
Abstract
Timely reporting of disease outbreak and access to the outbreak site are necessary for prompt investigation and control. Local health departments (LHDs) establish the reporting time frames, methods, and communication channels within their jurisdictions in advance. This report describes a salmonellosis outbreak investigation in a federal correctional center (FCC) that was delayed due to issues with jurisdictional ownership and with separate reporting protocols for the FCC. The setting of the outbreak within an FCC posed additional unique challenges to the outbreak investigation. These challenges resulted in the outbreak response being delayed by 6 days and inconclusive investigation. It is recommended that LHDs and FCCs work together to create an advance protocol for improved public health coordination, oversight, and response.
Introduction
Timeliness of disease reporting is essential for prompt disease investigation and control. Many health departments require certain disease conditions or health events to be reported within a certain time period. This time frame is usually determined based on the mortality and morbidity rates of that event in order to provide lifesaving interventions to the patient and population at risk. Thus, certain health conditions are required to be reported immediately by the quickest possible means, whereas others may be required to be reported later by a more routine route.
In addition to timeliness of reporting, quick access to resources is necessary to carry out an investigation. This may include access to a facility or site of an outbreak and access to medical records, the laboratory facility, or laboratory outcomes. An investigation can be seriously hampered and intervention hindered if access is delayed or denied.
This outbreak report describes the challenges encountered in responding to and investigating a salmonellosis outbreak in a federal correctional facility (FCC) in Texas. Salmonella infections have been reported to be major causes of enteric outbreaks in correctional facilities worldwide (Cieslak et al., 1996; Greig, Lee, & Harris, 2011).
In Texas, Salmonella infections are required to be reported within 1 week to the local health department (LHD) that has jurisdictional oversight (Texas Administrative Code, 2014; Texas Department of State Health Services, 2014b). Jurisdiction is usually determined by the domicile of the case(s) involved in the outbreak (Centers for Disease Control and Prevention, 1996; Texas Department of State Health Services, 2014b). The issues arising from delayed reporting, unclear jurisdictional ownership and reporting channels, incomplete access to the outbreak site, and the setting of an FCC are highlighted.
The Report: Initial Notification and Response Process
The Texas Department of State Health Services, Health Service Region 6/5 South (DSHS HSR6/5S) received a call from an epidemiologist at an LHD regarding an outbreak of salmonellosis in an FCC in their area of coverage and was seeking advice on jurisdictional ownership and how best to proceed.
At the time of the report, 35 inmates had presented with gastrointestinal illness within 1 week. Normally, only 1 to 2 gastrointestinal illnesses were observed per week. Additionally, 13 stool samples were positive for Salmonella.
Immediate Challenges to Response
DSHS HSR6/5S immediately set out to conduct an outbreak investigation; however, the FCC authorities declined assistance, insisting that the situation was under control. The FCC authorities also notified DSHS HSR6/5S that they were following a notification protocol designated from their regional office to the national headquarters, which was different from the Texas Department of State Health Services (2014a, 2014b) notification channels and protocol. At this point, DSHS HSR6/5S promised to follow up with the prison service daily to monitor the situation. However, the following day the prison authorities invited DSHS HSR6/5S to conduct an investigation. Figure 1 illustrates the time line and response process.
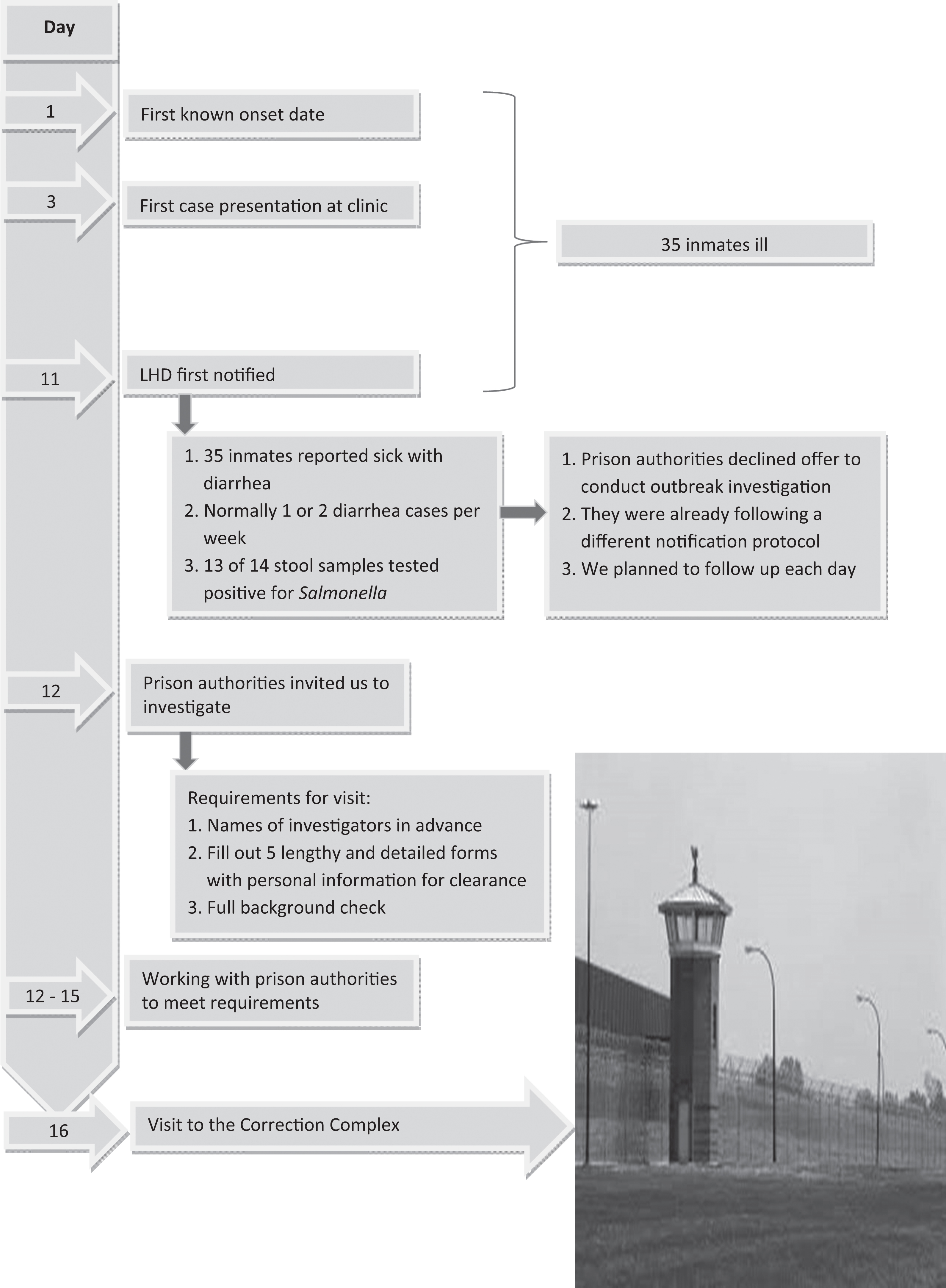
Time line and response process.
As we were about to go to the facility to conduct the investigation, we were told that we need to send the names of the outbreak investigation team members in advance. This was to enable the facility to conduct background checks and provide access clearance to all members of the investigating team. The process required filling out five lengthy and detailed forms with personal information for clearance and background check. This process normally would take us a few weeks to conclude. The Texas DSHS 6/5S authorities had to work with the prison authorities to expedite this process for another 4 to 5 days, including the intervening weekend, to be granted access to the prison to conduct the investigation. These prison system requirements, which were unfamiliar to us, resulted in a 6-day lapse between time of report and site visit.
Methodology
To investigate this outbreak, we reviewed prison protocols including food processing procedures. The site visit was conducted by a team of four epidemiologists and two sanitarians. Prison officials were interviewed to obtain relevant background information on the outbreak and intervention provided. Inspections of kitchens and cafeteria areas were done by the sanitarians.
Inmates were then interviewed using a structured questionnaire that included a list of menu items served in the cafeteria 1 week before the first case presented at the clinic. Cases in this outbreak were defined as Salmonella according to the DSHS case definition for salmonellosis, an illness of variable severity commonly manifested by diarrhea, fever, abdominal pain, nausea, and vomiting. Laboratory confirmation was by the isolation of Salmonella from a clinical specimen, in this case a stool sample (Texas Department of State Health Services, 2014a). A case is further classified as confirmed if it is laboratory confirmed and probable if it is epidemiologically linked to a confirmed case.
Results
A proper case–control study approach could not be fully accomplished, as no controls were made available. Nineteen interviews were completed using the prepared questionnaire. The 19 interviewed were inmates who had reported illness including inmates who worked in the kitchen. All were adult males, as this was in the male section. One was excluded from analysis because he was found to have flu and was not part of the outbreak. The major symptoms reported by the inmates are summarized in Table 1.
Major Symptoms Reported by Interviewed Sick Inmates.
Note. N = 18.
The earliest known onset date of illness for this outbreak was September 19, but the first eight cases were seen in the clinic on September 21 and by this time at least 15 inmates were already ill. Total number reported sick in this outbreak was 35, and all had reported illness before the notification to the LHD on the September 28 (see Figure 2). No noninmates (e.g., staff members) reported illness.
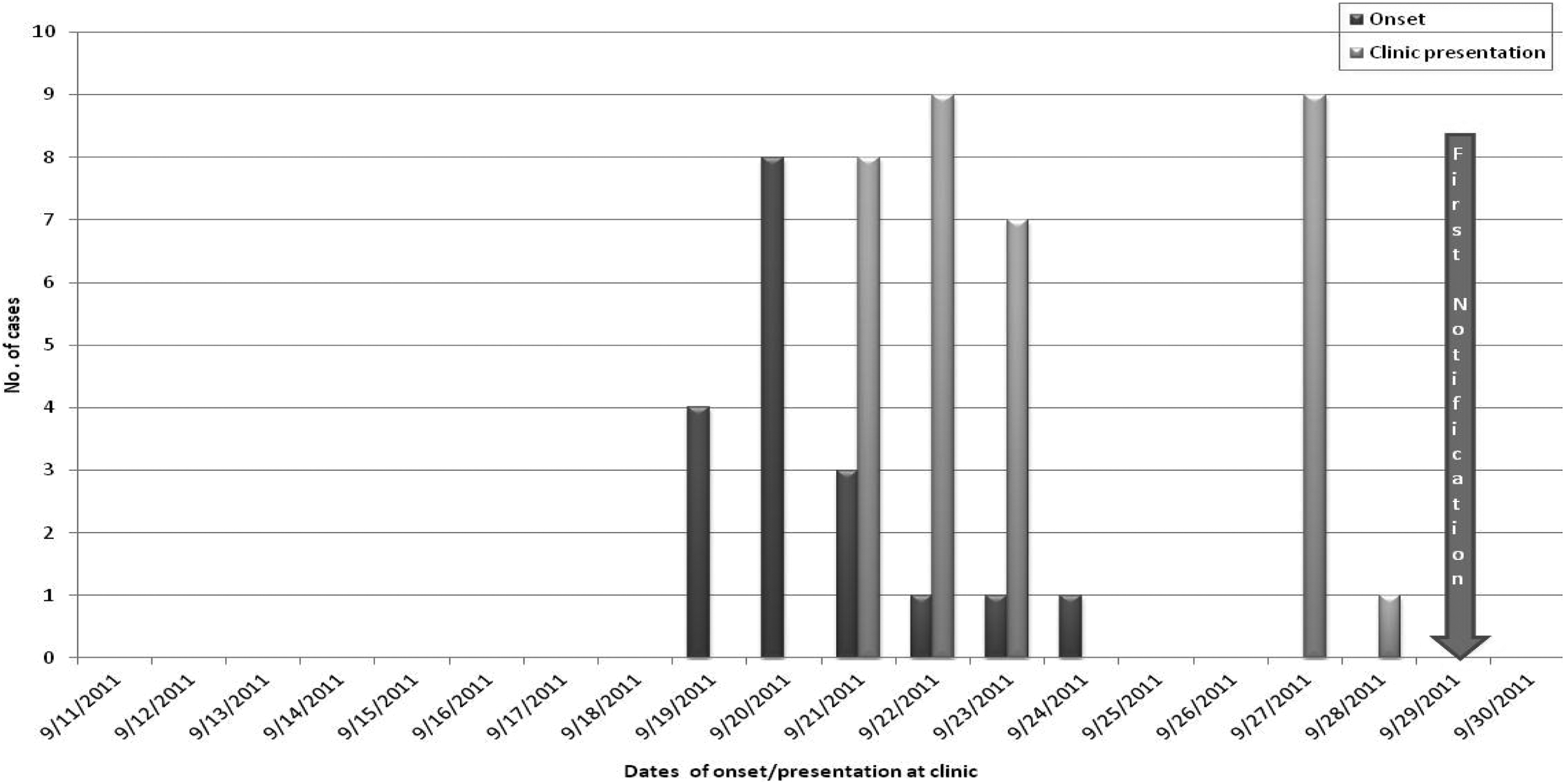
Epidemic curve of the outbreak (n = 18) and time line of presentation at the clinic (N = 35).
The duration of illness was between 1 and 14 days with a median of 4 days. Three reported cellmates who were also sick, the others did not. Four (4/18) inmates sought medical attention the very first day they had symptoms, another 4/18 the second day, while the majority (10/18) sought medical attention between 3 and 6 days after the onset of symptoms. Reasons given for delay in seeking medical attention include lack of trust in the prison medical services and the inability to pay the $2.00 co-pay. Twelve (67%) of the 18 inmates reported that they received medical attention the very first day they requested, while the other 6 said they were attended to between the second and eighth day of their requests.
There was no consistent or significant association of food items served and development of sickness. Anecdotally, 6/18 of the inmates implicated the chicken fajita served on Monday September 19 for lunch, 2/18 said it was the refried beans, and another 2/18 cited the meat loaf. Some inmates also mentioned ongoing construction work in the kitchen/cafeteria area as not conducive for use as an eating area. The sanitarians inspected the kitchen and eating area and did not find any violations. Food items served during the time the incident occurred were not available for evaluation or testing.
Thirteen out of 14 stool samples collected were positive for Salmonella. Only two isolates were available for serotyping and pulsed field gel electrophoresis (PFGE) analysis. Both were Salmonella typhimurium and were indistinguishable on PFGE.
Discussion
This outbreak was not reported to the LHD until 11 days after the first known onset date and 9 days after the first case presented at the clinic. This was at variance with what is required by state law for reporting cases of Salmonella infections (Texas Administrative Code, 2014; Texas Department of State Health Services, 2014b).
When the outbreak was reported, there was an additional delay of 6 days before a formal outbreak investigation could be conducted due to issues relating to jurisdiction and ownership of the outbreak and issues of obtaining security clearance for access to the FCC. There was also incomplete access to the inmates as not all of the 35 reported sick inmates were available for interview and no well inmates for comparison. There was limited access to the prison environments that were part of the outbreak for inspection. These challenges and delay greatly hampered this outbreak investigation, as the public health department did not have the opportunity to intervene early and fully nor to provide necessary leadership in outbreak management. For example, specimens were incompletely collected and processed; only 14 out of the reported 35 patients had specimens collected, only 2 of the 13 positive samples were available for serotyping and PFGE analysis.
In addition, initial data as to when the outbreak started proved inaccurate and led investigators to err on the time period on which to focus concerning food history and possible contamination. The delay was responsible for the nonavailability of the possible implicated food items for laboratory testing as they had been disposed of. These findings are consistent with other reports (Dishman, Wilson, Tobin-D’Angelo, & Drenzek, 2012; Tubach & Vajnar, 2014) in which delay in or lack of reporting from the facility, unreliable data, or logistical issues with conducting outbreak interviews, such as lockdown or prisoners under disciplinary actions, have been documented. This was compounded by the reluctance of inmates working in the kitchen to report illness and lack of possible implicated food items for testing.
Prisons and jails typically emphasize and prioritize security over infection prevention and control (Dishman et al., 2012), and typical prison settings are conducive to the spread of enteric infections. It is usually a crowded locked down environment; inmates are responsible for food preparation and handling and environmental cleaning; and access to medical care is limited.
This outbreak investigation highlights the fact that the correctional facility environment might pose peculiar challenges to outbreak investigation that are not seen in the general public environment. Security is crucial in the prison environment and so is the confidentiality of information. At any one time, more than 2 million people are incarcerated in the United States (Flanigan et al., 2009). Many are released with conditions that favor the occurrence and propagation of communicable disease (Hammett, Gaiter, & Crawford, 1998). It is recommended that mechanisms of prevention, timely identification and notification, and intervention be put in place. There should be a definite line of public health reporting whether the facility is federal, state, or county and also a procedure for public health to navigate security and access to the facility at short notice without delay.
With this in mind, it is recommended that LHDs and correctional facilities in the same localities work together to create an advance protocol for improved public health coordination, oversight, and response. They need to operate as community health partners.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. For information about JCHC’s disclosure policy, please see the Self-Study Program.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.