
Abstract
Introduction
Taxane-induced peripheral neuropathy (TIPN) is a debilitating side effect of taxane chemotherapy. However, real-world studies on TIPN requiring treatment are limited. This study evaluated the incidence, characteristics, and outcomes of TIPN requiring treatment in patients with breast cancer.
Methods
A retrospective study was conducted at King Hussein Cancer Center and included adult patients with breast cancer treated with taxane-based chemotherapy regimens from January 2023 to August 2025. Patients who developed TIPN requiring pain medications were identified. Baseline characteristics, taxane related data, onset of TIPN requiring treatment, clinical outcomes, and pain management strategies were assessed using descriptive analysis.
Results
Among 1353 patients, 201 (15.0%) developed TIPN requiring treatment. The mean age was 54 years (SD ± 10.5). Among these patients, 135 (67.2%) received docetaxel and 66 (32.8%) received paclitaxel. Early-stage breast cancer was reported in 133 (66.0%) patients, while 68 (34.0%) had metastatic disease. TIPN requiring treatment occurred most frequently after the third cycle with docetaxel (n = 104, 77.0%), and after the fifth cycle with paclitaxel (n = 30, 45.5%). TIPN requiring treatment resulted in emergency department visits in 16 (8.0%) patients, chemotherapy dose reductions in 63 (31.3%), treatment discontinuation in 23 (11.4%), and cycle delays in 3 (1.5%) patients. Initial pharmacologic management consisted of gabapentin monotherapy (80.0%), duloxetine monotherapy (10.5%), and combination of gabapentin and duloxetine (7.0%).
Conclusions
During the study period, TIPN requiring treatment affected one- in- seven patients with breast cancer and resulted in significant treatment modifications, highlighting opportunities for proactive management strategies to improve patient care and safety.
Introduction
Taxanes, including paclitaxel and docetaxel, are cornerstone chemotherapeutic agents in the management of both early-stage and metastatic breast cancer. 1 Despite their proven clinical benefits, their use is associated with several adverse events, such as myelosuppression, hypersensitivity reactions, and peripheral neuropathy. 1 Taxane-induced peripheral neuropathy (TIPN) is a common and often dose-limiting adverse effect of taxanes.2–4 Reported incidence rates are substantial, affecting 43.0% to 80.0% of patients receiving taxane-based therapy, reaching as high as 97.0% among patients treated with paclitaxel.5,6 Some studies have demonstrated that paclitaxel is associated with a higher incidence of neurotoxicity compared to docetaxel.7,8
Risk factors for TIPN extend beyond age, body surface area, obesity, diabetes, and cumulative dose. Recent studies have highlighted the significant contribution of racial and genetic factors to the risk of TIPN.9,10 For instance, African American patients have been reported to experience a 73.0% higher risk of TIPN compared with White patients, even after adjustments for taxane type. 10
Although TIPN has been widely reported in the literature, evidence from the Middle East, particularly regarding patients requiring pain management, remains limited. Considering differences in the incidence of TIPN across racial and ethnic groups, this gap is clinically significant and needs further assessment. Therefore, this study aims to evaluate the real-world incidence, clinical characteristics, outcomes, and management strategies of TIPN requiring pain treatment among patients with breast cancer treated with taxanes at a comprehensive cancer center in Jordan.
Methods
This was a single-center, retrospective observational study conducted at King Hussein Cancer Center (KHCC), a comprehensive cancer center located in Amman, Jordan. The study included adult patients with breast cancer treated with taxane-based chemotherapy regimens and developed TIPN that necessitated pharmacologic pain management between January 2023 and August 2025. The study was approved by KHCC Institutional Review Board (approval number 25 KHCC 118), with a waiver of consent because of the retrospective nature of the study that carries no more than minimal risk to patients.
Patients who received taxane-based chemotherapy regimens including docetaxel or paclitaxel, were identified through electronic medical records. Patients with early-stage and metastatic breast cancer who developed TIPN that necessitated pharmacologic pain management were identified through the pharmacy billing system, which was used to extract patients list who dispensed pain medications during the study period. Afterward, we reviewed their electronic medical records, particularly physician progress notes, to identify evidence of TIPN requiring treatment, where we looked for keyword including the presence of numbness, weakness, neuropathy, and/or neuropathic pain. When physician documentation was unavailable, clinical nurse coordinator (CNC) notes were reviewed to confirm the development of TIPN requiring pharmacologic interventions. Patients’ characteristics and treatment-related data were collected, including demographics, disease stage, comorbidities, type of taxane administered, number of chemotherapy cycle associated with TIPN requiring treatment, pain management strategies, and clinical outcomes.
TIPN treatment strategy was evaluated by assessing the initiation of analgesic medication for neuropathic pain, including the dose and type of medications (e.g., gabapentin, duloxetine, or combination therapy). Dose escalation was defined as any documented increase in medication dose after treatment initiation and was confirmed through reviewing physician notes and the pharmacy billing system. Clinical outcomes were assessed after the development of TIPN requiring pharmacologic treatment including Emergency Department (ED) visits, chemotherapy dose reductions, treatment delay, or permanent discontinuation of chemotherapy.
Statistical analysis
Descriptive statistics were used to summarize patient and treatment characteristics. Continuous data were reported as mean ± standard deviation (SD), median, and range, while categorical data were presented as frequencies and percentages. All statistical analyses were performed using Microsoft Excel 2018 (Microsoft Corp., Redmond, WA, USA).
Results
During the study period, a total of 1353 patients with breast cancer received taxane-based chemotherapy regimens at KHCC. Of these, 852 (63.0%) received docetaxel and 501 (37.0%) received paclitaxel. Overall, 201 (15.0%) patients developed TIPN requiring pharmacologic management and were included in the final analysis. Among these 201 patients, 135 (67.2%) had received docetaxel, whereas 66 (32.8%) had received paclitaxel. The mean age was 54 years (SD ± 10.5), with 99.0% being females, and 1.0% were males. Comorbidities were reported in 101 (50.2%) patients, while 100 (49.8%) patients were medically free. Hypertension was the most common comorbidity, accounting for 60 (29.8%) patients. Among the included patients, 133 (66.0%) had early-stage breast cancer, while 68 (34.0%) patients had metastatic disease. Table 1 summarizes the baseline characteristics of patients who developed TIPN requiring treatment.
Baseline characteristics of patients who developed TIPN requiring treatment (n = 201).
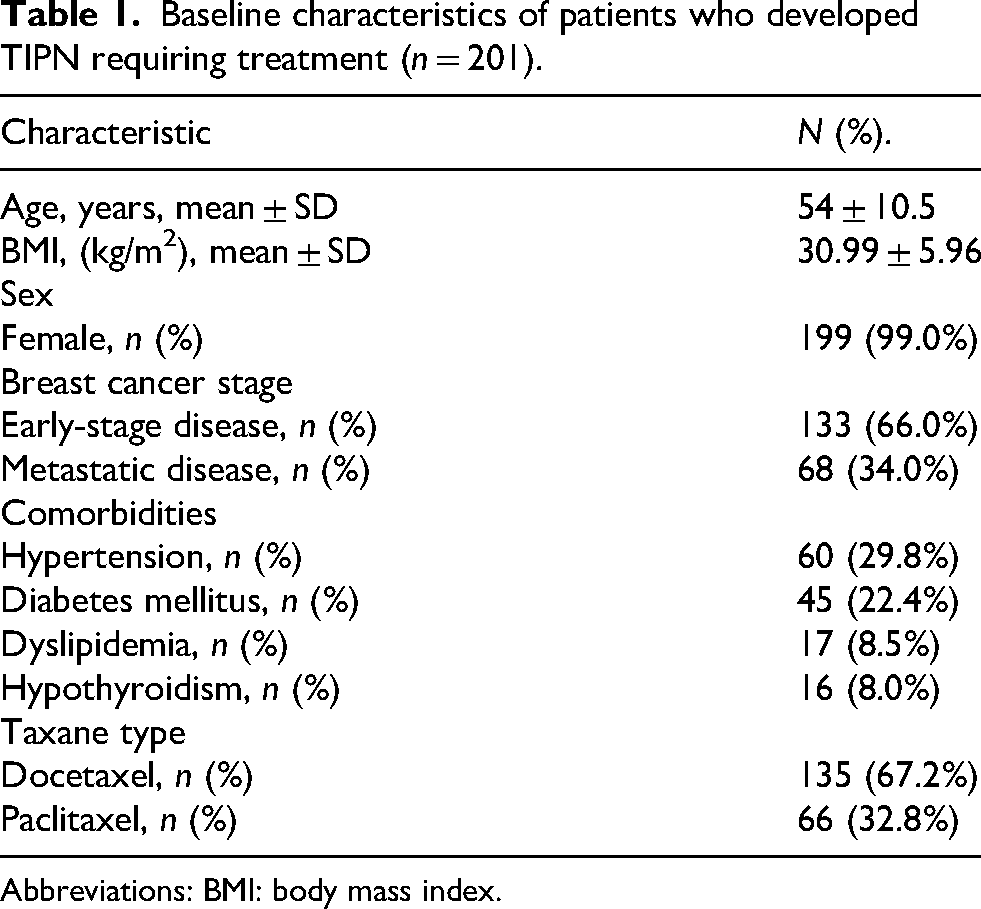
Abbreviations: BMI: body mass index.
Among patients treated with docetaxel, TIPN requiring treatment most commonly occurred after the third cycle (104 patients, 77.0%), followed by the fourth (25 patients, 18.0%), second (4 patients, 3.0%) and fifth cycles (3 patients, 2.0%). In paclitaxel-treated patients, TIPN requiring treatment was most commonly observed after the fifth cycle (30 patients, 45.5%), followed by the fourth (28 patients, 42.4%), and third cycles (8 patients, 12.1%).
The clinical outcomes related to TIPN requiring pain medications included emergency department visits that were required for 16 (8.0%) patients, chemotherapy dose reductions for 63 (31.3%) patients, treatment discontinuations for 23 (11.4%) patients, and chemotherapy cycle delays for 3 (1.5%) patients. Subgroup analyses were conducted to evaluate the clinical outcomes of TIPN requiring pain medications according to disease stage. For patients with early-stage breast cancer, 34 (25.6%) required dose reductions, and 14 (10.5%) required treatment discontinuations; however, no delays in subsequent chemotherapy cycles were reported. Among patients with metastatic breast cancer disease, 29 (42.0%) required dose reductions, 9 (13.2%) required treatment discontinuations, and 3 (4.4%) required treatment delays in subsequent chemotherapy cycles.
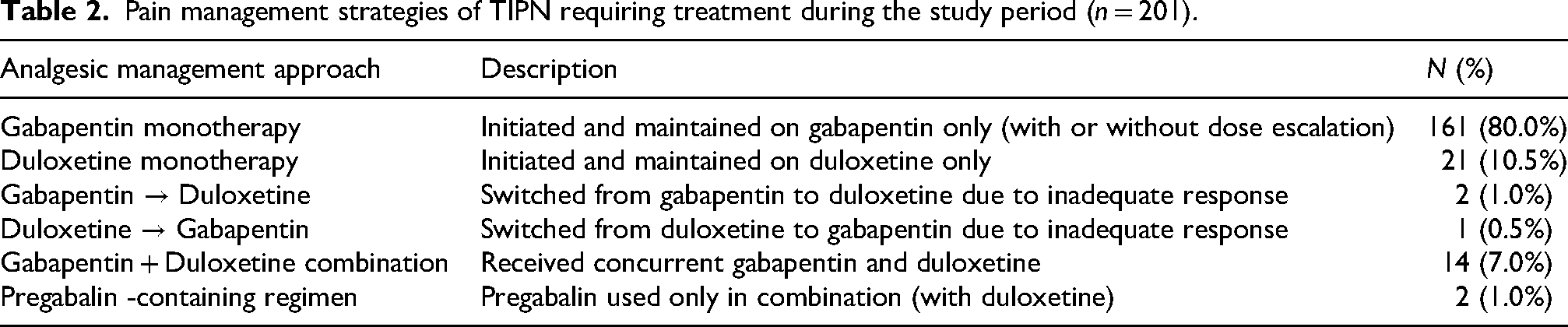
Gabapentin monotherapy was the most frequently prescribed treatment for TIPN, accounting for 161 (80.0%) patients. Among patients receiving gabapentin monotherapy group (n = 161), the most commonly prescribed starting regimen was 300 mg once daily (36.0%), followed by 300 mg twice daily (28.5%), 300 mg three times daily (21.0%), and 400 mg once daily (7.5%). Higher starting doses (400 mg twice or three times daily) were less frequent, accounting for 7.0% of patients. Among patients who initiated higher starting doses, gradual dose escalation every three days was implemented.
Dose escalation of gabapentin was observed in 39 (19.5%) patients, typically involving stepwise increases in dosing frequency from 300 mg once daily to twice or three times daily or changing the dose from 300 mg to 400 mg. Escalation to doses of 600–800 mg three times daily was required in 1.5% of patients. Duloxetine monotherapy was prescribed for 21 (10.5%) patients, and was initiated at 30 mg once daily, with escalation to 60 mg once daily when needed. Pregabalin use was minimal in our cohort (1.0%) and was primarily observed as part of combination therapy; however, one patient received pregabalin monotherapy with dose escalation. No switching to or from pregabalin was observed. Pain management strategies of TIPN requiring treatment during the study period are summarized in Table 2.
Pain management strategies of TIPN requiring treatment during the study period (n = 201).
Discussion
This study evaluated real-world incidence, clinical characteristics, outcomes, and management of TIPN requiring pharmacologic treatment among patients with breast cancer. The observed incidence of 15.0% reflects a clinically significant neuropathic pain necessitating pharmacologic interventions, rather than the overall incidence of TIPN of any grade. As such, our findings represent a treatment-oriented endpoint including subset of patients requiring active clinical management because of common adverse events of taxanes.
Unlike studies reporting the overall incidence of TIPN, which include all grades of neuropathy across a broad clinical spectrum, our results specifically included moderate-to-severe cases that required treatment decisions in routine practice. This distinction is essential when interpreting and comparing incidence rates across studies, as variability in outcome, patients’ characteristics, and sample size may influence the reported incidence rates. Our findings provide real-world evidence on clinically relevant burden of TIPN in Jordanian population and address an important gap in region-specific data of oncology supportive care.
The incidence of TIPN requiring pharmacologic interventions in our cohort was lower than the reported rate by Seretny et al. 5 However, direct comparison is limited by substantial differences in the outcomes. The meta-analysis by Seretny et al. incorporated heterogeneous study definitions and captured all-grade TIPN using clinical grading systems, including mild (grade I) symptoms that did not require treatment. In contrast, our study specifically evaluated TIPN requiring treatment, thereby reflecting a more clinically meaningful endpoint indicating at least moderate neuropathy.
A study by Kim et al. 11 reported a 21.9% incidence of TIPN requiring pharmacologic treatment in a real-world cohort, which is broadly comparable to our observed incidence of 15.0%. This reflects the use of similar definitions centered on clinically significant cases requiring interventions. However, differences in patient characteristics, treatment protocols, and supportive care practices may account for the observed variation in incidence. Compared with the incidence rate of grade 2–3 TIPN reported by Park et al., 12 which ranged from 11.0% to 30.0%, our findings fall within this range and are consistent with those reported internationally.
Although both taxanes are associated with peripheral neuropathy, our findings suggest a difference in the onset of TIPN requiring treatment, with docetaxel-associated peripheral neuropathy appearing earlier compared to paclitaxel. However, comparisons based solely on cycle number should be interpreted cautiously, as treatment schedules differ between paclitaxel and docetaxel. Karafiath et al., 13 reported a more acute onset of neuropathy with docetaxel in patients with breast cancer. The underlying mechanism has been proposed by Scripture et al. 14 and Velasco and Bruna, 15 who suggested that paclitaxel toxicity is primarily dose-dependent and cumulative, whereas docetaxel may involve additional immune-mediated or metabolic pathways that could contribute to an earlier onset of symptoms. Based on our study, cycle-based onset may not reflect equivalent cumulative drug exposure or elapsed time from treatment initiation.
In our cohort, a high mean body mass index (BMI) was observed among patients requiring pharmacologic management for TIPN. Prior literature, including Bao et al., 16 has suggested obesity as a potential risk factor for TIPN. This has been hypothesized to relate to altered pharmacokinetics of lipophilic agents such as taxanes, potentially leading to prolonged exposure in patients with higher body fat composition, as also discussed by Scripture et al. 14 Because our study included only patients who developed TIPN requiring treatment and did not include a comparison group, our findings should be interpreted as descriptive characteristics of the affected patients rather than evidence of an association or risk factor. Further studies with appropriate comparator groups are needed to evaluate the relationship between BMI and TIPN requiring treatment.
Approximately one third of patients who developed TIPN requiring treatment had hypertension. Because our study was descriptive in nature with no comparison, no conclusion regarding the impact of comorbidities as risk factors for TIPN can be drawn. Previous studies, such as Bao et al., 16 have proposed that underlying metabolic and vascular conditions may contribute to an increased vulnerability to neuropathic toxicity of chemotherapy. In this context, no formal association analysis was performed in our study to make a final conclusion regarding this issue.
Clinically, TIPN had a notable impact on antineoplastic treatment delivery, with a significant proportion of patients experiencing chemotherapy modification or interruption. This finding is consistent with prior reports by Park SB et al. 12 and Gauthier et al., 17 who identified peripheral neuropathy as a major dose-limiting toxicity in breast cancer treatment. In our study, descriptive analysis according to breast cancer stage demonstrated that chemotherapy dose reductions, treatment discontinuations, and treatment delays were more common among patients with metastatic disease compared to early-stage breast cancer. These differences may reflect variations in treatment intention, cumulative taxane exposure, and clinical decision regarding the treatment of TIPN between palliative and curative treatment settings. We also observed that 8.0% of patients required an emergency department visit, which highlights the acute clinical burden of TIPN. While peripheral neuropathy is often characterized as chronic toxicity, our findings suggest that symptoms may escalate to acute presentations requiring urgent care, consistent with the concerns raised by Hertz et al. 18 regarding the significant physical distress associated with TIPN.
Regarding the pharmacologic management of TIPN, our study revealed a predominant use of gabapentin monotherapy. This represents a notable discrepancy from the recommendations of the American Society of Clinical Oncology (ASCO) 19 for the management of TIPN that recommends the use of duloxetine as the only agent with established phase III evidence for the treatment of TIPN, based on landmark trial by Smith et al. 20 This observation reflects a gap between guideline recommendations and real-world practice. The predominance of gabapentin prescribing is likely influenced by institutional practice patterns, and medication accessibility. These findings are consistent with prior studies describing similar trends in clinical practice reported by Herz et al. 18 and Gauthier et al. 17 While Tsavaris et al. 21 suggested potential benefits for gabapentin in TIPN, the evidence remains inconclusive compared to the robust data supporting duloxetine. Our real-world data highlight an opportunity to align more closely with evidence-based strategies for TIPN. Although incorporating duloxetine as a primary first-line therapy, as supported by Smith et al., 20 the present study was not designed to evaluate its impact on treatment disruption or ED visits. Our findings highlight an opportunity for oncology pharmacists to lead evidence-based practices for the prevention, early recognition, and management of TIPN. Beyond promoting evidence-based management, oncology pharmacists play a key role in implementing regular neuropathy assessments, educating patients about reporting early symptoms, facilitating timely identification of clinically significant neuropathy, and recommending appropriate pharmacologic management. In addition, pharmacist participation in multidisciplinary care may support appropriate chemotherapy dose modifications when indicated, while minimizing unnecessary treatment interruptions and maintaining efficacy of antineoplastic treatment.
Although preventing TIPN remains an important clinical objective, no pharmacologic intervention has demonstrated sufficient evidence to support its routine use for prevention. Consequently, current clinical practice focuses on early recognition of neuropathic symptoms, patient education, regular symptom monitoring throughout treatment, and timely chemotherapy dose modification when clinically indicated to reduce the risk of severe or persistent neuropathy. These measures remain the cornerstone of preventing clinically significant TIPN until effective preventive therapies become available.
This study provides insight into the real-world incidence, outcomes and clinical management of TIPN requiring treatment among a relatively good sample size of Jordanian population; however, several limitations should be acknowledged. First, the retrospective, single-center design of our study, which may limit the generalizability of the findings. Second, the use of documentation in the medical records for data collection, which may have resulted in incomplete data and underreporting of TIPN. In addition, we did not use a standardized assessment tool to evaluate the severity of peripheral neuropathy, since this was not routinely available in physician's notes. Furthermore, no grading system for TIPN such as the Common Terminology Criteria for Adverse Events (CTCAE) was reported since these data were not routinely available in the medical records. Finally, we did not account for all potential confounders, such as nutritional deficiencies (e.g., Vitamin B12), hypothyroidism, and diabetes, which may influence the outcomes of TIPN. Future research should focus on prospective studies incorporating standardized neuropathy assessment tools to better characterize TIPN severity, treatment strategies, and clinical outcomes. Such studies would help clarify optimal management strategies and support the development of evidence-based approaches to improve patient care and minimize chemotherapy-related disruptions.
Conclusion
In this study, approximately one-in-seven patients with breast cancer on taxanes experienced TIPN that required pharmacologic management. In addition, half of the affected patients had substantial disruption of their chemotherapy regimens. Our findings reveal a critical gap between real-world clinical management and evidence-based guidelines, highlighting the need for prospective studies and standardized neuropathy assessment tools to identify high-risk patients and implement preventative measures that maintain treatment continuity.
Footnotes
Acknowledgements
None
Ethical considerations
The study was approved by the King Hussein Cancer Center (KHCC) institutional review board (IRB) (Study # 25 KHCC 118) with a waiver of consent because of the retrospective nature of the study that carries no more than minimal risk to patients.
Authors’ contributions
Tala Al-Bdour and Zahieh Abualoush contributed to the study design and framework. Data collection and preparation of study materials were undertaken by Tala Al-Bdour, Wala’a Alshwayat and Zahieh Abualoush. Data analysis was performed by Tala Al-Bdour. Validation and Supervision: Nour Faqeer. First draft of the manuscript was written by Tala Al-Bdour, all team members reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data supporting the findings of this study can be accessed from the corresponding author upon reasonable request.