
Abstract
The burden of hepatitis C virus (HCV) infection is disproportionately high in U.S. federal and state prisons. This offers a unique opportunity for targeted HCV screening and treatment. New, highly effective, oral direct-acting antiviral (DAA) agents have the potential to eliminate many of the hurdles previously imposed by older interferon-based therapies. However, a relative deficit of providers motivated or empowered to treat HCV, along with a lack of treatment data on use of DAAs in prisons, greatly restricts the ability to treat the prison population. Here, we present a retrospective chart review of HCV treatment with DAAs by a family practitioner in a California state prison. Our data demonstrate that focused treatment by a primary care practitioner can achieve high HCV cure rates even in historically difficult to treat populations. Treatment of prison populations per local and national guidelines by family practitioners should be pursued to facilitate the eradication of hepatitis C in the United States.
Introduction
Hepatitis C virus (HCV) is one of the leading causes of morbidity and mortality in the United States, with 2.2 to 3.2 million Americans chronically infected (Denniston et al., 2014). In 2013, the Centers for Disease Control and Prevention (CDC, 2016) reported 19,368 deaths associated with HCV, an increase of 75% from 2003. In fact, HCV mortality is now greater than the combined mortality from all other infectious conditions reportable to the CDC (Ly, Hughes, Jiles, & Holmberg, 2016), emphasizing its significant burden on the health of the American public.
A disproportionately large HCV burden is borne by U.S. federal and state prison systems. Each year, approximately 30% of all people with HCV will be incarcerated, and recent estimates indicate that 17% of inmates have chronic HCV compared to just 1% to 2% of the general population (He et al., 2016; Ranieri et al., 2017; Varan, Mercer, Stein, & Spaulding, 2014; Zampino, Coppola, Sagnelli, Di Caprio, & Sagnelli, 2015). In some California state prisons, prevalence is as high as 35% (Fox et al., 2005). The comparatively high disease burden within the prison population offers a unique opportunity for focused screening and treatment. Since the vast majority of infected inmates are eventually released back into the community, there is a critical need to target the prison population for treatment if we are to achieve the goal of HCV eradication in the United States.
The emergence of direct-acting antiviral (DAA) treatment options has greatly increased our capacity for treating chronic hepatitis C in a safe and effective manner. In addition to attaining cure rates greater than 90% (Ara & Paul, 2015), the DAAs are ideal for use in correctional facilities because of their short treatment cycles, few contraindications, and mild side effect profiles (Spengler, 2018). The short treatment cycles are of particular significance for use within the prison system. In California, for example, HCV-infected inmates without cirrhosis are eligible for treatment with a 5-month minimum sentence and those with cirrhosis require only an 8-month minimum as per California Correctional Health Care Services (CCHCS) Care Guide: Hepatitis C. Older interferon-based treatments necessitated a much longer sentence to ensure treatment completion and adequate follow-up, limiting the number of eligible patients.
Despite the efficacy, tolerability, and short treatment duration of DAA therapy, significant barriers remain for HCV treatment in prison systems. A 2016 analysis by Beckman et al. (2016) found that only 0.89% of the 106,266 inmates known to have hepatitis C in the 41 states they queried were receiving any treatment. The price of the medications remains a major obstacle, with a 12-week regimen of ledipasvir 90 mg/sofosbuvir 400 mg costing approximately $94,000 (Beckman et al., 2016), although data have shown cost-effectiveness of such therapy (He et al., 2016).
A second barrier to treatment is a lack of provider expertise. Prisons often have limited access to specialists, and few primary care providers (PCPs) are experienced in hepatitis C management (Arora et al., 2010). This issue is being addressed in ongoing public health initiatives, such as the Extension for Community Healthcare Outcomes (ECHO) and telemedicine models that promote primary care–based hepatitis C treatment (Arora et al., 2010; Beste et al., 2017). However, data remain limited on the success of treatment with DAAs by independent PCPs, especially in the prison setting. Such data are crucial to help inform administrators, legislators, physicians, and the public about the efficacy of various HCV treatment plans and outcomes in prisons and to encourage PCP-driven therapy across the prison systems.
In this report, we analyzed HCV treatments using DAA-based regimens administered over a 2-year period by a family medicine practitioner at a California state prison.
Method
This is a retrospective chart review of all inmates with chronic hepatitis C at a California state prison. Patients included in the study cohort were treated with the new generation of DAAs from December 2014 to January 2017. Those treated with regimens that included peg interferon were excluded from the analysis. The designated prison is a California Department of Corrections and Rehabilitation (CDCR) maximum-security facility that currently houses 3,065 male inmates, 1,237 (40.4%) of whom have chronic HCV. Before data acquisition and analysis, approval was obtained from the California Protective Health Services, CDCR, and the University of California, Davis institutional review board.
A family physician (Dr. ***) working for CDCR managed all hepatitis C cases during the study time period. Now the designated and sole hepatitis C treatment champion at the prison, Dr. *** received one-on-one training from the outgoing champion prior to his retirement in 2013. He has had continuous communication with the CDCR hepatitis C oversight committee, which has reviewed and approved his HCV treatment proposals. His HCV treatment strategies have been strictly based on current American Association for the Study of Liver Diseases (AASLD) guidelines, and he has received continuous back-up from a board-certified hepatologist via telemedicine.
At the prison where this study was conducted, HCV-positive inmates were treated per the guidelines set by the CCHCS oversight committee and the AASLD. As outlined in Figure 1, patients were triaged based on the criteria developed by the CCHCS, which excluded many patients from the treatment-eligible group. Treatment eligibility was based on a combination of Fibrosis-4 (FIB-4) scores and fibrosis stage determined by liver histology and/or FibroScan®. Cirrhotic patients with documented decompensated disease (history of active esophageal variceal bleeds, ascites, or hepatic encephalopathy) were seen by a telemedicine hepatologist for case review and approval of treatment. Once approved for treatment, verbal consent for treatment was obtained from patients. A treatment application was then submitted to the CCHCS hepatitis C oversight committee, which employs the most current AASLD hepatitis C treatment guidelines to determine the appropriate treatment regimen for each patient based on viral genotype.
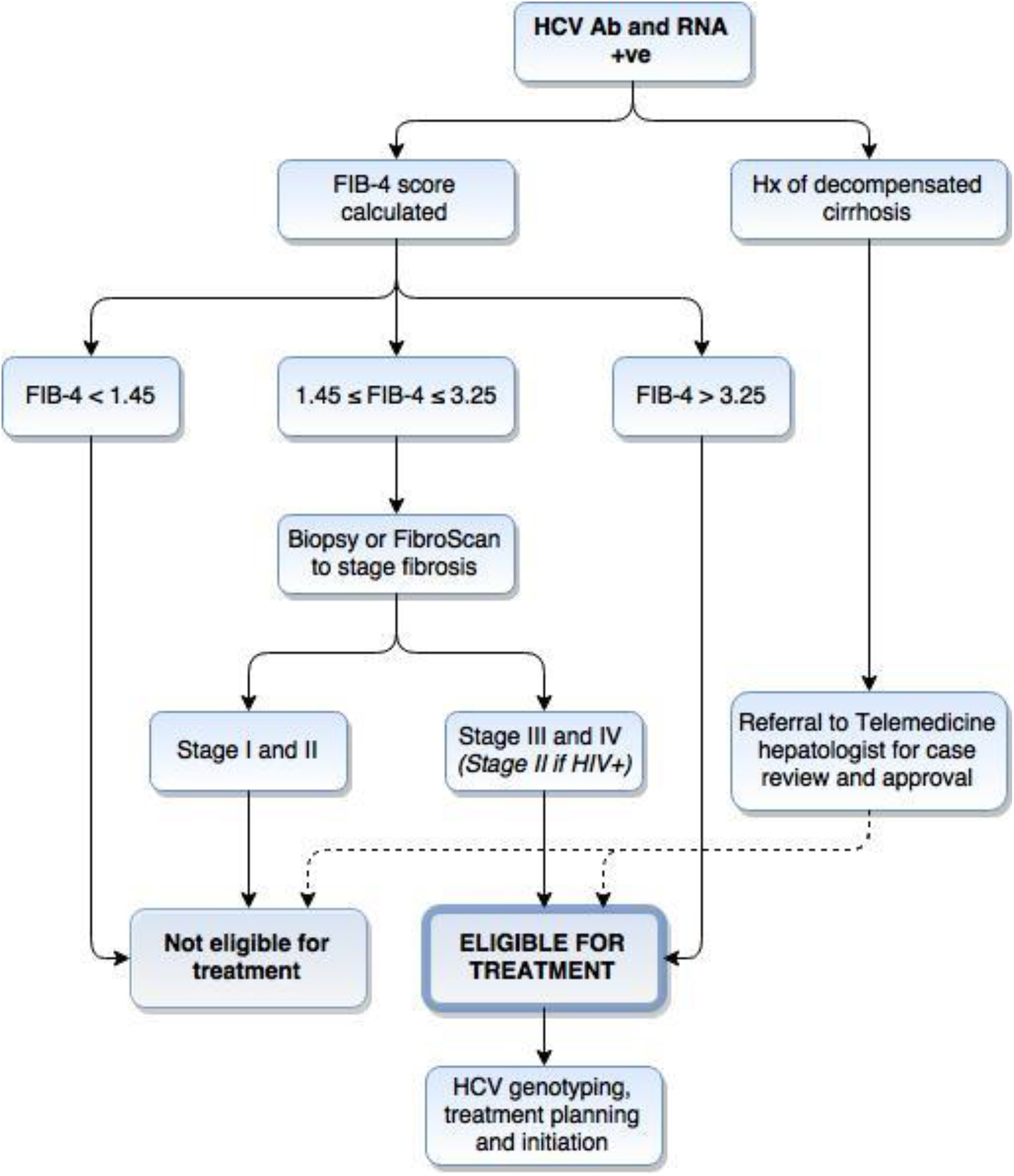
Triage of patients for direct-acting antiviral HCV therapy. Treatment eligibility was based on the criteria developed by California Correctional Health Care Services. Patients were triaged for therapy based on fibrosis stage as determined by biopsy results, FibroScan®, and/or FIB-4 scores. Cirrhotic patients with documented decompensated disease were seen by a telemedicine hepatologist for case review and approval of treatment.
All patients received their prescribed DAA medications direct administered once per day, and ribavirin twice per day, if applicable. Dr. *** and a registered nurse or licensed vocational nurse managed the patients throughout treatment at a weekly hepatitis C clinic. Treatment tolerance was monitored with blood counts and liver function labs taken at Weeks 0, 2, 4, and every 4 weeks thereafter until completion of treatment. Treatment response was evaluated with serum HCV RNA levels obtained before initiating treatment, at Week 4, upon treatment completion, and 12 weeks posttreatment. “HCV cure,” or sustained virologic response (SVR12), was defined as a nondetectable HCV viral count at 12 weeks posttreatment. Responders and nonresponders were grouped by several demographic variables, and χ2 tests of independence were used to determine whether treatment response was independent of patient demographic and disease characteristics.
Results
During the 2-year study period, 132 patients met the inclusion criteria and received HCV treatment with DAAs. The cohort was all male, with a median age of 53 ± 8.0 years (Table 1). The cohort was racially and ethnically diverse, with 44.7% White, 37.9% non-White Hispanic, and 9.8% African American patients. Asian and Native American patients made up a small minority of the sample at a cumulative 6.8%.
Baseline Demographics.
A majority (84.1%) of patients were infected with HCV genotype 1, while genotypes 2, 3, and 4 made up 6.1%, 7.6%, and 2.3% of the cohort, respectively. Ninety-five patients (71.9%) were cirrhotic based on histological evidence, FibroScan®, or a pretreatment FIB-4 > 3.25, and 16 (12.1%) showed symptoms of decompensated cirrhosis prior to treatment. One patient had confirmed hepatocellular carcinoma (HCC) and 10 patients (7.6%) were coinfected with HIV. Of the 59 (44.7%) patients who had been treated for chronic HCV previously, 32.2% failed prior treatment due to null or partial response, 27.1% due to HCV relapse, and 18.6% due to adverse events or treatment intolerance.
Of the 132 patients treated, 123 (93.1%) achieved SVR12. Eighty-nine of the 95 patients with cirrhosis (93.7%) and 15 of the 16 patients with decompensated cirrhosis achieved SVR12, as did 9 of the 10 (90%) patients with HIV coinfection. All nine subjects who did not attain SVR12 failed treatment due to relapse and included four Hispanics (44.4%), three Whites (33.3%), one African American (11.1%), and one Native American (11.1%). Six of the treatment failures were treatment naive and three had previously failed peg-interferon/ribavirin treatment. Seven (77.8%) of the patients were infected with HCV genotype 1 and the other two (22.2%) were infected with genotype 3. Of the 132 patients who initiated treatment during the study period, only 1 dropped out and therefore did not complete treatment.
A χ2 analysis of responders and nonresponders showed that SVR12 rates were independent of all documented patient and disease characteristics including age, race, body mass index, cirrhosis, decompensation, prior treatment exposure, HIV coinfection, and HCV genotype (Table 2). Grouping treatment modalities by HCV genotype (Table 3) and SVR/treatment failures (Table 4) show a predominance of ledipasvir 90 mg/sofosbuvir 400 mg treatment for genotypes 1 and 4 (83.9% and 100.0%, respectively) and sofosbuvir-based treatments (e.g., simeprevir/sofosbuvir, sofosbuvir/ribavirin) for genotypes 2 and 3 (87.5% and 100.0%, respectively). No significant difference in SVR12 rates was found between treatment regimens (p = .95).
Treatment Characteristics.
Medication Regimens by genotype.
Note. SOF = sofosbuvir; LEDI = ledipasvir; SIM = simeprevir; VIEK = ombitasvir, paritaprevir, ritonavir, dasabuvir; EBV = elbasvir; GRZ = grazoprevir; DAC = daclatasvir; RIBA = ribavirin.
Medication Regimens by SVR and Treatment Failure.
Note. SOF = sofosbuvir; LEDI = ledipasvir; SIM = simeprevir; VIEK = ombitasvir, paritaprevir, ritonavir, dasabuvir; EBV = elbasvir; GRZ = grazoprevir; DAC = daclatasvir; RIBA = ribavirin; SVR = sustained virologic response.
Discussion
This study supports the essential contribution and feasibility of HCV treatment by PCPs, especially in the prison setting where few studies have yet been performed (Post, Arain, & Lloyd, 2013; Ranieri et al., 2017). With an overall SVR12 rate of 93.1%, our study shows that incarcerated patients with HCV can be cured with DAAs at rates that match and surpass those observed in the general population, even with very limited specialist support. Notable, too, is the high cure rate even with the inclusion of patients from historically difficult to treat populations, such as those with decompensated disease, cirrhosis, and prior nonresponse to treatment. In the era of primarily interferon-based therapies, these patients were substantially less likely to achieve cure (Kemmer & Neff, 2007). Our findings agree with extant literature that suggests that even in these challenging patients, DAAs can be expected to demonstrate efficacy on par with that observed in patients without complicated disease (D’Ambrosio, Degasperi, Colombo, & Aghemo, 2017).
Several factors unique to correctional settings may have contributed to the high cure rate seen in this study. First, medication regimens for inmates are very tightly controlled. Inmates receive their medications directly from a nurse who verifies the correct medication and dose, and they are required to consume the medication in front of the nurse. Likewise, due to the regimented nature of prison schedules with the convenience of an in-house clinic, and the inmates’ largely positive relationships with the clinic staff, inmates rarely skip follow-up appointments. Thus, treatment compliance is at or near 100%, which is rarely seen in the outside world. A second factor that might contribute to the high success rate is a reduced risk for behaviors that could lead to reinfection. Although the inflow of contraband, such as intravenous drugs and hypodermic needles, remains a concern, inmate access to these materials is more restricted than it would be outside of the correctional setting. Unregulated tattooing and intra-inmate sexual activity continue to constitute sources of risk for the spread of HCV within the prison community. However, efforts to mitigate these risks have been initiated and include free access to condoms and education programs designed to inform inmates of the risk factors for HCV transmission.
Remarkably, cirrhotic patients responded to DAA treatment at the same rate as non-cirrhotics. Patients with decompensated disease and a history of treatment nonresponse also achieved SVR12 at the same high rates as patients without these pretreatment factors. The lack of a significant relationship between disease stage and SVR12 rate therefore argues against the rationing of treatment based on concerns about reduced efficacy in patients with more advanced disease. Treating HCV early with DAAs can eliminate the driving force behind progressive liver damage and thereby greatly reduce the risk of the disease’s most life-threatening and expensive complications, such as decompensation and HCC.
The high cure rate seen in our analysis is crucial for justifying the use of limited state or federal funds to pay for expensive DAA treatments. With the demonstration of SVR12 rates over 90%, legislators and taxpayers can be assured that their money is being spent efficiently on achieving real cures and not wasted on ineffective or inconsistent treatments. Additionally, several studies of targeted screening and treatment of HCV in prison populations have demonstrated cost-effectiveness of such plans. Using a simulation model to project long-term costs and benefits of HCV screening and treatment in U.S. prisons, He et al. (2016) found that the implementation of universal opt-out screening and treatment of inmates over a period of 10 years would decrease HCV disease-related expenditures by $760 million by reducing HCV transmission, advanced liver disease, and liver-related deaths. Their findings decry the shortsighted view of treatment protocols that ration treatment for only the sickest patients, given the extremely high costs of managing decompensated cirrhosis, HCC, and liver transplantation. As noted by Liu, Watcha, Holodniy, and Goldhaber-Fiebert (2014), the bulk of the financial benefit of expanded treatment will likely be appreciated outside of the correctional system—particularly by the Medicaid system—while the initial costs are borne by the prisons. However, this should not discourage correctional systems from implementing more widespread treatment, as the overall cost benefit stands to reduce state and national health care expenses while improving population health inside and outside of the prison setting.
The findings of our study also make a compelling argument for the expansion of independent PCP-based hepatitis C management. Greater familiarity with HCV treatment among PCPs would increase the number of providers able to care for hepatitis C patients and reduce reliance on less accessible (and more expensive) specialists. There are ongoing efforts to educate PCPs in HCV management, notably the ECHO and telemedicine models that promote primary care–based hepatitis C treatment (Arora et al., 2010; Beste et al., 2017). The results of this study suggest that PCPs working in prisons could be ideal targets for these programs. Beyond its important implications for prison medicine, transitioning the bulk of HCV management from specialists to PCPs in the community at large will allow a much greater patient population to access HCV care by increasing the availability of highly qualified care providers in the communities that need them most.
There are a few key limitations to consider in the interpretation of this study’s findings. These include its relatively small sample size, retrospective nature, limited study duration, and single site of investigation. Additionally, because the prison where this study was conducted continued to use ribavirin- and interferon-based treatments as well as DAAs during the study period, patients receiving those treatments had to be excluded from analysis, reducing our sample size. Further studies, with emphasis on larger sample sizes and multicentered data gathering, will be required to demonstrate the efficacy and cost-effectiveness of DAAs in incarcerated populations with HCV. Nevertheless, we believe the findings of this study are promising in their suggestion of PCP-guided DAA treatment efficacy in prisons and hope that this helps broaden discourse and clinical practice regarding HCV.
Footnotes
Declaration of Conflicting Interests
The authors disclosed no conflicts of interest with respect to the research, authorship, or publication of this article. For information about JCHC’s disclosure policy, please see the Self-Study Program.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.