
Abstract
Introduction
Despite significant declines in the national smoking prevalence over the past few decades, tobacco use rates among individuals with mental illnesses (MI) have seen little change; rates for some diagnostic groups (e.g., schizophrenia) are estimated at 2 to 3 times the national average (Centers for Disease Control and Prevention, 2009, 2013; McClave, McKnight-Eily, Davis, & Dube, 2010; Morisano, Bacher, Audrain-McGovern, & George, 2009). There are genetic (e.g., genetic polymorphisms that are related to increased smoking in certain MI diagnostic groups; Faraone et al., 2004; Koenen et al., 2005; Lyons et al., 2008), bio-behavioral (i.e., coping with the severity of MI symptoms and amelioration of the side effects of psychotropic medications; Barnes et al., 2006; Postma et al., 2006), and psychosocial (i.e., permissive attitudes and cultural norms of smoking in behavioral health facilities; Lawn, 2008; Sheals, Tombor, McNeill, & Shahab, 2016) reasons associated with elevated tobacco use among individuals with MI. Persons with MI who use tobacco are therefore more likely to experience poorer physical health, have worsened psychiatric symptomology, and report adverse mental health outcomes as compared to their non–tobacco-using counterparts (Dodd et al., 2010; Kotov, Guey, Bromet, & Schwartz, 2010; Saiyad & El-Mallakh, 2012; Tran et al., 2009). By not addressing tobacco use in these populations, those with MI will continue to be disproportionately affected by tobacco-related diseases and mortality (Ziedonis et al., 2008).
Persons with MI who use tobacco desire to stop their tobacco use (McClave et al., 2010; Prochaska et al., 2011; Siru, Hulse, & Tait, 2009); but in behavioral health settings, their engagement in tobacco treatment may be hindered by several individual- (e.g., poor confidence in quitting), provider- (e.g., permissive attitudes toward smoking, and low confidence in delivering tobacco treatment), and organization-related (e.g., absence of smoke-free policies or resources for tobacco treatment) factors (Johnson et al., 2009; Johnson, Moffat, & Malchy, 2010). To enhance treatment, current clinical practice guidelines for addressing tobacco dependence recommend that health care providers routinely engage patients in tobacco treatment (U.S. Preventive Services Task Force, 2015). This may be achieved through brief interventions, using the 5As (Ask, Advise, Assess, Assist, Arrange) approach (Fiore et al., 2008; U.S. Preventive Services Task Force, 2015). However, few clinicians in psychiatric facilities routinely engage patients in treatment (Ratschen, Britton, Doody, Leonardi-Bee, & McNeill, 2009; Rogers & Sherman, 2014). In fact, as compared to those without MI, individuals with MI are less likely to receive advice to stop smoking, especially if they have a severe MI (i.e., schizophrenia, bipolar disorder, or major depression; Mitchell, Vancampfort, De Hert, & Stubbs, 2015).
Understanding providers’ behavioral intentions to address tobacco use for individuals with MI may offer an opportunity to improve treatment in this population. As a guiding framework, the theory of planned behavior (TPB) asserts that behaviors occur in specific contexts (Ajzen, 1991). Underlying the main constructs of the TPB is the assumption that behavior is a result of salient beliefs (i.e., behavioral, normative, and control beliefs) relevant to specific behaviors. The TPB proposes that attitudes (i.e., the extent to which a person has favorable or unfavorable judgments), subjective norms (i.e., the perceived social pressure to execute or not execute), and perceived behavioral control (i.e., the perceived ease or challenge of performing) toward a behavior each independently predict the intention to perform the behavior. Intention to perform the behavior then predicts the actual behavior (Ajzen, 1991). As examples, the TPB has been used to understand the relationship of smoke-free air laws and intention to quit smoking in the United States (Macy, Middlestadt, Seo, Kolbe, & Jay, 2012), the provision of tobacco treatment among health care providers in community settings in Vietnam (Shelley et al., 2014), and the intentions of providing tobacco treatment among mental health professionals in the Netherlands (Blankers, Buisman, Hopman, van Gool, & van Laar, 2016). Applying the TPB framework within an inpatient psychiatric setting may be useful to comprehend providers’ intentions and behaviors in engaging tobacco treatment among individuals with MI.
At 26.5%, Kentucky has one of the highest adult smoking prevalence rates in the United States (Nguyen, 2016). It has been estimated that between 2009 and 2011, 41% of individuals with MI in Kentucky were also persons who currently used tobacco, as compared to a national average of 21.4% among those without MI (Centers for Disease Control and Prevention, 2013). Moreover, in 2009, rates of smoking among hospitalized patients with MI in Kentucky were as high as 74% for individuals with schizophrenia as compared to 31% in the state (Diaz et al., 2009). The high smoking prevalence among individuals with MI in Kentucky may be attributed to the neglect of tobacco treatment within mental health services and poor engagement of these patients in cessation interventions (Currie, Nesbitt, Wood, & Lawson, 2003). Hence, the purpose of our study was to examine the intentions of staff in a state psychiatric facility in Kentucky to engage patients in tobacco treatment. Specifically, among staff in the facility, we examined factors associated with
intentions to provide tobacco treatment and
reported provision of evidence-based tobacco treatment (i.e., 5As).
Method
Participants
Data for this study were based on a 15 to 20 minute survey administered to staff at a state psychiatric hospital. To be eligible for the survey, staff had to meet the criterion of being currently employed at the facility on a part-time or full-time basis. A total of 270 staff was targeted based on quotas derived from available staff roles at the time of the survey; however, only 206 completed the surveys. The goal for quota sampling was to obtain a representation of different disciplines. In addition to direct providers (i.e., physicians, nurses, social workers, psychologists, etc.), 11 non–direct providers (i.e., security, dietary) also participated in the survey for a 76.3% (206/270) response rate.
Ethical Considerations
The study was approved by the University of Kentucky Medical Institutional Review Board (IRB No. 15-1096-P6K). A cover sheet explaining the study objectives and procedures was attached to the survey questionnaires. We explained that the study was voluntary and that participating in the study implied consent. Questionnaires were made available in staff break rooms and on request. Unit managers assented for staff to use work time, as required, to complete the surveys. Participants were offered the opportunity to be entered into a drawing for the chance to win one of five $20 cash incentives. Participants interested in the drawing further completed a contact sheet (separate from the questionnaire) on which they provided their name, phone number, and e-mail address. These contact sheets were separated from the survey, such that it was not possible to match the contact information to survey responses.
Investigative Procedures
This study is based on a cross-sectional, descriptive design. We obtained survey responses from a convenience sample (with targeted quotas) of staff at a psychiatric facility over a period of 4 months (March 1 to June 30, 2016). Hard copies of the surveys were made available to all staff at the hospital. On completion of a survey, the staff member would place the survey in a specified, private, location in the office of the principal investigator. The return of the surveys to that location preserved anonymity of the surveys.
Measures
Demographic Variables
The demographic variables used to characterize the sample included sex (males vs. females), age (in years), ethnicity (White vs. non-White), education level (high school vs. some college/trade school vs. college graduate), marital status (married/widowed vs. unmarried couple vs. separated/divorced vs. single/never married), work tenure (in months), and primary discipline or job role (psychiatrists/advance practice registered nurses/pharmacists, nursing staff [LPN, ADN, BSN], social work and psychology, mental health associates/state-registered nursing assistants, therapists, and other [security staff, dietary staff, quality control staff, unit clerks]).
Tobacco Use Status
Information on current tobacco use (having used part or all of a tobacco product in the past month; Centers for Disease Control and Prevention, 2013) was obtained from participants. Electronic nicotine delivery devices (i.e., e-cigarettes or vaporizers) were included in tobacco use status. Those endorsing tobacco use in the past month were coded as “Persons who use tobacco” and those who did not were coded as “Persons who do not use tobacco.”
Intentions to Provide Tobacco Treatment
Intentions to provide tobacco treatment was assessed by three questions based on the TPB (Ajzen, 1991, 2011; see Table 1). A mean score of the scale (range = 1-7) was derived, and the scale demonstrated strong internal consistency (α = .92).
Questions on Intentions, Attitudes, Subjective Norms, and Perceived Behavioral Control Using the TPB Framework.
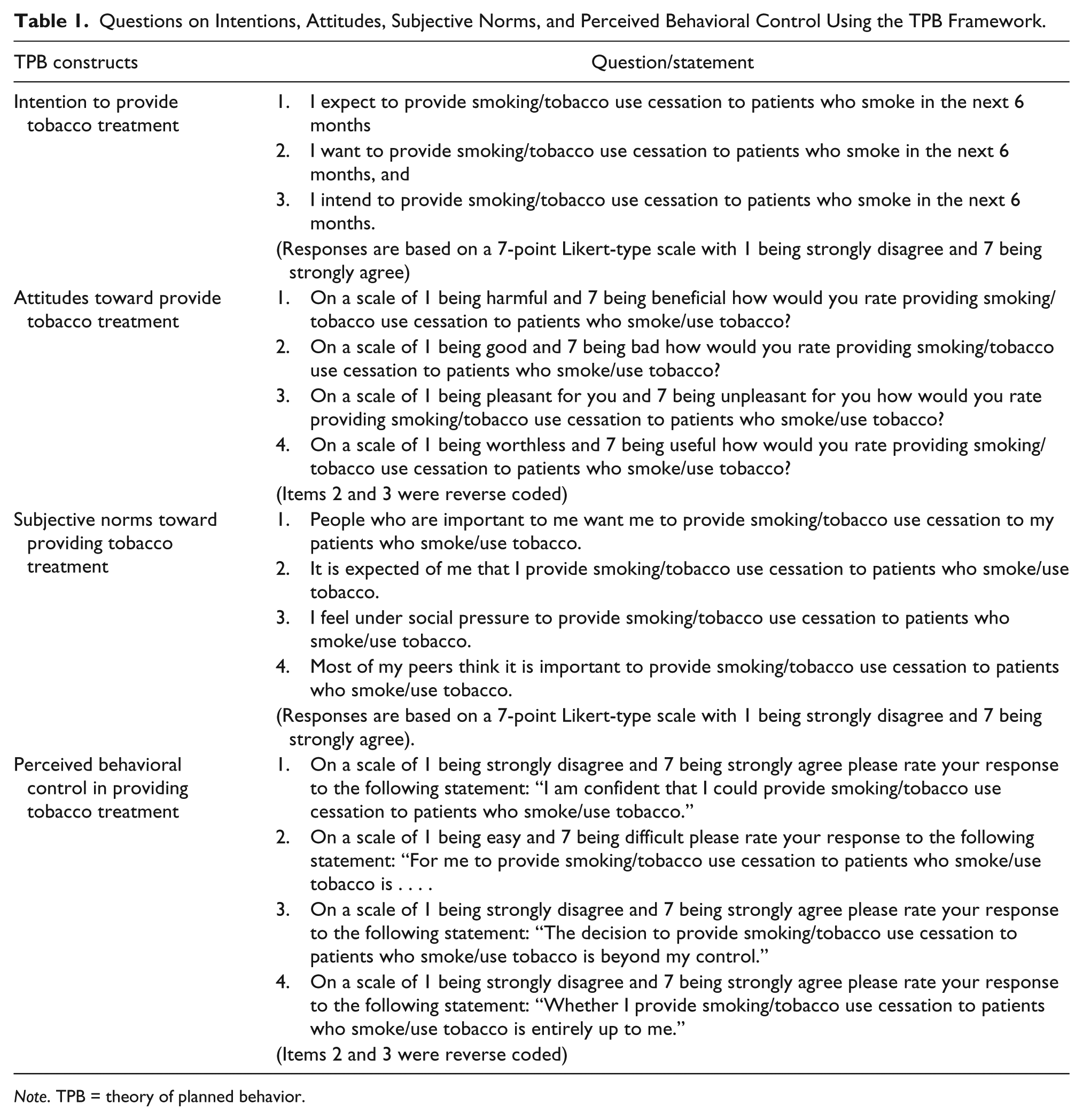
Note. TPB = theory of planned behavior.
Attitudes About Providing Tobacco Treatment
Attitudes about providing tobacco treatment were assessed by four questions based on the TPB (Ajzen, 1991, 2011; see Table 1). A mean score (range = 1-7) was derived, and the scale demonstrated acceptable internal consistency (α = .80).
Subjective Norms About Providing Tobacco Treatment
Subjective norms toward providing tobacco treatment were assessed by four questions based on the TPB (Ajzen, 1991, 2011; see Table 1). A mean score (range = 1-7) was derived, and the scale demonstrated adequate internal consistency (α = .79).
Perceived Behavioral Control in Providing Tobacco Treatment
Perceived behavioral control toward providing tobacco treatment was assessed by four questions based on the TPB (Ajzen, 1991, 2011; see Table 1). A mean score (range = 1-7) was derived, but the scale did not demonstrate adequate internal consistency (α = .50).
Use of Brief Interventions for Tobacco Treatment (5As) in Practice
We developed a five-item brief measure to determine the use of brief interventions for tobacco treatment in practice based on recommended clinical practice guidelines for treating tobacco use and dependence (Fiore et al., 2008). Specifically, we asked participants: In your practice/role, how often do you
ask patients whether they smoke cigarettes or use other tobacco products
advise patients who smoke or use other tobacco products to quit?
assess the readiness of patients who smoke/use other tobacco products to quit or cut down?
assist patients in stopping smoking/tobacco use by providing medications and/or counseling
arrange for patients to be referred to smoking/tobacco use cessation services or follow up with them on their abstinence?
Each question was based on a 4-point Likert-type scale with response choices of 1 (never), 2 (seldom), 3 (occasionally), and 4 (very often). For analysis, the scale was adjusted from 0 (never) to 3 (very often). A mean score was derived with higher score indicating greater use of brief interventions. The scale demonstrated adequate internal consistency (α = .87).
Data Analysis
Of 206 participants, 11 (5.0%) did not provide responses to the main outcome variables; hence, only responses from 195 surveys were included for analysis. Descriptive analysis was based on means (with standard deviations) and frequencies (with percentages) to describe the sample. Differences between demographic and the main outcome variables by tobacco use status were examined using chi-square analyses for nominal and ordinal variables and independent sample t tests (with Levene’s test for equality of variance) for continuous variables.
In addition, a hierarchical multivariate linear regression analysis procedure was used to determine the associations between the intention to provide tobacco treatment and attitudes, subjective norms, and perceived behavioral control, while controlling for potential mediating demographic variables. A hierarchical multivariate regression analysis is a statistical method that examines the relationships between certain independent and dependent variables. The hierarchical multivariate analysis can be useful to determine whether some theoretically related variables actually demonstrate the relationships they are purported to have. For this regression analysis, demographic variables were entered first, followed by each of the variables in the TPB (attitude, then subjective norms, then perceived behavioral control). A final multivariate regression analysis was developed by examining the variables that were most associated with the provision of brief interventions while including demographic variables and all variables of the TPB. All analyses were conducted using IBM SPSS Statistics Version 23. An alpha level of .5 was set for statistical significance in all analyses.
Results
Sample Description
The sample was predominantly female (79.5%), predominantly White (75.9%), and on average 35.3 (SD = 12.4) years of age. The majority of participants had a completed college degree (71.3%) and were either single or separated/divorced (54.8%). Most participants were mental health associates/state-registered nursing assistants (43.1%) and on average had worked at the facility for 35.2 (SD = 63.9) months. Eighteen percent of participants were persons who use tobacco. A greater proportion of participants who used tobacco were White as compared to non-White (21.6% vs. 8.5%), χ2(1, N = 195) = 4.1, p < .05. These observed differences in tobacco use contrasts to the prevalence in the state of Kentucky, which has a slightly higher tobacco use prevalence among non-White ethnic groups (e.g., 30.2% among Black, 28.2% among Hispanic, and 41.5% among non-Hispanic other ethnicities, compared with 29.3% among White; Nguyen, 2016). There were no other significant demographic differences between persons who did and did not use tobacco (see Table 2).
Sample Characteristics by Tobacco Use Status.
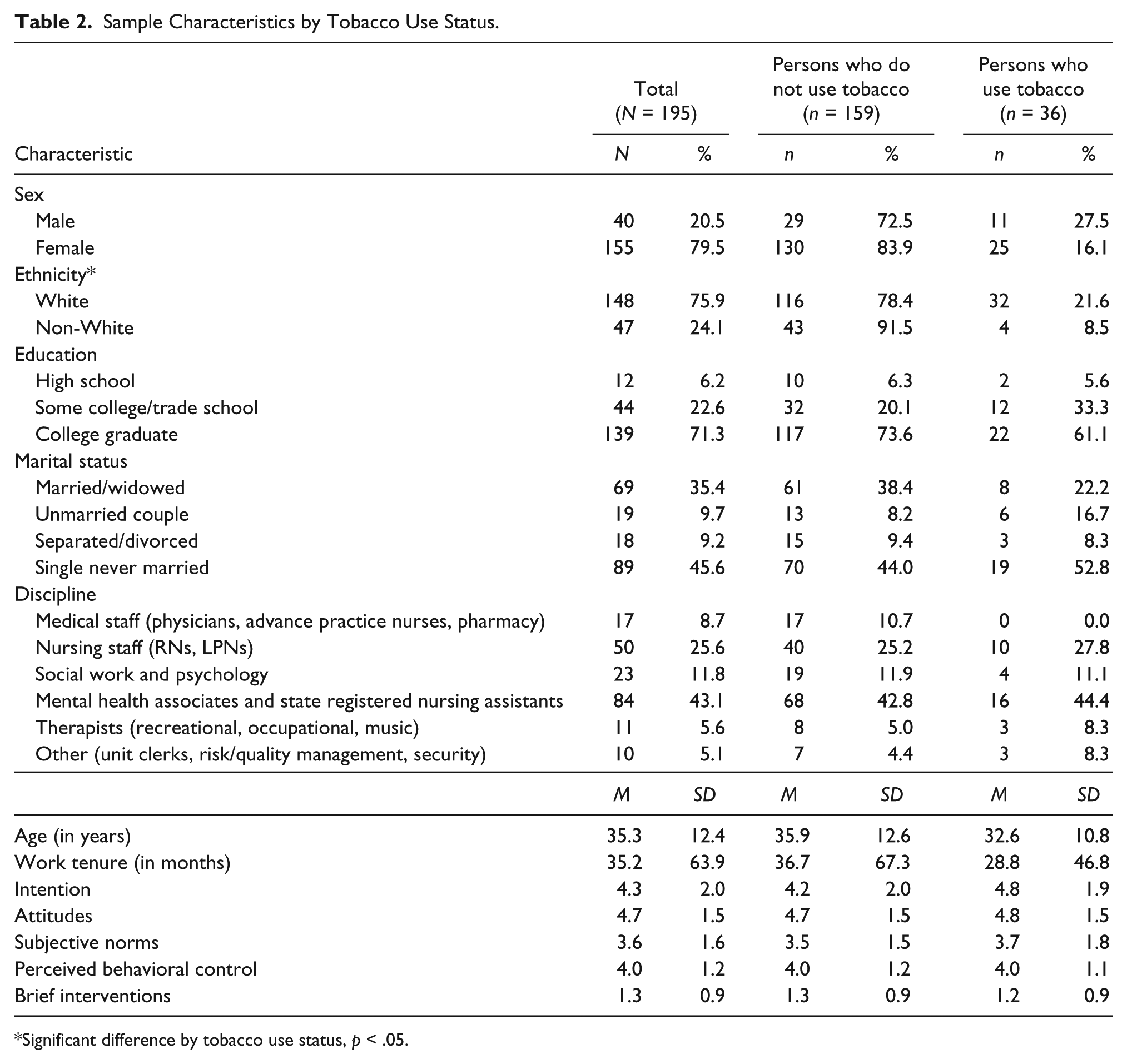
Significant difference by tobacco use status, p < .05.
Factors Associated With the Intention to Provide Tobacco Treatment
On average, participants had mid- to moderate scores on attitudes about providing tobacco treatment (M = 4.7, SD = 1.5), subjective norms about tobacco treatment (M = 3.6, SD = 1.6), perceived behavioral control in delivering tobacco treatment (M = 4.0, SD = 1.2), and intentions to provide tobacco treatment (m = 4.3, SD = 2.0; see Figure 1). There were significant differences by job role in intention, F(5, 189) = 3.9, p = .002, and subjective norms, F(5, 189) = 5.9, p < .0001. Nursing staff had lower intention scores than medical staff but higher mean subjective norms scores than all other job roles. There were no significant differences between persons who did and did not use tobacco in these variables; thus, tobacco use status was not included in subsequent multivariate analyses.
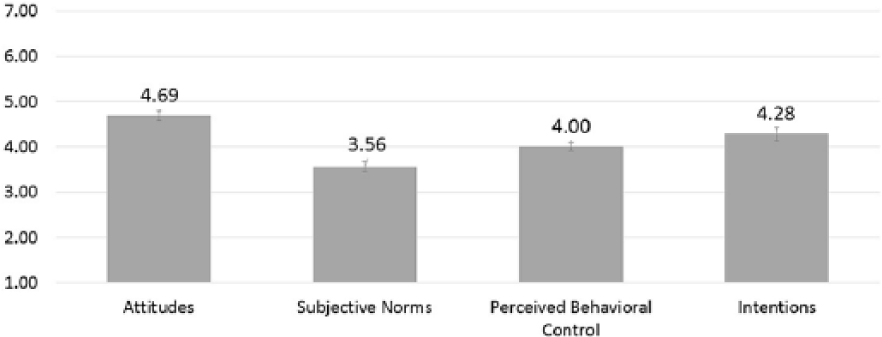
Mean scores on variables of the theory of planned behavior (i.e., attitudes, subjective norms, perceived behavioral control, and intentions to providing tobacco treatment).
A hierarchical multivariate regression analysis was used to examine the association between the variables of the TPB by regressing intention to provide tobacco treatment on attitudes, subjective norms, and perceived behavioral control while controlling for demographic variables. In the first step of the hierarchical regression analysis, demographic variables significantly accounted for 9.8% of the variance in intentions to provide tobacco treatment. In the subsequent addition of attitudes, subjective norms, and perceived behavioral control in the second, third, and fourth steps of the analysis, each accounted for an additional 10.5%, 18.2%, and 3.5%, respectively, in the variance of intentions to provide tobacco treatment. The final model (fourth step) indicated that no demographic variables were significantly associated with intentions to provide tobacco treatment. However, attitudes, subjective norms, and perceived behavioral control were each independently associated with intentions to provide tobacco, with subjective norms having the strongest associations (see Table 3).
Regression of Intention to Provide Tobacco Treatment on Demographics, Attitudes, Subjective Norms, and Perceived Behavioral Control.
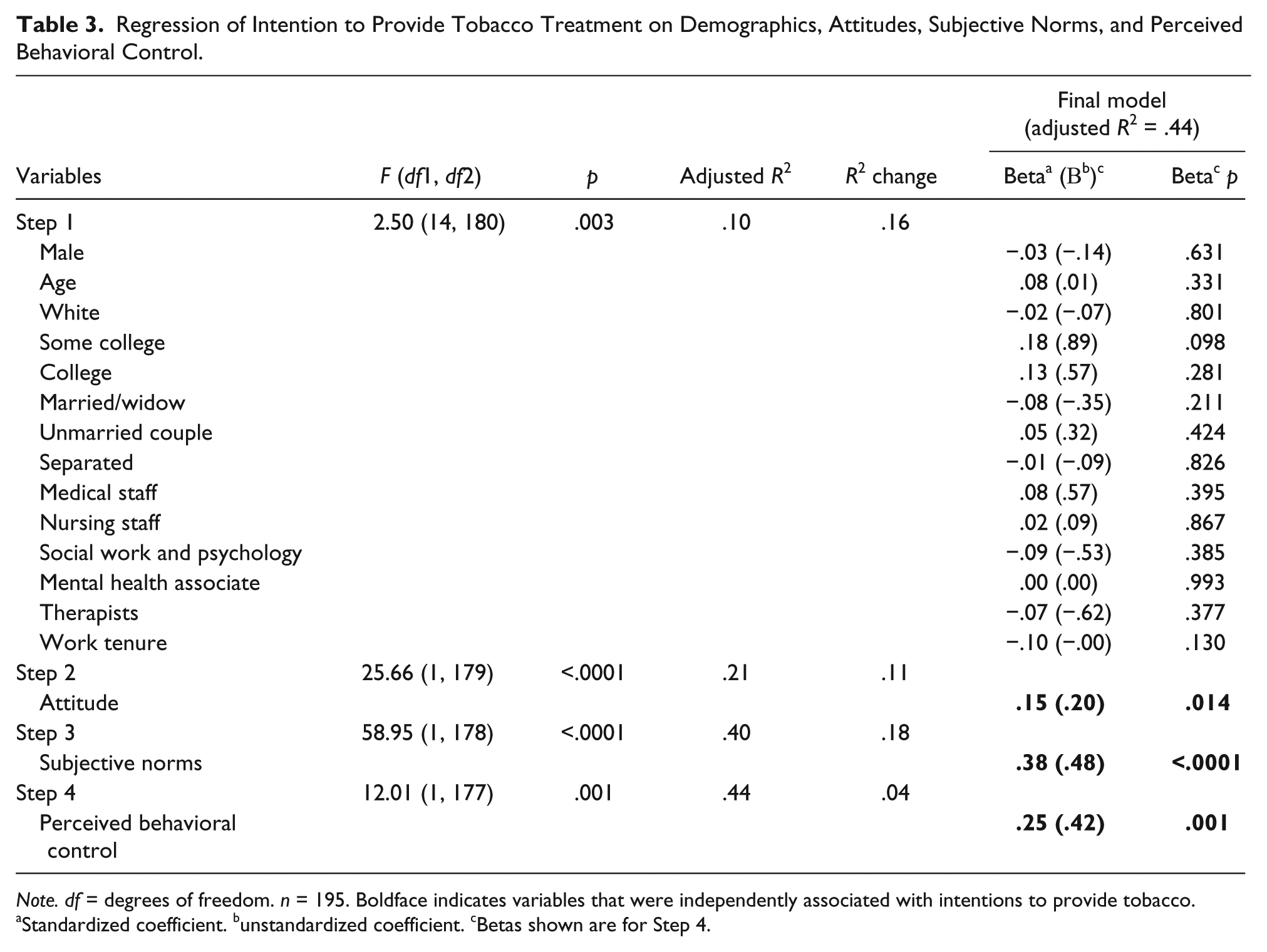
Note. df = degrees of freedom. n = 195. Boldface indicates variables that were independently associated with intentions to provide tobacco.
Standardized coefficient. bunstandardized coefficient. cBetas shown are for Step 4.
Factors Associated With the Provision of Brief Interventions
Among the brief interventions, on a scale of 0 to 3, the most frequently endorsed intervention was Ask (M = 1.62, SD = 1.16), followed by Advise (M = 1.58, SD = 1.10), Assess (M = 1.24, SD = 1.06), Assist (M = 1.17, SD = 1.11), and Arrange (M = 0.85, SD = 1.04). On average participants had low scores on providing all components of the brief interventions (M = 1.3, SD = 0.9). There were significant differences in providing all components of the brief interventions by type of staff, F(5, 189) = 7.7, p < .0001, with medical staff having the highest scores and “other” staff with the lowest scores (see Figure 2).
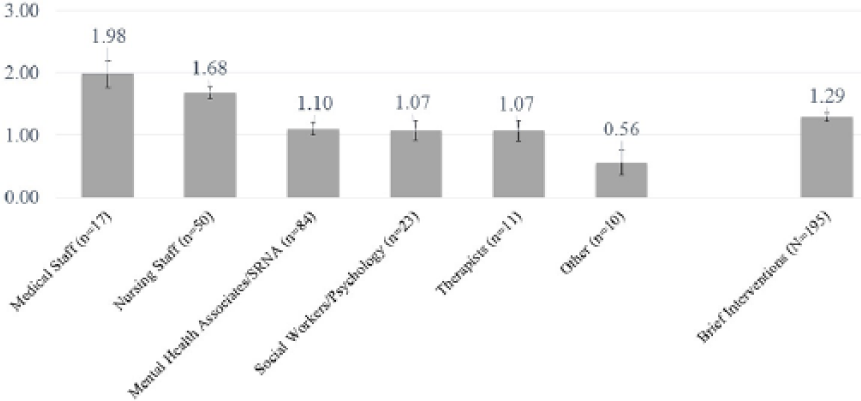
Mean scores on the provision of brief interventions (scale of 0-3) by job role.
A multivariate regression analysis was performed to identify factors that were associated with the provision of brief interventions from among demographic and the TPB variables (see Table 4). In the final multivariate model, being older, being a medical or a nursing staff, having a shorter work tenure, higher subjective norm of providing tobacco treatment scores, and higher perceived behavioral control in providing tobacco treatment scores were significantly associated with higher scores on providing brief interventions.
Regression of Use of Brief Interventions on Demographics, Attitudes, Subjective Norms, Perceived Behavioral Control, and Intentions to Provide Tobacco Treatment.
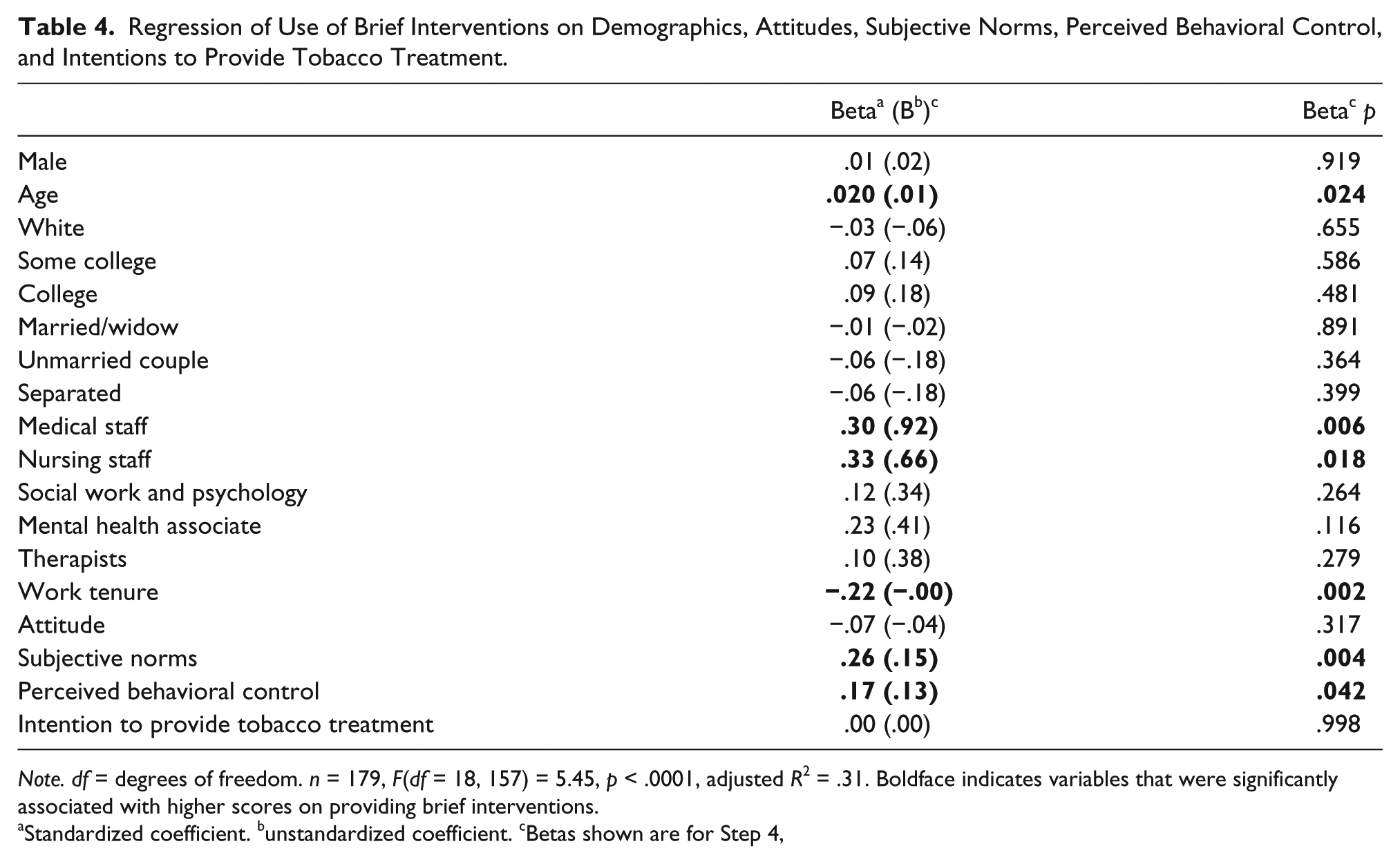
Note. df = degrees of freedom. n = 179, F(df = 18, 157) = 5.45, p < .0001, adjusted R2 = .31. Boldface indicates variables that were significantly associated with higher scores on providing brief interventions.
Standardized coefficient. bunstandardized coefficient. cBetas shown are for Step 4,
Discussion
This study assessed factors that were associated with the intention to provide tobacco treatment as well as provision of the brief interventions for tobacco treatment among staff at a state psychiatric hospital. The key findings were that as confirmed by the TPB, greater attitudes, subjective norms, and perceived behavioral control in providing tobacco treatment were associated with the intention to provide treatment. Moreover, age, job role, work tenure, subjective norms about tobacco treatment, and perceived behavioral control in providing treatment were associated with greater reported use of the clinical practice guidelines in providing tobacco treatment. These findings may have important implications for the delivery of tobacco treatments within behavioral health settings.
Several studies have used the TPB as a framework to examine tobacco treatment practices in various settings with similar findings to our study. For example, Shelley et al. (2014) found that in multivariate analyses using constructs of the TPB, only normative beliefs (e.g., “My supervisors think that helping smokers quit is a priority,” “Most of the staff thinks that promoting smoking cessation is part of their job”) remained a significant factor in asking patients about tobacco use or advising them to quit smoking. However, in a structural equation modeling study based on a survey of 506 mental health professionals in the Netherlands, Blankers et al. (2016) found that although subjective norm was not a predictor of the intention to provide support to tobacco using patients in the next year, staff attitudes and perceived behavioral control were. However, it is important to note that subjective norm in the Blankers et al. (2016) study was measured with questions assessing the policy environment (e.g., “There is a strict smoking policy,” “The policy is clearly written on the ward”) and not the peer expectations on the health care providers. In light of our present study that found subjective norms to be the strongest predictor of tobacco treatment intentions and behavior, it may be important to target enhancing such norms in relation to provider job roles. Future studies may need to examine the salient aspects of subjective norms that can enhance the intentions and practices of mental health providers in providing tobacco treatment to patients.
We also found that staff reported screening for tobacco use but were less likely to engage patients in evidence-based tobacco treatment. This finding is similar to an analysis of the National Ambulatory Medical Care Survey, which found that between 2006 and 2010, psychiatrists in the United States screened for tobacco use at 60% of patient visits but provided cessation counseling for only 23% of smokers (Rogers & Sherman, 2014). Our study also found higher rates of screening (i.e., asking “occasionally/very often”) for tobacco use among providers at 54.4% as compared to providing treatment (i.e., assisting “occasionally/very often”) at 37.9%. Prior studies have suggested that important obstacles to providing tobacco treatment in mental health settings may be related to perceived provider-related barriers, perceived client-related barriers, and perceived tobacco-related barriers (Johnson et al., 2009). The low rate of evidence-based tobacco treatment provision in our current study suggests the need to identify context- or site-specific factors that may be obstacles to treatment provision. Future studies that assess such site-specific hindrances to tobacco treatment can be instrumental in determining strategies to mitigate such barriers.
Finally, although 18% of the staff in our study were persons who used tobacco, their tobacco use did not significantly affect their intentions to provide tobacco treatment or their practice of providing evidence-based tobacco treatment as compared to staff who did not use tobacco. This finding is contrary to other studies that have demonstrated that providers who use tobacco are less likely to provide tobacco treatment to patients. For example, a recent study in Australia among mental health practitioners found that those practitioners who currently smoked cigarettes were less likely to advise patients with MI to stop smoking and were less likely to use all of the 5As for tobacco treatment as compared to providers who did not smoke cigarettes (Sharma, Meurk, Bell, Ford, & Gartner, 2017). The dissimilar findings of our current study may be unique to the particular hospital setting, given that the hospital has a tobacco-free–grounds policy and also provides staff who use tobacco with support (in terms of smoking cessation medication and counseling) to quit. Nonetheless, future studies may be needed to understand reasons why providers who use tobacco products would support providing tobacco treatment to persons with MI.
Limitations
There are some important limitations that need to be considered in interpreting the findings of this study. As this study is based on a sample from a single site, our findings cannot be generalized to other behavioral health settings. In addition, because the study was a cross-sectional analysis, it is possible that participant responses may have changed over time. During the 4-month survey collection period, there were staff turnovers, which could have affected the availability of participants to meet specific job role quotas.
Moreover, as a convenience sample, the responses from the surveys may not fully represent the views of all staff at the psychiatric hospital; nonetheless, with a 76% response rate from targeted quotas of staff, we believe that the findings are strengthened by having all clinical disciplines represented. However, because the survey methodology aimed to preserve anonymity, it is possible, but highly unlikely, that some staff may have filled out multiple surveys. To minimize the challenge of multiple responses, and to enhance the fidelity of the study, future studies may use computer-based survey methodology to appropriately identify potentially duplicate surveys.
Finally, the sample internal consistency reliability for the perceived behavioral control score was low (α = .50). As such, our findings may have been affected by the poor reliability in this specific measure. This indicates the need to either revise the actual questions that measure perceived behavioral control or change the scoring scale. For example, perceived behavioral control toward providing tobacco treatment could be changed to questions such as, “If I wanted to, I could provide tobacco treatment to persons with mental illness who use tobacco” on a scale of definitely true as 1 to definitely false as 7. Or another question could be “How much control do you believe you have in providing tobacco treatment to persons with mental illness who use tobacco” on a scale of no control as 1 to complete control as 7. Future studies may explore the use of other questions that could be adapted from the TPB to assess perceived behavioral control in providing tobacco treatment among clinicians in psychiatric hospital settings. In addition, the largest percentage of participants were technical staff whose education/training may have limited their sense of perceived behavioral control to provide tobacco treatment.
Implications for Nursing Practice
Psychiatric mental health nurses (PMHNs) are well positioned to advocate for tobacco treatment among patients with MI (Cataldo, 2001). Guo, Wang, and Shu (2015) have observed that low self-efficacy in delivering different components of tobacco treatment by PMHNs presents an important barrier to engagement in treating patients. Specifically, although PMHNs may have greater self-efficacy in determining patients’ tobacco dependence, they have lower self-efficacy in assessing their readiness to engage in treatment, discuss methods for smoking cessation, and understand the influence of smoking cessation on psychiatric symptoms (Guo et al., 2015). This finding reinforces the need to provide evidence-based tobacco treatment training to PMHNs and PMHN students (Price, Jordan, Jeffrey, Stanley, & Price, 2008; Schwindt & Sharp, 2013). Several training programs and manuals exist to enhance the competency in providing tobacco treatment by health care providers. For example, the American Psychiatric Nurses Association has endorsed a manual based on evidence-based guidelines that is specific to promoting and enhancing tobacco treatment skills among practicing nurses (Sharp, Bellush, Evinger, Blackman, & Williams, 2009). Hence, certified tobacco treatment training programs (see a list from the Association for the Treatment of Tobacco Use and Dependence, www.attud.org) should be promoted to enhance treatment competency among PMHNs.
In addition, because peer subjective norms may be an important factor in providing tobacco treatment, it is critical for PMHNs to advocate for tobacco-free behavioral health settings (Moss et al., 2010). Tobacco-free initiatives can “de-normalize” a pro–tobacco use culture in behavioral health settings (Schroeder & Morris, 2010). In fact, the implementation of tobacco-free policies is associated with increased provision of evidence-based tobacco treatment by providers in psychiatric settings (Etter, Khan, & Etter, 2008). Such tobacco-free initiatives in psychiatric hospital settings are also associated with increased cessation attempts, reduced tobacco consumption, and improved tobacco treatment outcomes among patients (Hehir, Indig, Prosser, & Archer, 2013; Stockings et al., 2014). Hence, PMHNs should be equipped with resources to lead the development of tobacco-free policies in their work settings (Cataldo, 2001).
Conclusions
Engaging tobacco using patients with MI in treatment is an important aspect of evidence-based care. By understanding factors that influence provider intentions to deliver tobacco treatment and their treatment practices, we can better determine strategies to enhance tobacco treatment in behavioral health settings. Our findings suggest that in our study sample, attitudes, subjective norms, and perceived behavioral control were associated with intentions to provide tobacco treatment, but only subjective norms and perceived behavioral control were associated with reported evidence-based tobacco treatment provision when controlling for other variables. Future studies may examine provider intentions and practices of delivering tobacco treatment in other behavioral health settings using the TPB as a framework. Such research can provide further directions in developing context specific interventions for providers to enhance tobacco treatment for patients with MI. These studies can be instrumental in providing treatment guidelines and policies to further address the disproportionate tobacco-related disease burden among those with MI.
Footnotes
Acknowledgements
We want to acknowledge the staff and department managers at Eastern State Hospital for their support in the execution of the study.
Author Roles
Chizimuzo Okoli conceived, planned, analyzed and drafted the introduction, results, and discussion sections of the article. Janet Otachi assisted in drafting the Abstract section, data analysis, and drafting the Results section of the article. Sooksai Kaewbua assisted in reviewing drafts of the article. Marc Woods assisted in planning the study and reviewing drafts of the article. Heather Robertson managed the project and assisted in reviewing drafts of the article. All authors are responsible for the article content.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Okoli is a consultant with ![]() , a community mental health program, and Director of Evidence Based Treatment and Tobacco Treatment Services at Eastern State Hospital.
, a community mental health program, and Director of Evidence Based Treatment and Tobacco Treatment Services at Eastern State Hospital.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.