
Abstract
Introduction
Breast cancer is the most common cancer among women. Due to advances in treatments, breast cancer survivors are one of the largest groups (22%) of the approximately 13.7 million cancer survivors in the United States (American Cancer Society, 2012). Cancer survivors’ quality of life (QOL) and their psychological adjustment are important outcomes (Hewitt, Herdman, & Holland, 2004), and identifying their determinants is crucial for program development and survivorship care. Women with a sexual minority orientation, defined as reporting a lesbian or bisexual self-identity or reporting a preference for or having a female partner, are thought to be overrepresented among breast cancer survivors, in that lesbians have more risk factors than heterosexual women for breast cancer (Brown & Tracy, 2008). For example, there is consistent evidence for lesbians’ greater rate of obesity, one of the risk factors for breast cancer (Aaron et al., 2001; Boehmer & Bowen, 2009; Boehmer, Bowen, & Bauer, 2007; Case et al., 2004; Cochran et al., 2001; Dibble, Roberts, Robertson, & Paul, 2002; Valanis et al., 2000).
To date, a number of studies have compared breast cancer survivorship by sexual orientation, concluding that QOL, anxiety, and depression do not significantly differ by sexual orientation. Rather, sexual minority and heterosexual survivors of breast cancer reported mostly good QOL and low psychological morbidity (Arena et al., 2006; Boehmer, Glickman, Milton, & Winter, 2012; Boehmer, Glickman, & Winter, 2012; Fobair et al., 2001). Although studies that assess differences between heterosexual and sexual minority women with respect to their psychological adjustment after breast cancer are important, it is likely that sexual minority women’s adjustment after breast cancer is affected by issues unique to their sexual minority status. The minority stress model postulates that sexual minorities are exposed to chronic stress due to their sexual minority status, which has been linked to adverse mental health outcomes (Meyer, 2003). Thus, sexual minority–specific experiences, consisting of expectation of rejection, concealing one’s sexual orientation, and internalized homophobia, may also be linked to lesbians’ and bisexuals’ adjustment after breast cancer. Only few studies examined these sexual minority–specific issues and their links with adjustment after breast cancer (Boehmer, Linde, & Freund, 2005; McGregor et al., 2001). One study of lesbians with breast cancer linked internalized homophobia to greater distress (McGregor et al., 2001) but did not include bisexual women in the sample. Another study concluded the amounts of time identifying as sexual minority and disclosure of sexual orientation were unrelated to coping and lower distress (Boehmer et al., 2005). However, self-identified lesbians and bisexuals used less maladaptive coping compared with women who reported partnering with women but did not self-identify as lesbian or bisexual. In addition, within the noncancer population, a number of studies point to particular demographic differences between bisexual and lesbian women. Lesbians are almost universally with a same-sex partner and about half live with their partner, whereas 90% of bisexual women report an opposite-sex partner and only a small percentage live with their partner (Herek, Norton, Allen, & Sims, 2010). Furthermore, compared to bisexual women, lesbians more strongly identify as a sexual minority; are more closely linked to the lesbian, gay, bisexual (LGB) community; and are more likely to disclose their sexual orientation (Herek et al., 2010). Others point to differences in minority stressors between lesbian and bisexual women (Ebin, 2012). In addition, increasingly studies suggest that bisexual women have worse health outcomes than lesbian women, including worse mental and physical health (Bostwick, Boyd, Hughes, & McCabe, 2010; Cochran & Mays, 2009; Conron, Mimiaga, & Landers, 2010; Ebin, 2012; Fredriksen-Goldsen, Kim, Barkan, Balsam, & Mincer, 2010; Steele, Ross, Dobinson, Veldhuizen, & Tinmouth, 2009). Given these prior studies’ findings, this study’s purpose was twofold. First, we compared the QOL and adjustment of lesbian and bisexual breast cancer survivors. Second, we examined whether unique sexual minority–specific issues contribute to lesbian and bisexual survivors’ adjustment.
Method
The institutional review boards of Boston University and the Massachusetts Department of Public Health approved all aspects of this study.
Recruitment
The sample for this study was recruited for a larger study of breast cancer survivors, which had the focus of comparing heterosexual to sexual minority women; the latter was a group that combined lesbians, bisexuals, and women with a same-sex partner or a same-sex partner preference. Using 2000-2005 data from the Massachusetts Cancer Registry, we recruited heterosexual and sexual minority women survivors, with primary diagnoses of DCIS (ductal carcinoma in situ) or I-III breast cancer (Boehmer, Clark, Timm, Sullivan, & Glickman, 2011; Boehmer et al., 2010). After we had obtained passive physician consent, survivors were mailed an invitation letter and a consent form. Then, we made up to 10 attempts, including three voice mail messages, to screen survivors for eligibility over the telephone. During the 5-minute telephone screening, we asked questions about cancer history to exclude ineligible survivors and asked about survivors’ sexual orientation, inquiring about sexual identity and preference for sex of partner. Eligible participants verbally consented and then completed a 35-minute telephone survey. To increase the number of sexual minority women, we used convenience-based recruitment methods to supplement the sample of survivors (Boehmer et al., 2011). This convenience sample fit the same eligibility criteria: primary nonmetastatic, nonrecurrent breast cancer, diagnosed in the years 2000 to 2005, and not currently undergoing active cancer treatment. However, the convenience sample was geographically unrestricted, resulting in sexual minority women who were mostly living outside of Massachusetts (Boehmer et al., 2011). Because of the current study’s aims, to compare lesbian and bisexual women and to link sexual minority–specific aspects to QOL and adjustment, we retained only the 180 lesbian- or bisexual-identified survivors, excluding 258 survivors, who self-identified as heterosexual or other.
Measures
We obtained from the Massachusetts Cancer Registry the stage, date of diagnosis, and date of birth, from which we calculated age at interview. All other data, including age, stage, and diagnosis date for the convenience sample, were collected during a 35-minute telephone interview.
Demographic Data: These consisted of race, marital status, education, employment, and health insurance. We ascertained individual income during the interview, and we derived two measures of neighborhood socioeconomic status from participants’ addresses. Using Census 2000 data, we obtained (a) poverty level, the percentage of the population in a census block living under the Federal Poverty Level, and (2) the census block’s median household income.
Clinical and Functional Measures: These included time since diagnosis, calculated from the diagnosis date to the interview date. Survivors reported their cancer treatments, from which we derived measures of surgery, radiation, chemotherapy, and receipt of tamoxifen or aromatase inhibitor therapy. Survivor comorbidities were captured using a comorbidity measure developed by Ganz et al. (2002). From participants’ self-reported medication use, we determined if survivors were currently on antianxiety, antidepressant, antipsychotic, or mood stabilizer medications. From participants’ weight and height, we derived the body mass index. We used the breast cancer module of the EORTC Quality of Life Questionnaire, QLQ-BR23 (Aaronson et al., 1993; Fayers et al., 2001) to assess systemic therapy side effects, arm symptoms, body image, sexual functioning, sexual enjoyment, hair loss, and future perspective. In this sample, scores on all subscales of the QLQ-BR23 had acceptable or high internal consistency reliability estimates: systemic side effects (α = .67), arm symptoms (α = .75), body image (α = .79), and sexual functioning (α = .83).
Psychosocial Factors: Survivors’ perception of their physician was assessed using the Trust in Physician Scale (Anderson & Dedrick, 1990), which had high internal consistency in this sample (α = .89). We measured social support using a six-item short form of the Interpersonal Support Evaluation List (Arena et al., 2006; Cohen & Hoberman, 1983; McGregor et al., 2001), which also had high internal consistency (α = .83). We determined survivors’ spouse/partner status, living arrangement, ever having attended a cancer-related support group, and ever having sought mental health counseling to deal with breast cancer.
Coping: This was measured using the Mini-MAC, an abbreviated version of the Mental Adjustment to Cancer scale (Watson et al., 1994), which entails five coping styles: fighting spirit, hopelessness, anxious preoccupation, fatalism, and cognitive avoidance. Scores on all subscales had internal consistency reliability estimates that raged from acceptable to high: fighting spirit (α = .53), hopelessness (α = .92), anxious preoccupation (α = .85), fatalism (α = .53), and cognitive avoidance (α = .77). We used the Benefit Finding Scale to measure positive perceptions of the breast cancer diagnosis (Antoni et al., 2001), which had high internal consistency (α = .95).
Sexual Minority Factors: We built on a previously used measure of discrimination (Krieger, 1990; Stuber, Galea, Ahern, Blaney, & Fuller, 2003) that asked participants if they ever felt discriminated against because of their age, race or ethnicity, gender, sexual orientation, appearance, income level, or having cancer. Reports of discrimination were summarized as a score, which had good internal consistency (α = .65). We also categorized discrimination experiences into none, sexual orientation discrimination only, nonsexual orientation only, and both types of discrimination. We used an index to capture the years of having a lesbian or gay identity (Mohr & Fassinger, 2000) and the Outness Inventory to capture the types of persons to which an individual had disclosed her sexual orientation (Mohr & Fassinger, 2000). The Outness scale had an internal consistency of .81. Finally, we used the LGB Identity Scale, which assesses five dimensions of LGB identity, to reflect the degree to which individuals had difficulties related to their sexual orientation. The dimensions are Identity Confusion, Internalized Homonegativity, Need for Privacy, Need for Acceptance, and Difficult Process. Scores on all subscales had acceptable internal consistency reliability estimates: Internalized Homonegativity (α = .69), Need for Privacy (α = .80), Need for Acceptance (α = .74), and Difficult Process (α = .78). The sum of the latter four dimensions generates a summary measure of negative identity (Mohr & Fassinger, 2000), which had high internal consistency (α = .87).
Outcomes: We used the SF-12, an abbreviated version of the widely used Medical Outcomes Study Short-Form Health Survey (SF-36) to measure QOL, summarized into the Physical Component Summary (PCS) and the Mental Component Summary (MCS; Ware, Kosinski, & Keller, 1996). To measure anxiety and depression, we used the Hospital Anxiety and Depression Scale (Zigmond & Snaith, 1983). In this sample, all of our outcomes had acceptable or high internal consistency: SF-12 (α = .90), Anxiety (α = .81), and Depression (α = .79).
Statistical Analysis
We compared lesbian and bisexual survivors on their demographic, clinical, functional characteristics, psychosocial, coping, and sexual minority–specific variables using t tests and chi-square tests to examine differences. Our main analyses involved multiple least squares regressions, as we explain below.
In our overall sample of sexual minority and heterosexual women, several of our predictor variables had missing values. However, with the exception of seven variables, the fraction of missing values was no more than 3%. The seven variables with more substantial amount of missing values were the discrimination score (11% missing), percentage of those living below the poverty level (8% missing), median neighborhood household income (8% missing), trust in physician scale (8% missing), personal income (7% missing), benefit finding (4% missing), and fighting spirit (4% missing). To address the missing values in our analyses, we performed regression imputation by averaging Markov chain Monte Carlo simulations from a multivariate normal model for the data. The categorical/ordinal variables of income, education, marital status, and cancer stage were treated as quantitative, and means of the simulated values were rounded to the closest whole number. The imputation was performed using SAS PROC MI. This strategy was applied only to predictor variables in our regression models, not to the dependent variables. The imputation was performed on the combined sexual minority and heterosexual sample, with the exception of our sexual minority–specific predictor variables; since only sexual minority women responded to these variables, we limited the sample for their imputation to sexual minority women.
We assessed differences in QOL and adjustment by sexual identity using multiple least squares regression models using a stepwise variable selection. Our procedure forced sexual identity into the model and allowing for a stepwise variable selection criterion that excluded and retained predictor variables when the p value was greater or less than .1, respectively. The fit of our final models were summarized with R2 statistics.
Results
With one exception, lesbian and bisexual breast cancer survivors were similar with respect to their demographic, clinical, and functional characteristics, as shown in Table 1. Survivors’ demographic characteristics reflected an average age of 56 years, most were of White race, most were never married or formerly married, the majority was employed, almost all had health insurance, about two thirds had income of $30,000 or more, few resided in high-poverty neighborhoods, and most resided in middle-income neighborhoods. One exception to this demographic similarity was education, in that bisexual survivors were more educated than lesbian survivors. Lesbian and bisexual survivors had also a similar clinical presentation, in that they were 6 years postdiagnosis, most had early-stage disease, the majority had breast-conserving surgery, about two thirds had radiation, about one third to half had chemotherapy, and most had hormone therapy. Most lesbian and bisexual survivors had one or more comorbidities, few were on antianxiety medications, and almost none on mood stabilizer or antipsychotic medications, whereas almost half used antidepressant medications. Lesbian and bisexual survivors were also similar with respect to their body image, sexual function, sexual enjoyment, their future perspective, systemic therapy side effects, arm symptoms, and being upset about hair loss.
Demographic, Clinical, and Functional Characteristics of the Sample.
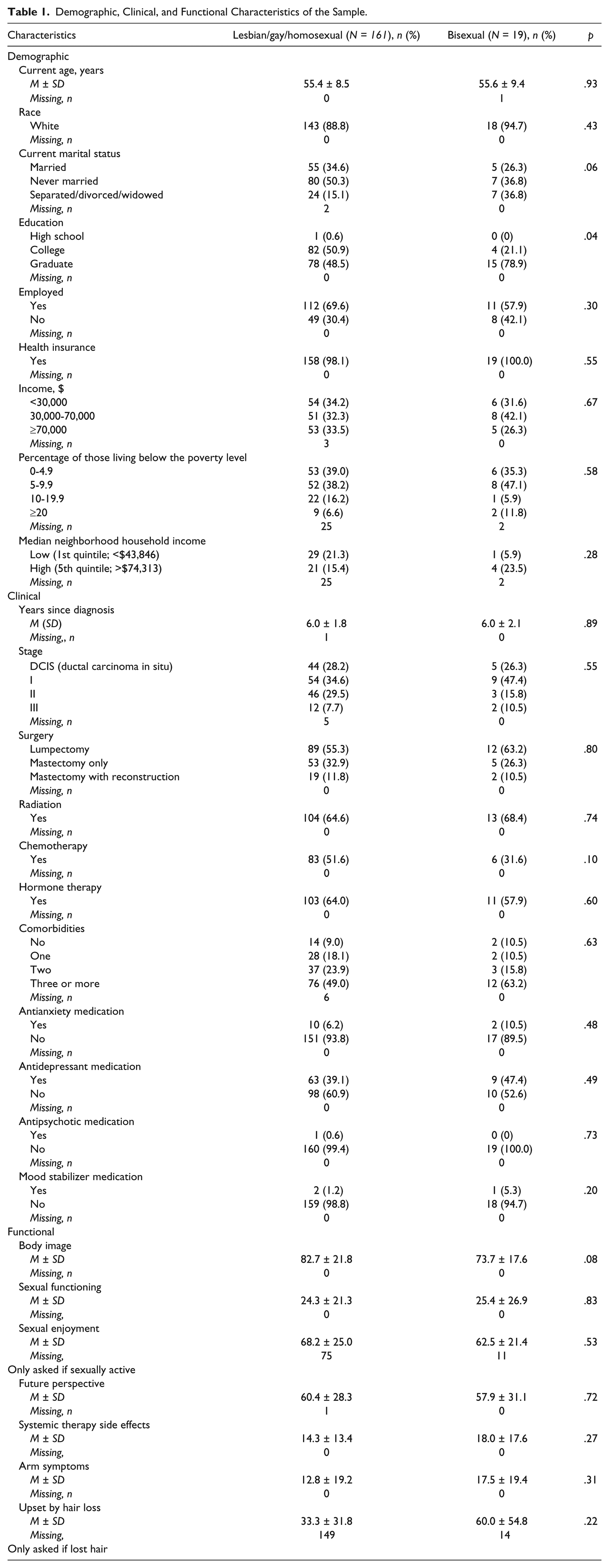
Table 2 describes survivors’ psychosocial, coping, and sexual minority–specific characteristics. Compared to bisexual survivors, lesbian survivors were more likely to trust their physician, be partnered, and living with their partner and were more likely to report exclusively female partners. Lesbian and bisexual survivors were similar with respect to their social support, prevalence of living alone, use of cancer support groups or mental health counseling, and coping styles.
Psychosocial, Coping, and Sexual Minority–Specific Variables.
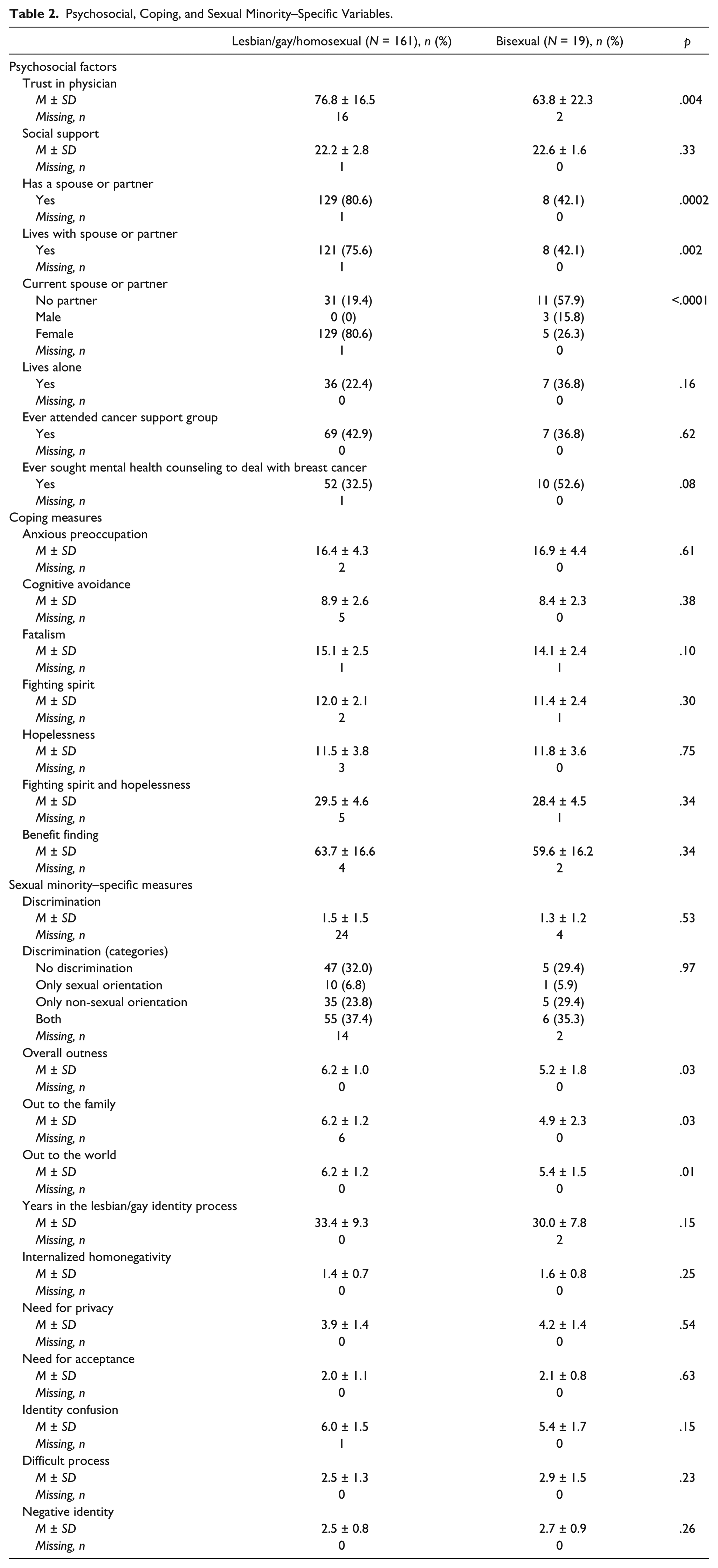
Of the sexual minority–specific characteristics, only disclosure significantly differed by sexual identity, in that lesbians were more open about their sexual orientation with their family, the world, and overall compared to bisexuals. However, survivors were similar with respect to their sexual identity processes and reported similar frequency of discrimination experiences.
We found no evidence of significant differences between lesbian and bisexual survivors on outcomes; rather lesbian and bisexual survivors shared similar physical health: (M = 50.3, SD = 9.8 vs. M = 47.2, SD = 14.9) and mental health-related QOL (M = 51.5, SD = 9.5 vs. M = 47.7, SD = 10.2), depression (M = 3.1, SD = 3.2 vs. M = 3.9, SD = 3.3), and anxiety (M = 5.0, SD = 3.6 vs. M = 5.3 ± 2.5).
Table 3 presents the explanatory factors for breast cancer survivors’ physical health (PCS), which explained 40% of the variance in PCS. Sexual identity had no significant relationship with PCS, indicating no evidence for a difference between bisexual and lesbian survivors in physical health. In addition, none of the sexual minority–specific factors contributed to lesbian and bisexual survivors’ physical health. Better PCS was associated with employment and having a partner, whereas PCS had an inverse relationship with health insurance, comorbidities, systematic side effects, and arm symptoms.
Stepwise Regression Modeling of Physical Component Summary and Sexual Orientation.
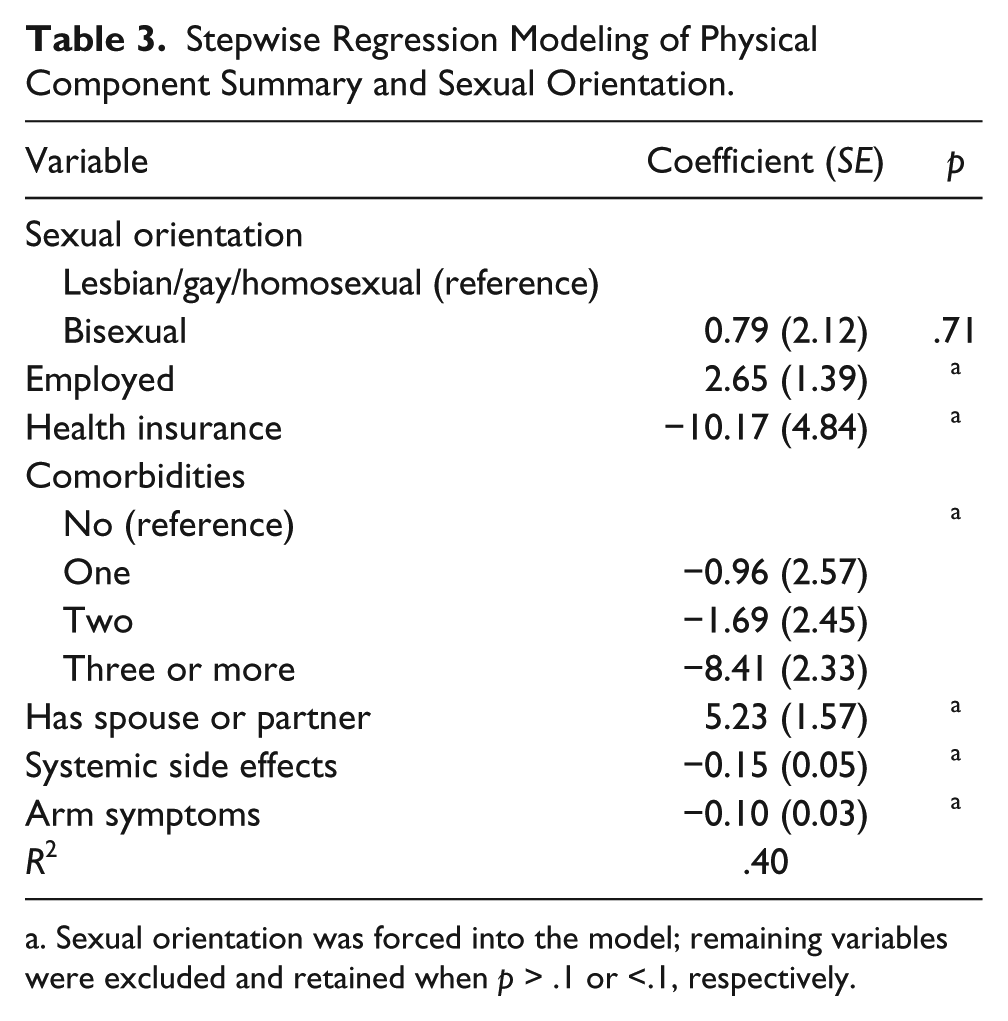
Sexual orientation was forced into the model; remaining variables were excluded and retained when p > .1 or <.1, respectively.
Table 4 presents the explanatory factors for mental health (MCS), which explained 39% of the variance in MCS. Sexual identity had no significant association with MCS, and none of the sexual minority–specific factors contributed toward explaining lesbians and bisexuals’ MCS. Better MCS was associated with earlier stage of disease, more social support, better body image, and positive future perspective. On the other hand, White race, Stage III cancer, having a male partner, and anxious preoccupation coping were associated with worse MCS.
Stepwise Regression Modeling of Mental Component Summary and Sexual Orientation.
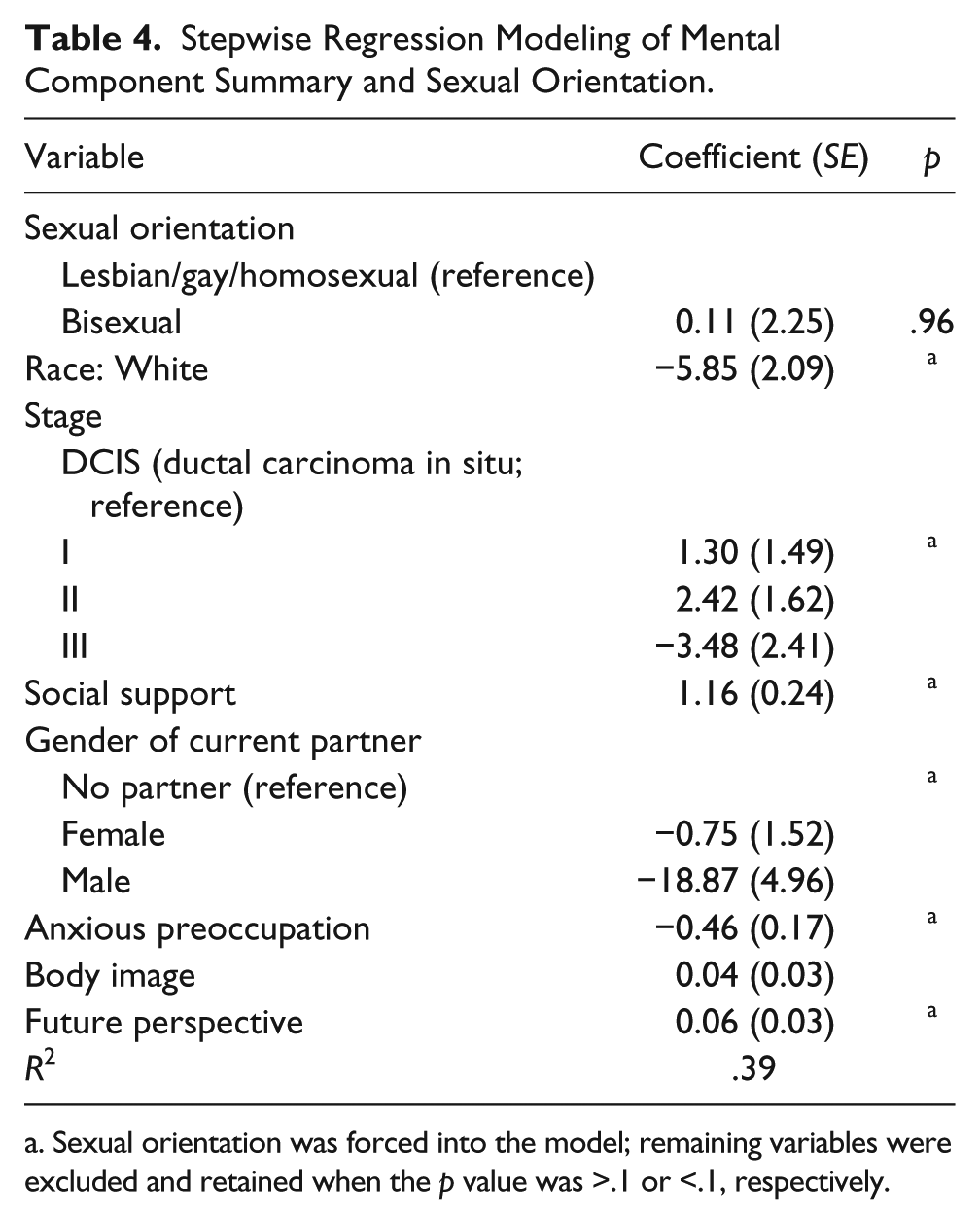
Sexual orientation was forced into the model; remaining variables were excluded and retained when the p value was >.1 or <.1, respectively.
Table 5 presents the explanatory factors for depression, which explained 61% of the variance in depression. There was no significant association between sexual identity and depression. The sexual minority factor “difficult process” made a significant contribution toward explaining lesbians and bisexuals’ depression, even after other indicators had been controlled for. Employment, earlier cancer stage, more social support, more fatalism, or fighting spirit coping, better body image, and better future perspective was associated with lower depression. On the other hand, Stage III cancer, using mood stabilizing medication, and hopelessness coping were associated with more depression symptoms.
Stepwise Regression Modeling of Depression and Sexual Orientation.
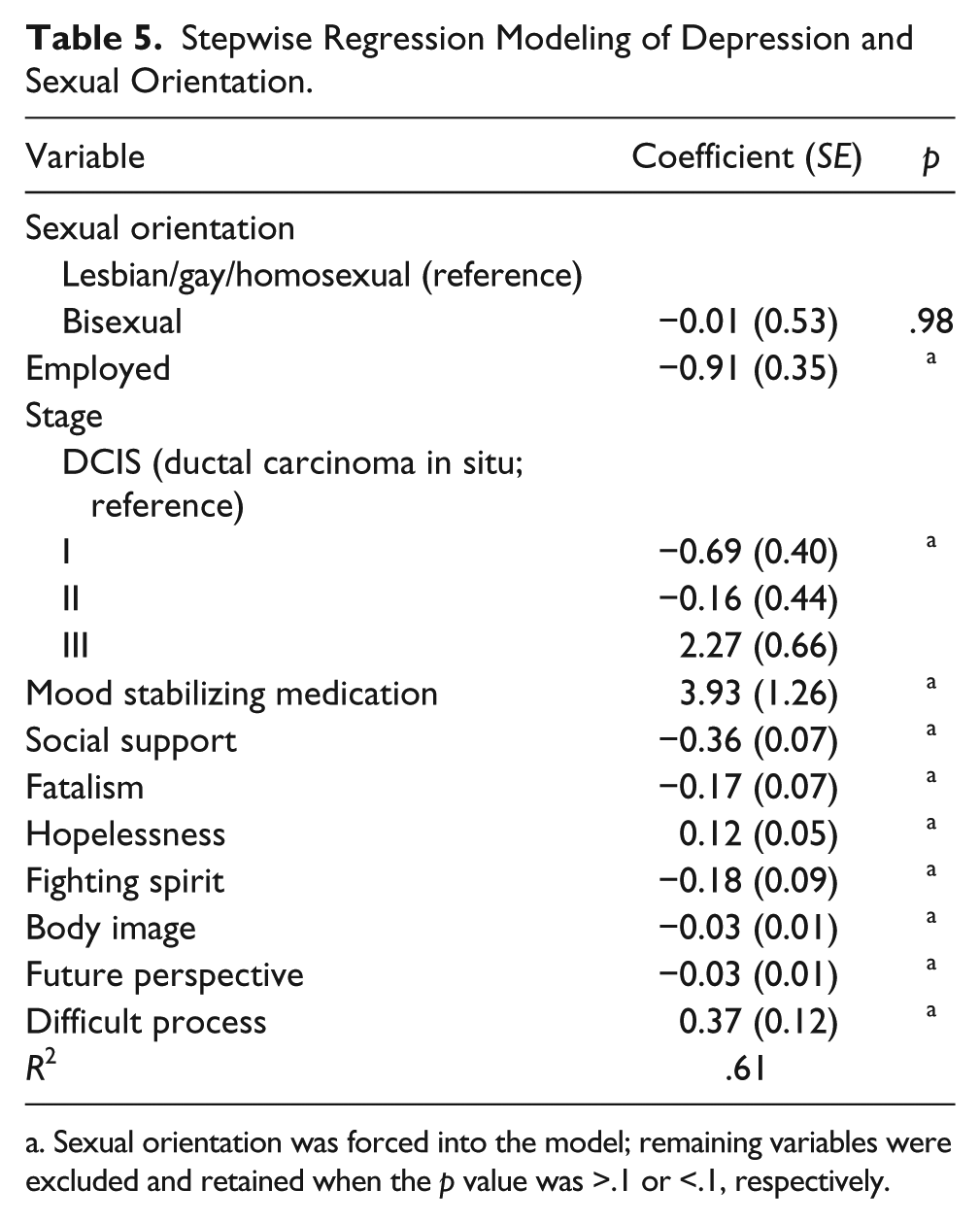
Sexual orientation was forced into the model; remaining variables were excluded and retained when the p value was >.1 or <.1, respectively.
Table 6 presents the explanatory factors for anxiety, which explained 49% of the variance in anxiety. Sexual identity was not significantly associated with anxiety, however, greater sexual orientation disclosure was related to less anxiety. Being older, separated, divorced, widowed, or never married, having sought mental health counseling, fighting spirit coping, better body image, and better future perspective related to less anxiety. Residing in impoverished neighborhoods, attendance of cancer support groups, anxious preoccupation, and experiencing arm symptoms were associated with greater anxiety.
Stepwise Regression Modeling of Anxiety and Sexual Orientation.
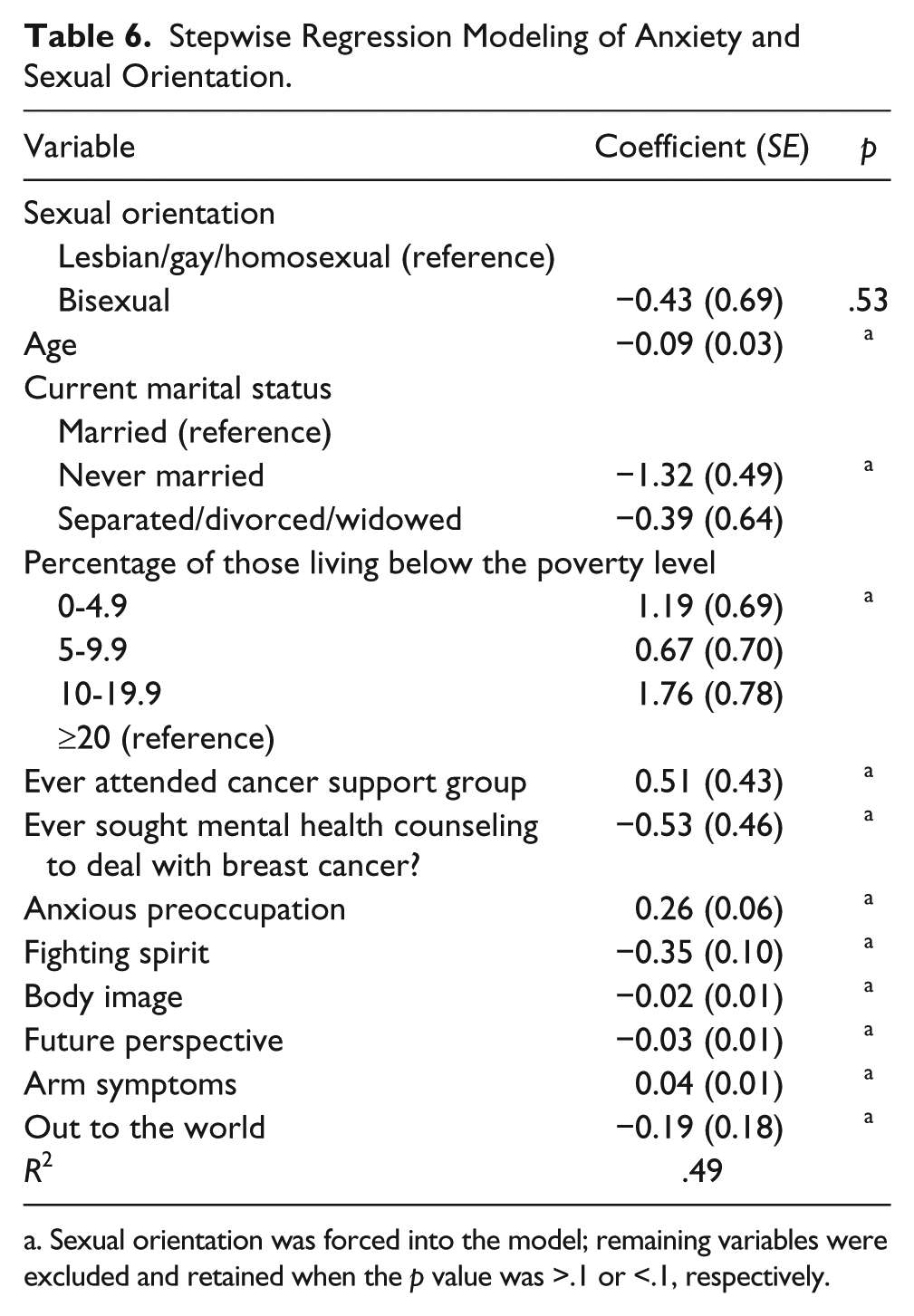
Sexual orientation was forced into the model; remaining variables were excluded and retained when the p value was >.1 or <.1, respectively.
Discussion
In this study, we assessed differences between lesbian and bisexual survivors and explored the contribution of sexual minority–specific factors to lesbian and bisexual survivors’ adjustment. The lesbian and bisexual survivors were similar on almost all characteristics. However, lesbian and bisexual women significantly differed in partner and living arrangements, confirming earlier findings that more lesbians are partnered, and if so with a woman, and are more likely living with their partner compared with bisexual women (Herek et al., 2010). Prior findings of lesbians’ greater disclosure of their sexual orientation, including disclosure to health care providers, compared with bisexual women (Durso & Meyer, 2013; Herek et al., 2010) are consistent with this study’s finding of lesbians’ greater disclosure and trust in physicians.
Six years after their breast cancer diagnosis, this study’s lesbian and bisexual survivors reported similar, generally good adjustment. This is in contrast to earlier studies’ conclusions about worse general and mental health among bisexuals compared to lesbians (Bostwick et al., 2010; Cochran & Mays, 2009; Conron et al., 2010; Ebin, 2012; Fredriksen-Goldsen et al., 2010). We believe there are a number of possible explanations for our study’s absence of disparity in bisexual and lesbian women’s physical and mental health, anxiety, and depression. First, it is feasible that our study sample’s general and mental health may be more affected by their shared history of breast cancer than by their respective sexual identity. Second, mental health tends to improve with age (Franco et al., 2012), and our sample of breast cancer survivors was on average 56 years old, somewhat older than many comparative studies of lesbian and bisexual women’s physical and mental health. Third, our sample of lesbian and bisexual survivors were similar with respect to many aspects of the minority stress model, which commonly explain poor mental health, as well as anxiety and depression. Specifically, lesbian and bisexual survivors reported similar levels of discrimination and had similar scores on each of the LGB scales, suggesting comparable comfort with their sexual minority identity, possibly explaining the absence of a mental health disparity in our study. Finally, lesbian and bisexual survivors’ successful coping with their sexual minority status may put them in a position to cope with a breast cancer diagnosis, possibly applying similar coping mechanisms. Future research is needed to examine these possible interpretations in samples of lesbian and bisexual breast cancer survivors.
The perception that one’s sexual minority identity development has been a difficult process was associated with greater depression in lesbian and bisexual survivors. Openness about sexual orientation in daily life, through disclosing one’s sexual minority identity to coworkers and heterosexual friends, was associated with lower anxiety. These findings somewhat resonate with McGregor et al.’s (2001) finding of a linkage between internalized homophobia and greater distress among lesbians with breast cancer. Our findings are confirmative of the minority stress model (Meyer, 2003), which suggests that issues of disclosure and negative perceptions of one’s sexual minority identity are linked to adverse mental health outcomes.
Sexual minority–specific factors made no significant contribution toward explaining lesbian and bisexual survivors’ physical or mental health. However, our study detected other relevant factors that make a strong contribution toward lesbian and bisexual survivors’ physical and mental health. For example, we interpret the negative association between health insurance and physical health as an indication that survivors in poor physical health were more likely to receive some type of health coverage, possibly through Medicaid or Medicare. Having a partner was associated with survivors’ better physical health, which we suggest may be an indication of the interrelationship of physical health in couples that has been demonstrated among older heterosexual spouses (Hoppmann, Gerstorf, & Hibbert, 2011). With respect to mental health, our study found that survivors with a female partner fared better compared to unpartnered survivors, whereas survivors with a male partner had worse mental health. This finding is consistent with sexual minority women’s positive perceptions of their female partners (White & Boehmer, 2012).
Despite these intriguing findings, this study has a number of limitations. We only have onetime observational data on long-term survivors. Therefore, we can only describe important correlates of lesbian and bisexual survivors’ health-related QOL, anxiety, and depression approximately 6 years after diagnosis. Our findings are not generalizable to lesbians and bisexuals soon after diagnosis, with recurrences, second cancers, or more advanced disease. We lack information about nonresponders, in that their reasons for refusing study participation are unknown and those who refused may differ from those who participated. This study cannot be generalized to other breast cancer survivors of sexual minority status, such as women who have a female partner but do not self-report a lesbian or bisexual identity. The number of bisexual survivors in our sample was small, and therefore we may have not been able to identify additional differences that exist between bisexual and lesbian survivors. Also, the small sample did not allow for further stratification or examination of interactions, which might have identified subgroups of survivors with particular needs for mental health services. Finally, our sample consisted of mostly White, highly educated survivors, which does not allow us to generalize to lesbian and bisexual survivors with less education or those who are racial and ethnic minorities.
This study had several noteworthy strengths. Consistent with the recent Institute of Medicine (2011) report on LGB and transgender health, we examined lesbian and bisexual survivors separately to identify differences between these two groups. Although we did not find many differences between lesbian and bisexual breast cancer survivors, there is a need to build on this investigation with future research studies. Specifically, we need studies with partners and spouses to understand the reasons for our study findings, which linked having a partner to better physical health, linked marital status to anxiety, and found an association between a male partner and poor mental health. Future studies also should examine the needs of lesbian and bisexual survivors who are without a partner. In addition, future studies should consider assessing the experiences of partners of lesbian and bisexual survivors to gain an understanding of the partners’ needs, their coping with the breast cancer diagnosis and treatment, as well as identify any unmet relationship needs that survivors or their partners may have.
This study’s findings are particularly instructive for nurses, mental health professionals, and other medical providers who provide services to breast cancer survivors. Professionals should be aware of the considerable need for mental health services among lesbian and bisexual survivors, in that about half of this study’s 6-year survivors used antidepressant medications, about 40% attended a cancer support group, and 30% to 50% sought mental health services because of their breast cancer. Specifically, this study linked two sexual minority–specific factors to mental health outcomes. Disclosure of sexual orientation was related to less anxiety and perceiving the development of sexual identity as a difficult process was associated with depression. Therefore, there is an opportunity for providers to have a direct positive impact on sexual minority women’s mental health. Consistent with guidelines for culturally competent care (McNair & Hegarty, 2010), we suggest providers offer a safe and welcoming environment to facilitate open communication and disclosure of sexual orientation. This includes using intake forms that facilitate the disclosure of sexual orientation, staff trainings in cultural awareness and acceptance, and sensitive and open clinician–patient communication to ease sexual minority women’s barriers to disclose their sexual minority orientation and discuss experiences with their sexual minority status that reduces their QOL during and after a cancer diagnosis. An accepting and welcoming attitude toward lesbian and bisexual women also includes inquiring about women’s partnership status and support system in a neutral way, rather than assuming that women have male partners and traditional family structures for support. Furthermore, professionals who treat survivors who report being without a partner or present with a male partner should not label them heterosexual, unless details about sexual orientation have been ascertained. Professionals may consider offering survivors the opportunity to include a significant support person into medical or auxiliary service visits, and should be inclusive of single as well as partnered women of any sexual orientation. Furthermore, cancer support groups and mental health services should be offered, and if not available locally or within an institution, referrals should be made to address these needs elsewhere. Professionals can be proactive in that they can provide information about such services, rather than putting the burden on lesbian or bisexual survivors to state their needs. However, any cancer support group or mental health service has to be culturally appropriate to lesbian and bisexual women or if available should cater specifically to lesbian and bisexual or other sexual minority women. Finally, our study points to opportunities for programs that address and modulate survivors’ coping, body image, and future perspective to improve their anxiety, depression, and QOL. Moreover, nurses and other professionals should assess lesbian and bisexual survivors’ systemic side effects, arm symptoms, body image, and future perspective, to possibly alleviate their impact on QOL, anxiety, and depression.
Footnotes
Acknowledgements
The authors are grateful to the participants who took the time to respond to our questions and complete the survey.
Author Roles
Ulrike Boehmer originated the study, interpreted the findings, and led the writing. Mark Glickman provided his statistical expertise to direct the analysis and to interpret the findings. Michael Winter conducted the analyses and helped interpret the findings. Melissa A. Clark provided conceptual input and helped interpret the findings. All authors contributed in significant ways to the final article by discussing earlier drafts and reviewing and revising the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the American Cancer Society, Grant No. RSGT-06-135-01-CPPB.