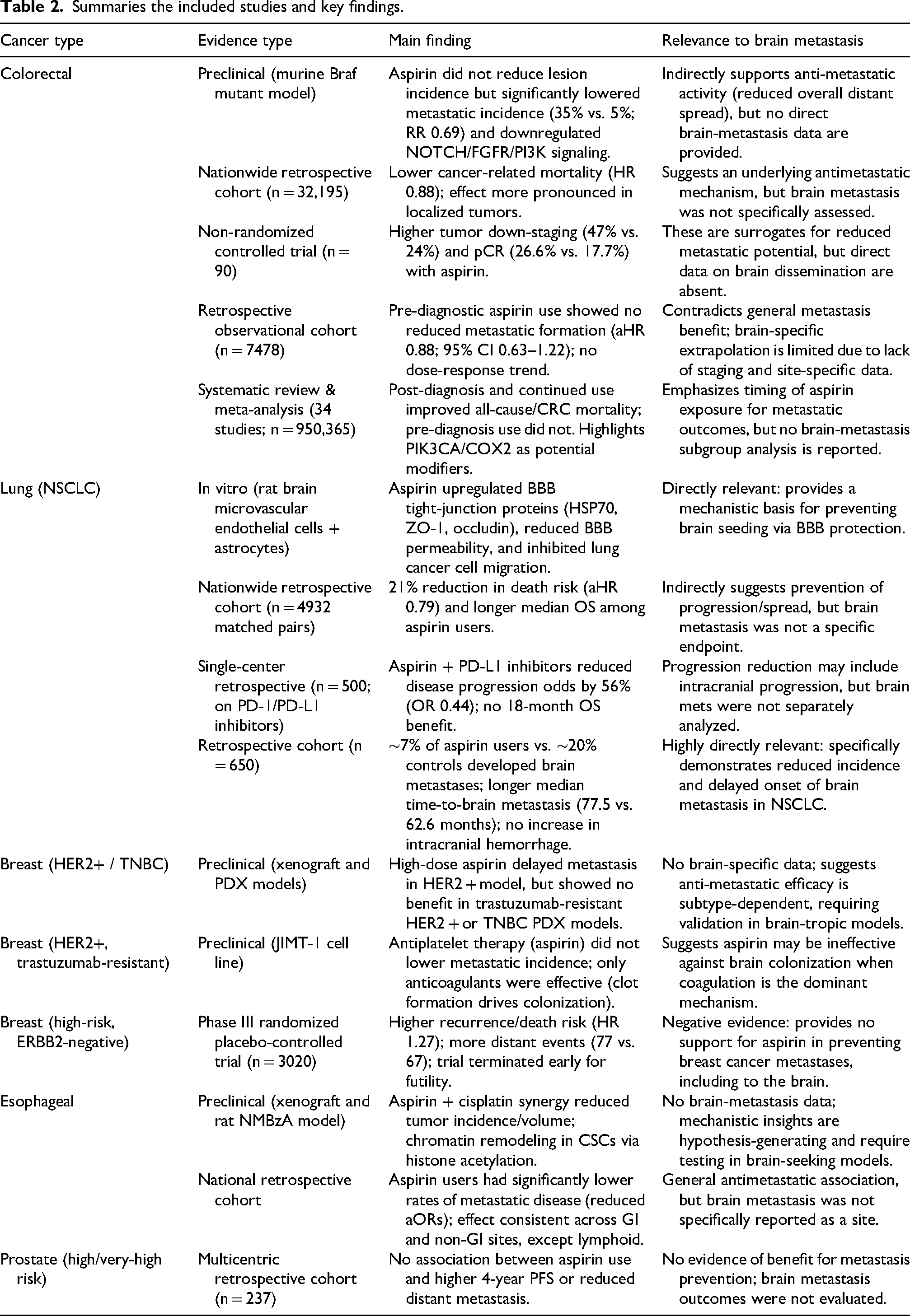
Across tumor types, aspirin's antimetastatic signal is strongest and most consistent in colorectal and NSCLC cohorts and meta-analyses, weaker and discordant in esophageal cancer, and largely absent or negative in breast and prostate cancer. Preclinical data often support benefit, but human evidence is heterogeneous, cancer-specific, and limited by observational designs and bias. Preclinical murine and in-vitro studies plus multiple retrospective cohorts and one small non-randomized trial provide low–to–moderate level, largely hypothesis-generating evidence. Results suggest a possible antimetastatic and survival benefit for post-diagnosis/continued aspirin in CRC and NSCLC, but inconsistent or negative data in breast and prostate cancer, with substantial confounding and bias. Table 2 summaries the included studies and key findings.
Summaries the included studies and key findings.
Aspirin safety for cancer patients
Bleeding is a serious side effect of aspirin, and this risk should be balanced against the reduced risk of cancer. A systematic review and meta-analysis of 118 observational studies of aspirin and 18 cancers in 2021 aimed to test whether taking aspirin is associated with an increase in the survival of patients with cancer. Many authors of the 118 studies had little or no knowledge about bleeding in their patients, since they built the studies on recorded data with no direct contact with the patients. Other authors mentioned the expected excess in GI bleeding in aspirin patients, while only a few authors reported fatal bleeds. One of the studies was a cohort of over 18,000 colon cancer patients, and it showed that deaths from GI bleeding in aspirin users were 0.40% compared with 0.36% in non-aspirin users. Furthermore, it mentioned that taking PPI along with aspirin had reduced bleeding in the patients. Another study mentioned that 3% of aspirin patients and 3.2% of non-aspirin patients had had a fatal bleed. A different study of liver cancer patients who were treated by transarterial chemoembolization reported that six patients who were aspirin users and seven patients who were non-aspirin users had died because of upper GI bleeding. 45
A systematic review and meta-analysis designed in 2023 to assess the relationship between aspirin and the risk of incident HCC was conducted on MEDLINE, Embase, Scopus, and PubMed databases and included 12 cohort and 4 case-control studies involving 36,698 aspirin users. The meta-analysis conducted on three studies found that the use of aspirin was linked to a slight yet statistically significant rise in the risk of bleeding (adjusted HR 1.11, 95% CI 1.02–1.22, p = 0.02), with no notable statistical heterogeneity observed (I2 = 0%, p = 0.54). A consistent finding of roughly a 10% increase in bleeding risk was observed in the other study as well. 46
A retrospective cohort study in 2023 aimed to demonstrate the relationship between antiplatelet medication and intracranial hemorrhage (ICH) in patients with primary brain tumors. The study included 387 patients, with 130 exposed to antiplatelet agents and 257 not exposed. The one-year cumulative incidence of any intracranial hemorrhage (ICH) was observed to be 11.0% (95% CI, 5.3–16.6) among individuals taking antiplatelet medications, compared to 13.0% (95% CI, 8.5–17.6) in those not on such medications (Gray test, p = 0.6). The cumulative incidence of major ICH was comparable between the two groups, with 3.3% in the antiplatelet group and 2.9% in the control group, yielding a p-value of 1.0. 47
A matched cohort study was conducted in 2022 to evaluate the influence of antiplatelet agents on the risk of ICH. The study cohort comprised 392 patients with metastatic brain tumors, of which 134 were treated with antiplatelet agents, while 258 served as control subjects. The cumulative incidence of any ICH at one year was 19.3% (95% CI, 14.1–24.4) in patients who were not treated with antiplatelet agents, while it was 22.5% (95% CI, 15.2–29.8; P = .22, Gray test) for those who were receiving antiplatelet therapy. The cumulative incidence of major ICH was 5.4% (95% CI, 2.6–8.3) in the control group compared to 5.5% (95% CI, 1.5–9.5; P = .80) in those taking antiplatelet agents. 48
Studies indicate that antiplatelet medications may increase intracranial bleeding risk in patients with intracranial disease. Concomitant use of gastroprotective agents (e.g., proton pump inhibitors) may mitigate GI bleeding risk but does not address intracranial hemorrhage risk. Patient selection, careful monitoring, and inclusion of bleeding outcomes in trials are essential.
Aspirin in combination strategies: translational insights for oncology practice
Recent studies suggest that combining aspirin with other treatments may improve its efficacy against metastatic brain tumors.28,30 This section discusses three combination strategies: radiotherapy, antioxidants such as ascorbic acid, and immunotherapy.
Many preclinical studies report potential when aspirin is paired with radiation therapy: for example, an in vivo 2021 study by Shubhankar Suman et al. investigated dietary aspirin's influence on PGE2 levels in genetically modified mice exposed to high-energy radiation and at elevated risk of intestinal tumors, finding that aspirin-supplemented mice had lower post-irradiation PGE2 levels. 49 Which suggests aspirin may reduce radiation-induced inflammation and improve therapeutic effectiveness. In a 2024 review, Ji Man Low and colleagues examined repurposing safe drugs, including aspirin, as radiotherapy enhancers across more than 100 preclinical and clinical studies of tumors with inflammatory and immunosuppressive microenvironments (e.g., brain and lung), analyzing effects on PGE2 signaling and immune pathways and concluding that aspirin's dual actions—reducing inflammation and activating cell-death pathways such as p53—may increase radiosensitivity. 50 Likewise, a 2023 review by Levis et al. of strategies for brain metastasis from lung cancer treated with stereotactic radiation (SRS/SRT) synthesized clinical, case series, and preclinical data and highlighted biological factors that modulate radiation response—chronic inflammation, elevated COX-2 and PGE2, PTEN loss, hypoxia, and immune contexture—concluding that controlling these factors (for example with controlled-dose aspirin) may improve radiation success and protect healthy tissue. 51
Some research also suggest combining antioxidants with aspirin to counter metastasis-related processes: a 2024 preclinical study by Nada M. El Ezaby et al. used 80 mice bearing solid tumors divided into aspirin-only, ascorbic acid-only, combination, or untreated groups and found that the aspirin + ascorbic acid group showed greater tumor growth suppression, reduced oxidative stress, and enhanced immune parameters compared with either agent alone. 52 A 2025 narrative review by Wang et al. examined oxidative stress–inflammation crosstalk in cancer and brain metastasis, emphasizing roles for ROS and PGE2/NF-κB signaling and proposing that combining anti-inflammatories like aspirin with antioxidants could remodel the improve responses to radiation or immunotherapy. 53
Recent evidence also suggests further investigation for the potential therapy of aspirin as an adjunct to enhance the effectiveness of antitumor immunotherapy. A preclinical study published in 2025 by Yang and colleagues aimed to investigate the role of aspirin in restoring anti-tumor T cell cytotoxicity in metastasis models with immune suppression driven by platelets. This study involved animal models with tumor metastasis characterized by peritumoral platelet accumulation and elevated production of Thromboxane A2 (TXA2), which activates the ARHGEF1 pathway that restricts T-cell function. These models were treated with aspirin as a COX-1 inhibitor to reduce TXA2 production, and T-cell function was monitored. The results show that aspirin may successfully suppressed the inhibitory effect of platelets, restoring the cytotoxicity of T cells and increasing their effectiveness in attacking cancer metastasis. These findings open prospects for the use of aspirin as a supportive agent to improve the immune response against metastatic cancer. 28
Clinically, immune checkpoint inhibitors (e.g., anti-PD-1, anti-CTLA-4) improve prognosis in some metastatic cancers (such as melanoma) but many patients do not respond, potentially due to immunosuppressive prostaglandin and platelet pathways; a recent phase II trial adding high-dose aspirin to dual checkpoint blockade (pembrolizumab + ipilimumab) in advanced melanoma did not significantly raise the overall response rate (∼63%, comparable to immunotherapy alone) yet subset analyses hinted at benefit—patients who tolerated and continued aspirin during induction showed significant survival improvements and immunologic correlates (differential cytokine changes and increased proliferating FoxP3+ Tregs) associated with favourable outcomes—although higher bleeding-related toxicities led to trial interruption before the efficacy time point. 29 Complementary preclinical work by Liu et al., in 2024 investigated aspirin's effects on colon cancer via the TIGIT-BCL2-BAX axis using Jurkat T cells and mouse models with high TIGIT expression and found aspirin reduced TIGIT and BCL2, increased BAX, promoted apoptosis, and lowered pro-tumor cytokines, supporting its immunomodulatory adjuvant potential. 54
From a retrospective clinical perspective, Mina Aiad et al.'s 2022 study of 500 NSCLC patients treated with immune checkpoint inhibitors (PD-1/PD-L1), some of whom used low-dose aspirin (81 mg daily), reported that aspirin use was associated with a significant reduction in disease progression (AOR = 0.44, p < 0.001) and a non-significant trend toward more complete responses with PD-L1 inhibitors, consistent with the hypothesis that aspirin-mediated PGE2 inhibition may enhance antitumor immunity in patients. 39
Altogether, these preclinical, retrospective, and early clinical signals raise the possibility that thoughtfully combining aspirin with radiation therapy, antioxidants such as ascorbic acid, or immunotherapies could improve control of metastatic brain tumors and reduce harm, and that further mechanistic studies and well-designed clinical trials are warranted to translate these simple, promising combinations from bench to bedside.
In practical terms, low-dose aspirin (75–100 mg daily) initiated after cancer diagnosis shows the most consistent signal of benefit, particularly in NSCLC and colorectal cancer. However, its use for brain metastasis prevention is not yet standard of care. Oncology pharmacists should screen for contraindications (bleeding risk, thrombocytopenia, anticoagulant use) and only consider aspirin as an adjunct within clinical trials or after multidisciplinary discussion of individual risk-benefit profiles Figure 3 demonstrate the potential of combining aspirin with other treatment strategies as an adjuvant therapy.
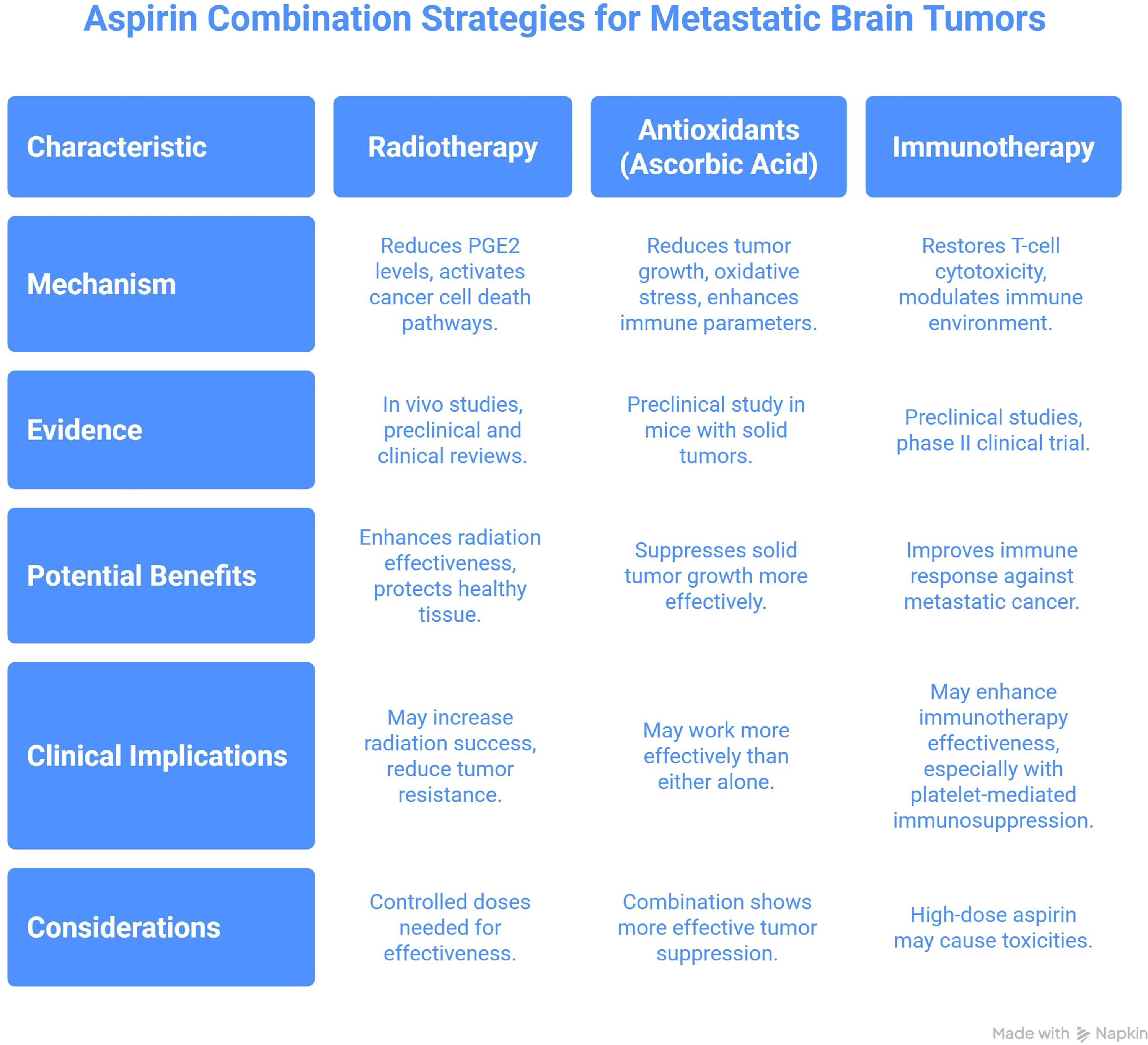
Aspirin combination strategies for metastatic brain tumors: rationale and current evidence.
Future directions
Integrating AI and radiomics into clinical workflows shifts imaging to quantitative data, improving drug delivery and patient stratification.55,56 Yet direct radiomics-based assessments of aspirin's anti-metastatic effects are rare. insights can be drawn from related drug studies, for example a 2022 multicenter trial (n = 113 glioblastoma, mean 55y) using MRI radiomics with random survival forest predicted PFS/OS (C-indices 0.680–0.715 and 0.692–0.750). 57 Moreover, DiCenzo et al. applied pretreatment quantitative ultrasound radiomics in 82 breast cancer patients; K-nearest neighbors yielded 91% sensitivity, 83% specificity, and 87% accuracy, illustrating applicability for risk stratification and drug studies including aspirin. 58 In 226 node-positive breast cancer patients, post-NAC chest CT radiomics (AUCs 0.812, 0.762, 0.832) outperformed qualitative reads (0.642), with clinical-radiomics models reaching 0.866. 59 AI-supported drug repurposing is also gaining traction; reviews advocate computational models for repurposing aspirin in colon cancer.60,61 While specific ML data on aspirin's antimetastatic effects remain scarce, these radiomic frameworks offer a translatable strategy for brain metastasis prevention: they could quantify vascular permeability and parenchymal changes non-invasively, enabling early prediction of intracranial aspirin efficacy and patient selection for preventive trials. Moreover, while AI automation reduces diagnostic errors, ethical issues (data bias, security, workforce impacts) must be addressed. 55
Limitations: lack of direct evidence in brain metastasis settings
It is important to emphasise that almost all mechanistic data on aspirin in brain metastasis are extrapolated from systemic cancer models or primary glioma studies. Future research on aspirin use in neuro-oncology must address several key gaps, as current evidence largely extrapolates from systemic cancer cohorts with limited direct data on brain metastases, underscoring the need for prospective randomized controlled trials (RCTs) and well-designed real-world registry analyses to generate high-quality, neuro-oncology–specific evidence. The EANO–ESMO guideline for brain metastasis management highlights that molecular heterogeneity and pathway activation underlie variable therapeutic responses, while current treatment strategies still rely heavily on retrospective studies, reinforcing the urgent need for prospective trials to guide systemic therapy. 62
Another major challenge is optimizing aspirin dosing, as the balance between its antitumor efficacy, antithrombotic benefits, and risk of intracranial hemorrhage may differ substantially in patients with central nervous system involvement compared to other cancers. Amy Lam et al. noted in their study on long-term low-dose aspirin for cancer prevention that bleeding risk increases significantly, even when adjusted with gastroprotective agents like H2RA or PPI. 63 while Richard J. Lin et al. emphasized that patients with primary or secondary brain tumors face both elevated venous thromboembolism (VTE) risk and higher intracranial hemorrhage risk during prolonged anticoagulant or aspirin therapy, necessitating careful dose balancing throughout active cancer treatment. 64 Furthermore, aspirin's therapeutic effects are likely heterogeneous across tumor types, as molecular subtype, genetic mutation status, and tumor biology all shape its antitumor impact; integrative analyses reveal subtype- and mutation-specific vulnerabilities in brain metastases that can guide precision therapies and improve aspirin-related outcomes. 65
A more refined understanding of these molecular and clinical variables will be crucial for improving patient selection, optimizing treatment combinations, and ultimately determining whether aspirin can evolve from a repurposed adjunct to a truly integral component of personalized neuro-oncologic care.
Conclusion
Aspirin remains a low-cost, well-tolerated adjuvant candidate for metastasis prevention, supported by strong mechanistic evidence for its antiplatelet, anti-inflammatory, and immune-modulating actions. Yet, its effects on brain metastases are poorly studied; Current evidence supporting aspirin for prevention of brain metastasis remains low-to-moderate certainty and predominantly hypothesis-generating, with most data extrapolated from systemic cancers. Biologically, aspirin may protect the BBB and disrupt platelet–tumor interactions, but prospective trials are needed to confirm its efficacy, safety, and optimal dosing—particularly in high-risk or brain-metastatic patients. Combining aspirin with targeted or immunotherapies warrants exploration. Integrating advanced technologies such as AI and radiomics introduces a promising precision-oncology dimension. These tools have shown value in predicting treatment response and disease progression in cancers like glioblastoma and breast cancer, transforming imaging into a quantitative, data-driven science. Although radiomics-based models assessing aspirin's metastasis-preventive role remain limited, evidence from other drug trials supports their potential in risk stratification, therapy optimization, and repurposing. AI-assisted aspirin research in colon cancer further reinforces its role in precision medicine. However, ethical challenges—including data privacy, algorithmic bias, and clinical implementation—must be carefully managed. Ultimately, uniting aspirin's biological potential with AI-driven predictive modeling could open new avenues for individualized screening, prevention, and treatment of metastatic disease.
Footnotes
Acknowledgments
None.
ORCID iDs
Ethical considerations
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Authors contributions
NK conceived the study idea, designed the review methodology, led the development of the research protocol, and served as the primary writer of the manuscript. All authors contributed to literature screening, and original draft writing. ZA provided critical revisions, supervised the overall project, and ensured the scientific accuracy and integrity of the final manuscript. All authors reviewed and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data is available from the corresponding author upon reasonable request.