
Abstract
The United States has the highest rate of incarceration in the world. Many correctional facilities have outsourced the medical care for this population that often presents with complex health issues. This study evaluates the reasons that inmates present to an emergency department (ED) and compares them to the general population ED visits. The most common presenting complaints were trauma (16.8%), abdominal pain (13.5%), chest pain (9.0%), and self-injury (8.7%). These presenting complaints differed significantly from those of the general population (abdominal pain [8.1%] and chest pain [5.2%]). Inmate-patients seen in the ED presented with a significantly higher frequency of trauma, 16.8% versus approximately 1.5%.
Introduction
With 716 of every 100,000 Americans in jail or prison, the United States has the highest rate of incarceration in the world. American prisons not only constitute the single largest population of inmates but also account for over half of the world’s entire prison population (Walmsley, 2013). In 2013, more than 2.2 million people were incarcerated in jails and state or federal prisons in the United States (Glaze & Kaeble, 2014).
The Eighth Amendment has been interpreted under Estelle v. Gamble (1976) to require that the correctional system provide inmates with medical care. However, as the primary purpose of the Eighth Amendment is to protect against “cruel and unusual punishment,” the law remains vague in the medical setting. The ruling in Estelle v. Gamble stipulates that prison officials must not be indifferent to medical needs of inmates and that care is required if the medical need is serious (Posner, 1992). Many correctional facilities have outsourced medical care in order to improve the quality of health care for inmates while providing a cost savings to the facilities (Lafaive, 2004; Reeves, Brewer, DeBilio, Kosseff, & Dickert, 2014; Trestman, Ferguson, & Dickert, 2015). This is not surprising, as this socioeconomically underprivileged population presents with a cadre of complex medical issues for any health care system. Inmates often come from communities with limited access to health care. Many individuals have preexisting drug and/or mental health issues. Furthermore, a significant portion of this population is aging, presenting additional health-related issues and concerns.
Despite all this, there continues to be controversy regarding the benefits of outsourcing routine inmate health care to private companies (Kutscher, 2013; Leonard, 2012; Robbins, 1999). As a response to these debates, most studies have focused on chronic illness and infectious disease in this population as well as disparities that might exist in treatment (Maruschak, Berzofsky, & Unangst, 2015; Rosen, Hammond, Wohl, & Golin, 2012). However, there has been limited data on the acute care needs in the incarcerated. Medical issues that require immediate intervention involve transporting prisoners outside of the correctional facility to a nearby hospital or emergency department (ED) and encompass everything from chest pain and abdominal pain to injuries such as traumatic brain injury and facial fractures (Ferguson, Pickelsimer, Corrigan, Bogner, & Wald, 2012; Henning, Frangos, Simon, Pachter, & Bholat, 2015). Information regarding the treatment of acute illness and injury in the inmate population is lacking. In New York State, prisoners who are acutely ill present to the emergency room and are triaged appropriately. In most facilities, they share medical resources with the general public, but inmates also often require additional correctional and medical resources for transportation and supervision (Bale, 2009). To optimize efficiency of these limited resources, as well as to determine any disparities in care, it is first essential to understand the nature of the presenting complaints and the services required.
The primary objective of this study was to determine the specific health care needs of the incarcerated population that require transportation to an outside ED. Secondary objectives were to determine how the utilization of the ED from the incarcerated population compares to the general population.
Methods
We conducted a retrospective chart review of Department of Corrections (DOC) patients treated in the ED at an academic Level I Trauma Center in New York State. In 2013, the ED in this facility had an annual census of 67,000 patients. All adult patients 18 years of age and older who presented to the ED from January 1, 2013, to December 31, 2013, were eligible for inclusion. Patients with the DOC as the payer were identified electronically through department billing records. Electronic medical records were reviewed for chief complaints, ICD-9 diagnoses, number of readmissions, number of revisits, age, gender, prison location, and whether labs and imaging were obtained. For comparison to the general ED population, the Centers for Disease Control and Prevention (CDC) National Health Ambulatory Medical Care Survey (2011) was utilized. This is a national sample of visits to the ED and outpatient departments of noninstitutional general and short-stay hospitals.
Results
There was a total of 576 ED visits from 410 different DOC patients (mean age males 39.6 years ± 14.4 years, females 33.2 years ± 12.2 years; 89.2% male). The patients came to the ED from county jail (49.1%), state prison (48.6%), and unknown (2.3%). A total of 66.8% of patients underwent laboratory studies, 72.9% underwent imaging studies, and 39.8% of the presentations resulted in hospital admissions.
The 10 most common presenting complaints for inmate-patients seen at the ED were trauma (16.8%), abdominal pain (13.5%), chest pain (9.0%), self-injury (8.7%), neurologic symptoms (7.1%), hematologic symptoms (5.9%), seizures (4.5%), other (4.3%), abscesses (4.0%), and pulmonary symptoms (4.0%). One third of the inmates’ trauma involved facial trauma (33.0%). Adding trauma and self-injury together accounted for one quarter of the overall visits (25.5%). The total number of overall visits and the corresponding number of patients by presenting complaint are shown in Figure 1.
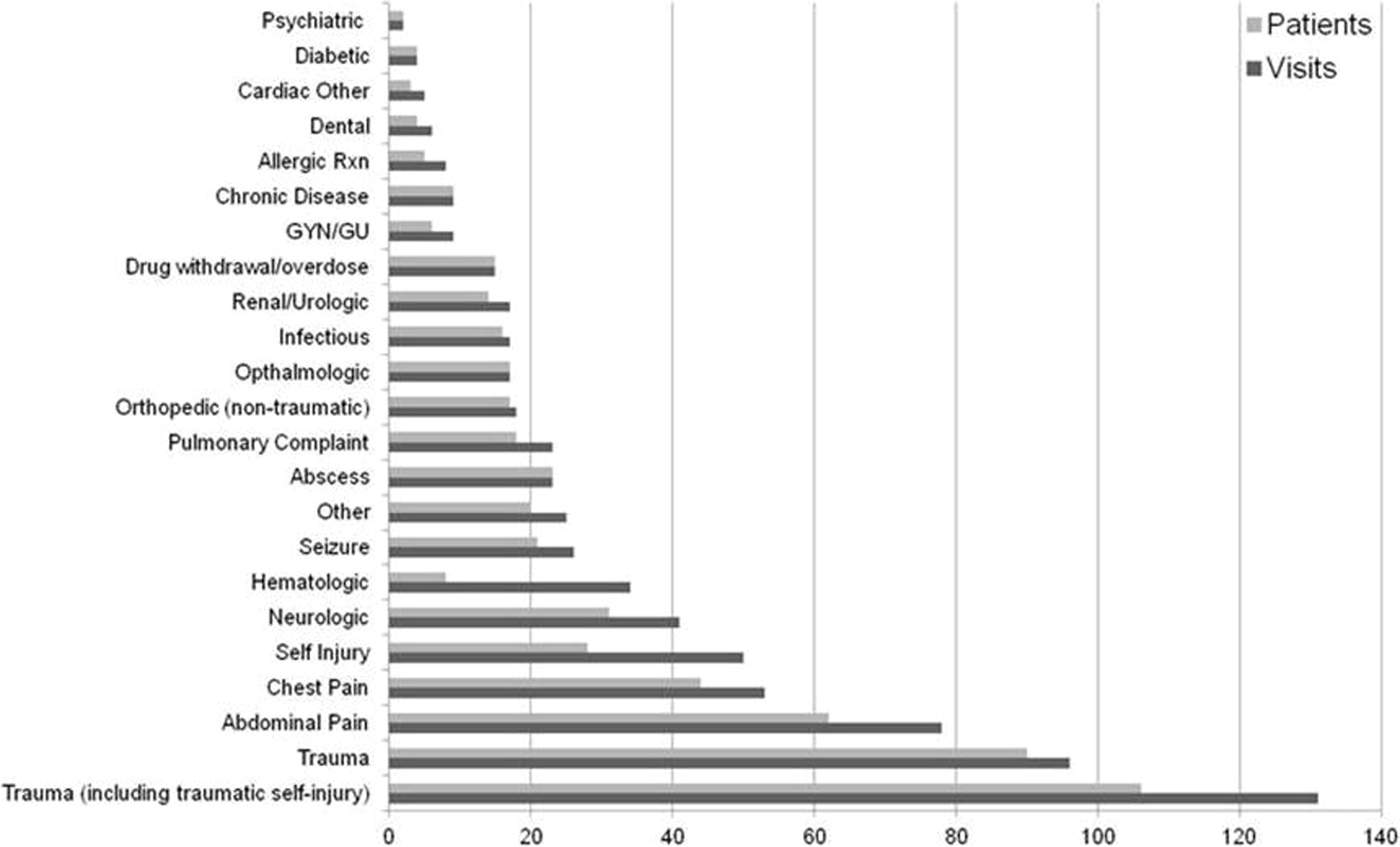
The total number of overall visits and the corresponding number of patients by presenting complaint.
Twenty percent of the inmate-patients seen at the ED had more than one visit during the study period, accounting for 43% of all visits. Hematologic symptoms, mostly comprising sickle cell crises, accounted for the greatest rate of revisits at 4.25 times over the year. The patients seen at the ED had a low proportion of mental health complaints, with 13.4% being diagnosed with Axis I mental health conditions. Axis I diagnoses include all clinical psychological disorders that cannot be attributed to mental retardation or personality disorders and include schizophrenia, mood disorders such as depression and bipolar disorder, anxiety disorders, and eating disorders.
According to the CDC (2011), the chief complaints for the general population were abdominal pain (8.1%) and chest pain (5.2%), rates both significantly different from the prison population (χ2 = 22.5, 95% confidence interval, CI [2.7, 8.5], p < .0001; and χ2 = 16.8, 95% CI [1.6, 6.4], p < .0001, respectively). Inmate-patients seen in our ED also present with a significantly higher frequency of trauma 16.8% versus ∼1.5% χ2 = 176.6, 95% CI [22.8, 25.0], p < .0001, compared to the CDC general patient population.
Discussion
This study indicates that inmates are utilizing our ED for a wide range of health care needs. While academic health centers may seem like a reasonable partnership for correctional facilities to outsource medical care in order to attend to inmates’ complex medical needs, it is not clear if these visits represent truly emergent issues. While the ED is well equipped to deal with complex medical patients, it is not the most appropriate treatment location for all medical care. Utilization of the ED for routine or nonemergency care may be an inappropriate and ineffective financial and health care model for the justice system, given that ED costs for the same medical services are generally higher compared to other care settings (McWilliams, Tapp, Barker, & Dulin, 2011).
Fewer than 40% of these patients required hospital admission, indicating that the majority could potentially have been seen in less acute settings. EDs nationwide are already experiencing overcrowding and extensive wait times (Hing & Bhuiya, 2012). Inmates require additional space to accommodate security escorts and safety provisions such as secure rooms, and for less acute conditions, it may be in the patients’ best interest for their care to be provided in a different environment. Certainly, many of these discharged visits, such as trauma, should be seen in the ED, and further research needs to be conducted to determine which of these visits could be handled in other settings.
The ED involves episodic care. In this study, many presenting complaints are chronic in nature, indicating a possible breakdown in ongoing care that either does not exist or is inadequate and has resulted in the escalation of severity, thus requiring emergency care. A large proportion of patients in the study presented for multiple visits within the same year. These individuals could represent two types of patients: inmates with chronic health issues that are not being adequately addressed or inmates with severe health crises that require emergency attention and potentially inpatient hospitalization. Patients with chronic health issues require continuity of care that is not practical in an ED environment. ED care for the management of acute exacerbations of chronic conditions is only one component of effective health care. This subset of the ED patients could present an area to investigate for potentially more efficient health care models.
It is not surprising that the majority of ED visits are trauma related. Injuries among inmates have been shown to occur at a higher rate than in the general population (Green, Hutchinson, Johnson, & Wilcox, 1996; Thorburn, 1999). The high rate of trauma in general (16.8% of visits), and facial fractures (1/3 of all traumas in this series) in particular, may suggest a need for greater access to trauma and otolaryngological/oral maxillofacial services within the justice system.
This study indicates that this population has unique health care needs that require acute care apart from what is available within the correctional facility. Continued monitoring of ED utilization by inmates may lead to identification of areas to focus on to increase the effectiveness of justice system health care infrastructure.
Limitations
This is a retrospective chart review at only one ED in New York State over the course of one calendar year. It is also limited by the imperfect identification of patients’ presenting complaints by emergency physicians. The biggest limitation in this study to assessing acute illness and injury in the inmate population is that their ED care is only a snapshot of their health care experience. The study did not attempt to identify areas for quality improvement for patients who did require admission and/or further care. This study did not include any information regarding inmate care before or after the ED encounter.
Conclusion
Inmates presented to our ED for a wide range of health issues. A greater percentage of the inmates than the general population presented to the ED due to trauma.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.