
Abstract
Drawing upon research with criminalized women in Massachusetts, this article examines barriers to health care before, during, and after incarceration. Although very few of the surveyed women reported having had to forgo medical treatment because of an inability to pay, almost all of them reported being unable to access consistent, ongoing health care services. Typically, the women recalled sequential contact with dozens of providers at dozens of facilities, treatment plans that had been developed but never executed, psychotherapy that opened wounds but was terminated before healing them, and involuntary interruptions in legally prescribed courses of psychiatric medications. Acknowledging that these problems are related to wider structures of health care delivery in the United States, this article ends with a modest proposal for developing a role for health care advocates assigned to coordinate care for those with complicated medical problems to help them manage their health care needs over a long period of time.
Incarcerated Americans in prison and on parole face financial, administrative, structural, and interpersonal barriers to health care (Bowen, Rogers, & Shaw, 2009; Marlow, White, & Chesla, 2010). While abundant research shows that women’s health care needs often are more extensive and complex than men’s (Weisman, 1998), little is known about the relevance of gender to the health care experiences of Americans under correctional supervision as they move in and out of the prison system. The few studies of health and health care of criminalized women focus on women’s experiences in prison (Fearn & Parker, 2005), although the number of women under correctional supervision outside of prison is substantially greater. Morash points to “the large and growing number of women on probation and parole … in just one decade, there was a 56% increase in women on probation or parole” (2010, p. 3), a rate of increases that outpaces that for men. This research examines barriers to health care for this understudied population of postincarcerated women. Findings from interviews with a cohort of Massachusetts women indicate that, while access to health care is available, medical care frequently is disrupted and fragmented, leading to potentially poorer health for this population and increasing health care costs.
Literature Review
Continuity of Health Care Services
U.S. health care services are managed and delivered by a decentralized assortment of public and private institutions and agencies that increasingly fail to fulfill the mission of helping Americans maintain good health (Institute of Medicine, 2002). Lack of long-term planning, absence of a central organizational structure, deficient coordination among providers, unreliable insurance benefits, inconsistent eligibility for public programs, intermittent funding of preventative health measures, ambivalence regarding mental health services, and inadequate primary care, especially for the chronically ill, are some of the aspects of fragmentation that have been identified by scholars and policy makers (Bergeson & Dean, 2006; Hoffman & Sered, 2005; Jonas, Goldsteen, & Goldsteen, 2007; Porter & Teisberg, 2006; Richmond & Fein, 2007; Sered & Fernandopulle, 2005). While the federal 2009 Affordable Care Act addresses a variety of shortcomings and offers the potential for health care coverage for millions of currently uninsured Americans, the reform does not substantially unify or systematize health care services.
Individuals involved with the criminal justice system face additional layers of fragmented care because of entry into and out of prison and deficits in prison health care services (National Commission on Correctional Health Care, 2002). Ross and Lawrence argue that “The present demand-for-service and episodic style of ambulatory care in jails and prisons [which] treats each encounter as unprecedented, each complaint as isolated … is the single greatest impediment to quality of care” (1998). According to Bowen et al. (2009), when an individual enters prison, there often is irregularity and discontinuity in the medications they receive for mental illnesses. Moreover, changes and delays in medication were shown to cause anxiety, confusion, and distress among prisoners and contribute to poor relationships with prison medical staff. Marlow et al. found “the services participants [in their study] accessed were often inconsistently available, both as a result of their criminal lives and the availability of the services themselves” (2010, p. 24).
While the medical consequences of fragmented care for Americans with a history of incarceration have not been investigated, studies of the general population show that continuity of care is associated with greater use of preventive services and better control of chronic illnesses. According to Nutting, Goodwin, Flocke, Zyzanski, and Stange (2003), continuity of primary care relationships is most important for the most vulnerable populations. Cabana and Jee reviewed the medical literature and came to the conclusion that “increased SCOC [sustained continuity of care] heightens patient satisfaction, decreases hospitalizations and emergency department visits, and improves receipt of preventive services. [Also] the positive effect of SCOC on health care use has been well documented for patients with chronic conditions” (2004, p. 978). Saultz and Lochner reviewed studies from 1966 through 2002 and concluded that “a significant association exists between interpersonal continuity [of care] and improved preventive care and reduced hospitalization” (2005, p. 159; Pladevall et al., 2004). In a study assessing the immediate impact of disrupted and lost Medicaid coverage on Oregon adults, Carlson, DeVoe, and Wright (2006) found that those whose coverage was disrupted were less likely to have a primary care visit and more likely to report unmet health care needs, unmet medication needs, and medical debt than those continuously insured.
Health Care Needs of Criminalized Women
According to the Agency for Healthcare Research and Quality, “Women’s interactions with the health care system are characterized by fragmentation of services, poor communication with clinicians, and gender bias in receipt of treatment and services. While fragmentation of care is not limited to women, it is more pronounced” (Clancy, 2001). Weisman points to the tendency “to separate organizationally, or to fail to coordinate, reproductive health services and other components of women’s basic care” (1998, p. 121; Bean-Mayberry et al., 2007). “Since no provider has been trained in, or is accountable for, care of the whole woman, important health problems—such as the health consequences of sexual abuse or domestic violence—have been neglected both in research and in clinical practice” (Weisman, 1998, pp. 121–122). The estimated 60% of American women who have been victims of violence, rape, or abuse (Moracco, Runyan, Bowling, & Earp, 2007, p. 3) 1 experience especially high rates of long-term emotional disturbances and a variety of somatic symptoms, perceive their health less favorably than other women, make twice as many physician visits per year as nonvictimized women, and incur substantially higher medical expenses throughout their lives (Fickenscher, Lapidus, Silk-Walker, & Becker, 2001; Koss et al., 1994; Messina & Grella, 2006; Walker et al., 1999).
Chesney-Lind (2003) defines the criminalization of victimization as the recognition that large numbers of women are incarcerated because they have had the misfortune of having experienced violence. In a study addressing the mental health of women inmates, Green, Miranda, Daroowalla, and Siddique (2005) found that 98% of the 100 women they interviewed had been exposed to trauma, the most common of which was trauma associated with violence by an intimate partner (71%). Seventy-four percent reported problems with either drugs or alcohol and 25% reported having depression. Women inmates have higher rates of HIV infection and other sexually transmitted diseases than male inmates and higher rates of drug use disorder, and are in greater need of mental health services (Anno, 2000; Arriola, Braithwaite, & Newkirk, 2006; Arriola, Smith, & Farrow, 2006; Massachusetts Public Health Association, 2003; Ross & Lawrence, 1998; Staton, Leukefeld, & Webster, 2003). Overall, women inmates are 3 times more likely to report poor physical and mental health than women in the general population (Marquart, Brewer, Mullings, & Crouch, 1999; Young & Reviere, 2005). In one highly suggestive study conducted in Washington State, the adjusted relative risk of death among former inmates, as compared with other state residents, was significantly higher among women than among men (Binswanger et al., 2007).
Struggling with more numerous, severe, and complex health challenges than either nonincarcerated women or incarcerated men, criminalized women are in particular need of coordinated and continuous health care services (Eliason, Taylor, & Williams, 2004). 2 However, in one study, nearly 22% of incarcerated women missed important medications at least once during their prison sentence (Stoller, 2001). Relatedly, women in prison have reported waiting very long periods of time before receiving the care that they needed—in some cases, women have waited over a month to see a doctor while suffering with pain (Hatton, Kleffel, & Fisher, 2006). On average, women serve shorter sentences than men, highlighting the importance of Hyde, Brumfield, and Nagel’s (2000) finding that women inmates serving shorter sentences made more health care requests and used health care provider services more frequently than inmates with prolonged incarcerations. Ultimately, the health needs of women are not fully met as prisons often follow a male-centered and/or emergency room model for delivery of health care to female prisoners (Young & Reviere, 2005).
After release, criminalized women are often ill or hurt, and because they rarely are well integrated into a single primary care setting, they tend to make heavy use of emergency rooms (Staton, Leukefeld, & Logan, 2001; Staton et al., 2003; Staton-Tindall, Duvall, Leukefeld, & Oser, 2007). Emergency units are designed to deal with acute emergencies, not chronic conditions, and are therefore notorious for discharging patients quickly, although this is often in vain as people end up returning as repeat patients (Rhodes, 1995). Typically, emergency rooms are ill-equipped to deal with intertwined chronic physical, mental, and emotional problems, and even less equipped to deal with the constellation of abuse, drugs, legal issues, financial crises, and homelessness that are likely to plague criminalized women (Starfield & Shi, 2002).
In sum, substantial literature indicates the critical importance of comprehensive health care services for criminalized women as well as the elimination of barriers they face trying to access health care in prison and postincarceration. The present study builds on this literature through in-depth examination of how these complex constellations of needs and barriers impact the health care demands and health outcomes for specific women over the course of their adult lives.
Methodology
Data were collected between March and July 2008 at an urban Massachusetts residential recovery program for women recently released from incarceration. Upon formal approval from the program’s directors and the Suffolk University’s Institutional Review Board, and with the verbal agreement of the program participants, the authors attended weekly house meetings for 3 months to explain to the women the nature of the study, that their comments would be kept confidential, and that their participation was voluntary and would not affect the conditions of their parole negatively or positively. Thirty-two court-ordered women entered Kingston House during the 3-month period, and all of them volunteered to participate. The $15 mass transit ticket offered to participants as compensation for their time may have been a prime motivating factor for many of the women.
Interviews of 60 to 90 minutes were conducted by the principal investigators in a private office within the residential facility. Immediately prior to each interview, the participant was told that she could refuse to answer questions, she could terminate the interview at anytime, and she would receive the mass transit pass in any case. Participants were asked to sign a consent form indicting their understanding of the project. The interviews covered nine areas of inquiry including employment, education, family, relationships, children, drug use, criminal activity, and current and past health, health care, and access to health care. To gain a deeper understanding of the women’s lives, interviews included open-ended questions such as “What are some of the factors that have made it easier or harder for you to take care of your health?” and “Has it ever happened that you couldn’t afford medical care when you needed it? If so, what did you do?” Their answers were not verified through external records in order to protect their privacy and participation in the study.
Notes taken during the interview were later entered into a secure database at which time names and other identifying information were removed. Qualitative data derived from the open-ended questions were analyzed using an inductive/grounded theory approach that allows researchers to identify themes articulated by respondents in response to questions as well as spontaneously during the interviews (Ryan & Bernard, 2000; Strauss & Corbin, 2000). We used an open coding process to code the data according to categories that emerged as we examined the data, sorted by these codes to detect emerging themes, and then reconstituted and refined the categories to accommodate divergent experiences and meanings. Relationships among the themes together with specific illustrative statements form the basis of this article.
The Women
From the outset, it is crucial to clarify that the women interviewed in this study are not “hardened criminals.” The typical length of time they were incarcerated preceding this study is approximately 1 year. The respondents have spent far more of their adult lives in shelters, rehab programs, sober houses, transitional housing, and halfway houses than in prison. In short, prison is not a watershed event in their lives; rather, their relatively short episodes of incarceration are one station, and not necessarily the most important station, on the landscape of facilities that they visit over the course of life journeys characterized by sexual abuse and physical and emotional violence.
The demographic characteristics of our research sample are comparable to the characteristics of female inmates under the supervision of the Massachusetts Department of Correction as of January 1, 2006 (Annual Report, 2006). The median age of the sample is 35 years with ages ranging from 21 to 47. The majority is White (19), followed by African American (9) and Hispanic (5). Thirty of the women were born in the United States, and 20 have always lived in Massachusetts.
All of the women in this study live with chronic and acute physical and mental distress. Hepatitis C is the most common physical illness (14). Other physical illnesses include gynecological problems such as ovarian cysts (10), asthma (8), and chronic pain (3). Dental problems were cited by 28 of the women. Mental health issues include anxiety/depression (19) and other mental illnesses (14). Twenty-four of the women take prescription drugs on a regular basis.
All of the women (32) have used an illicit substance. Fourteen started serious use of illegal drugs before age 18; 11 began before age 14. Ten of the women had left home by the age of 15, and almost half (15) were on their own before the age of 18. Eight left home as minors because of physical or sexual abuse. Twenty-three of the women report having been hurt or afraid of being hurt at some time in their lives. For many, this was intimate violence. For others, the violence was committed by strangers. Close to one third of the women (10) report having experienced serious injuries.
Seventeen of the women were arrested for the first time before the age of 18. First arrest typically was for minor crimes such as drinking in public, trespassing, prostitution, driving under the influence, shoplifting, or having an open container of alcohol. The median age for first incarceration in a state or county facility was 25. While a few of the women were incarcerated in the wake of having committed one significant felony, most were incarcerated for minor offenses. The crimes they were incarcerated for immediately prior to this research were similar to the type of crime they were first incarcerated for in their youth. For many, a probation violation led to this incarceration.
Twenty-six of the women have never been married (thus, they are ineligible for dependent coverage through a spouse’s health insurance plan), and only 11 were employed either full time or part time before going to prison. In fact, only three women report having been covered through employment-based health insurance prior to their recent incarceration.
Respondents are unemployable or marginally employable for a variety of reasons. First, almost half (17) did not finish high school and approximately one third (11) have been formally diagnosed with learning disabilities. Second, the majority suffers from anxiety disorders that interfere with their ability to remain employable. Third, they may find it difficult to coordinate family responsibilities with the kinds of full-time jobs that offer health insurance. And fourth, many employers are unwilling to hire women or men who have been convicted of a felony. As one respondent who was found guilty of conspiracy in an assault and battery perpetrated by her boyfriend noted, “What is the likelihood that anyone will hire me once they do a background check even though I was never directly involved in the crime? I was just standing there when he tried to rob this guy.”
Findings
In this section, we present aspects of the fragmented health care system that our respondents described throughout the interviews. We begin with issues related to health care coverage policies, move to provider interactions, and end with issues of short-term facilities and the lack of coordination among facilities. However, we stress that this typology is artificial: In real-life institutions, policy and providers are an interconnected system. A change or disruption in one part of the system results in another part of the system often exacerbating the original problem.
Bureaucratic Challenges
Given their exclusion from mainstream employment-based insurance networks, the majority of the women depend on public programs, typically Mass Health (Medicaid), for health care access. While Massachusetts traditionally has had generous Medicaid eligibility policies, the women of this study find that their disrupted living arrangements are a poor fit for the bureaucratic requirements of Medicaid. For example, most of the women have spent much of their adult lives in halfway houses and detoxification programs, in homeless shelters, and on the streets, and half of the women (17) were homeless or living in shelters before their most recent incarceration. Describing a very typical sequence, one respondent commented, “I think my [Mass Health] card was sent to wrong address.” According to another, “I think my [Mass Health] card is with the halfway house I was in before [prison].” The women typically are taken off Mass Health when sent to prison, though in some cases their Mass Health seems only to be “frozen” and in need of activation when they are released. One woman explained, “The prerelease [staff person] was working on it [getting me on Mass Health]. I don’t know the whereabouts of it [Mass Health card] now.”
Often, the women acknowledge their own failure to stay on top of the appropriate application processes, a sequence that many of them find challenging in the wake of their limited educational attainments. For example, 47-year-old Clarisse deals with learning disabilities and a long history of domestic abuse. “[Before prison] I applied for Mass Health but didn’t follow-up so I didn’t have anything [coverage] … . I applied [for Mass Health] in prison and they said after I get out I have to call to give them my social security and my birth certificate, but they are lost.”
An additional set of bureaucratic complications is related to policy changes regarding services and eligibility. Thirty-nine-year-old Tyra, for instance, initially was covered by Medicare through SSI (Supplemental Security Income; assists disabled adults or children who have very limited or no income or resources) Disability because of her drug and alcohol addiction. Then, the policy changed. Disability no longer covered people suffering from these conditions, and she was “kicked off.” She then reapplied because of her bipolar diagnosis but was turned down 3 times. Finally, she hired a lawyer and now is back on Medicare. Even more commonly, the women pointed out that dental coverage sometimes has been covered by Medicaid and sometimes has not and that they did not always know what the situation was or would be when they embarked on dental treatments.
Provider Disruptions
Typically, particular facilities treat only one kind of problem, or treat women at only one stage of life or of illness. Thus, women may find themselves sent away from providers with whom they may have established a relationship. Carrie, who is 24, explains, “The clinic in [my hometown] will see you until you are 18, and then you are out. I don’t have a primary care physician. I’d like to see a doctor soon. It’s hard to take care of yourself when people [providers] don’t want to see you.”
Due to their reliance on Medicaid and free clinics, the women are vulnerable to the vagaries of state and federal budgets. Thus, it often was the case that good therapeutic relationships ended suddenly because providers left and moved on. Ashlee, who has been in and out of therapy for many years, noted that “It seems like once I get used to a counselor they have to leave and stop seeing me.” She spoke about one therapist whom she felt was really helping her, but that one had to leave the clinic she was working at and so she could not see her anymore.
Because of disruptions in health care coverage and provider relationships, respondents make great use of emergency rooms which, typically, are not equipped to handle the women’s complex physical, emotional, financial, and social problems. When we asked 37-year-old Janet how many times she has gone to the emergency room in the past 5 years, she replied, “Too many to count.” As an asthma sufferer since infancy, she has gone to the emergency room many times when her inhaler ran out and she could not pay for a refill. She has also gone to the emergency room for “homelessness that almost caused me to freeze to death.” While sitting in the emergency room offered her a day’s respite from the cold, once deemed ready for release she was back out on the streets.
Short-Term Facilities and Programs
Almost all of the women in this study have been in multiple short-term (7 day) detoxification programs. Referrals to detox can be initiated by the police department, a medical provider, a probation or parole officer, a family member, or (often) a call by the woman herself to a Massachusetts state hotline that directs her to a facility with an open bed. Some women have been in more than a dozen different detoxification facilities. Brittany, age 35, has been in hospitals for drugs and mental health problems more than 20 times since age 23, with each length of stay ranging from 1 day to 5 days to more. Marissa at age 25 has had 38 detoxes (some simple detoxes, some dual diagnoses). She estimates that she has spent about half of her adult life in various programs and facilities.
Christina explains why the detox system tends not to work. Now 32 years old, she has used heroin for the past 5 years. During that time she has been in a variety of standard 7-day detox programs. “I’d stay clean about a week on methadone. They wean you down and then at nothing I go back to heroin and leave the program. The programs basically abandon you when you are withdrawing from methadone. They don’t keep you long enough.”
Thirty-two-year-old Kaitlin’s experiences are illustrative. She comes from a middle-class family, graduated from high school, and attended some college. Beginning at age 15, she was in a relationship with a boyfriend who abused her physically and emotionally. In the wake of the ongoing abuse she developed anorexia, attempted suicide, and was diagnosed with posttraumatic stress disorder. She began abusing drugs at age 23. “Whenever I go [to a therapist] it’s two times and that's all. I end up either using [drugs] or I back off.” Following numerous failed detoxes and outpatient programs, she finally found some measure of success at a substance abuse treatment facility offering long-term programs. “It was a really good situation. I got sober there and stayed sober the whole time.” However, after 9 months at that facility, she was moved to a “sober house” and quickly relapsed.
In Kaitlin’s case, it is unclear whether the main problem was lack of communication between the treatment facility and the sober house or that she is not able to manage her mental health, physical health, and drug issues outside of a fully supervised care facility. What is clear is that in moving from an intensive facility to a freer, less supervised one, mechanisms were not put in place that enabled her to maintain her health. 3
Lack of Coordination Among Facilities
Transitioning from one clinic or program to another frequently leads to disrupted medical treatment. As one respondent explained, “They found out my cholesterol is high. At [a temporary respite facility] they were supposed to write me a prescription but the electricity went out [so they didn’t] and then I left there and came here [to the halfway house she now is living in].” According to another respondent, “My medical records, they got lost in transit when they moved me from prison to jail.”
The rigid time- and place-bound nature of prison health care results in an especially acute lack of coordination among services. Inmates have finite sentences and cannot go back to prison doctors after they are released nor can they see their previous doctors or therapists while they are in prison.
Upon being sent to prison, the women report, their regimes of medication are interrupted, laboratory tests that were conducted are never analyzed, and diagnostic procedures are terminated before effective treatment program can be established. Most of our respondents had been treated with psychiatric medications that require several months of regular usage to achieve therapeutic efficacy. However, prison policy is to take women off their medication when they arrive, thus disrupting medication regimes that help them maintain a reasonable level of functioning. In many cases, the sudden withdrawal from psychiatric medicine causes physical and emotional symptoms even more severe than the symptoms that the medication was prescribed to treat. Describing a case that may not be so unusual, Breanna recalls seeing “a girl sliced her body up in jail, because they took her off her meds. They sewed her back up and sent her back [to her cell].”
The single most common complaint voiced by the women was the long waiting time to see a doctor or nurse in prison. While many Americans feel frustrated when they cannot see their medical providers right away, for women in prison lengthy waits often mean that treatments begun outside prison are interrupted and that treatments begun inside the prison are not completed properly. According to Marissa, for example, the prison clinic received lab results indicating that she is infected with human papillomavirus (HPV) but waited 2 weeks to relay the results to her. In fact, she was only informed of the HPV infection on the very day that she was released. “They [the nurse] told me I definitely would get cancer and that I need to take care of this right away.” She was told that she needs to have a colposcopy. However, the prison health system did not offer her any care nor did the nurse offer to make phone calls for her to set up an appointment to follow up with a doctor after her release.
Marissa’s experiences were not unusual. Several women reported that during routine examinations the prison dentist diagnosed but did not fill cavities, that they received the first stage of medical diagnosis or treatment while they were in prerelease (the last stage of their incarceration time), and that they were informed of serious test results on the day of their release. Pregnant and postpartum women particularly struggle due to the absence of adequate postrelease health care arrangements. Not only do they confront the rupture of having their baby taken away (often), but also they may find that without the baby they no longer “count” as mothers for medical purposes.
Many of the women left prison without a sufficient supply of medication to last them until they can see a provider and get a new prescription. Often, the women stretch out their supplies of medicine by skipping days or taking half doses. Sometimes, the deficit may seem small but have grave implications. In Marissa’s case, she was released from prison while taking antibiotics. She had one day left to finish the course but was not given any pills to take with her. While in many circumstances missing one day of antibiotics could be insignificant, that was not the case for Marissa, who had been diagnosed with methicillin-resistant Staphylococcus aureus—a multiple-drug-resistant staph infection that is notoriously difficult to treat.
Unwanted Patients
As noted above, the majority of the women in this study have been victims of sexual or physical violence. In the experiences of our respondents, medical personnel rarely acknowledge the abuse and thus neglect linking them with appropriate services. Ninety percent of the interviewees recall having a family doctor while growing up. However, not a single interviewee mentioned that the doctor was helpful or advocated for them regarding the physical and sexual abuse they experienced. Even when they confided in their doctors, help was insufficient and fragmented. Ashlee, for example, recalls being abused as a child. “I was too afraid to tell the [family] doctor about the abuse. Then later I told him and he gave me some phone numbers, a hotline phone number.” And that was all.
Though all of the women make use of emergency rooms, not a single respondent mentioned that an emergency room doctor or nurse noticed or intervened regarding the physical and sexual abuse that they suffered as children. As adults, many of the women have gone to the emergency room in the wake of violent attacks. Thirty-eight-year-old Lillian was raped numerous times when “I was on the streets whoring. I can’t even count how many [times].” We asked her whether she went to the police. She replied, “I went to the police. They do the exam, hospital, and then send you back out.”
Several women reported that emergency room staff treated them with suspicion, assuming that they are trying to trick doctors into giving them narcotics or that they are thieves. Carrie, 24 years old and with a complex and lengthy history of being abused, forced into prostitution, STDs, bladder infections, asthma, and anxiety and depression in addition to drug addiction, explained how she has had to beg for services: “I had a blood clot and went to the emergency room. They thought I was looking for pain meds and sent me away and told me to stay off the street. I went to [another hospital] and they found the embolism and I was hospitalized for 2 months.”
Though most of the women express satisfaction with providers they encounter outside of prison, and overtly nasty interactions are rare, respondents have had isolated experiences in which medical providers were insulting, condescending, sexually abusive, or quick to assume that the patient worked in prostitution. After these sorts of interactions, the women moved on to another provider or facility; became more savvy about hiding from health care providers their histories of drug use, homelessness, and incarceration; or avoided medical care or psychotherapy altogether.
Discussion
All of the study women narrated health care histories characterized by fragmentation and chaos caused by bureaucratic changes and errors, high turnover of providers at public clinics, the short-term nature of most rehabilitative programs, and endemic lack of coordination among facilities—all compounded by the women’s self-acknowledged inability to stay on top of paperwork and appointments (see Figure 1). Typically, the women recalled sequential contact with dozens of providers at dozens of facilities, diagnostic tests that had been ordered and never carried out or carried out and then repeated in another facility, treatment plans that had been developed but never executed, sporadically managed chronic illnesses, contraindicated medications that had been prescribed by providers who did not know their medical history, appointments that had been made but not kept, medication and medical equipment that had been misplaced or taken away during moves between facilities, psychotherapy that opened wounds but was terminated before healing them, and involuntary interruptions in legally prescribed courses of psychiatric medications. While prison health care typically was rated as inferior to care outside of prison in terms of women’s lack of autonomy regarding making appointments or choosing providers, the same kinds of disruptions, fragmentation, and confusion characterized their care both inside and outside prison.
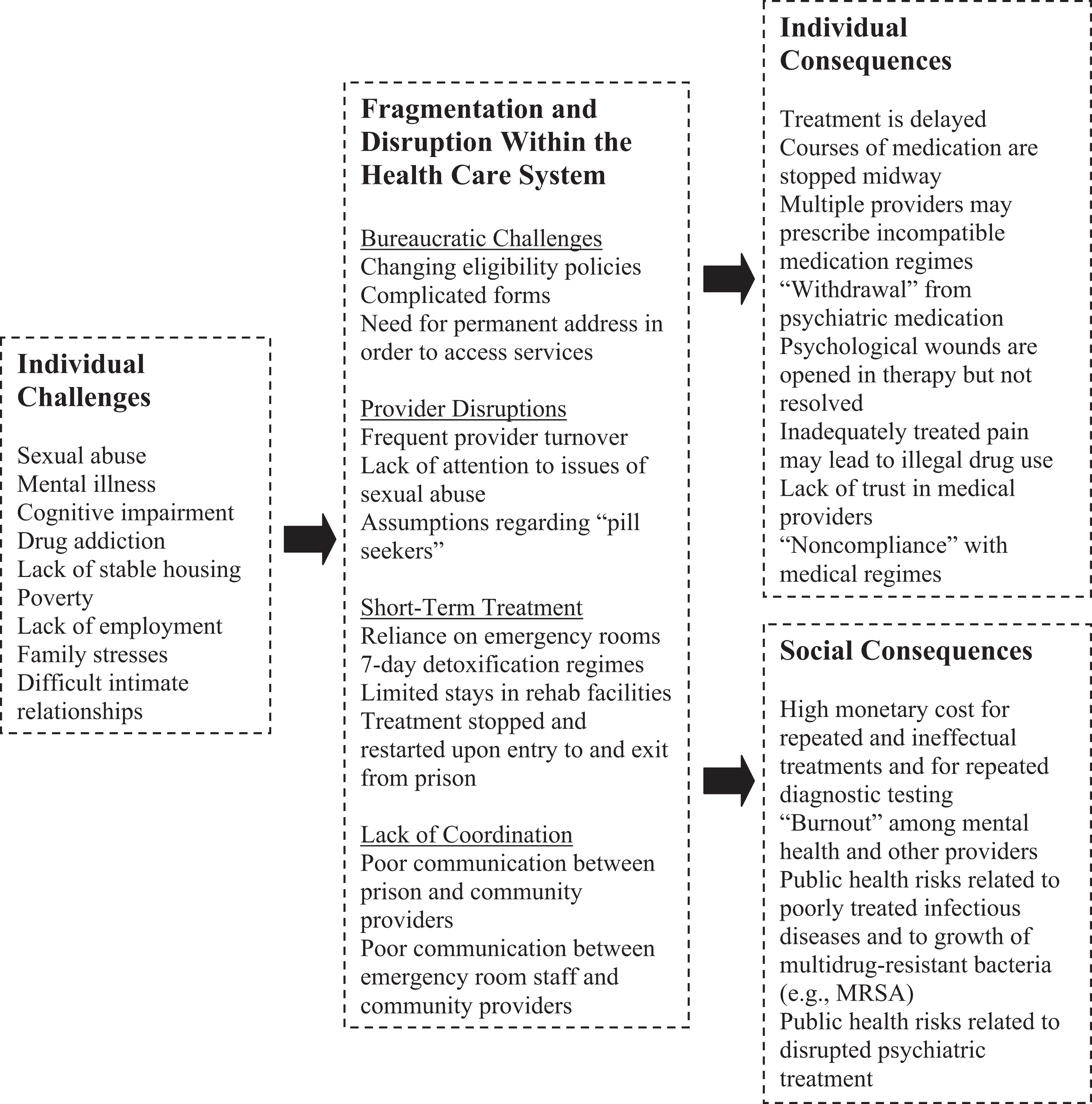
Consequences of Fragmentation and Disruption Within the Health Care System.
Overall, respondents did not have a clear understanding of how the health care system works, were often refused admission to beneficial programs, became ineligible for services that had been helpful in the past, had treatments stopped midstream, did not have the option of developing and implementing a long-term health care plan, hid information about themselves in order to receive care, begged for treatment that would be freely given to others, and dealt with providers and institutions that do not know their medical histories. In their stories, it is clear that the current health care service model for criminalized women not only fails to address their complex and chronic health problems but also, in fundamental ways, echoes them. Their own needs are never put in the center, their numerous problems are not seen in their full context, and dimensions of their being are isolated and then treated in different facilities and programs.
Figure 1 offers a schematic representation of the processes and consequences we have described in this article. When women carrying burdens of poverty, homelessness, victimization, and chronic illness access health care services that are disjointed, uncoordinated, and frequently disrupted, they may find that their problems are not resolved and sometimes actually exacerbated.
Fragmented care has negative consequences not only for the individual who bounces among numerous providers and facilities but also for society as a whole, in terms of both financial costs for redundant services and public health risks (Bowen et al., 2009; Cabana & Jee, 2004; Carlson et al., 2006; Pladevall et al., 2004; Saultz & Lochner, 2005). Poorly treated infectious diseases spread throughout shelters and prisons. Interrupted treatment of infections contributes to the rise of multiple-drug-resistant bacteria. Ineffectively treated pain may increase use of illegal drugs with all of the resultant public health dangers, while disruptions in regimes of psychiatric medication and psychotherapy may increase the likelihood of behaviors that endanger not only the individual but also the community at large.
A Modest Recommendation
Recommendations for systemic reform are beyond the scope of the present study. Still, we wish to offer the relatively modest suggestion that criminalized women could benefit from a permanent health care advocate or caseworker who helps them manage their health and health care needs over a long period of time and across all of the providers and facilities that they access (see Sun, 2006, on case management and the “one-stop shopping” model as a factor in substance abuse treatment effectiveness for women). 4
Some correctional facilities are trying innovative approaches to create bridges to care on the outside. In Massachusetts, Hampden County’s public health model for correctional health care has initiated a comprehensive program that includes education, prevention, treatment, and continuity of care (Grella & Greenwell, 2007). However, transitional case management programs typically continue for a relatively short period of time. To date, the largest multisite trial of transitional case management for parolees provided weekly case management sessions for 3 months and monthly contact for an additional 3 months postrelease. This trial led to outcomes not substantially better than those of standard programs, leading the trial investigators to suggest that more intensive case management may be necessary in order to produce more positive results (Prendergast et al., 2009). “Specifying a particular ‘dose’ of case management in terms of a minimum number of sessions fails to capture the complex nature of case management by applying a medical model where a needs-based model may be more relevant” (Prendergast et al., 2009).
The experiences of the women interviewed in the present study suggest that the model of a case manager associated with a given facility who works with a client on meeting specific goals while she is enrolled in a particular program would be unlikely to have a high impact. Rather, criminalized women may be more likely to benefit from a health advocate who would help coordinate services, ensure continuity of frontline care, keep track of past and present medication, understand the limitations that interfere with the client’s success at following through on treatment protocols, maintain contact even when the client misses appointments or changes addresses, and work with that client even when she moves from program to prison to home to a shelter to jail or to the streets.
Admittedly, even the best advocate is not able to arrange appropriate care when services do not exist or clients cannot access existing services because of cost or eligibility requirements. At the same time, the Massachusetts study suggests that availability of services is a necessary but not sufficient condition for good care. Thus, in conjunction with system-wide efforts to reform the endemic structural fragmentation that plagues American health care, medical advocacy could be one way to assist those with complicated medical problems in navigating the health care landscape.
Study Limitations and Directions for Future Research
This study was designed to elicit women’s perceptions of their lifetime experiences addressing health concerns. It is likely that medical records or interviews with health care providers would offer rather different kinds of information. With the important caveat that external “proof” would not make the respondents’ own perceptions more or less personally valid, future studies could explore issues such as provider burnout or the rate of redundant diagnostic testing for similar populations.
The current study was limited by the memories and concerns of the respondents on the particular day and time of the interview. Although the interviews were lengthy and open-ended, we assume that respondents tend to emphasize the events that felt most pressing at that particular time. Partly to address that limitation, we currently are conducting a 5-year prospective study with a cohort of criminalized women. In this study, we revisit the same women at 3-month intervals, each time asking the same questions about health and health care.
Finally, very few respondents of the present study reported having had to forgo medical treatment because of an inability to pay, a finding that is likely to be specific to Massachusetts and would not be characteristic of similar populations in most other states. We attribute the absence of financial barriers to Massachusetts’ high ratio of physicians to residents; the large number of medical institutions, especially in the Boston area; the state’s traditionally generous medical programs for uninsured and poor residents; and its comparatively liberal social service legislation and budgeting, especially for prison inmates. 5 Most important, in the wake of the 2007 Massachusetts health care reform, fewer than 3% of residents are uninsured, a rate that is substantially lower than in the rest of the country (Long, Cook, & Stockley, 2008, pp. 1–3). 6 Thus, studies of the health care needs of criminalized women in other regions of the country may well highlight financing and access issues in ways that were not relevant for the particular population of the current study.
Footnotes
Acknowledgment
We wish to thank Ashley Terhune, Ellesse Akre, and Joanna Prager for their help with this project.
Declaration of Conflicting Interests
The authors disclosed no conflicts of interest with respect to the authorship and/or publication of this article. For information about JCHC’s disclosure policy, please see the Self-Study Exam.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for the project has been provided by Suffolk University’s Summer Research Stipend, the Center for Women’s Health and Human Rights (Suffolk University), the Center for Crime and Justice Policy Research (Suffolk University), and the Massachusetts Bay Transit Authority (in-kind donations).