
Abstract
Keywords
Nurses who care for patients with psychiatric disorders value the therapeutic milieu as essential to the recovery environment. The milieu serves as a group setting in which therapeutic interventions are based on consistency, security, trust, and modeling aimed at influencing the attainment of a positive patient/client outcome. Activities and interactions that occur in the environment, including each interaction with the treatment team, must support patients’ recovery. These interactions are based on the therapeutic relationship between behavioral health care providers and patients.
Professional nurses and behavioral health associates (BHAs; also known as technicians or aides) spend the majority of direct care hours with patients admitted to inpatient psychiatric units. Because nurses and BHAs often face high levels of work-related stress, they frequently form close professional relationships with each other. Interdependence is essential for the nursing staff to feel secure and function in often emotionally volatile and unpredictable environments.
Trust is a vital component of the nurse–patient therapeutic relationship. Nurses follow guidelines on how to foster a trusting relationship, including attentive listening, responding to patients’ feelings, consistency, and empathy (Kneisl, Wilson, & Trigoboff, 2004). They are taught strategies designed to nurture therapeutic relationships and gain patients’ trust. However, here is little formal education addressing appropriate staff responses to patients’ betrayal of the trusting relationship that occurs when nurses or other staff members are physically assaulted.
Nurses and BHAs learn through educational programs and acquire through clinical practice behavioral methods displaying acceptance and being nonjudgmental and caring without bias. Nonetheless, nurses and BHAs react humanly to traumatic encounters such as when they are assaulted. Basic education, training, and professional standards that guide practice may inadequately address complex individual and group responses to traumatic incidents resulting in actual or threatened injury of coworkers. Consequently, we explored the individual and work group response of registered nurses (RNs) and BHAs to physically violent patient interactions occurring on the acute, inpatient behavioral health nursing units of a private, urban, psychiatric hospital. What was discovered in this investigation could assist nurse administrators and nursing staff to identify problems that may require ongoing staff development programs and staff support services addressing the responses of nursing staff to coworker assault.
Background
Varying definitions of violence appear in published literature. Researchers and theorists often use the terms aggression and violence interchangeably (Irwin, 2006). Duxbury (2002) referred to aggression as verbal abuse and threats and violence as physical acts. The phrase “challenging behavior” has also been used to describe conduct that puts individuals or others in jeopardy (Duff, Redhead, Paxton, Iceton, & Rochester, 2006).
Statistics concerning the incidence of violence by patient directed at nursing staff are difficult to obtain. The literature revealed two barriers to obtaining accurate data: (a) lack of clear, consistent definitions of violence (Love & Hunter, 1996; Maguire & Ryan, 2007; Nolan, Dallender, Soares, Thomsen, & Arnetz, 1999; Zuzelo, 2010) and (b) failure of staff to report violent incidents (Bilgin & Buzlu, 2006; Ferns, 2006; Meyers, Kriebel, Karasek, Punnett, & Wegman, 2005; Zuzelo, 2010). Underreporting of nurse- or nursing staff–directed violence has been attributed to education; gender; socialization; personal experience, including self-esteem and self-perception; and social context and power dynamics (Ferns, 2006). The reporting of violent incidents has often been reserved for the most serious events (Maguire & Ryan, 2007).
The rate of psychiatric nurses subjected to physical violence is highly variable with incidence rates between 55% to 62% (Bilgin & Buzlu, 2006; Inoue, Tsukano, Mitsutaro, Kaneko, & Okamura, 2006). Bilgin (2009) found that 61% of nurses working in a psychiatric hospital had been physically assaulted during their career. Nolan et al. (1999) reported that nurses suffered violent incidents involving physical contact significantly more than psychiatrists, whereas Amoo and Fatoye (2010) indicated that of the staff attacked by patients, 93.1% were nurses and 6.9% were physicians. Maguire and Ryan (2007) revealed that in the 30 days preceding their study, 41% of nurses were treated for physical aggression, 38% experienced mild physical violence, and 1% encountered severe physical violence. Also, Yarovitsky and Tabak (2009) concluded that 76% of the staff working in a closed psychiatric ward had experienced an attack. Violence is also international in scope; 72.4% of psychiatric nurses in Switzerland reported feeling seriously threatened once or repeatedly, and about 70% experienced a physical attack once or repeatedly during their professional lives (Abderhalden, Needham, Friedli, Poelmans, & Dassen, 2002).
Data from the Bureau of Labor Statistics revealed that 48% of nonfatal injuries from occupational assaults and violent acts occurred in health care and social services, with most injuries affecting nurses, aides, orderlies, and attendants (U.S. Department of Labor Occupational Safety and Health Administration [OSHA], 2004). According to the Department of Justice’s National Crime Victimization Survey conducted during1993 to 1999, the average annual rate for nonfatal violent crime for all occupations was 12.6 per 1,000 workers, the nonfatal violent crime rate for mental health professionals was 62.8 per 1,000, and the rate for mental health custodial workers was 69 per 1,000 (U.S. Department of Labor OSHA, 2004). Inpatient unit characteristics, particularly frequent patient admissions and rapid patient turnover, influenced opportunities for violence (Bowers et al., 2009).
Female and male patients caused similar numbers of injuries (Lam, McNiel, & Binder, 2000), but the severity of the injuries correlated with the sex of the offender. Most serious attacks were committed by male patients (Yarovitsky & Tabak, 2009). Findings from a 14-month study (Tuninger, Levander, Bernce, & Johansson, 2001) showed no difference in rates of violence between patients with or without violent criminal records. In contrast, patients held in the hospital under mental health legislation demonstrated higher levels of aggression (Bowers et al., 2009).
Diagnoses most frequently associated with violence include schizophrenia (48.8%), bipolar manic illness (29.9%), and comorbid substance abuse (22.3%; Amoo & Fatoye, 2010). Biancosino et al. (2009) noted that schizophrenia was the diagnosis most frequently represented in violent patients and that personality disorders were more frequently diagnosed in violent patients. Additionally, unemployment has been found to be a socioeconomic demographic variable associated with aggression (Amoo & Fatoye, 2010; Biancosino et al., 2009).
Qualitative and quantitative investigations have explored psychiatric nurses’ perceptions of violence (Bilgin & Buzlu, 2006; Duxbury, 1999, 2002; Duxbury & Whittington, 2005). Currid (2008, 2009) identified violence toward mental health nurses as a stress-inducing experience. A strong positive correlation between psychological distress and negative change in professional functioning among nurses has also been reported (Yarovitsky & Tabak, 2009). Exposure to threats and violence at work also contributed to psychological distress in nurses’ aides (Eriksen, Tambs, & Knardahl, 2006). Psychiatric nurses’ responses to aggression and violence from patients evidence negative emotions related to fear, anger, frustration, despair, hopelessness, helplessness, apathy, desensitization, resentment, and job dissatisfaction (Bimenyimana, Poggenpoel, Myburgh, & Van Niekerk, 2009).
Bilgin and Buzlu (2006) demonstrated that 92% of psychiatric nurses believed that nurses working with mentally ill patients can expect to be assaulted at some time in their career. Most respondents believed that physically assaulted nurses are no less professionally competent than those who have not been attacked. Furthermore, Yarovitsky and Tabak (2009) disclosed that the higher the number of years of nursing staff education the lower the incidence of attacks, whereas Chen, Sun, Lan, and Chiu (2009) suggested that nurse college education increased the risk of patient aggression. Nurses who were less sociable and less tolerant were more frequently victims of physical assaults in their current jobs than their more outgoing, tolerant colleagues (Bilgin, 2009). Other risk factors associated with nursing staff victimization include being female, being younger than 30 years or older than 44 years, being unmarried, having short duration of employment, and having higher levels of anxiety (Chen et al., 2009).
Many nurses have believed that internal factors, including patient diagnosis, are predictors of violent behavior (Duxbury, 1999, 2002; Duxbury & Whittington, 2005; Nolan, Shope, Citrome & Volavka, 2009). Nurses commonly identified problematic interactions as a contributing factor in patient aggression, but they did not view their interaction as part of the problem (Duxbury & Whittington, 2005). However, patients often reported that provocation by staff triggered aggression (Nolan et al., 2009). In postincident reviews of violent episodes, 61% of staff believed that the incidents could have been predicted, whereas only 20% of patients believed that the incidents could have been predicted (Bonner, Dip, & Wellman, 2010).
Nurses who worked for more than 15 years in mental health services displayed increased tolerance toward patient aggression. Nurses identified as “tolerant” reported less emotional exhaustion and depersonalization with a stronger sense of accomplishment at work (Whittington, 2002). Jonker, Goossens, Seenhuis, and Oud (2008) concluded that nurses with more than 12 years of experience showed significantly higher self-efficacy scores for the management of patient aggression than their less experienced colleagues. Greater age and experience were associated with reduced incidents of patient aggression.
Nurses often perceived that institutional factors contribute to patient violence. Bilgin and Buzlu (2006) reported that 46% of nurse respondents believed that employing institutions admitted patients whom the nurses were not trained or adequately staffed to manage. Many nurses identified the physical environment as inadequate to prevent violence (Bilgin & Buzlu, 2006; Duxbury, 2002; Duxbury & Whittington, 2005). Some reports linked insufficient staffing to high levels of patient aggression (Bimenyimana et al., 2009; Currid, 2008), although a recent study disclosed that a greater number of staff was associated with higher levels of patient violence (Bowers et al., 2009). Bimenyimana et al. (2009) identified the lack of management and interdisciplinary team support as well as a lack of a comprehensive orientation as nurse-identified contributing factors to patient violence. Both patients and staff perceived restrictive regimens as contributors to patient violence (Duxbury, 2002; Duxbury & Whittington, 2005).
Research studies have explored nurse perceptions, support, and treatment following an episode of patient aggression. Nurses perceived considerable support from colleagues when confronted with patient aggression (Jonker et al., 2008). Following an assault, most nurses experienced the nursing team as emotionally supportive (83.3%), whereas only half (50.6%) perceived nursing management as emotionally supportive (Bilgin & Buzlu, 2006). More than half (56.8%) of the assaulted nurses did not receive training to facilitate healthy coping, although most (87%) would have liked to have received training (Bilgin & Buzlu, 2006).
Nolan et al. (1999) compared nurses and psychiatrists who were physically assaulted by patients and reported that a higher proportion of nurses than psychiatrists received some support following violent incidents. Many did not receive any support following the violent event despite believing that support was needed. Yarovitsky and Tabak (2009) found that 65% of those experiencing a severe attack reported emotional injury, including fits of rage, fear of patients, sleep disturbance, and anxiety, although only 25% sought professional help for their symptoms. Last, Bimenyimana et al. (2009) observed that psychiatric nurses reported ineffective coping in response to patient aggression, including substance abuse, absenteeism, burnout, and job dissatisfaction.
A review of the literature revealed studies addressing violence in the psychiatric clinical setting with most examining the etiology and aftermath of patient violence or nurse perceptions following violence. There is a paucity of published research addressing the influence of violence on the therapeutic milieu of the psychiatric unit and the reaction of the nursing team or strategies used to continue to care for patients after episodes of violence or injury of members of the nursing staff.
Main Study Concept
We operationally defined violence as the use of physical force against another person or group, resulting in physical, sexual, or psychological harm. Indicators of violence include, but are not limited to, beating, kicking, grabbing, pushing, biting, pinching, and using an object to strike another (adapted from International Labor Office, International Council of Nurses, World Health Organization, & Public Services International, 2002).
Method
We used four focus groups to collect data to elucidate the individual and work group response of RNs and BHAs to physically violent patient interactions on two acute, inpatient behavioral health nursing units. We relied on the interactions between group members and the researchers moderating the discussion recognizing that during focus group processes, group members influence each other, consistent with real-life interactions (Morgan, 1997). The participants’ interactions explicated individual and group responses to direct and indirect experiences of violence that were witnessed or vicariously experienced.
Ethical Considerations
Participants were recruited via an invitation letter to staff members of three inpatient, behavioral health units from two institutions within one health care system. Institutional review board approval was granted. The letter described the study, assured confidentiality, and specified compensation for time. Food and friendly networking were used as incentives.
Sample and Setting
Participants were selected based on willingness to adjust schedules to accommodate a group size of 3 to 10 people per group interview. Nurse managers were solicited to encourage staff participation by answering questions, promoting interest during staff meetings, and referring potential recruits to the researchers if additional information was requested. BHAs and RNs were recruited to provide group discussion consistent with the team dynamic. Participants were included if they were direct care providers in full-time positions working with adult inpatients admitted with acute care, behavioral mental health diagnoses. Managers, supervisors, and educators were excluded, given their indirect care responsibilities and the potentially detrimental influence that authority figures may have cast on the group discussion. Part-time or per diem employees employed for less than 6 months were excluded, given their potential inconsistent interaction with patients and the staff teams.
Focus groups were conducted at two locations, a large, urban medical center with a unit devoted to acute psychiatric care and a small (less than 150 beds), private psychiatric facility with comprehensive behavioral mental health services. Group interviews were held in private conference rooms with seating arrangements conducive to discussions and audiotape recording.
Data Collection
Four 90-minute, audiotaped interviews were conducted over a 2-month period with the groups size ranging from 4 to 6 RNs and BHAs. It is generally recommended to have four groups of 6 to 10 members (Kreuger, 1994; Morgan, 1997; Twinn, 1998). Participants consented to participate in the study prior to the start of the interview. The group interview was organized using a questioning route framework rather than a topical framework. The questions were preestablished and designed to promote comfort within the group by beginning with broad queries before narrowing to focus on critical, potentially disquieting questions. The investigators served as the discussion moderators; there were at least two investigators in each focus group session.
Participants were asked to (a) identify patient-to-nurse behaviors that were likely categorized by staff as “physically violent”; (b) reflect on thoughts, emotions, and actions occurring in response to a physically violent patient to nurse encounter specific to the assaulted staff member, assaulting patient, and other inpatients; (c) describe the team’s response to the violent encounter; (d) reflect on the influence of the team’s response to subsequent patient care encounters with the assaulting patient and with the other inpatients; and (e) identify team and individual responses that were helpful or not helpful following occasions of violence.
Debriefing followed each group interview. Flip charts were used during each session to organize discussions and track key points to facilitate participant reflection. Interviews ceased when there was substantive repetition between groups as determined by the investigators.
Focus groups were audiotape recorded and transcribed verbatim. Transcriptions were verified for accuracy by the individual researchers. Identifying data were removed. Transcribed interviews were merged into a single, paginated master file to facilitate organized data analysis.
Analysis
We systematically analyzed data by questioning, scrutinizing, and comparing using the following steps: reading, rereading, and reflecting on transcribed master file, flip charts, and field notes; coding interview transcriptions line by line to extract significant statements and formulate meanings (Colaizzi, 1978); developing an audit trail (Wolf, 2003) for verifiable identification of subthemes derived from clustered significant statements; grouping subthemes according to meanings and organizing under themes; organizing related themes to form major themes; and confirming thematic analysis through an expert nurse researcher.
The research team met on three separate occasions to discuss emerging and established themes in the data. We explored alternative explanations and explicated preexisting biases and assumptions to assure fidelity to the phenomena of interest (Colaizzi, 1978). The audit trail, constructed to assure credibility and confirmability, was shared with a peer reviewer. The exhaustive description was shared with a qualitative research expert and with several interested reviewers (Colaizzi, 1978).
Findings
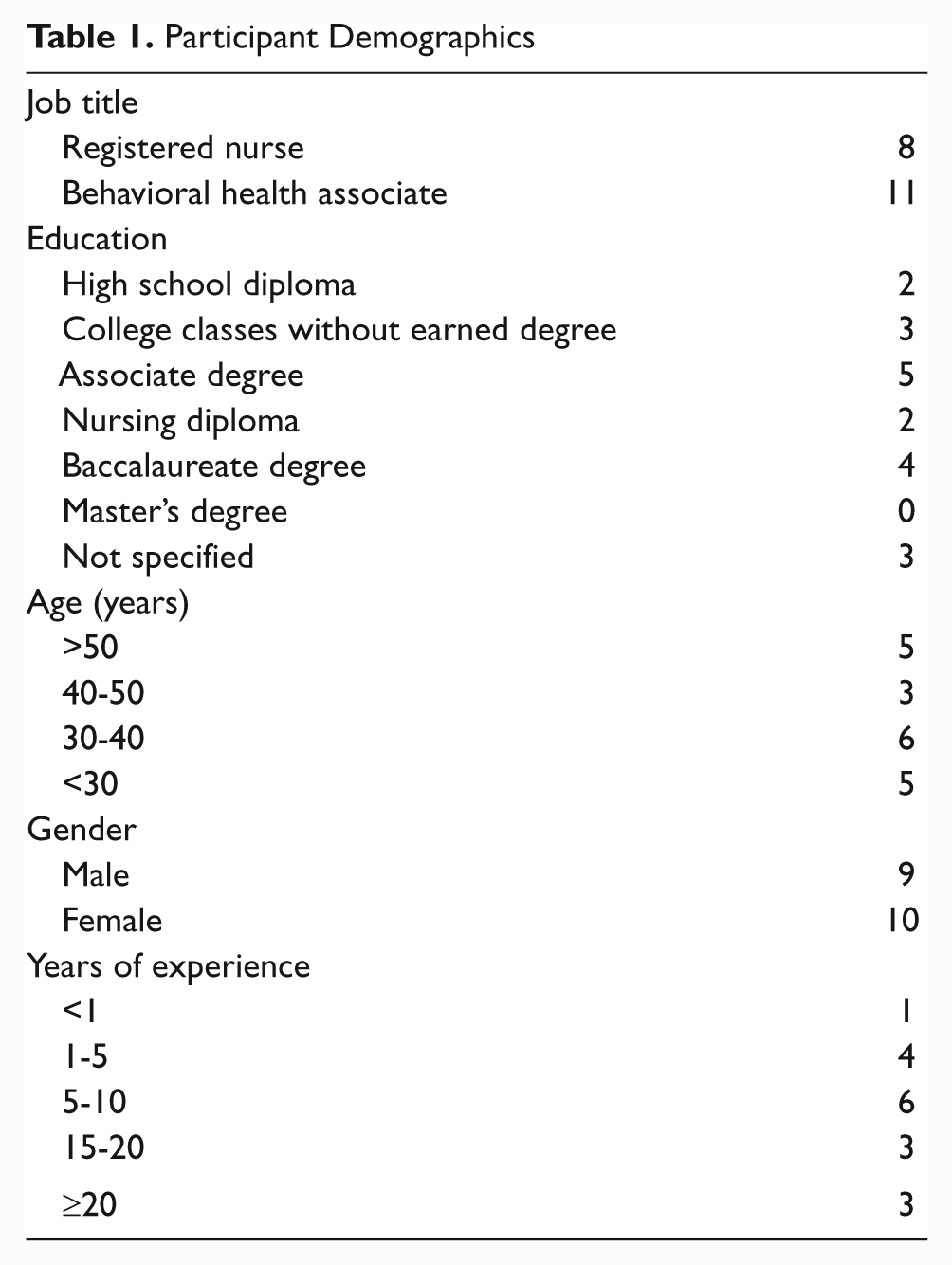
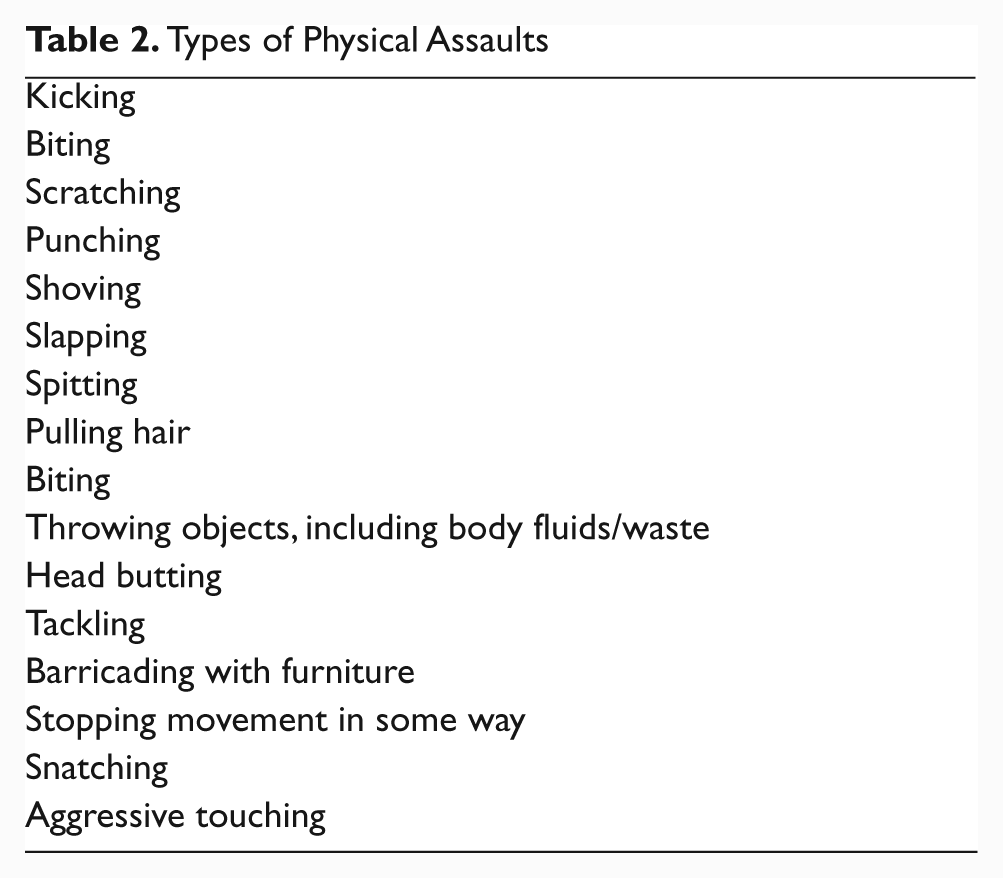
Participants (N = 19) included RNs (n = 8) and BHAs (n = 11) with varying levels of education and years of experience in behavioral health (Table 1). Participants across groups were consistent in their descriptions of encountered behaviors that were considered physical assaults (Table 2).
Participant Demographics
Types of Physical Assaults
Major themes, themes, and subthemes are woven in the narrative with selected quotes offered to provide description (Figure 1).
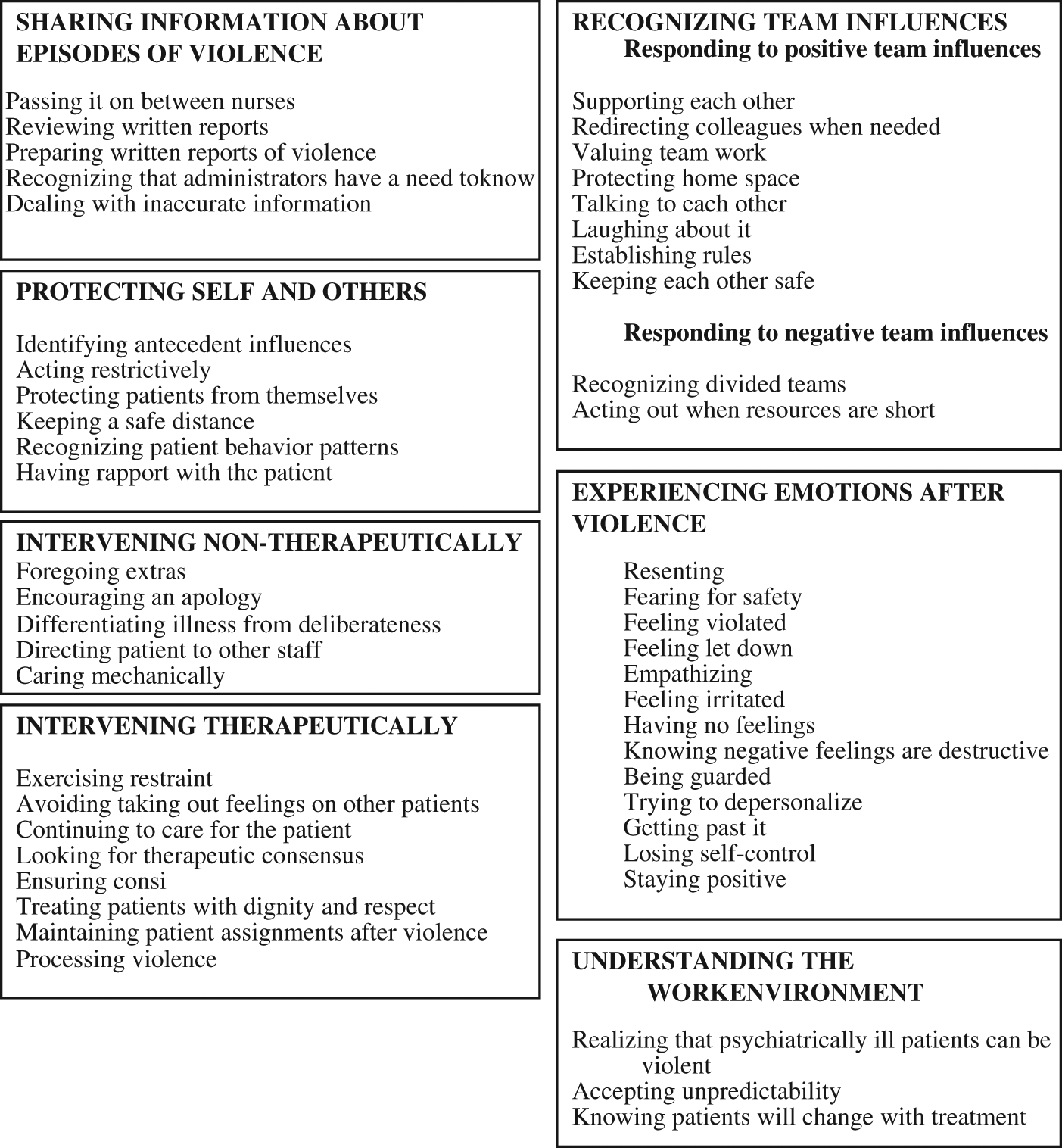
Major themes (capitalized) and themes
Sharing Information About Violence
Participants shared information about episodes of violence using a variety of communication strategies. They passed information to staff colleagues during shift report and commented that information “spreads fast” and the verbal sharing is perceived as more accurate than what is actually volunteered during formal report. “I get my best information from mouth to mouth from my co-workers. What they say on report sometimes has nothing to do with what actually happened.” Staff valued the opportunity for personal interaction with incoming shift team members. “The nursing report is good, but it is also good to have some type of interaction with the shift that is relieving you.”
Staff reviewed written reports and was particularly concerned about the accuracy of admission paperwork to appropriately prepare for the possibility of violence. “When the paperwork comes upstairs, you have to read it thoroughly to see what the past history is; to see if the patient has previously assaulted anybody or any other incidents like that.” The participants expected colleagues to accurately document details of violent events.
“We say exactly what the patient did. You know, they scratched this person or acted a certain way.” Written reports included incident reports and notes in the chart. When information was inaccurate, staff was concerned. As a consequence of misinformation, participants felt inadequately prepared to address patient circumstances. “A lot of times you will get report that somebody is just not taking their prescribed medications so are a little angry but when we get the patient on the unit, the patient is combat-ready!” Had staff received accurate information, they would “have treated the whole patient situation differently.”
Participants recognized that administrators need to know about occasions of violence and would often “telephone the nurse manager at home” or “call the supervisor.” Some used e-mail correspondence to tell the “boss about situations.”
Protecting Self and Others
Staff described the importance of protecting themselves and others by recognizing triggers for violence or minimizing the potential adverse effects of violent encounters. Participants recognized the importance of identifying antecedent influences that increased or created the potential for violence.
I’ve seen patients come in with a hostile attitude, but this often comes from previously experiencing environments so hostile, that they get to believe that “I have to be hostile to keep people off of me” and they bring this way of thinking into the hospital.
Staff often reflected on what violent patients may have been thinking or doing preceding the attack to use strategies to prevent future occasions of violence.
Some participants described staff adoption of a restrictive response to potentially violent patients. These staff described their actions as necessary to prevent violent encounters. Participants noted that preemptive and early limiting was necessary to prevent patient aggression. “Acting upon something immediately saves a whole lot of problems.” “I don’t see where you have to wait until the person hurts somebody before you put them in restraints.” Participants recounted occasions of patient restrictions implemented early to prevent violence. Staff noted that curtailing patient freedoms prevented behaviors from “escalating” to violence.
Following occasions of violence, staff worried about preventing further episodes. “I think the challenge is trying to get the patients not to do it again to themselves, to staff, or to one of their peers. I think the challenge is to try keeping the patient calm enough to get treatment or revise the treatment plan, so that he or she handles aggression in a different way instead of lashing out at themselves.” Staff wondered how violence could have been avoided. “I always wonder how we could have avoided it.”
Participants commented that staff needed to proactively protect patients and this was difficult since violence was often spontaneous. They believed that female colleagues were sometimes at risk of harm by male patients. “Protecting female colleagues from male patients is important. If there is a female nurse and it’s a male client, then we are going to make sure that the males (staff) are around.” Participants were not accepting of behaviors that were considered sexually deviant or inappropriate.
Staff believed that physical distancing was important to reduce the likelihood of personal injury. “Arm’s length” and “safe distance” were valued when interacting with patients.
You do not want the patient to come too close to you because you’re thinking that the patient might do the same thing to you that they did to your peer. So, keep them at arm’s length. Keep a little more distance, just to be on the safe side.
Participants recognized that patients attempted to avoid addressing personal issues by manufacturing conflict with other patients or staff. “The patient’s focus is to find someone with whom to have a problem. They try to create some kind of diversion or some kind of wall to avoid dealing with their issues.” Staff noted that it was difficult to recognize behavior patterns of new or unfamiliar patients. “Some staff trying to diffuse the situation can make the patient more agitated. You have to know your patient.” “We don’t know our new patient and our team approach may not be what is best for this person.” Participants noted that it was important to stay alert and be aware of the surroundings and patient body language.
Staff valued the relationships that they established with patients believing that this rapport contributed to quality outcomes. “When a staff member builds rapport with the patient, the staff member is able to go to this person, perhaps even when the patient is in seclusion, and get them to take their meds as needed. I see that happen a lot.”
A patient was in restraints and came to the unit on a stretcher. As soon as she got off the stretcher, we thought we were going to have to put her in restraints and call the resident because we thought we would need to immediately medicate the patient. A nurse recognized her and the patient remembered the nurse. The patient not only did not need restraints but did not need medication.
Intervening Therapeutically
Participants shared that staff is required to react to violence in ways that may be counter to an impulsive reaction. Staff was challenged to respond to violence in an appropriate, caring form that deterred or limited harm without contributing to the violence, harming the patient, or risking employment. “I guess knowing that you can’t really react like how you might initially want to react it makes it a little more difficult.” At times, a measured response was difficult. “You want to protect yourself, but what is too far and what is not far enough?”
Staff found it necessary to be conscious of responses to violence recognizing that anger influences subsequent interactions with patients, including those who were involved in the violence and also those who were not involved. “Two minutes later you might have the nicest patient on the unit come to you for something and you don’t want to bite their head off.” Staff shared that when violence was directed at coworkers, it was difficult to not feel anger and this anger could influence subsequent communications.
Participants identified a continuing obligation to provide care for a patient even though the patient initiated or participated in violence directed toward staff or patients. “I didn’t give it a second thought to ask him if he needed anything, if he needed help.” Participants were challenged to develop a consensus-based plan of care for patients. “I think the biggest challenge for me is to come to a consensus on what to do for the patient since there are often so many different care providers involved in the patient’s plan.” Reaching consensus was particularly important when developing a strategy to address patients who had interacted in a violent fashion during inpatient hospitalization.
Participants recognized that consistency was required when working with patients to ensure appropriate limits and support the therapeutic plan, particularly following violence. A consistent approach to consequences of behavior was viewed as very important.
Depending on what the consequences were for the patient during the prior shift, it is important to continue the same process into the next shift to make sure that whatever the disciplinary action or whatever the consequences, they are followed through throughout the whole shift or throughout the required consequence time.
Inconsistency was identified as contributing to an increased likelihood of problems.
Sometimes patients try to manipulate the staff and try to get their way because they try to test what you know, what you don’t know, how far they can go, and how far they can’t go. If you don’t know all the pieces in the plan, that may create problems with the staff and the patients because you’re not following the plan all the way through.”
Participants recognized that it is important to treat patients appropriately following an episode of violence. “We want them to get the respect and dignity they deserve.” Respectful interaction was an expectation although participants identified that self-protection was also an appropriate concern. “There’s nothing you can do but try to protect yourself at the same time that you are helping the patient. It’s hard sometimes.”
Participants expected professional behavior from their colleagues and from themselves. “I think we have to deal with violent patients just as well as we do with calm patients. You have to be professional at all times with the patients.” One aspect of professional behavior was to remain objective and to give patients the benefit of doubt.
I try to give everybody a clean slate when I’m working with them. Sometimes the patients who have been violent in the past do not behave that way during their hospitalization. The patients that have not been known to be violent are sometimes the ones that have violent outbursts.
Staff believed that it was important to maintain patient care staff assignments whether or not violence had occurred. “We would not reassign a person to a different area because of an incident. Only if a staff member expressed particular concern would assignments be reconsidered.”
Participants shared that it was difficult to process violent encounters but that such processing was necessary to maintain a therapeutic milieu. Staff realized that there was a risk of turning an angry response to violence into behaviors that could be damaging to patients. Sometimes, it is hard to separate it when you see one of your “family members” get hurt. It takes a certain level of patience, compassion, and understanding when dealing with the patient to process correctly because you could feel angry with them for hurting one of your “family.”
Participants acknowledged that they were sometimes challenged by the care demands of patients who had assaulted other patients or staff members. In response to these violent encounters, staff made conscious decisions about how much to do for patients or how closely to engage with patients depending on how staff judged the nature of the violence demonstrated by these patients. At times, staff met basic care requirements and did not intervene beyond this point. Participants recognized that they distanced themselves from some violent patients. “I distance myself. I have a tendency to want to; I will give the care that is expected. I will do what’s necessary to be done. Will I go overboard? Will I do the above and beyond? No.”
Participants regarded wounded colleagues as “family” and were unwilling to engage with perpetrators beyond the extent required for care deemed as necessary. Staff noted that providing care “above and beyond” expectations was the established norm in inpatient units, so care that did not include the “extras” was considered “bare minimum.”
Participants encouraged patients to apologize following episodes of violence. Staff commented that patients should not be permitted to believe that they can interact in violent ways by “doing some really bad stuff” and then “come up and be friendly afterwards.”
Participants made evaluative decisions as to whether violent behaviors were the result of “mental illness,” “manipulative stuff,” or deliberate decision making. Participants expressed concern that patients saw staff as available targets because staff could not retaliate, whereas patients could retaliate against each other if so desired. “The things that some violent patients would say or do to a staff member, they definitely would never try with another patient.”
Participants believed that some patients would likely never change. Some participants diagnosed patients as either deliberately violent or violent as a result of illness. “It depends whether or not the patient is really psychotic.” “Unfortunately, there are people who know how to use the system and they take advantage of the system. You know that because you see it in their personality and the way they interact and the way they manipulate everything.” Participants labeled patients based on their personal evaluation of the patients’ circumstances, behaviors, and histories and within the context of the participants’ previous experiences. “Honestly, some people should be in jail, rather than in psychiatric hospital.” Some participants believed that mentally ill patients were not responsible for violent actions if “god didn’t bless them with good mental health.”
Participants made a distinction between violent behaviors based on the perceived intentionality of the action. “I think in certain cases, there are two types of patients; there are patients that are really psychotic and have no reasoning over the harm they inflict and there are patients who know exactly what they are doing.” Patients labeled as “psychotic” elicited more empathy following violence than those considered “manipulative and physically aggressive.” Violence emanating from patients labeled as “deliberate” felt more “criminal” to the participants. “It’s more of a criminal act than a mental illness act, and it feels criminal.” “If you feel that the person is just a really mean, evil person, it has a whole different feeling.”
Participants were more inclined to be empathetic following violence if the patient demonstrated behaviors consistent with remorse. Some participants considered the perceived “motives” of violent patients when determining whether or not empathy was appropriate.
At times, participants were able to discern when colleagues needed a “break” from particular patients. “My colleagues don’t need to say anything; I can just see it in their faces.” “They get burned by these violent patients.” Participants respected their colleagues’ need for occasional disengagement from specific patients following a violent encounter. “Somebody else will pick up the slack or pick up the one to one or whatever else has to be because you need that down time.”
Participants noted that they were required to care for patients regardless of unpleasant or violent behaviors. They viewed this care expectation as a demand of the job. “You have to take care of the patients regardless.” At times, this care was provided in a perfunctory fashion. “I will give you your medications and if you have a dressing change, I will do it. I’m your nurse and that’s my responsibility.” Participants recognized that these things were expected to avoid negative feelings regarding patients. “You can’t walk around with negative feelings for the patient, because if not for the patients, what would we be doing?”
Feeling Influenced by the Team
Participants valued the positive effect of the team on the work environment and on the dynamics of the clinical setting. They supported each other and valued the team. Staff shared that the team support made the work environment “more comfortable” and “safe.” Constant checking-in and “having each other’s back” provided participants with the security of a “comfort zone.”
Staff acknowledged that there were times when staff members needed to redirect colleagues, particularly when observing colleagues “over responding” or “getting in too deep.” Staff shared that stressful situations could trigger an “overzealous employee response” that required modification. “Sometimes you can find yourself getting into a power struggle with patients. You can get caught up in it.” Colleagues intervened by “de-escalating” the situation and encouraging colleagues to “take a deep breath” or “step off the unit for a bit.” Participants noted that redirecting was not often required but when it was needed, it was valued.
Participants believed that team work is important, “probably the most important.” The BHAs and RNs expressed a need to work in partnership “like a well-oiled machine.” Staff observed that patients received adequate treatment only when team members were able to work well together. As a result, participants commented that “things get done and we have fun on the unit.” The staff evaluated team work as less than ideal when the team was “chaotic and out of control.” In this circumstance, participants observed that patients could feel intimidated by team members.
Although team members were important to participants, staff members also valued their home lives and were careful to separate work from home. “When I’m home, I don’t want to know what’s going on up here. When I come in I can find out.” Participants did not consider themselves so critical to operations that they needed to be contacted at home when violent events occurred. With experience, staff learned to leave work “at the door.”
Participants valued the opportunity to share their concerns and life experiences with colleagues. Communication was identified as an important aspect of team work. When staff was injured as a result of violent encounters at work, it was important for the victim to have the opportunity to “get reassurance” so that “you know that your team is going to be there for you.” As a result of this open, supportive communication, staff sometimes shared personal information.
Participants commented that laughing about the stressors at work, including minor issues related to violence, was the way that “everybody deals with it.” “You have to decompress; let the frustration out. When you’re telling the story, everybody puts their own spin on it and throws a joke or jab.” Humor was a way to handle the “bad stuff.”
Staff believed that unit rules and guidelines were important to reduce risk. “We have certain rules and guidelines, like you can’t hang at the nurses’ station, no patient can.” When rules and “directions” were changed by physicians, “it is difficult because it affects the team.” Rules were also important when using physical restraints during violent interactions. “If it’s an official violent episode, the patient normally goes into restraints, and the doctor is called immediately, has to write the restraint order, and the procedure begins.”
Participants kept each other safe from violence by watching patient behaviors and “keeping an eye” on colleagues who may be at risk.
I have been in a situation during which I am dealing with a verbally aggressive and hostile patient at one end of the hall and I don’t think anybody is watching. I deal with it and turn around to see that someone has been watching me, and that makes me feel better.
At times, staff needs to point out colleagues’ behaviors that increase the likelihood of a violent encounter.
One of the nurses went into the storage room where we keep the patients’ belongings and that door closes automatically. It does not stay open. I did not know the nurse was in there and no one else did either, but when I saw this nurse and a patient come out together, I said “don’t you ever do that again or let someone know where you are and what you’re about to do.”
Participants were occasionally influenced in negative ways by dysfunctional team dynamics. They recognized when teams were not unified. “There is a difference in the response when you have a team that works together versus a team that is not unified.” Lack of unity contributed to dysfunction. Divided teams caused “a lot of tension.”
Experiencing the Aftermath of Violence
Staff was concerned when resources were perceived as inadequate. On these occasions, “patients know that the staff is weak and patients subsequently act out more.” Similarly, participants observed that an all-female staffing pattern seemed to encourage more patient aggression.
Participants experienced varied emotional responses to assault behaviors directed by patients toward victims that included the participant himself or herself, staff comrade, or other patients.
They occasionally resented violent patients, particularly after working hard to role model and teach alternative behaviors to violence.
You taught them every type of behavior they could do other than being assaultive. I become really frustrated and I almost need a cool out time, because I just don’t even want to have to deal with them anymore. It’s like, they have taken up so much of your time and energy and you have thought that you have changed them in a way and then this happens and then, it’s back at square one.
Participants acknowledged the frustration but recognized the importance of “getting past it.”
Staff was fearful of possible injury. Care providers worried about the “safety of the environment.” Episodes of violence reminded staff that “people can be hurt” by patients. Following violence, participants described “getting ready for work with a lump in my stomach.” They would consider “what am I going to see today? It is very anxiety producing.” They viewed their reactions to a violent assault as “normal” and “scary.” Some remembered particularly violent assaults for years following the event. “For years I’ve looked around in that room and visualized the blood. It was very traumatic because this was a girl, who came in to do a job, who just walked in front of someone at the wrong time.”
Participants believed that their fear could not be displayed to patients. “You can never really show how scared you are in a situation when because once you do that, you have let them win. It’s a fine line, a game.” Participants saw this “game” as similar to “the real world.” At times, violence was so unanticipated that it increased participant fear. “We don’t come to work expecting to be punched in the face out of nowhere. Generally, you expect other certain things to happen before it escalates to that point and bam, that’s a scary thing.”
Participants felt violated by violent patients. They were upset and felt “cut to the core.” They recognized that some violence was the result of illness but were still angry.
I know that it was not intentional and that she did not mean to kick me in the process of this but I was angry because she didn’t think about what she was doing and the consequence was that I was hurt.
Participants felt “let down over and over again.” They shared that patients “agreed they would not do this” and “contracted to avoid violent behaviors” and then would “turn on you personally.” Staff was disappointed by patients who used violence. “I was bringing in books and crayons and working with her, and she put me out of work for six weeks.” At times, participants questioned whether or not they were making a difference
While participants empathized with patients and wondered what could have been done differently to prevent a violent outburst, they simultaneously felt badly for the assaulted staff member. Participants recounted stories of colleagues who had been hurt by patients. “My empathy went to the person who was hurt, not the person that was actually doing the hurting.” Staff was traumatized by their colleagues’ blood and wondered “is she okay? What can I do to make it better or to help her?”
Staff members occasionally found patients irritating and “working your nerves.” There were some patients whose discharge the staff eagerly anticipated. Participants commented that they felt “emotionally drained” when seeing very little “change in some patients.” Some participants did “not feel” following violence and “felt numb.”
Coping Strategies
Participants described strategies used to cope with violence in the work setting. They realized that negative feelings are self-destructive and so tried to avoid “holding grudges.” “If you harbor those negative feelings and resentments, you are doing a disservice to not only the patients but to your co-workers as well.” Participants’ advised that negative feelings negatively influenced job performance, so it was important to address these issues.
Staff became “guarded” during interactions with patients, although participants recognized that this guarded stance was not therapeutically ideal. Participants coped by depersonalizing the assaults but recognized that it was difficult to respond with the objectivity that was required. “One of the challenges is to try to depersonalize the incident.” Staff attempted to prioritize the needs of ill patients over their need to respond to personal trauma following violence. “Your mind really needs to be focused on depersonalizing the situation and dealing with the sick patient. Sometimes it’s hard to deal with that.”
Participants were pleased with themselves when they were able to avoid judging and depersonalize the violent attack. “After I got sent to the Emergency Department because of the incident, the next day I saw the patient, I didn’t take it personally.” Staff tried to avoid judging violent patients following an assault.
I don’t really judge people because I know the field I am in and I know that people are up against a lot in their life. Maybe I remind them of someone in their life who has done something wrong to them. Sometimes you have to take yourself out of the situation. It doesn’t have anything to do with you a lot of the time.
Participants believed that it was important for staff to “get past it” following episodes of violence. They recounted that “getting over the fear” and “moving on” were critically important perspectives. Staff noted that it was important to “find it within” to “get the job done.” Participants shared that there are times when self-control is lost. Staff shared occasions of verbal retaliation in response to episodes of violent assault. At times, participants were overwhelmed by emotions. “I have gone in the med room, closed the door and cried. Nobody knows I’m in there crying. I will vent and let go of stuff.”
Some coped by staying positive and focusing on the “rewards.” They noted that “there are a lot of rewards that come your way when caring for people with mental illness.” Participants believed that the rewards outnumbered the “drawbacks.” Participants understood the unique nature of their chosen work environment. They appreciated the challenges and rewards associated with practicing in a psychiatric setting.
Participants were mindful of the risk of violence inherent in their jobs. They were firm in the belief that staff “do not come to work to get hurt” but recognized that “violence can happen at any time.” They sensed that violence “cannot really be stopped. It is unfortunate.”
Staff learned to accept that patients’ behaviors were unpredictable. “Any patient at any second can just flip out.” Every work day was viewed as potentially different from previous work days. Patient behaviors were “uncalled for” and “sudden.” The unpredictability influenced staff members’ vigilance.
Patients can sense when something is going on or when a team may be focused on their behavior. You don’t treat them any differently, you still treat them like the other patients, but still in the back of your mind, you’re thinking, “is he or she going to try to scratch my face if I don’t give them coffee?”
Participants believed that staff members were “safe” targets for assaults because patients know that staff will not retaliate. Participants observed that so many patients have impulse control problems but know not to “threaten another patient who might be bigger or more out of control. But, they are safe threatening staff” particularly because “in the past, they have threatened and nothing happened” as a result of the behavior.
Participants understood that patients would change with treatment, particularly with medications. Participants were interested in watching patients transform with therapy. “It’s really interesting to watch the transformation that results when they are being treated well or not being badgered.” Participants appreciated when initially hostile patients were ready for discharge because “some of the most hostile, irritable, and angry ones saying ‘thank you’ and ‘giving you a hug or handshake’ when it is time to leave. Wow!”
Essential Structure
RNs and BHAs recounted personal experiences of patient-directed violence and the influence of these encounters on individual, team, and environmental dynamics. Commitment to protecting and supporting patients, often including those who were the aggressors, colleagues, and self, was central to the group discussions. Critical anecdotes revealed concern with workplace safety as well as a prevailing and consistent belief in the importance of remaining professional and avoiding potential negative or destructive interactions with patients. Participants expressed distress when personal, individual, and team behaviors were “less than” that expected of consummate professionals. At the same time, participants’ comments reflected a serious concern about the well-being and safety of self, colleagues, and patients potentially caught in the fray of violent encounters, particularly those without predictability.
Discussion
Findings suggest that RNs and BHAs found informal communications with colleagues to be more valuable than written ways of disseminating reports of violence or communications related to potentially violent patient encounters. This valuing of the interaction between employees signifies a sharing that is more than just a passing of information. It is this relating of experiences that contributes to the development of relationships. This is consistent with the findings by Yonge (2008) that the informal nature of psychiatric nursing report allows for team building and for staff to come to terms with their frustrations.
Many positive ways to protect self and others were described, including identifying antecedent influences, recognizing patient behavior patterns, staying alert, keeping a safe distance, and having a therapeutic relationship with the patient. These measures are all consistent with Watson’s (2008) theory of human caring, which recognizes creating a healing environment and the development of helping trusting relationships.
Nurses and BHAs described occasions of acting restrictively in response to patients’ violent or potential violent behavior. Caution needs to be taken when weighing safety for the patient and nursing staff with the patients’ right to a least restrictive setting. Restraint use as a strategy for deterring the potential for violence is inconsistent with hospitals’ and accreditation agencies’ policies. Underlying possibly restrictive action may be fears for safety; however, it is important to ascertain whether or not restrictive behaviors reflect a philosophy of nursing practice that validates such interventions. In this event, staff education and support is warranted to encourage alternate strategies for reducing the likelihood of workplace violence.
Possible strategies for enhancing patient and staff safety and supporting a therapeutic milieu include (a) event debriefing to provide a forum for staff to confer and discuss feelings about the incident and (b) postincident review to decrease the psychological impact of violence for staff (Bonner & Wellman, 2010). Nursing leadership may need to evaluate if reassignment of staff to another unit is appropriate or if reassignment of the patient is needed for the patient to receive treatment without bias.
In some cases, a referral for a member of the nursing staff to employee assistance may be warranted for the distress experienced after an episode of patient violence. Past research shows that nursing staff often do not seek professional help, even when having psychological symptoms related to physical violence by a patient (Nolan et al., 1999; Yarovitsky & Tabak, 2009).
Repeated exposure to violence may desensitize RNs and BHAs to the effects of violence. Desensitization could distort the perception and self-evaluation of nurses and BHAs to subsequent alterations in patient care. A formal process of seeking feedback may be necessary for nursing staff who regularly encounter patient violence.
The nursing staff is composed of licensed RNs and BHAs with varying levels of education. Judgments and assessments were made by all these staff regarding the intentions of the violent patients. Participants felt comfortable making these assessments based on the presence and absence of symptoms. These assessments were often based on a “feeling” rather than education, theory, or current evidence. Providing continuing education regarding psychiatric illness related to theories of violence would increase the knowledge base and provide a framework to make assessments based on scientific evidence, rather than affective responses.
Optimistic caring practices were identified for the continuing treatment of patients after violent episodes. Some cognitive processes that RNs and BHAs identified included “realizing psychiatrically ill patients can be violent” and “knowing that the patient will change with treatment.” Other encouraging key themes regarding continuing to care for violent patients included, “professionalism” and “treating patients with dignity and respect.” Realizing the challenging nature of treating patients after violence, the efforts of nursing leadership should seek to encourage these qualities by recognizing and reinforcing the acts of RNs and BHAs who demonstrate them.
There were themes that presented areas in which RNs and BHAs were not able to provide care to patients in an empathetic manner following an episode of violence. RNs and BHAs at times consciously decided to provide requisite care at a basic level. At times, staff withheld empathy. Care encounters without empathy prevents authentic engagement and adversely influences the development of relationships with patients and a sense of fulfillment in work. An environment in which caring practices are taught, encouraged, and role-molded may help transform the environment. Watson (2008) stated, “Nurses often become pained and worn down by trying to always care, give, and be there for others without attending to the loving care needed for self” (p. 47).
Limitations
A limitation of this study is the inability to generalize findings, given the small and convenience sample. The number of RN participants (n = 8) was particularly low when compared with the BHAs (n = 11), and the known level of educational preparation was largely less than an earned baccalaureate degree. Focus groups were orchestrated within one particular health care network, further limiting the generalizability of findings; however, we recognize that qualitative research is not generalizable in ways comparable to a positivistic approach. The discussions required reflection and sharing specific topics that were highly sensitive. Although participants were assured of confidentiality, it is possible that participants were cautious in their responses with a negative effect on the veracity of the data.
Conclusions and Implications
Findings suggest that there is a need for methodical attention to staff education and debriefing. Staff struggle with differentiating between perceived deliberate acts of violence related to established patterns of behavior and ingrained responses versus violence perceived as secondary to psychiatric illness. Staff judgments influence the patient–staff interactions that affect the milieu and so should be appropriately informed and clinically accurate.
Violent encounters are identified by behavioral health nurses and staff as likely risks inherent in clinical settings that provide services to patients challenged by mental illness. The University of Iowa Injury Prevention Research Center (2001) has provided a violence typology that may be useful for facilitating violence reporting and supporting research and policy development. Participants did not offer a comprehensive sense of the incidence of violence by shift, day, unit, diagnosis, staffing pattern, or other quantifiable parameter. A system for tracking reported occasions of violence could be important to institutional efforts to reduce frequency of violent encounters in health care settings, including behavioral mental health facilities. Tracked data could provide opportunity for determining the effectiveness of interventions related to a decrease in episodes of violence on inpatient psychiatric units.
Contributing to the problem of designing strategies for violence reduction may be the tendency for nurses to excuse patient behaviors as the unalterable effect of mental illness. Ferns and Chojnacka (2005) suggest that nurses need to begin putting themselves first rather than patients so as to change the status quo perspective that violence is part of the job. Staff may be conditioned to expect violence and to carry on in the face of violence by providing the care, attention, and services required by patients. This expectation was revealed in the study findings.
It may be that an articulated policy of nonviolence could be helpful to assist staff in communicating behavioral expectations to patients and family. It is possible to view all occasions of violence as reportable and unacceptable; however, the management of the situation would vary depending on the event and its circumstances. Collecting these data and compiling it into an aggregate form would allow for intervention studies and benchmarking to ascertain whether or not implemented interventions are effective.
Footnotes
Patti Rager Zuzelo is a co-principal investigator. She directed the research study, coached focus group techniques, and led data analysis. Zuzelo finalized the manuscript and wrote the methods and findings sections. Staci Silver Curran is a co-principal investigator. She led authorship of the introduction and background while contributing to the conclusions and implications. Curran collected focus group data, contributed to data analysis, and developed the conclusions and implications. Mary Ann Zeserman collected focus group data, contributed to data analysis, and contributed to the conclusions and implications.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Einstein Healthcare Network and Albert Einstein Society.