
Abstract
During July to November 2012, two botulism outbreaks (12 cases total) occurred in one all-male prison; both were associated with illicitly brewed alcohol (pruno) consumption. Inmate surveys were conducted to evaluate and develop prevention and education strategies. Qualitative surveys with open-ended questions were performed among inmates from rooms where outbreaks occurred to learn about pruno consumption. Quantitative surveys assessed knowledge gained after the outbreaks and preferred information sources. For the quantitative surveys, 250 inmates were randomly selected by bed from across the correctional facility and 164 inmates were interviewed. Only 24% of inmates reported any botulism knowledge before the outbreaks and education outreach, whereas 73% reported knowledge after the outbreaks (p < .01). Preferred information sources included handouts/fliers (52%) and the prison television channel (32%).
Introduction
Foodborne botulism is an acute, descending flaccid paralysis that can lead to respiratory paralysis and death. Clostridium botulinum, the causative bacteria that produces the botulinum toxin, is ubiquitous in soil worldwide. Botulinum toxin production occurs with specific environmental conditions—low salt, low sugar, low acid (pH > 4.6), no oxygen, and warm temperature (optimum range = 86°F to 95°F; Barzilay, 2008). In the United States, during 2001 to 2011, approximately 18 cases of foodborne botulism were reported annually (Centers for Disease Control and Prevention [CDC], 2013a); foodborne botulism outbreaks have most commonly been associated with consumption of home-canned vegetables (Sobel, Tucker, Sulka, McLaughlin, & Maslanka, 2004). In recent years, however, a new source of foodborne botulism has emerged: illicitly brewed alcohol made from potatoes in correctional facilities. While potatoes have previously been associated with botulism outbreaks (Angulo et al., 1998; CDC, 2012), this alcohol—also known colloquially as pruno, hooch, or prison wine—is a novel source that has led to five outbreaks, affecting a total of 25 persons, since 2004 (CDC, 2013b). These outbreaks can accrue high costs—one outbreak in Utah affecting eight inmates was estimated to have cost approximately US$500,000 in public resources (CDC, 2012). Pruno consumption is reportedly a common practice in correctional facilities worldwide (LeDuff, 2003; Wilkinson, 2005) because of the relative ease of production; however, knowledge is limited regarding inmates’ awareness of the associated health risks, and most currently available information is from informal accounts of pruno consumption while incarcerated (Gillin, 2003; LeDuff, 2003).
One correctional facility in Arizona, Prison A, reported two botulism outbreaks during July to November 2012, affecting a total of 12 inmates. Prison A is an all-male, maximum security prison with a fluctuating population of approximately 1,050 inmates. Intensive investigation revealed that the two outbreaks were unrelated; the only link was consumption of pruno made from potatoes. After the second outbreak, Prison A took multiple steps to educate inmates about the risk from pruno. Information from the CDC’s Internet site and fact sheets for inmates from a previous botulism prison outbreak were distributed and shown on the prison television channel, and educational sessions about botulism were given to correctional officers and groups of inmate peer educators. Whole potatoes and certain food items containing processed sugar, including sugar packets, candy, and sugar-sweetened beverages, were removed from the correctional facility’s menu as an additional means of preventing botulism outbreaks.
The goal of our investigation was to learn more about pruno consumption in correctional facilities, assess inmates’ knowledge about the risk for botulism from pruno, and ascertain inmates’ preferred health information routes for future education.
Methods
The investigation had two parts: a series of qualitative, open-ended interviews with inmates in affected areas of the correctional facility and quantitative interviews with a random sample of inmates from other areas of the facility. Interviews were conducted by public health staff over unrecorded telephone lines in visitation areas to maintain inmate confidentiality, and no correctional officers were present. Project methods were reviewed by the Arizona Department of Health Services institutional review board and considered exempt as public health practice in an outbreak response.
Qualitative interviews were conducted among persons from rooms (each containing 16 inmates) where inmates had been sickened by botulism during the two outbreaks; questions involved discussion of common methods of pruno production, consumption habits, and knowledge about the risk for botulism. No demographic information was collected during these qualitative interviews.
Quantitative interviews, conducted during the 2 months after the second outbreak, included questions to assess inmate knowledge about botulism before and after the outbreaks and preferred sources of health information. We excluded inmates in solitary confinement, in the detention area, on suicide watch, and in the previously interviewed outbreak areas (144 beds excluded in total). We randomly selected 250 beds from the remaining available beds (N = 1,008) and interviewed inmates who agreed to the survey; vacant beds were not replaced with other beds after selection. Responses from the qualitative survey were used to design quantitative survey questions. We analyzed the results by using SAS® 9.3 (SAS Institute, Inc., Cary, North Carolina). Demographic information was collected for the quantitative interviews and analysis.
Results
Qualitative Survey
We interviewed 31 inmates on two separate dates in January 2013 regarding their knowledge of pruno production and consumption in Prison A. Questions were open ended, and responses varied widely.
Pruno production
The majority of inmates reported learning how to make pruno by talking with other inmates and through experimentation. The Internet and television shows (e.g., Moonshiners, Discovery Channel®) were also mentioned as information sources. Common ingredients include fruit, sugar, bread, and rice; however, any available foods or condiments can be used, according to the inmates. Potatoes, in particular, were mentioned by the inmates as a good or the best ingredient in making stronger pruno. The process for making pruno was explained as simply sealing all items in a container (e.g., a trash bag or water bottle), mashing the ingredients together, and waiting for fermentation to occur (a 2- to 8-day process). When the liquid is fermenting, the container swells due to the gas production, producing a distinctive, potent odor difficult to conceal from correctional officers. Inmates reported heating the liquid by using body heat or hot water; others insisted that no heating was necessary. The reported volume made in each batch was also highly variable, ranging from a few cups to 3 to 4 gallons.
When the fermentation process is complete, the liquid is separated from the mash solids through a strainer (usually clothing). The liquid portion is then ready for consumption, although notably, one inmate reported distilling the fermented liquid to make stronger alcohol. Inmates reported it was challenging to acquire the ingredients and supplies needed to make pruno, and it was common to reuse items between batches. For example, the mashed base ingredients, also called the starter or kicker, can be used to make multiple pruno batches. Plastic bags are also reused for multiple batches. One inmate reported that both the starter and the bag that were used to make the alcohol that sickened inmates in November had been recycled from a previous pruno batch.
Pruno consumption
Inmates reported that pruno consumption was common and ubiquitous. They reported making batches as frequently as they were able to collect the needed ingredients and that this was more challenging and took longer in maximum security, as compared with lower security, facilities. Inmates and correctional officers commented that inmates consumed more alcohol around the holidays; the annual Super Bowl championship football game was also mentioned as a popular time for pruno consumption. The pruno is commonly shared among inmates who contribute to the ingredients. For example, inmates might spend weeks collecting ingredients, all of which are passed to one brewer. When fermentation is complete, the same inmates share the result. Inmates reported sharing between cells by fishing, or sliding items from underneath one cell door to another. Inmates who had spent time in other correctional facilities reported that pruno production and consumption is similar in other prisons.
Storage places for pruno in the cells included boxes for inmates’ classified legal documents (which inmates reported were less likely to be checked by correctional officers) and holes in walls, bunks, or ceilings. Some informal sources (Gould, 2005; Hogshire, 1994) suggest that pruno is commonly hidden in toilets; hence, another name for pruno is toilet wine. However, none of the responses from inmates interviewed in this investigation mentioned hiding pruno in toilets.
Inmates reported that the primary reasons for drinking pruno were to get drunk or to have fun. When respondents were asked if convincing inmates to stop drinking pruno was possible, inmates responded that it would be impossible.
We also inquired about any other illnesses associated with pruno consumption. Respondents often reported that they had not heard about any health risks, but others mentioned the possibility of vomiting, diarrhea, and blindness. No inmates reported knowing about botulism from pruno before the outbreaks occurred. Similarly, they had not heard of any increased risk associated with particular ingredients. The inmates interviewed often believed that illness from pruno was caused by others making the pruno wrong or using either rotten or unripe ingredients.
Another key part of the interviews was to assess the preferred way to receive health information. Television and handouts or fliers were frequently mentioned as the best ways to get health information to inmates. However, inmates did not trust certain information sources inside the correctional facility, and visitors were listed as the most trusted source of information. One other frequent comment was that inmates had learned about the risk for botulism only after the November outbreak; few reported hearing about the July botulism outbreak.
Quantitative Survey
A total of 163 inmates agreed to participate from the 250 selected beds, for a response rate of 65%. Nonresponses were attributable to refusals or vacant beds. Although data were not available to discern refusals from vacant beds, the facility reported that approximately 91% of beds were occupied; with this estimate, 228/250 beds would be occupied, for a true response rate estimate of 71%. All respondents were male, with the majority (55%) aged 26 to 35 years. Forty-nine percent self-reported as being of Latino or Hispanic ethnicity, 29% were White non-Hispanic, 10% were Black non-Hispanic, and 10% were American Indian/Alaska Native. English was the self-reported first language of 73% of respondents; 22% reported that they were native Spanish speakers (Table 1).
Quantitative Survey Respondent Characteristics by Age Category, Race or Ethnicity, Education Level, and Time Incarcerated in Prison A.
Self-reported highest education level attainment included junior high school or less (28%), GED or high school diploma (47%), or college education (24%). Inmates interviewed were also asked how long they had been in Prison A: 29% had spent < 6 months; 38%, 6 months to 2 years; 20%, 2 to 5 years; and 12%, > 5 years. The majority of respondents (79%) had a television in their cell, and 82% of these inmates reported watching the prison’s television channel.
Preoutbreak knowledge
Twenty-four percent of inmates said they already knew about botulism before the outbreak (Table 2). Twenty percent reported that they knew about foods and drinks that can cause botulism, with frequent answers including pruno and potatoes. Sixty (37%) inmates reported they had previously heard of persons getting sick from drinking prison-brewed alcohol. Respondents described sickness from pruno as including diarrhea, vomiting, alcohol poisoning, or kidney problems; blindness was also mentioned as a potential side effect of drinking pruno by 17 inmates (10%). Four (2%) said they had heard of persons getting botulism from drinking pruno before the current outbreaks; sources of such information included news or inmates in other facilities.
Quantitative Survey Responses Regarding Inmates’ Reported Botulism Knowledge Before and After Botulism Outbreaks.
Postoutbreak knowledge
After the second outbreak, 73% of inmates reported they had heard of botulism; 69% of these inmates said they knew botulism was associated with pruno or potatoes and other root vegetables. Other suspected sources of botulism included rotten food and items commonly included in pruno (e.g., fruits, vegetables, sugar, tomato paste, and bread or rice). The majority of inmates (80%) who had heard of botulism knew a person could get it from drinking pruno, and 74% described botulism as a “serious” or “very serious” disease.
Predictors of knowledge
No significant differences existed in reported botulism knowledge before the outbreaks occurred by age, race/ethnicity, education level, time incarcerated, presence of television in the cell, or survey date.
After the November outbreak, inmates with any college education were more likely to have heard of botulism than inmates with less education (39/39 or 100% vs. 79/123 or 64%, respectively, p < .01). Also, inmates with a television in their cell were significantly more likely to have heard of botulism (100/130 or 77%) compared with inmates with no television (18/33 or 55%, p < .05). No significant differences existed in postoutbreak knowledge by age, time incarcerated, or date interviewed.
Sources of health information
The most commonly mentioned sources of information about botulism in this facility included the prison television channel (44%), handouts or fliers (35%), other inmates (18%), outside television shows (10%), and correctional officers (6%). When asked how they usually received health information, the inmates reported getting information from staff at prison health services (24%), the prison television channel (21%), and handouts or fliers (21%). Inmates also reported getting information from family or friends outside the facility or from reading books or magazines. Preferred health information sources for future information included handouts or fliers (52%), the prison television channel (32%), prison health services staff (20%), and outside television (14%; Figure 1).
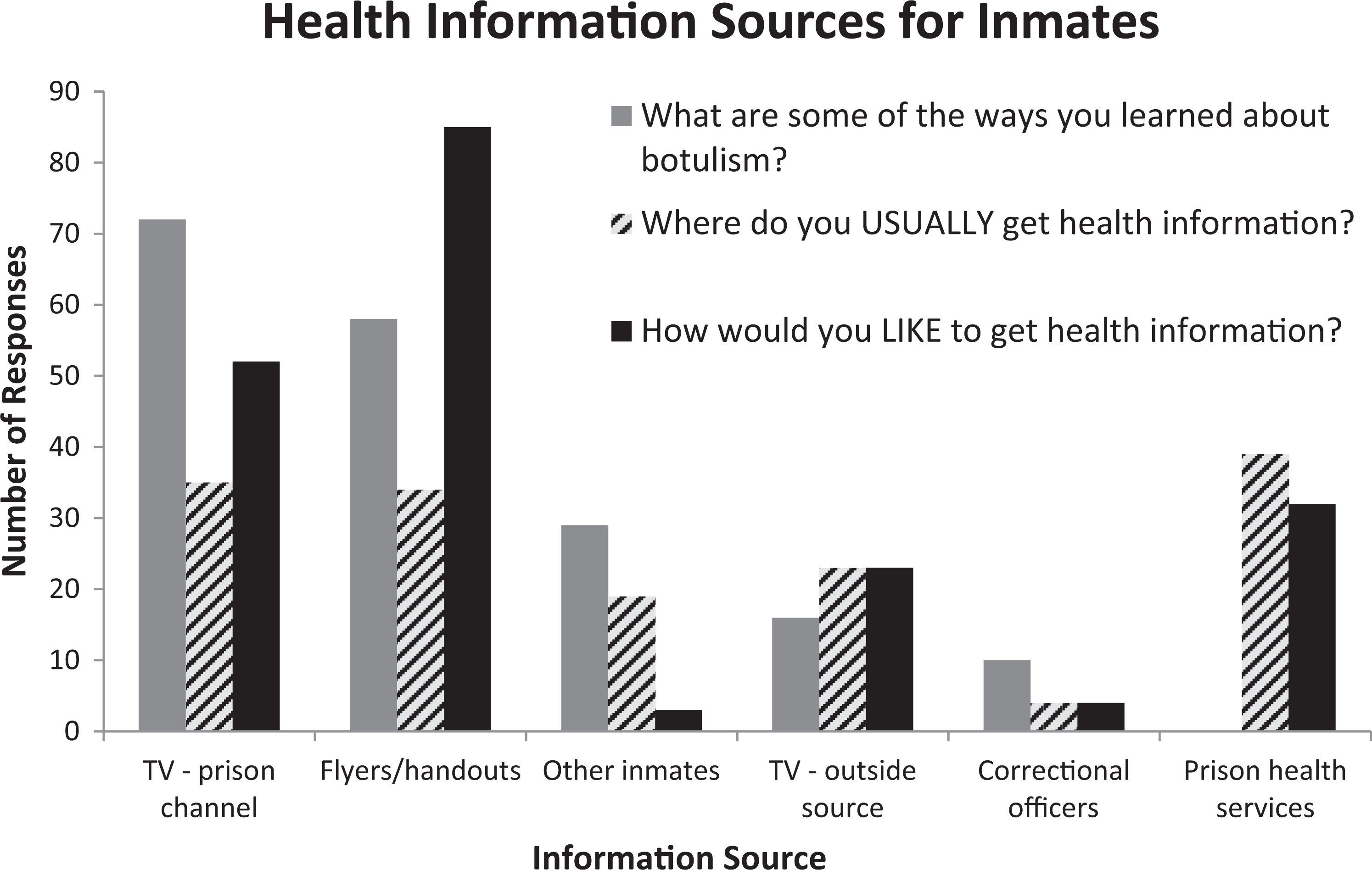
Inmates’ reported current and preferred health education sources.
Discussion
The findings of this investigation illuminate a number of concerns regarding pruno culture and consumption in this setting and demonstrate the effectiveness of an inmate education campaign to increase botulism knowledge and awareness of its association with pruno consumption. First, pruno consumption is ubiquitous, as reported by others (Wilkinson, 2005). Given the frequency of consumption, that only five pruno-related botulism outbreaks have been described in the literature is surprising. The low number of reported outbreaks might be the result of rare use of high-risk ingredients (i.e., potatoes), differences in brewing methods among prisons where outbreaks have occurred and other facilities, or a lack of recognition or reporting of outbreaks. Also notable is that all outbreaks occurred in maximum security facilities in Western states (California, Utah, and Arizona); the association with location is unclear.
Inmates often indicated that convincing inmates to stop drinking pruno would be challenging. Similarly, inmates reported that they believed others experienced botulism only because they made the pruno incorrectly—either from green or spoiled potatoes or from letting pruno cook too short or too long. Considering these views and the likelihood that inmates will continue to consume pruno despite health risks, standard botulism prevention strategies are needed in correctional facilities. Specific information about particularly high-risk ingredients (e.g., root vegetables) should be included in the materials as well as what factors increase or do not increase the risk for botulism. Our data indicate that education delivered by handouts or fliers and the prison television channel are the preferred media for health education in a correctional setting.
Inmates’ self-reported botulism knowledge did significantly improve after the outbreak and ensuing educational outreach. Although approximately a quarter of respondents reported that they had heard of botulism before the outbreak, less than 10% knew about the risk associated with pruno; however, 80% reported being aware of the risk associated with pruno after the educational outreach.
Another strategy employed by Prison A to decrease pruno production and the subsequent risk for pruno-associated botulism outbreaks was to eliminate potatoes served to inmates. However, reports from inmates participating in this investigation do not indicate that eliminating potatoes or other root vegetables is likely to reduce pruno production or whether that action would be effective in reducing the risk for pruno-associated botulism.
Limitations
Our investigation had certain limitations. First, response bias might have affected the survey results, and we were unable to assess the characteristics of nonrespondents because the refusals occurred at the cell level (before arrival to the visitation area) and demographic information about these persons was unavailable. Additionally, inmates were asked questions about retrospective knowledge of botulism before the outbreaks occurred 2 to 6 months prior, which might have been affected by recall bias. However, this would likely decrease the reported effects of the education campaign because respondents might have thought they already knew about botulism before the outbreak when they actually learned about it through prison education. Also, some inmates could have arrived at the facility after the outbreaks and education and thus know less about health risks from botulism than inmates who had received the education. Lastly, knowing whether inmates’ increased awareness of botulism and the association of pruno with the disease were the result of the education outreach, the occurrence of the second outbreak, or a combination of the two is impossible.
Recommendations and Conclusions
Because of the morbidity and mortality associated with botulism and the increased risk among incarcerated populations for this disease, effective and evidence-based prevention strategies are needed. The results of this survey indicate that inmate education about the risks for botulism by using paper-based educational materials or in-house television channels might be an effective way to increase awareness among this population. Other means for minimizing the risk and morbidity from botulism outbreaks in correctional facilities should include education for correctional officers regarding signs and symptoms of botulism to ensure rapid detection of cases and prevent progression to respiratory paralysis and death. Further study of the role of regulation of high-risk food items in correctional facilities (e.g., potatoes and other root vegetables) is needed to determine whether this is an effective strategy for reducing the risk for botulism in correctional facilities. No other botulism outbreaks have been reported from this facility as of February 2014.
Footnotes
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Acknowledgments
We would like to thank Nandini Sreenivasan, Maroya Walters, Agam Rao, and Mountain Vista Medical Center.
Declaration of Conflicting Interests
The authors disclosed no conflicts of interest with respect to the research, authorship, or publication of this article. For information about JCHC’s disclosure policy, please see the Self-Study Exam.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.