
Abstract
Background
Outpatient cancer chemotherapy increasingly requires patients to manage oral anticancer agents at home, making adherence support and adverse event monitoring critical. Community pharmacists may contribute to treatment continuity through regular telephone follow-up (TFU), but evidence in the community pharmacy setting remains limited.
Objectives
This study aimed to evaluate the relationship between community pharmacy–based TFU and treatment completion among patients receiving postoperative adjuvant chemotherapy for gastric or colorectal cancer.
Methods
We conducted a retrospective observational study of patients who received oral anticancer–containing adjuvant chemotherapy at a community pharmacy in Japan between January 1, 2022, and December 31, 2024. Patients were classified into TFU and non-TFU groups according to whether a community pharmacist-led telephone follow-up was conducted after initial counseling. The primary endpoint was treatment completion based on the planned regimen duration. Patients who completed the planned treatment duration, including those requiring dose reductions or temporary postponements, were considered to have completed treatment. Adverse events were graded using CTCAE v5.0-JCOG.
Results
Sixty-three patients were included (TFU: n = 33; non-TFU: n = 30). The treatment completion was significantly higher in the TFU group than in the non-TFU group (58% vs. 23%, p = 0.006). Grade 1 adverse events were more frequently identified in the TFU group, whereas Grade 2 events were more common in the non-TFU group, suggesting earlier detection and intervention through TFU.
Conclusions
Community pharmacist-led TFU may support treatment continuity and facilitate early detection of adverse events during adjuvant chemotherapy. These results highlight the role of community pharmacies in collaborative cancer care beyond hospital-based settings.
Keywords
Introduction
Outpatient cancer chemotherapy has increased in recent years. With the introduction of molecular targeted agents and immune checkpoint inhibitors, alongside traditional cytotoxic anticancer drugs, the number and complexity of regimens used in personalized cancer chemotherapy have expanded. Consequently, the management of medication adherence and the monitoring and management of adverse events have become increasingly complex in the outpatient setting.
In the 2020 revision of Japan's national medical and dispensing fee schedules, two new systems were introduced to improve the quality of outpatient cancer chemotherapy: Renkei Jujitsu-kasan (the Enhanced Collaborative Care Fee) for hospitals and Tokutei-yakuzai Kanri-shidō Kasan 2 (the Specific Medication Management Guidance Fee 2) for community pharmacies. The Specific Medication Management Guidance Fee 2 reimburses community pharmacies that collaborate with hospitals registered for the Enhanced Collaborative Care Fee, based on their understanding of the patient's treatment plan and provision of a structured follow-up until the next scheduled hospital visit. At Kyowa Pharmacy, part of our organization, this fee has been claimed since May 2020, and pharmacists have provided clinical information to hospitals through tracing reports generated during Telephone Follow-Up (TFU). Tracing reports are structured, pharmacist-generated clinical communication documents used in Japan to convey non-urgent, but clinically important information—such as adverse events, medication adherence, and patient-reported concerns—to prescribing physicians outside the formal prescription framework.
Previous studies reported initiatives involving TFU conducted by community pharmacies for patients receiving outpatient cancer chemotherapy, 1 as well as changes in pharmaceutical interventions resulting from strengthened collaborations and the use of tracing reports between hospitals and community pharmacies.2,3 However, it remains unknown whether regular TFU by community pharmacists contributes to the early detection and management of adverse events or supports treatment continuity among patients receiving oral anticancer therapy—treatment in which medication administration is largely managed at home by patients or their families. Moreover, previous studies have mostly focused on hospital-based pharmacist interventions, and evidence on the impact of community pharmacy–based TFU on treatment completion in postoperative adjuvant chemotherapy remains limited. Therefore, the present study aimed to evaluate the effectiveness of community pharmacist–led TFU in patients with gastric or colorectal cancer receiving postoperative adjuvant chemotherapy.
Methods
Study design
This study was conducted as a retrospective observational study evaluating the treatment completion rate of postoperative adjuvant chemotherapy among patients with cancer, according to whether TFU was provided by community pharmacies.
Study population
The study population consisted of patients who received postoperative adjuvant chemotherapy for gastric or colorectal cancer at Kyowa Pharmacy between January 1, 2022 and December 31, 2024. Patients were identified from the electronic pharmacy record system and were included if they met the following criteria:
received postoperative adjuvant chemotherapy with regimens containing oral anticancer agents (e.g., S-1 or capecitabine) after surgery for gastric or colorectal cancer. received prescription support and follow-up care from community pharmacists at Kyowa Pharmacy; and were followed up until chemotherapy completion or discontinuation.
Patients were excluded if:
chemotherapy initiation occurred outside the study period; or essential data (age, sex, cancer type, cancer stage, date of treatment initiation, or chemotherapy regimen) were missing and not supplemented.
Study methods
This study classified patients into two groups based on whether they received TFU and compared these groups. The study design and timing of TFU implementation are shown in Figure 1.
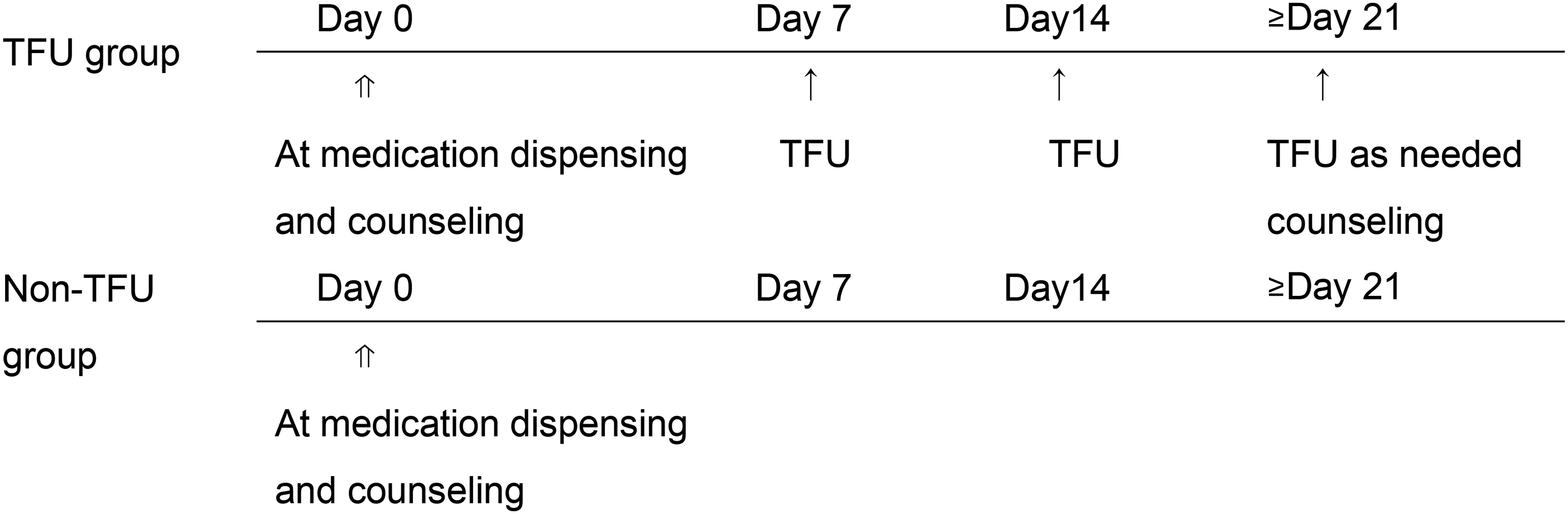
Study design and patient grouping for the telephone follow-up (TFU) analysis.Abbreviations: TFU, telephone follow-up. Day 0: Day of treatment initiation and initial medication counseling. Day 7 and Day 14: Fixed follow-up periods after treatment initiation. ≥Day 21: Additional TFU was conducted as needed based on adverse events, treatment-related concerns, or pharmacist-patient consultation regarding ongoing monitoring. During TFU, pharmacists assessed medication adherence, adverse events, supportive care use, and the need for hospital consultation.
Eligible patients who received initial medication counseling were classified into the following two groups. The decision to conduct TFU was based on routine pharmacy practice, pharmacist availability, and patient agreement, rather than on predefined clinical criteria. The implementation of TFU was not randomized and depended on routine pharmacy workflow and pharmacist judgment in daily clinical practice.
TFU group (intervention group): Patients whose pharmacists confirmed adverse events and medication adherence by telephone after initial medication counseling. Non-TFU group (control group): Patients who did not receive TFU after initial medication counseling and were managed only during in-person visits to the pharmacy. Patients in the non-TFU group received routine in-person medication counseling at prescription dispensing without a scheduled telephone follow-up.
TFU was conducted during the first and second weeks after treatment initiation or a regimen change. Thereafter, TFU was provided as needed based on the occurrence of adverse events or the treatment schedule, following a consultation with the patient. During TFU, pharmacists assessed medication adherence, adverse events, supportive care use, and the need for a hospital consultation. TFU was conducted by community pharmacists involved in routine outpatient cancer care. Additional follow-up calls were performed based on discussions between pharmacists and patients regarding treatment-related concerns or persistent adverse events. Pharmacists referred to relevant clinical guidelines when necessary and communicated recommendations to physicians through tracing reports. Unsolicited telephone consultations initiated by patients to the pharmacy were not included as TFU in this study and were not classified into the TFU group.
The primary endpoint was the treatment completion status of postoperative adjuvant chemotherapy, defined as the number of patients who completed the standard duration of postoperative chemotherapy according to the cancer type. Patients who completed the planned treatment duration were considered to have completed treatment, even if dose reductions or temporary postponements were required during therapy. Patients who permanently discontinued treatment before completion of the planned regimen were classified as treatment non-completion. The secondary endpoint was the incidence of adverse events in relation to TFU. Adverse events were graded according to the Common Terminology Criteria for Adverse Events version 5.0 (CTCAE v5.0-JCOG). 4
Data were collected retrospectively from the electronic pharmacy record system and included patient background characteristics (age, sex, cancer type, treatment regimen, and concomitant medications), records of follow-up implementation, adverse event documentation, and dates of treatment discontinuation. Adverse event assessments were based on pharmacy records and follow-up documentation.
Treatment completion was evaluated using standard postoperative adjuvant chemotherapy regimens as reference criteria. Regarding colorectal cancer, 5 the standard regimen consisted of eight cycles of capecitabine plus oxaliplatin (CapeOX) administered at 21-day intervals, followed by five cycles of UFT plus leucovorin administered at 35-day intervals. Concerning gastric cancer, 6 the standard postoperative regimen was S-1 plus docetaxel (S-1 + DTX) administered for one year, consisting of S-1 monotherapy every 21 days during the first cycle, S-1 plus DTX administered every 21 days from the second to seventh cycles, and S-1 monotherapy every 42 days from the eighth cycle onward.
Additional standard regimens included SOX (S-1 plus oxaliplatin) administered for eight cycles at 21-day intervals and S-1 monotherapy administered for one year at 42-day intervals. The completion of these standard regimens was used as the baseline for the treatment completion assessment.
Statistical analysis
To examine the relationship between the presence or absence of TFU and the treatment completion status, cross-tabulation tables were constructed and either the chi-square test or Fisher's exact test was applied, as appropriate. The same statistical approach was used to analyze the reasons for treatment discontinuation. Differences in age between groups were assessed using Welch's t-test.
Statistical analyses were performed using Microsoft® Excel for Microsoft 365 and EZR (version 1.55). 7 A p-value of < 0.05 was considered to be significant.
Ethical considerations
This study was conducted in accordance with the Ethical Guidelines for Life Science and Medical Research Involving Human Subjects established in Japan and was approved by the Bioethics Committee of the Faculty of Pharmaceutical Sciences, Osaka Ohtani University (Approval No.: BE-0104-25).
Since this was a retrospective observational study, the requirement for individual informed consent was waived. Information regarding the study was publicly disclosed in the pharmacy to provide patients with an opt-out opportunity.
Results
Patient background
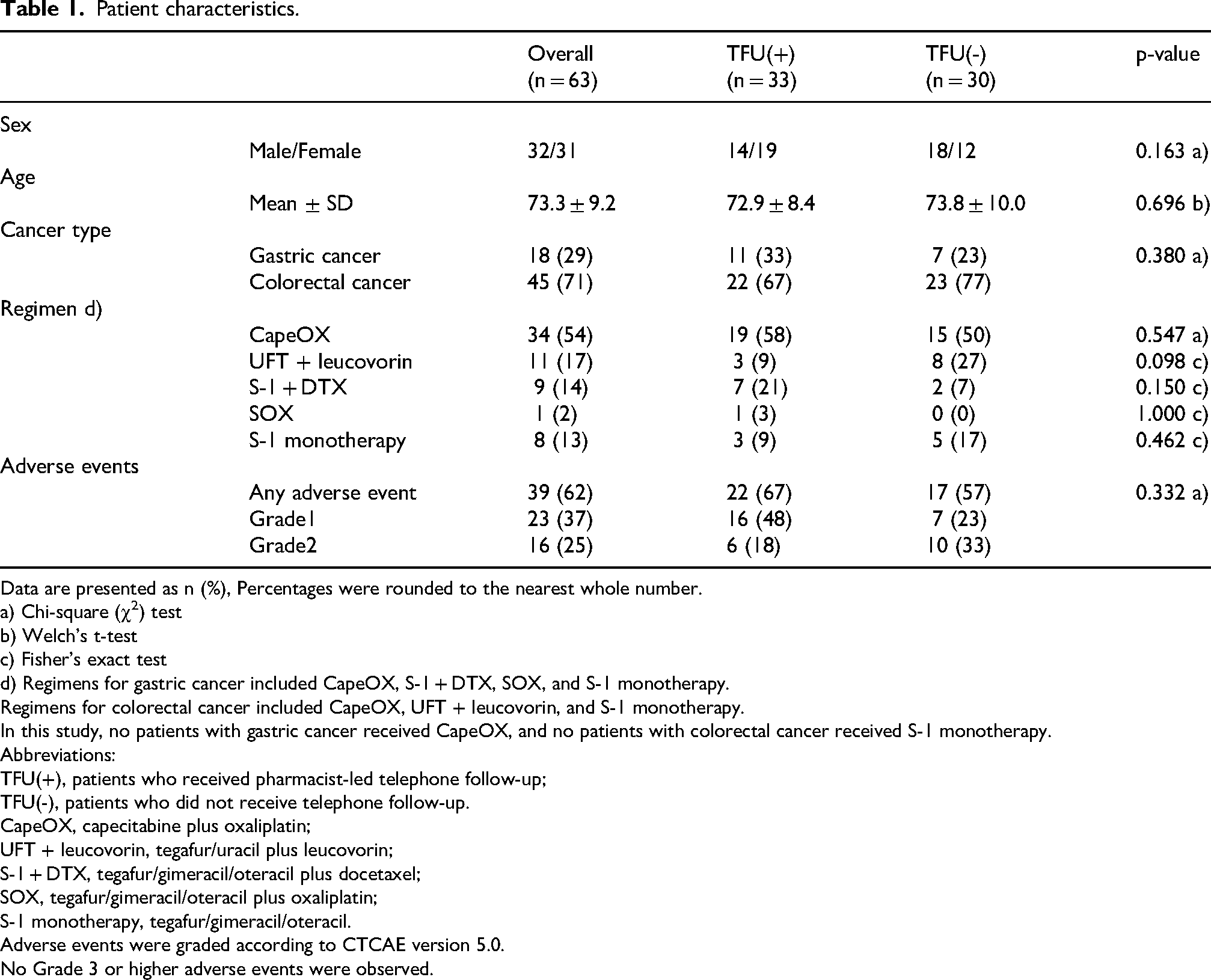
As shown in Table 1, 63 patients were included in the analysis, with 33 in the TFU group and 30 in the non-TFU group. Comparisons of patient background characteristics revealed no significant differences between the two groups in terms of sex, age, cancer type, treatment regimen, or the incidence of adverse events.
Patient characteristics.
Patient characteristics.
Data are presented as n (%), Percentages were rounded to the nearest whole number.
a) Chi-square (χ2) test
b) Welch's t-test
c) Fisher's exact test
d) Regimens for gastric cancer included CapeOX, S-1 + DTX, SOX, and S-1 monotherapy.
Regimens for colorectal cancer included CapeOX, UFT + leucovorin, and S-1 monotherapy.
In this study, no patients with gastric cancer received CapeOX, and no patients with colorectal cancer received S-1 monotherapy.
Abbreviations:
TFU(+), patients who received pharmacist-led telephone follow-up;
TFU(-), patients who did not receive telephone follow-up.
CapeOX, capecitabine plus oxaliplatin;
UFT + leucovorin, tegafur/uracil plus leucovorin;
S-1 + DTX, tegafur/gimeracil/oteracil plus docetaxel;
SOX, tegafur/gimeracil/oteracil plus oxaliplatin;
S-1 monotherapy, tegafur/gimeracil/oteracil.
Adverse events were graded according to CTCAE version 5.0.
No Grade 3 or higher adverse events were observed.
With respect to cancer types, the number of patients with colorectal cancer was approximately 2.5-fold higher than that of patients with gastric cancer. Regarding treatment regimens, CapeOX was used in more than 50% of cases, followed by UFT plus leucovorin. Although no significant differences were observed among regimens, there was a higher percentage of patients receiving UFT plus leucovorin in the non-TFU group, and a higher percentage of patients receiving S-1 + DTX in the TFU group.
Adverse events were observed in 67% of patients in the TFU group (22/33) and 57% of those in the non-TFU group (17/30). When stratified by grade, Grade 1 adverse events occurred in 48% (16/33) and Grade 2 adverse events in 18% (6/33) of patients in the TFU group. In the non-TFU group, Grade 1 adverse events occurred in 23% (7/30) and Grade 2 adverse events in 33% (10/30) of patients, indicating a slightly higher percentage of Grade 2 adverse events in the non-TFU group.
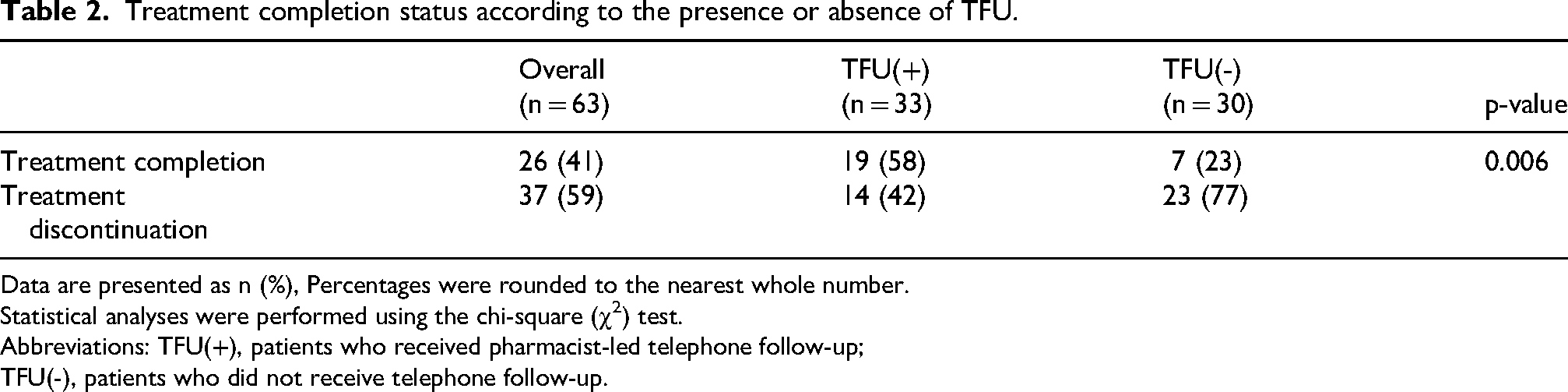
As shown in Table 2, the treatment completion rate was 58% (19/33) in the TFU group and 23% (7/30) in the non-TFU group. The treatment completion rate was significantly higher in the TFU group than in the non-TFU group (p = 0.006).
Treatment completion status according to the presence or absence of TFU.
Treatment completion status according to the presence or absence of TFU.
Data are presented as n (%), Percentages were rounded to the nearest whole number.
Statistical analyses were performed using the chi-square (χ2) test.
Abbreviations: TFU(+), patients who received pharmacist-led telephone follow-up;
TFU(-), patients who did not receive telephone follow-up.
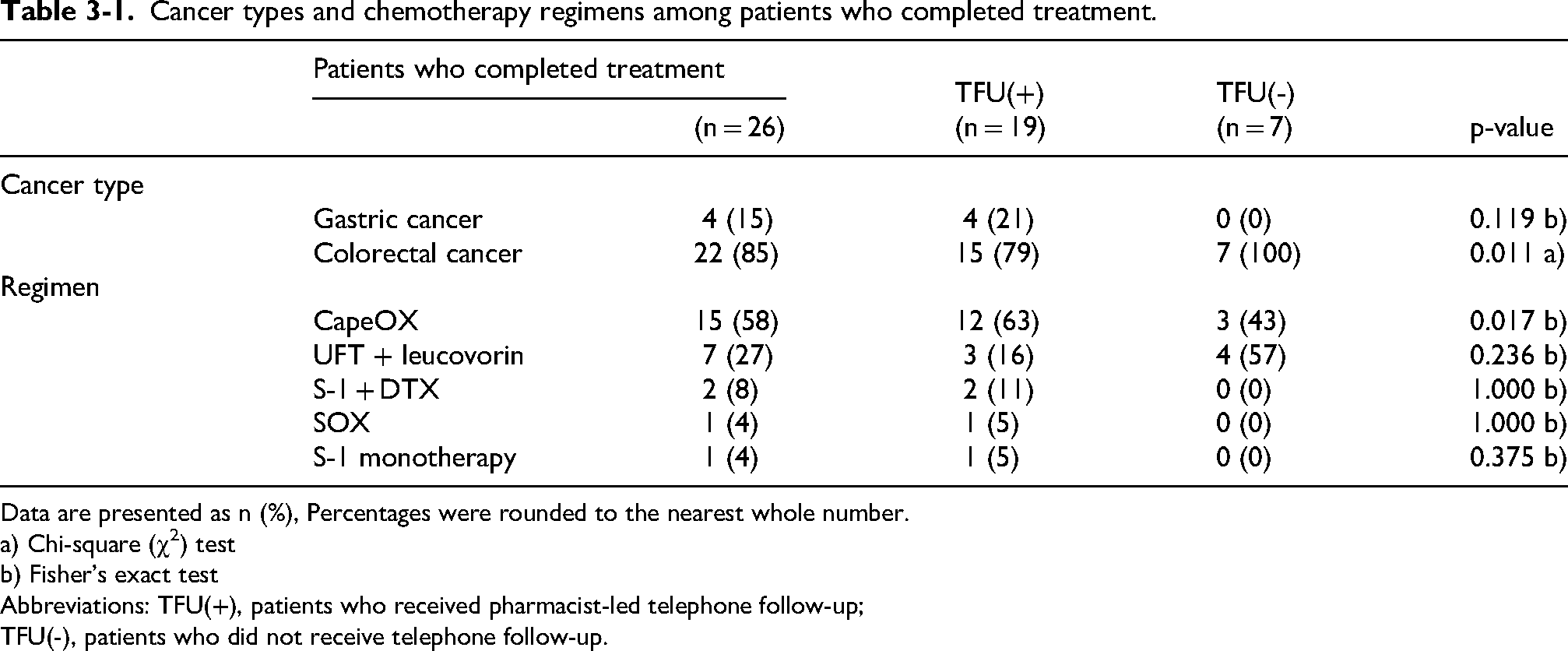
As shown in Table 3-1, among patients with gastric cancer (n = 4), all cases were included in the TFU group and none in the non-TFU group; however, no significant difference was observed (p = 0.119). In contrast, among patients with colorectal cancer (n = 22), treatment completion was observed in 15 patients in the TFU group and 7 in the non-TFU group, with a significantly higher completion rate in the TFU group (p = 0.011).
Cancer types and chemotherapy regimens among patients who completed treatment.
Cancer types and chemotherapy regimens among patients who completed treatment.
Data are presented as n (%), Percentages were rounded to the nearest whole number.
a) Chi-square (χ2) test
b) Fisher's exact test
Abbreviations: TFU(+), patients who received pharmacist-led telephone follow-up;
TFU(-), patients who did not receive telephone follow-up.
With respect to chemotherapy regimens, CapeOX was the most frequently administered regimen (n = 15), with 12 patients in the TFU group and 3 in the non-TFU group, showing a significant difference in treatment completion (p = 0.017). UFT plus leucovorin was administered to 7 patients, including 3 in the TFU group and 4 in the non-TFU group, with no significant difference (p = 0.236). Other regimens, including S-1 + DTX, SOX, and S-1 monotherapy, were administered to a limited number of patients, and no significant differences were observed according to the TFU status.
As shown in Table 3-2, among patients who experienced adverse events, 14 completed treatment. Eleven patients in the TFU group and 3 in the non-TFU group completed treatment, with a significantly higher completion rate in the TFU group (p = 0.049). When stratified by adverse event grades, treatment completion was achieved by 10 patients (26%) with Grade 1 adverse events, including 8 (36%) in the TFU group and 2 (12%) in the non-TFU group. Among patients with Grade 2 adverse events, treatment was completed by 4 patients (10%), including 3 (14%) in the TFU group and 1 (6%) in the non-TFU group. Although these differences were not significant, treatment completion rates were generally higher in the TFU group.
Treatment completion among patients who experienced adverse events.
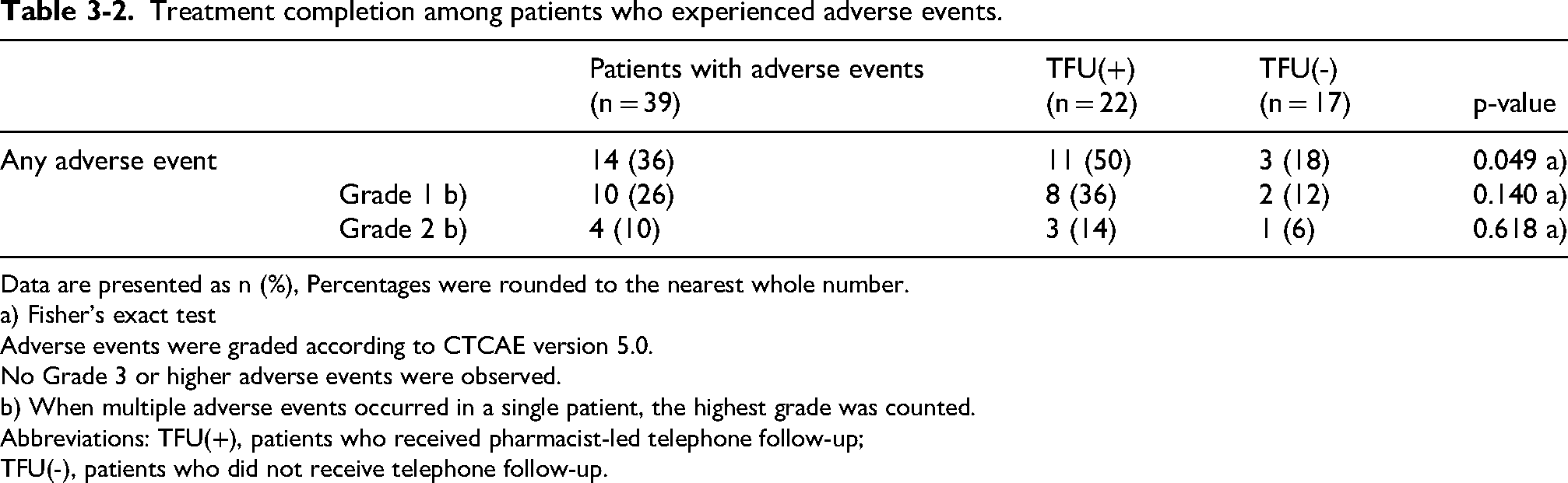
Data are presented as n (%), Percentages were rounded to the nearest whole number.
a) Fisher's exact test
Adverse events were graded according to CTCAE version 5.0.
No Grade 3 or higher adverse events were observed.
b) When multiple adverse events occurred in a single patient, the highest grade was counted.
Abbreviations: TFU(+), patients who received pharmacist-led telephone follow-up;
TFU(-), patients who did not receive telephone follow-up.
As shown in Table 4, the most common reason for treatment discontinuation was adverse events, accounting for 19 cases. Of these, 6 cases occurred in the TFU group and 13 in the non-TFU group, with a slightly higher number being observed in the non-TFU group (p = 0.420).
Reasons for treatment discontinuation by the TFU status.
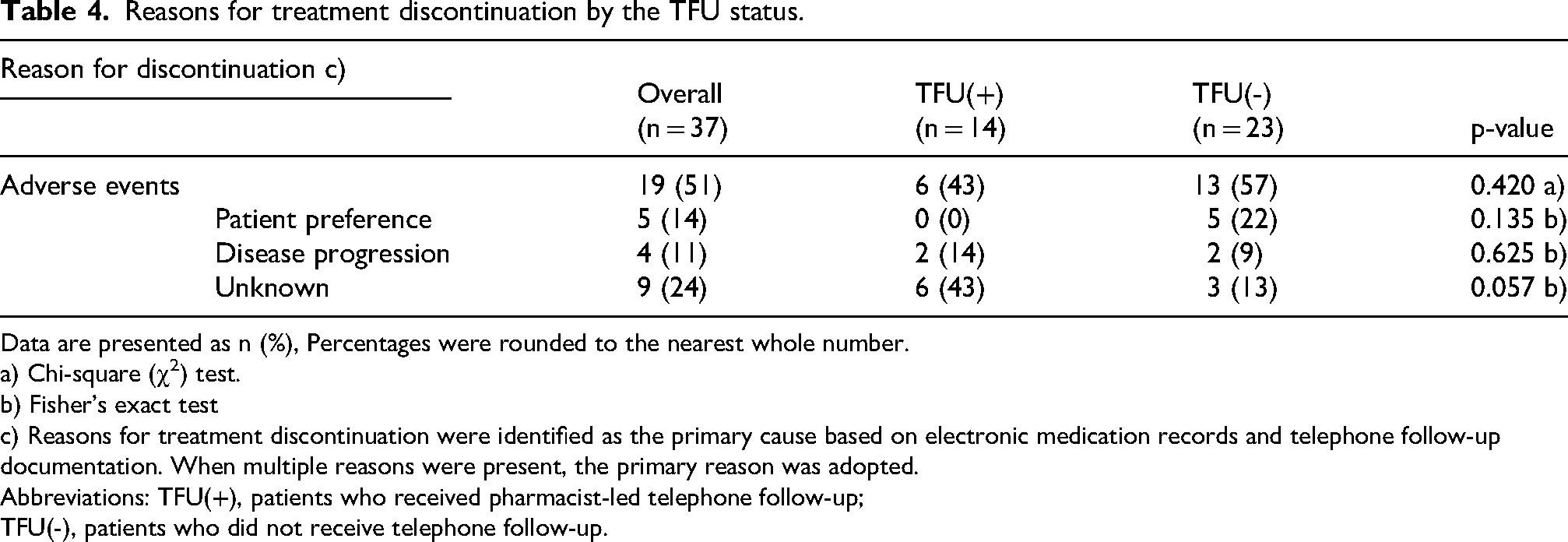
Reasons for treatment discontinuation by the TFU status.
Data are presented as n (%), Percentages were rounded to the nearest whole number.
a) Chi-square (χ2) test.
b) Fisher's exact test
c) Reasons for treatment discontinuation were identified as the primary cause based on electronic medication records and telephone follow-up documentation. When multiple reasons were present, the primary reason was adopted.
Abbreviations: TFU(+), patients who received pharmacist-led telephone follow-up;
TFU(-), patients who did not receive telephone follow-up.
Discontinuation due to patient preference was observed in 5 cases, all of which occurred in the non-TFU group. Discontinuation due to disease progression occurred in 4 cases, accounting for 11% of all discontinuations. In addition, 9 cases were classified as having an unknown reason because a clear cause was not identified, representing the second most common reason after adverse events.
Adverse events accounted for approximately half of all treatment discontinuations and were observed in both groups.
As shown in Table 5, nausea was the most common adverse event, occurring in 36% (8/22) of patients in the TFU group and 35% (6/17) in the non-TFU group. No marked differences were observed between the groups, including in the grade distribution.
Incidence of adverse events by symptom.
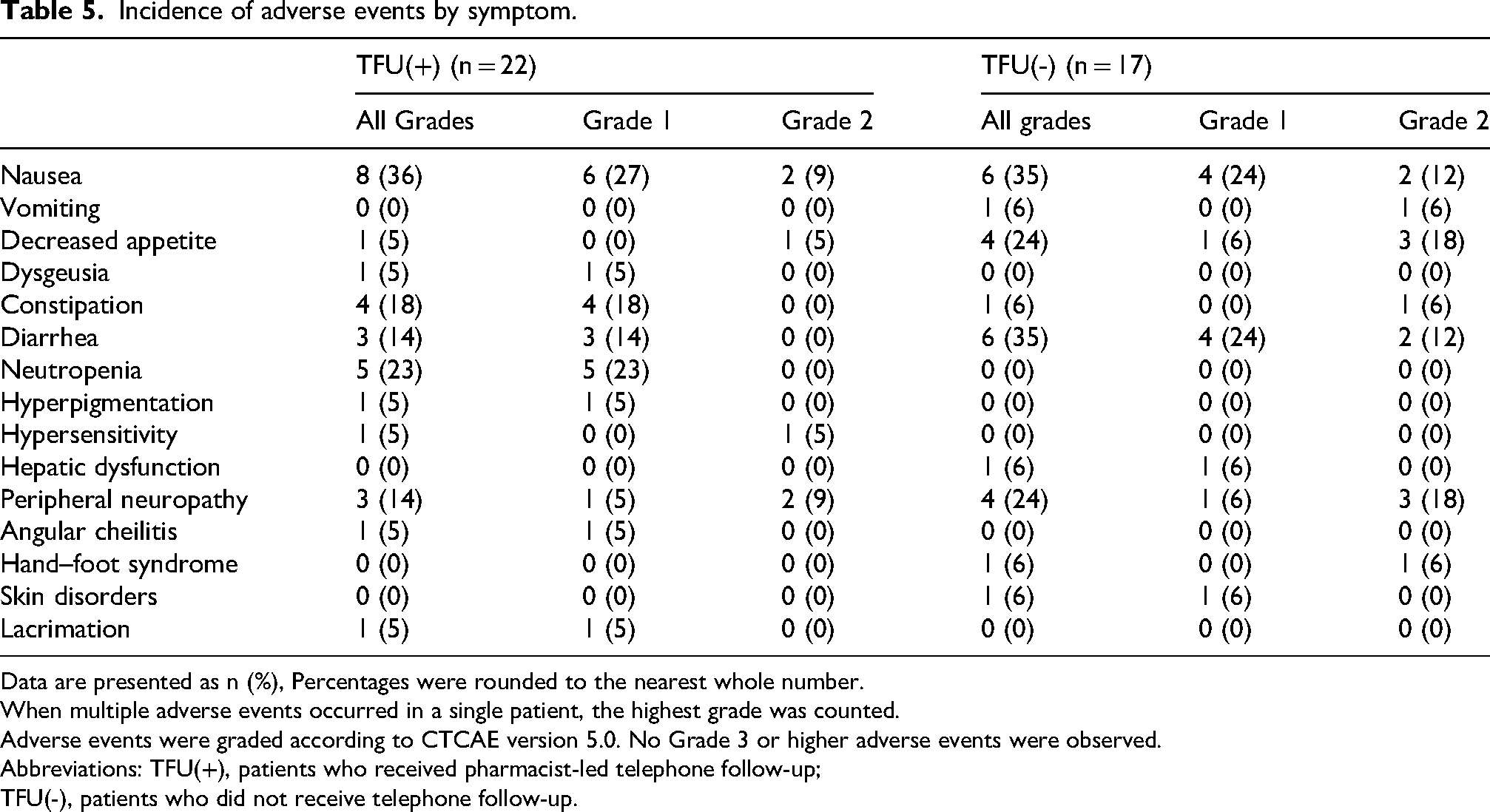
Data are presented as n (%), Percentages were rounded to the nearest whole number.
When multiple adverse events occurred in a single patient, the highest grade was counted.
Adverse events were graded according to CTCAE version 5.0. No Grade 3 or higher adverse events were observed.
Abbreviations: TFU(+), patients who received pharmacist-led telephone follow-up;
TFU(-), patients who did not receive telephone follow-up.
Constipation developed in 18% (4/22) of patients in the TFU group and 6% (1/17) in the non-TFU group. Diarrhea was noted in 14% (3/22) of patients in the TFU group and 35% (6/17) in the non-TFU group, with a higher percentage in the latter. Neutropenia occurred in 23% (5/22) of patients in the TFU group.
The incidence of other adverse events, including dysgeusia, hyperpigmentation, hypersensitivity, hepatic dysfunction, angular cheilitis, hand–foot syndrome, skin disorders, and lacrimation, was low.
Discussion
The present study suggests that TFU conducted by community pharmacists may be associated with higher treatment completion rates among patients with gastric and colorectal cancers receiving postoperative adjuvant chemotherapy. The significantly higher treatment completion rate observed in the TFU group highlights the potential role of regular medication support, including community pharmacist-led TFU, in supporting treatment continuation during outpatient cancer chemotherapy. Real-world studies previously demonstrated that pharmacist-led follow-up interventions for patients receiving outpatient oral anticancer therapy improved medication adherence, symptom management, and patient reassurance during treatment. 8
A community pharmacist-led telephone follow-up has also been reported to facilitate the early detection of adverse events and support continuous outpatient cancer care. 1
In addition, studies conducted in hospital settings demonstrated that pharmacist follow-ups improved patients’ quality of life during outpatient cancer chemotherapy. 8
However, to the best of our knowledge, the effects of telephone-based medication support provided by community pharmacists have yet to be investigated. The results of the present study extend this existing evidence by demonstrating the potential impact of TFU conducted in community pharmacies. The relationship observed between TFU and higher treatment completion rates suggests that community pharmacist-led TFU helps identify adverse events at an early stage, provides timely guidance on medication management, and supports patients in continuing treatment as planned. Collectively, these results indicate that TFU by community pharmacists play an important supportive role in outpatient cancer chemotherapy by promoting treatment completion and the continuity of care beyond hospital-based settings.
In recent years, outpatient cancer chemotherapy has become increasingly common, requiring patients and their families to manage medication administration in the home setting. 9 Consequently, maintaining medication adherence and appropriately managing adverse events have emerged as critical challenges in cancer care. In addition, according to reports from the Ministry of Health, Labour and Welfare of Japan, 10 the incidence of cancer among individuals aged 85 years and older is projected to increase by 2040 as the baby boomer generation continues to age. Although the total number of cancer patients is expected to remain stable or slightly increase, healthcare systems must respond to an increasingly older cancer patient population.
In the context of oral anticancer therapy, treatment decisions based on patients’ subjective judgment or difficulties in managing adverse events may lead to premature treatment discontinuation. Previous studies identified several factors affecting medication adherence, including the level of trust between patients and healthcare providers, patients’ attitudes toward treatment, and their understanding of therapeutic goals and adverse event management. 11 Since patients receiving outpatient cancer chemotherapy spend most of their time at home, the administration of oral anticancer agents primarily occurs in the home environment, effectively making the patient's residence the site of treatment. Under these conditions, the importance of collaborations between community pharmacists and medical institutions to obtain appropriate patient information and provide timely interventions for patients and their families has increased. 12
In the present study, which focused on patients receiving postoperative adjuvant chemotherapy for gastric or colorectal cancer at Kyowa Pharmacy, a specialized medical institution–affiliated community pharmacy for cancer care, within our organization, the results obtained suggest that community pharmacist-led TFU contribute to treatment continuation. Previous studies demonstrated that regular pharmacist follow-ups supported medication adherence, facilitated the early detection of adverse events, and provided reassurance to patients undergoing outpatient cancer chemotherapy. 13 Moreover, the effectiveness of TFU was shown to be enhanced not only through single-session information sharing, but also through a team-based medical care approach involving collaborations among pharmacists, physicians, and nurses. 8
The higher treatment completion rate observed in the TFU group than in the non-TFU group may be explained by the proactive involvement of community pharmacists beyond in-person medication counseling at the pharmacy counter. Through TFU, community pharmacists were able to confirm medication adherence and identify early signs of adverse events or changes in physical condition by communicating directly with patients or their family members. This allowed community pharmacists to provide timely feedback to healthcare institutions, including proposals for supportive therapy initiation or dosage adjustments via tracing reports or telephone consultations, before adverse events progressed. These early interventions may have contributed to preventing treatment interruption and supporting the continuation of postoperative adjuvant chemotherapy.
Although the treatment completion rate in the non-TFU group appeared to be low, real-world studies previously demonstrated that treatment continuation during outpatient oral anticancer therapy was often affected by adverse events, treatment burden, and challenges in self-management at home. These factors may contribute to lower completion rates in routine clinical practice than in controlled clinical trial settings. 8
Notably, treatment completion rates were higher among patients who developed adverse events in the TFU group than in the non-TFU group. One possible explanation is that regular TFU facilitated the early recognition of adverse events, enabling timely supportive care and communication with healthcare providers before symptoms became severe enough to require treatment discontinuation.
However, since this was a retrospective observational study, the possibility of confounding factors cannot be excluded. Patients who received TFU may have differed from those in the non-TFU group in terms of treatment motivation, communication with pharmacists, social support, or clinical characteristics not captured in this study. Therefore, the observed relationship between TFU and treatment completion needs to be interpreted with caution.
When stratified by cancer type, the significantly higher treatment completion rate in the TFU group among patients with colorectal cancer suggests that regular TFU by community pharmacists was particularly effective in this population. In postoperative adjuvant chemotherapy for colorectal cancer, the CapeOX regimen is frequently used and is associated with adverse events, such as hand–foot syndrome and peripheral neuropathy, which are risk factors for treatment discontinuation. 14 Through TFU, community pharmacists may have facilitated the early recognition of these adverse events, reinforced patient education regarding preventive measures, and shared clinically relevant information with healthcare providers, thereby contributing to a higher treatment completion rate. In contrast, no significant difference was observed among patients with gastric cancer, which may be attributable to the small sample size.
An analysis by chemotherapy regimen revealed significantly higher treatment completion rates in the TFU group for the CapeOX regimen, whereas no significant differences were observed for other regimens. This result likely reflects the predominance of colorectal cancer cases in the present study and the frequent selection of the CapeOX regimen in this setting. The CapeOX regimen, which combines capecitabine and oxaliplatin, is associated with adverse events that have a negative impact on patients’ quality of life and medication adherence if early management is delayed. 15 These characteristics underscore the importance of early interventions, suggesting that TFU is particularly beneficial for regimens requiring careful adverse event monitoring.
Among patients who experienced adverse events, treatment completion rates were significantly higher in the TFU group. This result suggests that TFU contributes not only to adverse event management, but also to psychological support, including reassurance and encouragement to continue treatment. The adverse events observed in this study were limited to Grades 1 and 2, with no Grade 3 or higher events being reported. This indicates that early advice, supportive therapy proposals, and recommendations for a medical consultation provided through TFU helped prevent the progression of adverse events to more severe levels. Although the lack of a significant difference in some analyses may be attributed to the small sample size and limited statistical power, these results are consistent with previous findings indicating that pharmacist-led follow-ups facilitate the early detection of adverse events and support treatment continuation. 16
Regarding reasons for treatment discontinuation, adverse events were the most common cause, followed by patient preferences and disease progression, which is consistent with previous findings. 17 In the TFU group, discontinuation due to adverse events was less frequent than in the non-TFU group; however, a higher percentage of cases were classified as having unknown reasons. This may reflect challenges in information acquisition when patients discontinue visits to the pharmacy or transfer to other medical institutions. In contrast, the higher incidence of discontinuation due to patient-related factors in the non-TFU group suggests that regular communication and psychological support from community pharmacists may be important for maintaining patients’ motivation to continue treatment.
The symptom-based analysis revealed the higher detection of adverse events in the TFU group, likely due to increased opportunities for patients to report symptoms during regular follow-ups. In particular, Grade 1 adverse events were more frequently identified in the TFU group, whereas Grade 2 adverse events were more common in the non-TFU group. These results suggest that TFU facilitates the early detection of symptoms and the timely initiation of an intervention at a mild stage before they progress to more severe toxicity. The higher detection of hematological toxicity in the TFU group may be attributed to the timing of TFU implementation, which coincided with the expected nadir period following chemotherapy administration.
Through TFU, community pharmacists were also able to provide guidance on infection prevention and self-care measures, such as fever management and oral care, which may have contributed to suppressing the development of severe hematologic toxicity.
Patients in the non-TFU group had fewer opportunities for an early assessment between hospital visits, which may have delayed the recognition of mild symptoms until they progressed to Grade 2 adverse events. These results suggest that TFU does not necessarily reduce the overall incidence of adverse events, but may facilitate early detection and timely intervention at a mild stage.
Finally, medication support provided by community pharmacists through TFU may offer not only clinical benefits, but also psychological reassurance for patients receiving oral anticancer therapy at home. As the number of elderly patients undergoing outpatient cancer chemotherapy continues to increase, the involvement of community pharmacists is likely to become increasingly important for ensuring the safety, continuity, and quality of cancer care.
This study has several limitations. It focused exclusively on postoperative adjuvant chemotherapy for gastric and colorectal cancers, limiting the generalizability of the findings to other cancer types. Furthermore, the study was conducted at a single center using a retrospective observational design. Since the TFU allocation was not randomized and depended on routine clinical practice, a selection bias may have been present, and patients who received TFU may have differed from those in the non-TFU group in ways that were not captured in this study. In addition, the content and timing of TFU varied among pharmacists, and an adverse event assessment relied on pharmacy records. Future studies need to include prospective, multicenter designs, the standardization of TFU interventions, and evaluations across a broader range of cancer types. Moreover, alternative follow-up modalities, such as video-based consultations or digital communication tools, need to be examined to complement TFU and enhance patient care.
Conclusion
The present results suggest that TFU conducted by community pharmacists may play an important role in supporting treatment continuity among outpatients receiving cancer chemotherapy. In this context, TFU may contribute to the early detection of adverse events, timely interventions, and sustained adherence to treatment in the outpatient setting.
In the future, specialized medical institution–affiliated community pharmacies for cancer care are expected to function as regional hubs for cancer treatment support in outpatient chemotherapy. The establishment of a multidisciplinary collaboration model that integrates hospital-based care with community pharmacy support may further enhance the quality, safety, and continuity of cancer care in an aging society.
Footnotes
Acknowledgements
The authors thank the pharmacists involved in patient care and data collection for their support.
Author contributions
NW conceived and designed the study. NW collected the data. NW performed the statistical analysis and drafted the manuscript. TI, MN, SO, and MM contributed to interpretation of the results and critical revision of the manuscript. All authors approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
The datasets generated and analyzed during the current study are not publicly available due to privacy restrictions but are available from the corresponding author on reasonable request.