
Abstract
Keywords
On April 29, 2002, President George W. Bush announced the creation of the New Freedom Commission on Mental Health, which was charged with making recommendations to promote the recovery and full community integration of individuals with severe mental illness (SMI). In their final report, the Commission wrote that recovery from mental illness is now a real possibility. The promise of “a life in the community for everyone can be realized.” Yet for too many Americans with mental illnesses, the mental health services and supports they need remain fragmented, disconnected, and often inadequate, frustrating the opportunity for recovery. Instead of ready access to quality care, the system presents barriers that all too often add to the burden of mental illness for individuals, their families, and communities. The Commission recommended a fundamental transformation of the nation’s approach to mental health care. This transformation must ensure that mental health services and supports actively facilitate recovery and build resilience to face life’s challenges (U.S. Department of Health and Human Services, 2003).
Problem Description
Federal policy reports and Veterans Health Administration (VHA) handbooks provided the impetus and the building blocks to construct a mental health delivery system that was, in some ways, antithetical to the existent provider system of care. Alternatively, these reports recommended a system driven by patient–provider collaboration rather than a provider-driven system (Substance Abuse and Mental Health Services Administration’s [SAMSHA], 2004; U.S. Department of Veterans Affairs, Veterans Health Administration [VHA], 2008; VHA, 2013). Given the dramatic shift in the culture of care for individuals with SMI, there was recognition that the implementation of change would not be quick or linear.
In anticipation of the many challenges associated with culturally transforming a large health care system, the VHA drafted a comprehensive handbook, the VHA Handbook 1109.01 (2008 Handbook), to uniformly guide the development and implementation of recovery-oriented mental health services (VHA, 2008). Since the publication of that report, mental health recovery concepts and services have been implemented in a broad range of VHA outpatient settings. However, one critical segment of the VHA mental health care continuum that remained qualitatively and substantively embedded in the traditional model of care was VHA psychiatric inpatient units, including this facility’s unit. A second handbook, the VHA Handbook 1160.06 (2013 Handbook), extended the principles outlined in the 2008 Handbook specific to psychiatric inpatient services, mandating essential components of inpatient recovery-oriented services (VHA, 2013).
Specific Aims
The purpose of this article is to describe an ongoing quality improvement implementation of recovery services in a VHA acute psychiatric inpatient unit. The factors involved in this quality improvement program will be described, along with a description of the intervention components, measures, impact, analysis, limitations and barriers encountered during implementation, and conclusions. SQUIRE 2.0 was used to frame the report of this quality improvement project (Ogrinc et al., 2016). This project demonstrates fidelity to both the broad transformation and specific directives of the 2008 Handbook and the 2013 Handbook. Adherence to the spirit and letter of the handbooks weave together to form the foundation of the unit’s cultural shift.
Available Knowledge
Given systematic reviews of the evidence and the VHA’s recommendation for implementation of Illness Management and Recovery (IMR); IMR content substantively informed this local curriculum development as a starting point (SAMSHA, 2009). Coauthors of this article have previously summarized evidence for IMR in a doctoral capstone project (Bartholomew & Zechner, 2014; Gilbride et al., 2014; Koval et al., 2016; McQuire et al., 2014; Saylers, Godfrey, et al., 2009; Saylers, Hicks, et al., 2009). However, there is little research or quality improvement reports on implementation of IMR or other evidence-based recovery-oriented services targeting Veterans during inpatient stays (McQuire et al., 2015; McQuire, White, White, & Salyers, 2013).
Rationale
SAMHSA’s (2004) framework of mental health recovery served as a conceptual basis for this program. SAMHSA defines mental health recovery as the process of change through which individuals improve health and wellness, live a self-directed life, and strive to reach their full potential through 10 principles of recovery: self-direction, person-centered, empowerment, holistic, nonlinear, strength-based, peer support, respect, responsibility, and hope. Notably, these mental health recovery concepts/principles seamlessly complement broader VHA initiatives, such as the goal of developing a positive service culture and building new partnerships (VHA, 2014a, 2016b, 2016b; VHA, Office of Research and Development, Quality Enhancement Research Initiative, 2013). Given the evidence for positive impacts of recovery-oriented services in outpatient settings, it is reasonable to assume it will have positive impacts in inpatient settings. In addition, professional expertise and empirical evidence also contributed to embracing the recovery model on this inpatient psychiatric unit (McQuire et al., 2014).
Context
In addition to establishing certain psychosocial rehabilitation programs, the 2008 Handbook emphasized implementation of evidenced-based therapies targeting individuals with SMI and psychiatric comorbidities and directed sensitivity to gender-based mental health issues (VHA, 2008). To facilitate these outcomes, the 2008 Handbook specified the need for specific positions at each VHA medical center (VAMC), including a Local Recovery Coordinator (LRC). Furthermore, medical center leadership was charged with ensuring that mental health services support and actively facilitate recovery, as well as build Veterans’ resilience to life’s challenges.
The 2013 Handbook specified uniform actions for inpatient mental health services (VHA, 2013). Leadership was charged with transforming inpatient psychiatric units, which entailed the development of a healing and recovery-focused inpatient environment including the following components: (a) implementation of mental health recovery-oriented programming (4-6 hours per day); (b) emphasis on interprofessional care approaches; (c) provision of evidenced-based programming; and (d) delivery of consistent programming across facility settings.
Setting
This VHA inpatient program is a 24-bed, locked unit that serves Veteran patients (hereafter referred to as Veterans), many of whom who are homeless, reside in transitional housing or rural areas, experience significant psychiatric comorbidity, are under commitment orders, and/or are medically complex. The average length of stay is 7 to 9 days. The mental health service at this medical center ranks high in overall ratings of quality and efficiency in comparison with all VAMC mental health services (U.S. Department of Veterans Affairs, Veterans Health Administration, 2014c).
Intervention
In chronological order of development, the critical components of the recovery-oriented inpatient program involved the following: development of Interprofessional Recovery Committee (IRC), creation of vision and mission statements, education of staff, integration of the Peer Support Specialist (Peer Specialist) role, development and delivery of recovery-oriented curriculum, development of the interprofessional program partnership, adoption of the Veteran’s Recovery Self-Help Resource Book [Resource Book] and Veteran’s Recovery Worksheet [Worksheet], and development of program evaluation.
Inpatient Recovery Committee (IRC)
Reflective of the broader principles, processes, and procedures underpinning the development and implementation of the recovery effort, an IRC was developed, consisting of an interprofessional group: Peer Specialist, medical director, nurse managers, psychiatric mental health nursing (PMHNP) residency director and residents, milieu staff, psychologists (including the facility’s LRC and Inpatient Recovery Coordinator), volunteers, and researchers. The IRC provided the overall implementation strategy for this effort including planning, coordination, mentoring and training, monitoring, and evaluation. The committee is led by the LRC, who serves in a unique position within VAMCs as a consultant to mental health senior leadership and to all programs in the mental health service line pursuant to the requirements and recommendations set forth in the inpatient 2013 Handbook. With feedback from current and former Veterans treated on the acute psychiatric unit and from milieu staff, the IRC developed a new Vision and Mission for the inpatient recovery services (Table 1).
Vision and Mission.
Staff Education
Education of milieu staff is one critical component of cultural change. To be effective, delivery must target evidence-based education as exemplified by this IPC’s adoption of the American Psychiatric Nursing Recovery-to-Practice (RTP) program (American Psychiatric Nurses Association, 2015; Stuart, Tondora, & Hoge, 2004). The RTP is a 6-module course that facilitates change in psychiatric–mental health nursing practice. While targeted for inpatient mental health nurses, the content is appropriate for interprofessional staff delivering recovery-oriented care for individuals with SMI. PMHNP residents completed the RTP facilitator training and, along with the LRC, provided training for milieu staff and outpatient providers in the early program development.
The recovery-oriented training presentations were also posted on the department share drive for continuous access, given that training is an ongoing process, and milieu staff turnover rates are anticipated. Milieu staff are now currently trained and mentored by the LRC and nurse managers. The training targets the history of recovery-oriented practice, the dimensions and principles of mental health recovery, and the utilization of recovery-oriented language during care delivery (e.g., shift reports, communications with the Veterans). Although not formally a part of the inpatient recovery effort, a 30-minute recovery-focused Introduction to Mental Illness course was also added to the facility’s new employee orientation in 2015. Collectively, these training efforts are anticipated to promote recovery principles and practice moving forward and outward throughout the system as new professionals and staff enter the system of care.
Integration of Peer Support Specialists
There are currently 13 certified Peer Support Specialists working in this mental health service, all of whom are Veterans, with one dedicated to the inpatient psychiatric unit. Peer Support Specialists are like every other staff member from an organizational perspective but are valuably distinguished by their lived experience with a psychiatric diagnosis and their own journey of recovery (Davidson, Bellamy, Guy, & Miller, 2012). They are certified in mental health and substance abuse treatment and recovery-oriented practices by VHA-recognized entities (Carlson, 2015). Functionally, Peer Support Specialists serve as role models by sharing their personal recovery stories that manifest hope that recovery from mental illness is distinctly possible, as well as assist in processes to eliminate the stigma of mental illness. The dedicated inpatient Peer Specialist provides Illness Management and Recovery, wellness, and social skills groups and assists Veterans in achieving their recovery goals (SC Department of Mental Health, 2009; Chinman, Henze, & Sween, n.d.).
Recovery-Oriented Curriculum for Veterans
IMR content substantively informed the local curriculum development. However, there was a perception among the IRC members that the Veterans’ recovery needs would only be partially addressed by using standard recovery-oriented, evidence-based therapies. In the context of the guiding framework of improving health/wellness, fostering self-direction, and facilitating self-potential, the IRC generated a list of population-related variables associated with Veterans hospitalized on the acute psychiatric unit. Rapidly apparent was the need for curriculum designed to address basic health/wellness care, such as diabetes, dental care, basic first-aid, exercise, and smoking cessation. Second, we identified a host of psychosocial-related challenges and needs, including unemployment, violent crime victimization, family issues, access to federal benefits, finances, and navigation of the VA facility. Third, we identified existential issues of the Veterans, such as a poor sense of belonging and lack of meaningfulness. Last, interlaced with all the above, stigma was identified as a significant barrier to mental health recovery.
Partnership for Wellness
In addressing gaps and barriers in recovery care, the IRC considered the needs of this facility’s Veteran population, using a bottom-up approach that incorporated ideas from disciplines outside of mental health. The IRC also reasoned that direct, repetitive, and predictable contact, occurring in a helpful venue, would be essential to countering stigma in staff outside of mental health services. This contact would involve those who typically do not have professional interactions with Veterans in acute psychiatric distress.
Borrowing a page from the handbook on employment, the Recovery Coordinators personally visited medical center chiefs, nurse educators, managers, coordinators, and other professionals throughout this VHA facility (VHA, 2011). Discussions centered on an opportunity to make a positive difference in the lives of Veterans admitted to the acute psychiatric unit. Without exception, discussions were welcomed, requests for volunteers were distributed, staff throughout the medical center stepped forward, and Veteran needs were matched with staff talents.
Mindful of providers’ official duties and responsibilities, a monthly unit schedule was developed. Potential psychological- and perceptual-based barriers concerning lack of familiarity with the unit and safety concerns were addressed through compassionate discussion, direct pairing group of facilitators with an IRC member for the first inpatient encounter, additional guidance, and immediate feedback in support of interprofessional medical center staff and outside volunteer group leaders.
To further address the variables and needs of the Veteran population, the IRC implemented traditional mental health provider/facilitator-led programming. This recovery-oriented programming (4-6 hours per day) included four categories of groups: (a) Illness Management and Recovery, (b) Wellness/Health Psychoeducation, (c) Resource Access/Utilization, and (d) Community Reintegration/Recreation.
Finally, the IRC maintained that additional program components were required to counter the stigma that surrounds individuals with mental illness. Specifically, the IRC wanted to ensure that all programmatic services and materials were marked by impartiality, respect, and dignity. Furthermore, the IRC reasoned that stigma could be additionally attenuated by integrating professionals from other departments (outside mental health services) of the medical center in the benevolent pursuit of teaching life skills. To this end, group leaders repeatedly reported deeply valued experiences and reactions, such as being able “to give back” and “do the right thing,” “I guess I didn’t really understand that these are people too,” and “it is the highlight of my month.”
Veteran’s Recovery Self-Help Resource Book and Worksheet
The IRC supplemented face-to-face groups/activities with a Resource Book, a 38-page document adapted by the LRC and a PMHNP resident from a workbook developed by a VHA workgroup and the SAMHSA model of recovery care described in the Rationale section of this article (Aiyappan, Belmore, & Dyer, 2014; SAMHSA, n.d.). Notably, the local distillation process was collective and inclusive, incorporating both Veteran and interprofessional input. The Resource Book includes four sections: Highlights of Inpatient Recovery Unit, Philosophy of Recovery-oriented Care, Understanding Your Treatment Program, and Recovery Self-Help Resources, with 15 subsections including such topics as acknowledging and affirming strengths, recovery goals, and daily goals.
With the goals of solidifying gains made during the Veteran’s inpatient stay and ensuring continuity of care, a Recovery Worksheet was also developed and operationalized. The Recovery Worksheet in the form of both a hard copy for the Veteran and an electronic progress note containing space for free text and a templated script for each of the recovery principles (Koval et al., 2016; SAMSHA, 2004). Operationally, the Peer Specialist meets individually with every Veteran nearing discharge and collaboratively completes this note with the Veteran and then alerts are sent (through the electronic patient record) to the Veteran’s outpatient mental health provider. Outpatient providers were trained by a PMHNP resident on the Recovery Worksheet, the recovery progress note, and the incorporation of recovery into the Veteran’s outpatient care (Koval et al., 2016).
Summarily, the IRC perceived a convergence of issues: (a) Veteran needs driving program development (patient-centered care) and the human resources required for programming and (b) stigma can be addressed through mentoring and meaningful interpersonal exposure for staff and volunteers. It appeared that addressing the first issue (e.g., available professional resources) would simultaneously address the second (e.g., stigma). As such, this curriculum substantively exemplified a paradigmatic cultural shift to recovery and Veteran-centric–based culture by mitigating stigma through increased interpersonal experiences with group facilitators.
Study of the Intervention: Measures and Processes
Given the breadth and depth of this programming, the logistics needed to execute it required the IRC to continuously assess fidelity to content and adherence to the schedule/process, as well as monitor quality and relevance. The IRC developed an ongoing quality improvement evaluation process that yields both quantitative and qualitative data. We intended this process to be reinforcing and meaningful to facilitators. This evaluation targeted the following areas: Veteran, program, and system indicators (Table 2 summarizes the Quality Improvement Indicators):
Quality Improvement Indicators.
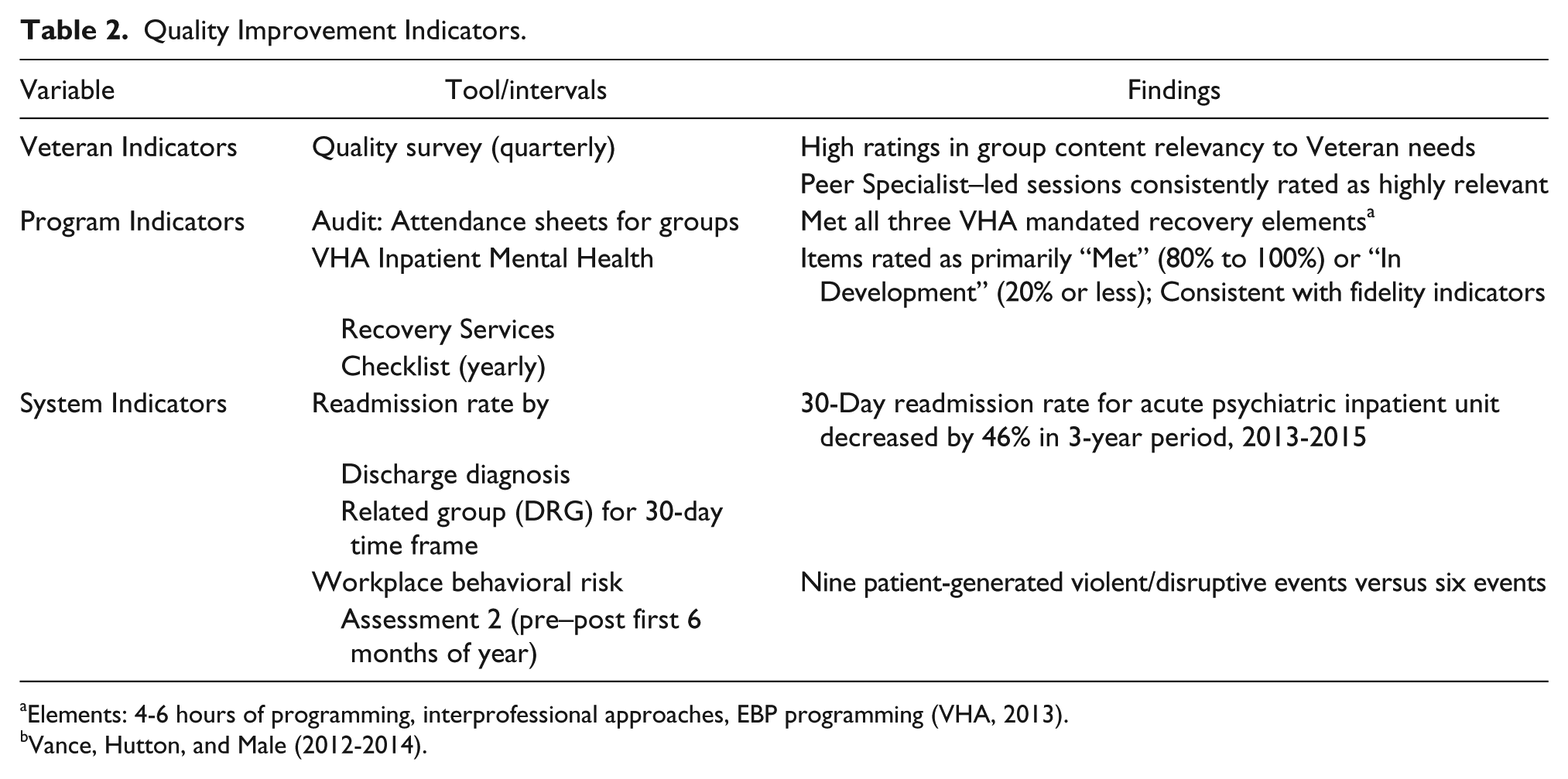
Elements: 4-6 hours of programming, interprofessional approaches, EBP programming (VHA, 2013).
Vance, Hutton, and Male (2012-2014).
Veteran Indicators
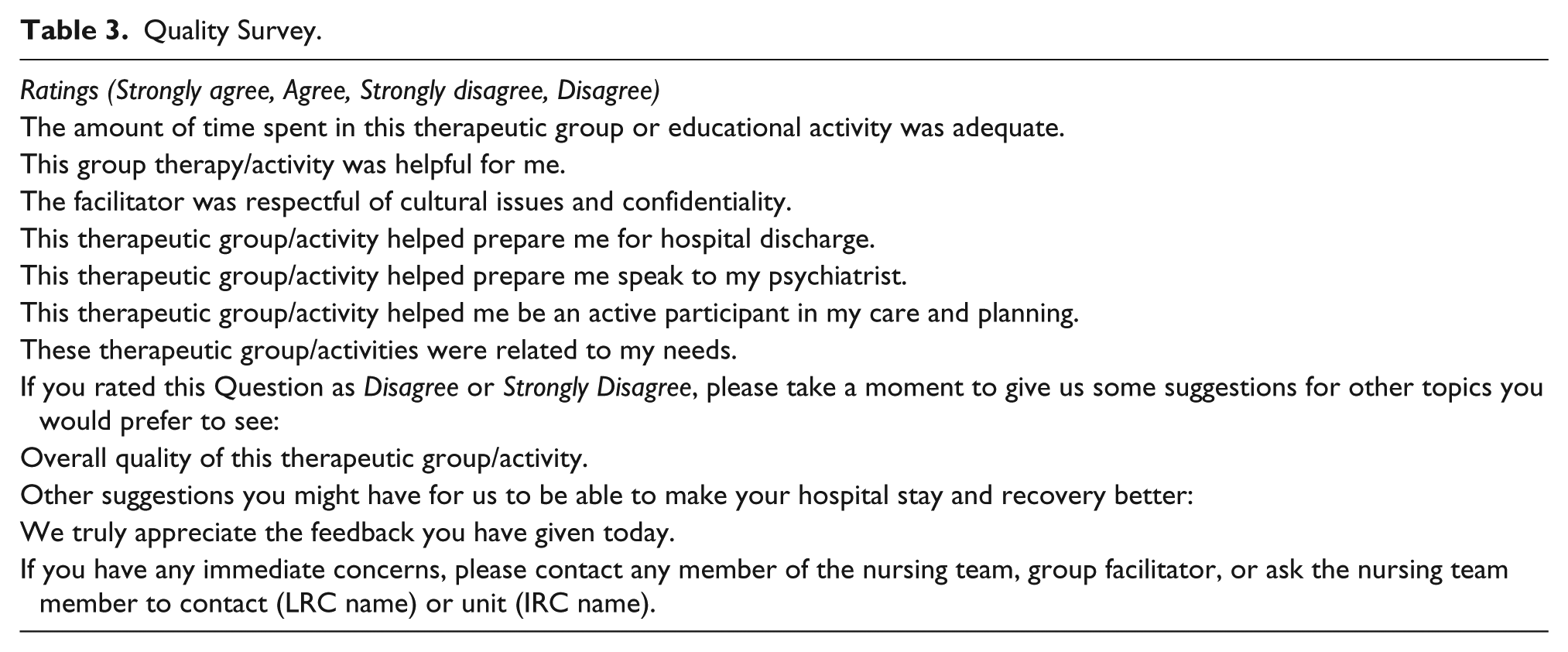
A participant review process is performed quarterly by the unit’s Peer Specialist who conducts a week-long audit of all programming through Veteran assessment using the site-specific Quality Survey (Table 3). Survey results are shared with all group facilitators and the IRC. These process measures allow the LRC to periodically meet with group/activity facilitators to review Veteran feedback, address any barriers, and, most important, provide an opportunity to express direct appreciation for the facilitator’s efforts (see Table 4).
Quality Survey.
Resources for Implementation of Inpatient Recovery-Oriented Services.
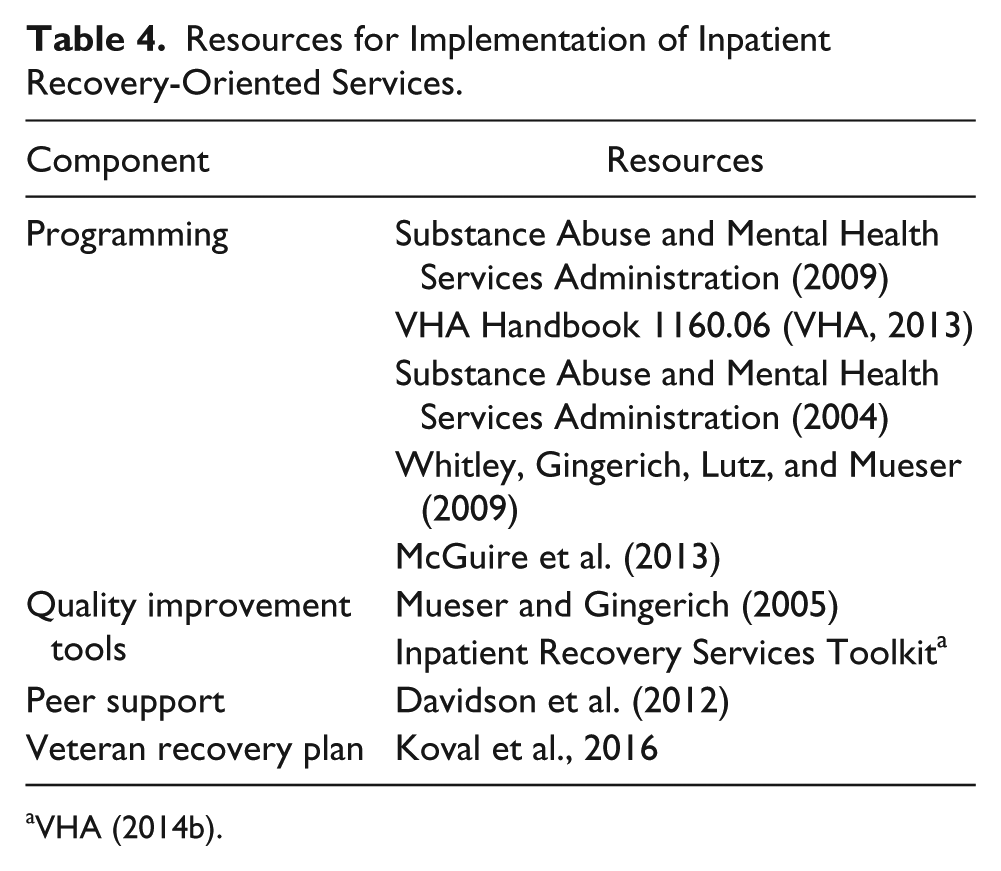
VHA (2014b).
Program Indicators
Audit-related processes were established that require attendance sheets indicating date/time, facilitator, and non-personal health information of attendees for all groups. Nursing staff maintains these data sheets in a secure log book in the nursing station.
The VHA Inpatient Mental Health Recovery Services Checklist (Checklist) was used to assess strengths and areas for potential improvement related to the components mandated in the inpatient recovery manual (VHA, 2013). There are four elements (20 items in total): (a) Organizational elements; (b) Individualized clinical, peer support services, spiritual treatment and engagement with clergy, evaluation and screening for VHA vocational rehabilitation); (c) Staff training and competency; and (d) Structural elements. Items are rated on the following scale: met, in development, not started. The Checklist is used by the IRC at yearly intervals to self-monitor for program fidelity and as a reporting tool. In addition, bimonthly IRC meetings address program revisions, barriers, and facilitators.
System Indicators
The total admission data were obtained through the VHA Support Services Center (VSSC). Information was gathered by searching the Clinical Care Program for the “Admissions, Discharges, and Transfers” report for the specific VAMC, then narrowing the search by month and year. VSSC was also used to obtain readmission data. The “Readmission Rate by Discharge Diagnosis Related Group (DRG) for Thirty Day Time Frame” report was used to gather information for the same VAMC and then narrowed by searching for the mental health DRG numeric groupings to separate mental health readmissions from other (e.g., medical or surgical) admissions in the same 30-day period. Searching for the month and year further narrowed this information (Koval et al., 2016).
Data of readmission percentages were compared before implementation of the recovery model (July to September 2013) to percentages of readmissions after implementation of the recovery model (July to September 2015). The VAMC’s patient flow team nurse manager tracked readmission data for medical diagnoses and assisted in readmission data collection for this project. No patient identifiers were used during any part of this quality improvement project (Koval et al., 2016).
Unique to the VHA, patient-generated violence/disruptive events are tracked by each facility via the Workplace Behavioral Risk Assessment (WBRA; Vance et al., 2012-2014). The WBRA is an internal data tracking tool to assist VAMCs in collecting and analyzing disruptive and violent behavior reports and to formulate a disruptive behavior risk metric for individual VAMCs. Disruptive behavior is operationally defined by the WBRA as behavior that is intimidating, threatening, dangerous, or that has, or could, jeopardize the health or safety of patients, employees, or individuals at the facility. The primary purpose for the WBRA is to inform the need for employee training in prevention and management of disruptive behavior in specific workplaces, such as inpatient psychiatry.
Results
Given the time lapse involved in this cultural transformation effort—nearly 3 years—its multifaceted nature, and the complexity of the independent variables, strong inference of causality between implementation efforts and outcomes are limited. Rather, as stated earlier, the primary scope and intent of this article is to share a comprehensive description of a cultural change process. Nevertheless, the authors have noted changes in various metrics monitored by the IRC over the period of this cultural change effort.
Veteran Indicators
Veteran feedback via post-group Quality Surveys collected from 2014 to 2017 indicates high ratings in group content relevancy to Veteran needs. In particular, the Peer Specialist–led sessions (primarily IMR and Wellness sessions) are consistently rated as being highly relevant by Veterans.
Program Indicators
This inpatient recovery program is consistent with the fidelity indicators set forth in the Checklist. The items were rated as primarily “Met” (80% to 100%) or “In Development” (20% or less) in yearly assessment (spring 2015-2017; VHA, 2014b). The checklist assisted in addressing organizational-level barriers and mapping of implementation strategies to performance improvement indicators. Most important, we have met three VHA-mandated elements of recovery-oriented care (4-6 hours of programming, interprofessional approaches, and EBP programming) relevant to the facility level (VHA, 2013).
System Indicators
Coauthors examined the likelihood that the recovery-oriented care affected the percentage of 30-day readmissions to the inpatient psychiatric unit. In July, August, and September of 2013, out of 191 overall admissions to the psychiatric unit, 25 were readmissions (13.1%). In the same 3-month segments in 2014, out of 166 admissions, 15 met the readmission criteria (9.0%; Koval et al., 2016). This represents an overall decrease in readmission percentage of 31.3% postrecovery implementation. Percentage of readmissions continued to decrease during those same months in 2015 as there were 136 total admissions during that quarter, only 10 of which were readmissions (7.4%). This represents another drop of 17.8% after implementation of the recovery cultural change efforts. This decrease was despite an outlier month in August of 2015 when there was a higher percentage of 30-day readmissions than in any month studied (7 readmissions out of 40 total admissions or 17.5%). In sum, during the 3-year period from 2013 through 2015, the 30-day readmission rate for the acute psychiatric inpatient unit decreased by 46%. Additionally, in the first 6 months of fiscal year 2014, there were nine patient-generated violent/disruptive events recorded whereas in the first 6 months of fiscal year 2015, there were five such incidents of disruptive behaviors.
Discussion and Lessons Learned
Success or failure of implementing recovery-oriented programs has been found to be associated with critical dimensions such as strong leadership, an organizational culture that embraces innovation, effective training, committed staff, close supervision, monitoring of program fidelity and outcomes, and a strong peer specialist program (Davidson et al., 2012; Mueser & Gingerich, 2005; Whitley et al., 2009). Strong leadership embraces the development and execution of policies and procedures fostering interprofessional collaboration, creativity, and ownership; support whole person care delivery programs; and psychoeducation of Veterans seeking care and their families (Tondora & Davidson, 2006).
All these dimensions characterize this mental health service and recovery program. These processes are all occurring within the context of a medical center with national leaders in mental health policy, funded mental health implementation research, strong academic partnerships, and interprofessional collaboration (Coxe et al, 2016). In addition, the Peer Specialist is highly valued by the Veterans, staff, and the IRC. These performance indicators are consistent with the literature on the positive systemic recovery-related effects associated with the use of Peer Support Specialists, such as engaging persons in care and decreasing hospitalizations (Davidson et al., 2012). Table 4 provides recommended resources for implementing inpatient recovery-oriented services.
Limitations and Barriers
The inpatient Handbook documents potential barriers to cultural transformation, such as (a) the severity of patients’ symptoms leads to a focus on stabilization, safety, and psychiatric/pharmaceutical interventions; (b) inpatient resources, staff, and staff training are insufficient to provide comprehensive recovery services; and (c) cultural transformation requires dedicated providers and immense resources (VHA, 2013).
Additionally, this unit has experienced severe milieu staff shortages, which not only limits their availability for training in recovery-oriented services but also limits their ability to use their recovery-oriented training in daily practice. Furthermore, weekend programming is a significant barrier, due to lower milieu staffing and absent interprofessional leaders. However, dedicated community-based volunteers have eagerly filled this void, including a local community art society teaching art classes, and a local blues music duet holding music sessions, where one patient joined in with his harmonica.
Also, the facility psychiatry residents and medical students have limited training in psychosocial interventions and recovery-oriented services; their curriculum tends to focus more on stabilization and psychopharmacology. Consequently, going forward, the need for recovery-oriented training of psychiatry residents and medical students is paramount. Finally, there are many other variables in the milieu that can affect recovery-oriented outcomes over time, including changes in providers and nursing-led efforts to address seclusion and restraint rates, and general ongoing evolution of traditional medical practice.
The coauthors have not established validity and reliability for this Quality Survey. In the next phase of the implementation, additional evaluation measures need to be included (Mueser & Gingerich, 2005). Consistent with measurement-based care, the coauthors are ready to employ a strategy that entails administration of a battery of brief, objective psychological instruments within 48 hours of intake and again within 24 hours of discharge. We anticipate that this battery of tests will inform the entire inpatient medical team as to areas of potential immediate focus, as well as inform discharge planning. We will accomplish this via the use of six Psychology Technicians who function under the supervision and training of the LRC. Furthermore, it is essential to capture information regarding any sustained changes post psychiatric inpatient discharge, and perhaps most important, any changes in the Veteran’s perception of hope and meaningfulness of life following psychiatric hospitalization.
Summary
This article reviews the developmental process over the initial 2 years of a quality improvement project targeting recovery-oriented inpatient services. The need for transformation of the inpatient culture was supported by policy reports, clinical frameworks, and specific policy directives. The components are described, including not only strong leadership and implementation of evidence-based programming but also an innovative hospital-wide partnership to address real-life challenges in the Veterans’ transition back to the community. Preliminary indicators of improvement, such as decreases in re-hospitalization, Veterans ratings of the program, and program fidelity, provide evidence of a success cultural transformation.
Conclusion
This psychiatric inpatient unit, as undoubtedly like many other inpatient units, has been gradually implementing elements of recovery-oriented care for many years. However, it was not until the paradigm shift in interprofessional collaborations, within the rubric of the VHA inpatient handbooks, that the “awakening” of this cultural transformation effort occurred. The famous French Chef, Paul Bocuse, was quoted as saying, “Without butter, without eggs, there is no reason to come to France”—an analog to butter and eggs are this facility’s dedicated and creative recovery-oriented practitioners, volunteers, structured program monitoring, and, most critically, the Veteran patients.
Footnotes
Acknowledgements
The authors acknowledge the leadership and support of Donald (Hugh) Myrick, MD, Acting Chief of Mental Health VISN7, Associate Chief of Staff, Mental Health Service; the Senior Executive Service; Service Chiefs including Edmund Lesinski, Chief, Community Engagement and Veteran Experience, Ralph H. Johnson (RHJ) VA Medical Center. In addition, the authors acknowledge the expertise and commitment of the Partnership for Wellness group leaders and the milieu staff, and the members of the Interprofessional Recovery Committee. Our committee is appreciative of the VA vision, directives, and resources related to recovery and the opportunity to partner with our Veterans living with mental illness to construct hopeful, fulfilling, and potentiated lives.
Author Roles
York and McDonagh: primary coauthors of drafts, interpretation of data.
McDonagh, Koval, Grubaugh, and York: data analysis.
Grubaugh, Koval, and Valvano: secondary coauthors, data acquisition.
Heran, Pelic (Christine), Pelic (Christopher), and Rhue: unit medical and nursing directors, contribution to concept and design, interpretation of data.
Heran, Grubaugh, and Valvano: critical revisions.
Wainwright: coauthor of Veteran Recovery Plan with Koval, IMR implementation, and Veteran Survey Analysis, data acquisition.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PMHNP Residency is supported by funding from the VHA Office of Academic Affiliations and the Ralph H. Johnson VA Medical Center.