
Abstract
Keywords
Introduction
In states across the country, the board of nursing or other administrative agency is charged with ensuring the nursing practice act is upheld by those possessing a registered nurse (RN) license (Russell, 2017). The board of nursing acts to enforce standards to ensure nurses are competent, provide care within the scope of practice, and are free from impairment due to substance use (SU), and thereby protect patients who receive nursing care. The rate of nurses’ SU is normative with the general population estimates of SU; that is, between 6% and 8% (Kunyk, 2015; Trinkoff, Eaton, & Anthony, 1991; Trinkoff & Storr, 1998; Trinkoff, Zhou, & Storr, 1999). When tracking such estimates, there are additional complexities to nurses who report SU, even when anonymity is assured, that may influence full disclosure. Specifically, nurses may fear SU disclosure could jeopardize their license and employment status, and therefore, their ability to earn a living. These hesitations are well-founded historically due to the “throw away” culture that permeated nurses when confronted with SU (Curtin, 1987). Today, due to the National Council of State Boards of Nursing (NCSBN) and industry partners, the alternative-to-discipline programs, which include nurse-accountability, the nurse may be given the option of a monitoring program versus employment termination (NCSBN, 2011).
Others argue, however, that SU in nurses continues to be surrounded by a discourse of “personal choice, as a failure of moral character” rather than a disease (Kunyk, Milner, & Overend, 2016, p. 315). When confronted with suspected SU and/or diversion, nurses will often be asked to submit a urine sample for SU screening. Often, policies in health care organizations require termination of employees who refuse to submit to such screenings. When a nurse is punitively discharged for refusing to submit to testing, it allows the individual, who may be impaired, to seek employment elsewhere, delaying treatment and continuing to practice, subsequently becoming a threat to public safety (Monroe & Kenaga, 2010).
In general, after a nurse is found to be impaired, stipulations for reentry into practice are typically required in alternative-to-discipline and monitoring programs. These include completion of SU treatment programs, restrictions in administering narcotics for a specified time period, restricted work hours (i.e., no overtime, no night shift work), limited work environments (i.e., no employment in hospice), mandatory and random drug screens, and attendance at support meetings (i.e., Alcoholics Anonymous); Monroe, Vandoren, Smith, Cole, & Kenaga, 2011). Nurses who seek reentry into practice and engage in such programs report stress from restricted practice and having to convince organizations to hire them, guilt and shame from the stigma of having a substance use disorder (SUD), gratitude for being caught from their addiction and being unable to rescue themselves, and keeping up with recovery, which includes self-care (Mumba, 2018).
In Indiana, the setting of the current study, nurses who self-report to the SU monitoring program, the Indiana State Nursing Assistance Program (ISNAP), are assured confidentiality. If the recovery monitoring agreement is not followed, however, and ISNAP closes the nurse’s file, then ISNAP notifies the Indiana State Board of Nursing (ISBN). At that point, the ISBN may order the nurse into the ISNAP program for further monitoring and disciplinary action. Two important distinctions should be made: Monitoring does not equal treatment for SU; and state statutes vary with regard to alternative-to-discipline programs. For example, the ISNAP program is not considered an alternative-to-discipline program in Indiana; rather, it is implemented as an assistance or monitoring program.
To ascertain an accurate description of nurses’ SU in the State of Indiana, we sought to expand our understanding of SU (including alcohol) in RNs through qualitative data collected via an online survey. We believe that this mode of data collection decreased factors, such as social desirability, and increased a sense of safety and anonymity in the disclosures forwarded by nurses who were experiencing SUDs as well as those peers who worked alongside them. We believe there is an interplay of individual, regulatory, organizational, criminal justice, and mental health/medical actors when understanding nurses’ experiences with SUDs (Foli, Reddick, Zhang, & Edwards, 2019).
Method
Study Design
The current study is part of an investigation of Indiana nurses (n = 1,478) focused on SU in nursing; additional findings have been and will be reported elsewhere (Foli et al., 2019). The online survey consisted of multiple single-item questions and validated tools, including measurement of the SU outcome variable via the WHO ASSIST (World Health Organization: The Alcohol, Smoking and Substance Involvement Screening Test; WHO ASSIST Working Group, 2002). At the end of the quantitative items, respondents were asked to “Please add any additional comments related to substance or alcohol use that you have experienced or witnessed in registered nurses.” Of the 1,478 nurses who completed the survey items, 373 (25%) provided comments to the question related to SU. The current study describes our analysis of these responses. The study received an expedited review and was approved by the Purdue University Institutional Review Board (IRB).
Participants/Sample
For our sample, we obtained the Indiana Licensed Registered Nurse database (N = 169,000 nurses holding an RN license) and performed stratified random selection based on year of licensing. First, we computed the proportion of each licensed-issued years (in 10-year increments) in the 169,000 RN database. Second, for our targeted, final sample of 4,000 nurses, we randomly selected nurses within each licensed-issued year group. For our 4,000 subjects, we selected 1,828 nurses within Group A (1-10 licensed-issued years), 796 within Group B (11-20 licensed-issued years), 688 within Group C (21-30 licensed-issued years), 468 within Group D (31-40 licensed-issued years), and 220 within Group E (>40 licensed-issued years).
Participants were incentivized with a $50 gift card (code) from Amazon. There was an interruption of 3 days in data collection due to our survey being “hacked” by individuals who generated multiple email addresses, thereby attempting to receive multiple gift cards. We paused the survey approximately 7 hours after realizing the issue and immediately notified the IRB. After the IRB approved the amendment to the study, we resumed data collection and stipulated that the nurse needed to contact the research team in order to receive a gift card code. When nurses emailed the research team member, there was a comparison check to determine whether the names (via the email address or signed emails) were included in our 4,000 sample of nurses (note that this check was disconnected from the respondents’ data). At this point, we encountered a second issue, wherein a subset of nurses had entered the study via a peer’s letter. When queried, the nurses admitted to having obtained study information from a peer/friend. Given that the nurses had completed the survey, we were obliged to remit gift cards to them. Of the total study sample (n = 1,478), this occurred approximately 297 times and may have minimally skewed the stratification of the sample. Table 1 presents the overall sample information, as well as comparisons between those nurses who contributed open-ended comments and those who did not on demographic and survey items. No significant differences in SU were found between those who contributed comments and those who did not.
Comparison Between Participants Who Did and Who Did Not Contribute to Open-Ended Responses Related to Substance Use.
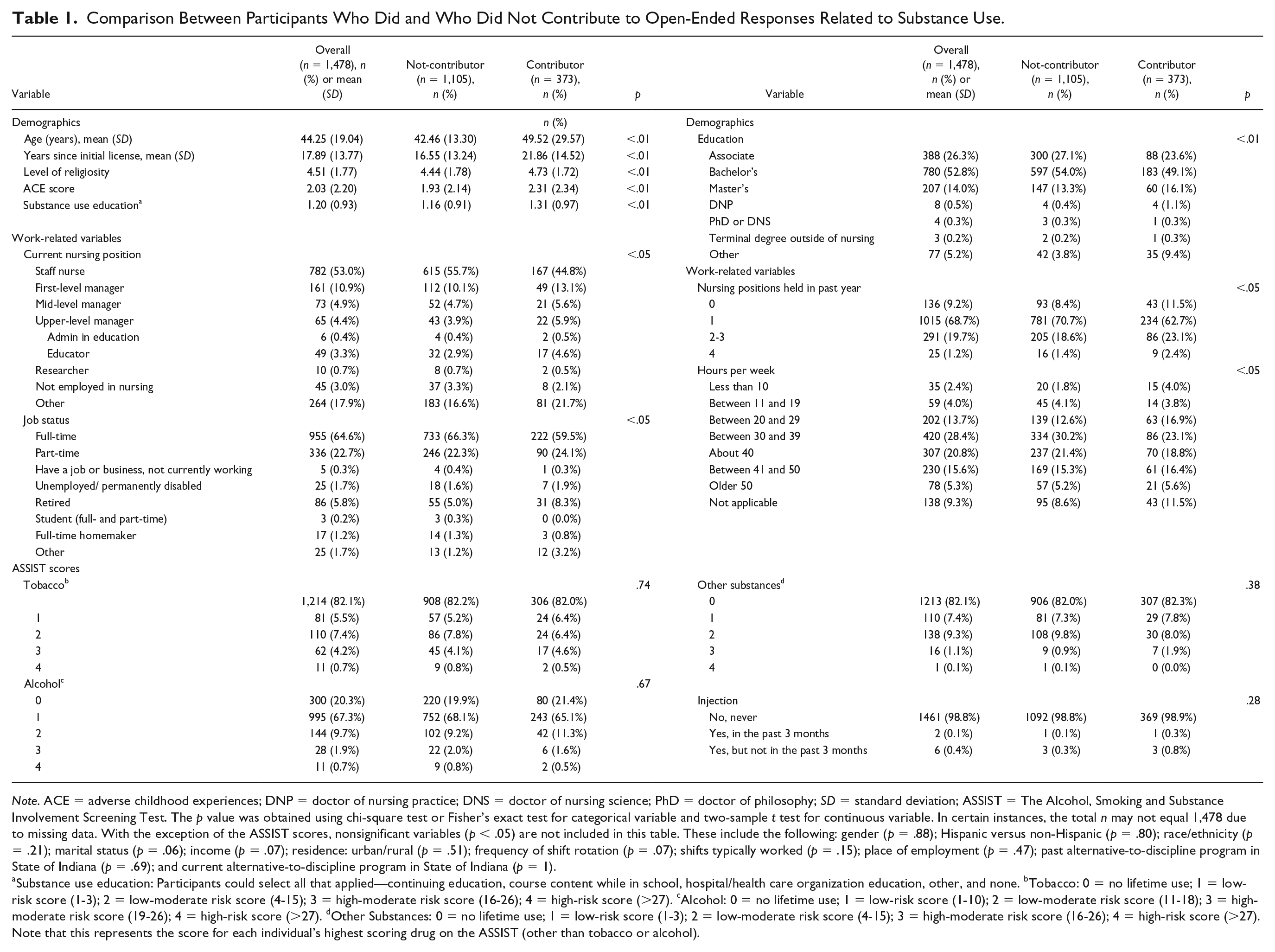
Note. ACE = adverse childhood experiences; DNP = doctor of nursing practice; DNS = doctor of nursing science; PhD = doctor of philosophy; SD = standard deviation; ASSIST = The Alcohol, Smoking and Substance Involvement Screening Test. The p value was obtained using chi-square test or Fisher’s exact test for categorical variable and two-sample t test for continuous variable. In certain instances, the total n may not equal 1,478 due to missing data. With the exception of the ASSIST scores, nonsignificant variables (p < .05) are not included in this table. These include the following: gender (p = .88); Hispanic versus non-Hispanic (p = .80); race/ethnicity (p = .21); marital status (p = .06); income (p = .07); residence: urban/rural (p = .51); frequency of shift rotation (p = .07); shifts typically worked (p = .15); place of employment (p = .47); past alternative-to-discipline program in State of Indiana (p = .69); and current alternative-to-discipline program in State of Indiana (p = 1).
Substance use education: Participants could select all that applied—continuing education, course content while in school, hospital/health care organization education, other, and none. bTobacco: 0 = no lifetime use; 1 = low-risk score (1-3); 2 = low-moderate risk score (4-15); 3 = high-moderate risk score (16-26); 4 = high-risk score (>27). cAlcohol: 0 = no lifetime use; 1 = low-risk score (1-10); 2 = low-moderate risk score (11-18); 3 = high-moderate risk score (19-26); 4 = high-risk score (>27). dOther Substances: 0 = no lifetime use; 1 = low-risk score (1-3); 2 = low-moderate risk score (4-15); 3 = high-moderate risk score (16-26); 4 = high-risk score (>27). Note that this represents the score for each individual’s highest scoring drug on the ASSIST (other than tobacco or alcohol).
Procedure
As email addresses were unavailable in the database, we used postal mail to send 4,000 letters to the sample and included a card with the study webpage address and the QR code linked directly to the online survey. One reminder postcard was mailed to all 4,000 nurses as we were unaware who had completed the survey due to the de-identification of response data. Our study webpage contained information about the purpose of the study, mental health resources, such as ISNAP, and the link to the online survey. Qualtrics software was used to house the survey and de-identified data. The IRB-approved consent was posted within the survey, after the welcome page, both of which included the principal investigator’s (PI’s) contact information. Documented consent was not collected due to the sensitive nature of the data; however, the participant clicked a radio button in the survey to indicate consent, and movement forward in the survey was contingent on this action.
Measures
WHO ASSIST
SU in RNs was measured using the WHO ASSIST (Version 3.0; WHO ASSIST Working Group, 2002), which is self-administered and designed to be used in research settings (Humeniuk, Dennington, & Ali, 2008; Humeniuk et al., 2008). The ASSIST is a well-validated, eight-item survey that identifies both lifetime and recent (within the past 3 months) use of substances across several categories: tobacco products, alcohol, cannabis, cocaine, amphetamine-type stimulants; sedatives and sleeping pills (including benzodiazepines), hallucinogens, inhalants, opioids, “other” drugs, as well as use of injection drugs. Due to the low reported use of some substances, we chose to measure the “other substances” using the highest scoring drug. Following the methods of Gelberg et al. (2015), “other substances” was defined by the score for the highest scoring drug category besides alcohol or tobacco. RNs were stratified into low risk (score 0-10 for alcohol; 0-3 for tobacco and other substances); low-moderate risk (score 11-18 for alcohol; 4-15 for tobacco and other substances); high-moderate risk (score 19-26 for alcohol; 16-26 for tobacco and other substances); and high risk (score >27 for alcohol, tobacco, and other substances).
Adverse Childhood Experiences
The Centers for Disease Control and Prevention—Kaiser Permanente Adverse Childhood Experiences (ACEs) study tool was used in the current study. The ACE tool comprises three domains: abuse, neglect, and household challenges. The ACE score is considered cumulative (dose-dependent): increasing scores have been linked to increased morbidity and decreased life span (Felitti et al., 1998). Specifically, the 10-item tool (score 0-10) assesses maltreatment and household dysfunction in the first 18 years of life (Felitti et al., 1998). Several states currently use the ACE add-on module as part of the Behavioral Risk Factor Surveillance System (Centers for Disease Control and Prevention, 2019). Merrick, Ford, Ports, and Guinn (2018), in the largest study to date (N = 214,157) with the most diverse sample, found that the most common ACE was emotional abuse and that ACEs were common across sociodemographic groups (61.55% of the individuals reported at least one ACE).
Data Analysis
Quantitative Analysis
As the objective of the current study was to explore nurses’ responses related to SU, we present descriptive statistics in Table 1 and comparison statistics (α = .05) of those nurses who offered comments and those who declined. The p value was obtained using chi-square test or Fisher’s exact test for categorical variables and two-sample t test for continuous variables. Of note is that the ASSIST (WHO ASSIST Working Group, 2002) survey responses indicate a very low rate of SU (self-report) and no statistical differences were found between contributors/noncontributors in SU (tobacco, alcohol, and other substances). However, as outlined in the results section, the qualitative analysis reveals themes that describe this phenomenon in nursing.
Variables that were found to differ between nurses who contributed and who did not contribute open-ended responses included the following: age, years since initial license, level of religiosity, amount of SU, education, current nursing position, job status, nursing positions held in past year, and hours worked per week. Of note is the significant difference between the two subsamples on ACE scores (Felitti et al., 1998) with those contributing responses reporting higher ACEs (p < .01).
Qualitative Analysis
A descriptive content analysis was undertaken for this study, following a process described by Elo and Kyngäs, 2008, Elo et al., 2014, and DeSantis and Ugarriza, 2000. From the responses recorded in and downloaded from Qualtrics, the coders, comprising the PI, a graduate research assistant, and an undergraduate student, first read the responses several times consciously avoiding premature closure or arriving at themes prior to considering all the passages. Field notes were taken based on reactions to the nurses’ responses. After careful and multiple readings, the team met to discuss overall impressions. After due consideration of the data were given, the team discussed findings related to patterns that had emerged and came to a consensus of themes. Iterations of the themes evolved with subsequent meetings until final themes were agreed on.
Trustworthiness was supported in each step of the data analysis process. First, in the preparation phase, we crafted our open-ended question in such a manner to allow the respondent to offer a wide variety of descriptions. We purposefully did not limit it to their personal experiences with SU and opened the experiences to more broadly encompass a lived experience surrounding substances. Stratified random sampling in the parent study allowed us to represent the larger population of RNs in the state. Second, in the organization phase, the three coders used printed copies of the documents to allow for conceptual tools, such as color coding of the responses. Multiple discussions of the temporal patterns, number of categories and concepts, and the order of the themes transpired. In the reporting phase, several iterations of final themes, supported by narratives, were reviewed. Frequency counts of primary and secondary reports of nurses’ SU were conducted and reported (Elo et al., 2014). Coders’ consensus was strong throughout the process; however, the PI was cognizant of power distributions and emphasized an openness to divergent ideas and analysis.
Results: Themes Related to SU in Nurses
Four themes emerged from the data (Table 2). Nurses were counted as contributors if they responded with an entry in the text field, including “no” or “no comment.” For the purposes of the data analysis, 287 1 nurses supplied comments that conveyed a message and could be interpreted thematically. The length of responses varied from several words or one sentence to half-page, single-spaced entries that detailed struggles with SU in themselves or peers. We have embedded direct, unedited quotes from the raw data to support the themes.
Themes Related to Substance Use in Nurses.
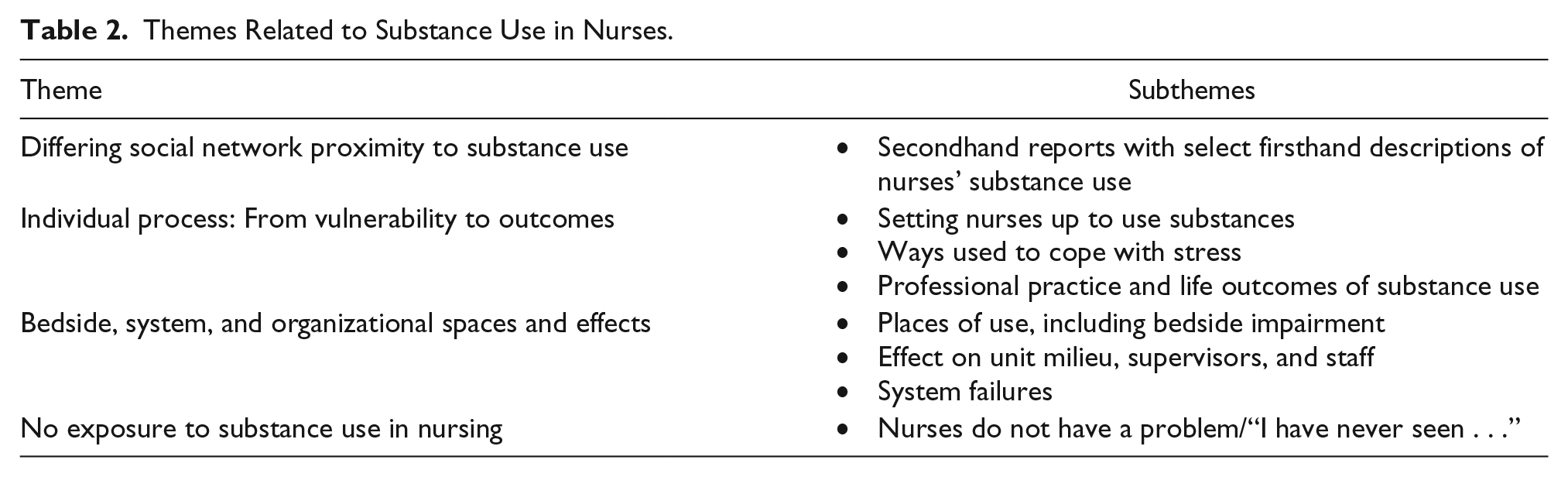
Theme 1: Differing Social Network Proximity to SU
In alignment with the quantitative findings of low-ASSIST scores (WHO ASSIST Working Group, 2002), most of the nurses’ comments were from a context of social network proximity—that is, reports of directly observed or awareness of SU in peers or associates (n = 250). In other words, they would often preface their entries by stating, “I heard of a nurse who . . .” or “I worked with a nurse who . . .” These accounts were most often detailed, lending trustworthiness to the data. One veteran nurse wrote, I worked with and had to be a witness to a peer who was stealing controlled substances from patients. I was also a victim of a different nurse while I was a patient in the ER and I was prescribed Demerol IV but got no pain relief. The nurse who cared for me was later sentenced to jail for stealing controlled substances.
However, 24 nurses described their own past (“clean and sober”) or current struggles with SUD. From the narrative below, the possibility of dual diagnoses is implied: Five years ago while I was in nursing, I realized that I had a drink problem. I sought help through AA [Alcoholics Anonymous] and have been sober from alcohol ever since. I struggle with temptation at times but for the most part I am able to function normally. My life has improved immensely since being sober, but I still deal with a lot of anxiety and depression. Much of it stems from feeling inadequate at my job and in my personal life. I go through bouts where I do well and then will have times maybe twice a year where I can barely get out of bed. It makes it challenging with my job and I am trying my best to keep m[y] job.
The entries are compelling and describe professional stress from being a nurse in today’s health care environment, which is emphasized in Theme 2.
Theme 2: Individual Process—From Vulnerability to Outcomes
As the narratives were examined, a second theme emerged that described how nurses are vulnerable due to family histories of SU, previous injuries, or using substances for medical use. Yet professional and job-related factors seem to create a “perfect storm” of vulnerability to SU. Threaded through the data, these job-related factors were increased stress, anxiety, depression, feeling inadequate at the job, heavy workloads with insufficient staffing, a lack of support, and workplace bullying. Furthermore, certain specialty areas, such as the emergency department and the intensive care unit (ICU), appear to add to nurses’ susceptibility. These environments typically are characterized by high stress levels and being exposed to traumatic experiences of patients and families, which may lead to nurses trying to cope with substances. Coping with secondary trauma through SU is described by this nurse: I started in an ICU as a new graduate RN and have worked in the critical care for my entire 10 year career. I have thought MANY times about leaving critical care, but have always stayed for fear of being bored and not feeling challenged in a less stressful, high-adrenaline, critical thinking dependent environment. For the first 5-6 years of my career I used alcohol as a coping mechanism for the trauma, death and dying I was experiencing at work. In the last 4-5 years I have grown in my maturity, emotional intelligence and coping skills and no longer use alcohol as a means of coping with the traumatic events I experience at work. I do, however, truly believe that the experiences bedside nursing staff live on a day to day basis can cause post-traumatic stress disorder (myself being one of them) and dependency on alcohol and drugs as a means of coping.
Specific vulnerabilities were also personal in nature: a family history of SU and previous injuries that required legitimate use of pain-relieving medications.
After a bad car accident many years ago I became dependent on opioid pain medication. It caused many problems for me. I no longer take these medications to control pain.
Nurses used different strategies to cope with the stressors they encountered. Several nurses described adaptive coping such as preemptively stopping or abstaining from SU because of a family history of addiction, pregnancy, and the responsibilities of being a parent and nurse. These nurses used yoga, diet, exercise, and spirituality to effectively cope. Former substance users indicated that they were “clean and sober now” through intentional efforts to remain so (i.e., attendance at Alcoholics Anonymous meetings).
I watched family members suffer from substance abuse and mental illness. I was a victim of their choices. I decided how not to be and work daily to avoid being/thinking like them even though I love them. It is difficult at times not to measure your own worth on others actions towards you. I have tried to educate myself so I could understand them instead of internalizing their behaviors.
However, there were nurses who maladaptively coped with stress through the use of alcohol and substances. Nurses’ descriptions surrounded the use of alcohol, although “pain killers,” sedatives, caffeine pills, and opioid diversions were also mentioned. Of importance are the clear narratives that link nurses’ use of alcohol to cope with the professional stress encountered as nurses. This nurse’s comments reflect this pattern seen multiple times in the data: The substance use seemed worse when I worked bedside. Most of the nurses I knew were on substances to reduce their anxiety, stress, depression. We regularly discussed it and regularly went out for drinks after work (and we worked night shift. So yes, we were going to breakfast and getting bloody Marys so we could go home and sleep). Some of us were taking Benadryl and Melatonin to help us sleep. Others were taking Xanax, valium, ambien or whatever else they could get their hands on. I would have gone the prescription drug route, but I was too afraid that I may like it and get addicted. Sometimes prescriptions were shared. If one nurse had a horrible shift, a nurse friend would give her a valium, Xanax, etc. so she could go home and sleep.
Although the results are inconclusive, select data appear to indicate that the use of alcohol to cope with professional stress may be an increasing problem in nursing.
When nurses use substances, there are professional practice and life outcomes that result. We divided these into negative and positive outcomes. Significant negative outcomes from the use of substances included the nurse electing to leave the organization prior to termination with no referral for assistance. This often occurred when the nurse was confronted with suspected use and requested to submit to a urine drug screen. Other nurses were terminated after the SU was discovered; this could include impairment while on duty or diversion activities. There were select nurses who had enrolled in ISNAP. However, some nurses were unsuccessful with monitoring agreements and began to use substances again. Other nurses were arrested, lost custody of children, divorced, and were incarcerated. The texts forwarded also indicated that suicide was an outcome of nurses’ SU: In the last 9 years I have known of 2 nurses (graduates of my university) who were arrested for drug theft and drug abuse at their place of work (hospital). One committed suicide. The other is in jail. Substance abuse is a real problem in our society. The immense stress nurses are under in the workplace puts them at risk . . .
Positive outcomes after the discovery of nurses’ SU was also found in the texts. Some nurses who had engaged with ISNAP had continued to practice or returned to practice successfully after monitoring agreements that included nurse accountability and subsequent treatment. Others received treatment through Alcoholics Anonymous or Narcotics Anonymous, support groups, and counseling: I have never experienced drug abuse. I do not do any type of drug. I have witnessed a co-worked be [sic] fired for taking medications that she stated she was giving to my patients on an oncology unit. She actually was injecting the medication into her arm. This was very disappointing. The nurse was very respected and had a very outgoing personality. The nurse went through the SNAPS (sic) program and is still working as a nurse. It is good to know that nurses are being given help and second chances.
This nurse also implies that there are effects on coworkers and organizational spaces when a nurse is found to be using substances and/or diverting medications from patients. This leads to the third theme identified in the data—the ripple effects caused by the individual who is using substances to those around them.
Theme 3: Bedside, System, and Organizational Spaces and Effects
The third theme approaches the phenomenon of SU within the context of patient care, system-level effects, and spaces beyond the individual nurse. Within the context of fellow care providers, several nurses reflected on how they felt after the nurse was discovered or how they felt being part of a unit with suspected diversion. The spaces of use included bedside impairment as this one nurse described: Worked with a nurse in Pediatric PACU (post-anesthesia care unit) at a large well known hospital and this nurse used pain medication meant for her pediatric patients and injected herself. She was noticed being slow to respond, falling asleep at her computer on multiple occasions.
Another nurse described the eventual outcome of a colleague’s impairment while on the job: Have worked with a nurse who would come to work on second shift smelling like alcohol, or would occasionally go to her vehicle for a “break.” She had also been investigated for “administering” narcotic medications to patients that did not typically take those medications and the patients denied receiving those medications. She was eventually escorted off the unit for a drug screen and was fired.
When a nurse is confronted or caught diverting and using substances, there is a cascade of effects on peers, supervisors, and the unit as a whole. The individuals who worked alongside the impaired nurse, as well as the middle manager, experience unanticipated and unpleasant ramifications when the nurse is confronted with SU as these two nurses attested: I had an employee once that received multiple prescriptions from multiple physicians in our practice. She also used alcohol excessively. This was quite draining on myself as a manager dealing with this issue and draining to staff who witnessed behaviors associated with her abuse. (Nurse X) I have worked at a couple [of] facilities where a nurse has come to work suspected to be impaired/under the influence of alcohol or drugs. It is stressful for the unit that day as well as the following weeks, not only because we are working short but because distrust for staff occurs. (Nurse Y)
Supervisors may be caught in the middle of social and political dynamics in an organization when addressing SU in an employee. They may be under censor and unable to disclose why a nurse has suddenly departed the unit: Two excellent PACU nurses that I supervised and I had only been at the facility for 3 months when I identified diversion of IV [intravenous] narcotics. One refused testing and was immediately terminated, the other agreed to testing and entered Rehab program. Other staff, surgeons, and anesthesia were very angry at me as these employees were now gone and it was my fault. I was unable to disclose reason for departure, and I was therefore labeled for next 8-10 months as a terrible manager, the work environment was quite difficult until I was able to “prove myself” to them as a knowledgeable, compassionate leader.
Nurses reported myriad emotions after learning about or reporting their colleague’s impairment: surprise/shock, stress, and relief after reporting diversion with a delay of action from supervisors. Nurses also reported altered perceptions of their colleagues, which reflected hidden stigma to SU (“she seemed so normal”) and sadness and grief.
I had to report a coworker after witnessing a morphine med discrepancy following observed changes in character like not being able to manage her patients/patient load well anymore. Also witnessed her suddenly become very sleepy on the job while recovering a surgical patient. She disappeared for a couple of hours and reappeared on the unit in a sleepy daze after waking up from a nap in an empty patient room. I had reported these observations to my nurse manager and director before the med discrepancy occurred. She was fired 6 days after the med discrepancy after refusing a drug test/paid leave of absence. She is currently on a paid leave of absence from her current employer and charges have been filed against her. . . . This whole situation has been difficult for me.
There were also patterns of responses that reflected system failures either in identifying and/or taking action when nurses were suspected of SU and/or diversion. Multiple accounts were offered that described how nurses would often quit or be terminated when requested to undergo a urine drug screen; thereby, exposing future patients and organizations to unsafe practices and delaying treatment for the nurse. A nurse recalled how a delay in administrative action continued to allow the nurse to practice without investigation: Despite nursing staff reporting possible theft and use of drugs or alcohol by their co-workers to Administration little investigation was done until the staff was so angry they were ready to call the State Board of Health themselves and risk being fired. The staff member was then investigated and the matter reported by Administration to the State Board of Health almost 2 years later.
When nurses are terminated or abruptly resign as a result of suspected SU, they seek employment elsewhere to sustain a livelihood and income to purchase substances. Long-term care facilities appear to be particularly vulnerable to nurses seeking employment after being confronted for SU issues in other facilities as these two nurses described: I was a witness in the past to an RN stealing meds from a patient at a long term care facility. She was terminated, but not reported. She has since been terminated from at least 3 other places, and still has her license. Unbelievable that no one turns her in to the State Board of Nursing.
Hiring nurses who may be impaired and seeking employment after working in and being discharged from an acute care facility may be exacerbated by the manpower shortage in long-term care facilities: Nursing homes will regularly discover the narcotic count is off and simply manually change it, allowing possible substance abuse to continue. Also, I have had aides that were insubordination and behaving strangely and I was told by my DON (director of nursing) that I could not drug test them because if they had to be sent home they had no other staff who would come in.
As described, refusal of drug testing often resulted in resignation or involuntary termination, no paths toward recovery, and continued impaired practice. In this comment, the nurse reflected on why nurses would defer receiving help when confronted with diversion: I have witness [sic] two episodes of diversion of medication. For both individuals, there was suspicious behavior, witnessed wastes, or missing medications; however, they both refused drug testing. Unfortunately, that leads to termination versus rehabilitation through ISNAP. I think it is the shame/guilt they feel that leads them to refuse admitting a very clear problem and forgoing their job altogether.
In sum, individuals and organizations are affected by nurses who use substances. Individual effects include sadness, stress, peer distrust, anger, hidden biases, and frustration. One nurse summed up system failures in this way: Have seen nurse be let go instead referred to get help. Not getting help does not stop the issue, the nurse can go elsewhere to work and continue the drug habit putting more patients at risk.
Hidden behind the impaired bedside caregiver are patient negligence and unsafe caregiving with system and organizational failures, which seem to only perpetuate the problem.
Theme 4: No Exposure to SU Issues in Nursing
Despite these reports, there were nurses who reported that they had neither been involved with nor witnessed others’ SU. Thirteen nurses explicitly stated that they had neither experienced nor witnessed SU within the profession, as described by this nurse: Thankfully, I have never had an issue with substance or alcohol abuse. I have never witnessed any abuse during my employment as an R.N. although I know that it is a problem.
An additional 83 nurses provided responses that were not included in the thematic analysis (“None”: n = 40; “N/A”: n = 39; “no comment”: n = 4). Given these comments, it is difficult to interpret whether these 83 nurses were validating no direct or indirect exposure to SU in nursing, whether they were unaware of the problem in the profession, or whether they chose not to describe a situation in detail.
Limitations
The study results are derived from nurses’ reports of peers’ and to a lesser extent, self-reports of the use of substances. Therefore, there is a question of whether these reports accurately describe this phenomenon. We assert, however, that the responses were detailed and reflect an affective impact on those responding to the question. The patterns within the descriptions were characterized by consistencies with strong coder consensus as themes emerged. Although the primary outcome variable, SU did not differ between those contributing comments and those who did not, additional variables were significantly different. These differences should be noted between the two subsamples of nurses. Last, the sample may have been skewed by nurses who shared their invitations to participate in the study with peers.
Implications for Practicing Nurses and Nurse Leaders
Our findings provide direction for nurses who work alongside those with SUDs or are experiencing SUDs themselves. First, interactions with and attitudes toward the individual nurse who is experiencing an SUD should be free from stigma. Several of the forwarded comments implied that the peer was surprised by the nurse who was using substances and contained judgmental connotations. We know health care professionals and nurses hold biases against patients with SUDs (Morgan, 2014; van Boekel, Brouwers, van Weeghel, & Garretsen, 2013); however, less is understood in terms of stigmas toward peers. Creating discourses that change shame and blame to trauma- and substance use–informed mental models of treatable diseases are necessary to shift the prevailing sense of stigma. Evidence exists that the dominant discourse of isolation and perceiving nurses with SUDs as separate from others prevails (Ross, Jakubec, Berry, & Smye, 2018). The dichotomy of what nurses know, epistemological knowledge, versus knowing self and aesthetic knowledge (Chinn & Kramer, 2015), should be part of the conversations in the health care workplace. The disconnect between the nurse understanding that SUDs are amenable to treatment and recovery is possible versus implicit or unconscious biases need to be addressed. The practice of supporting recovery efforts for nurses who are discovered to have SU issues involves not only the individual but the organizations in which nurses are employed.
Nurses are increasingly asked to work in challenging environments that place them in positions vulnerable to stress, psychological trauma, and violence. In addition to the data we have presented surrounding workplace conditions, Trinkoff, Zhou, Storr, and Soeken (2000) found associations between role strain, as measured by job demands and depressive symptoms, and SU in nurses. Peers and supervisors should maintain records of symptoms and behaviors, as well as resources, so that when, and if, confrontation occurs, there is supportive evidence with referrals to treatment available to help the nurse in recovery efforts. Middle and higher level managers should be thoroughly versed in organizational and state regulatory policies related to reporting nurses with suspected diversion and other activities related to SUDs. Managers need to listen to nurses who report peer’s suspected impairment and diversion and follow up in a systematic manner. Supervisors have the responsibility to understand their state’s board of nursing resources, such as alternative-to-discipline programs and the specifics of such programs. For example, how is confidentiality handled if the nurse self-reports and engages in a monitoring agreement? If a nurse decides to participate in the program, what disciplinary action(s) may be taken by the state board of nursing?
Orientation for all newly hired nurses as well as annual training for those in the organization should include an overview of organizational policies and recovery resources available to the nurse using substances. In this low-risk venue, the organization can communicate in a proactive way how supervisors, peers, and individuals can ensure patients are provided safe care and impaired individuals can be treated with compassion.
Due diligence in vetting employees by hiring managers is necessary to prevent those impaired nurses from skipping from one health care organization to another—and thereby, avoiding SU testing. This is particularly the case in long-term care facilities, where the availability of nursing staff is pressing. The hiring staff should investigate whether a complaint or disciplinary action has been taken against a nurse. For example, in Indiana, the Indiana Professional Licensing Agency (2019) search tool enables an individual to search by nurse license number to determine if previous disciplinary action has been taken and the status of the nurse license (i.e., probation or suspension). When a nurse license is entered, public documents attest to complaints and actions taken by the ISBN, in many cases related to SU. During hiring interviews, the interviewee may be asked about past performance and the terms of departure.
Implications for Education, Research, and Policy
Nurse educators have a responsibility to present information to students about the likelihood that they will interface with peers who may be dependent on substances. Targeted educational initiatives have been shown to be effective in influencing students’ SUD knowledge, skills, and attitudes (Stewart & Mueller, 2018). Moreover, educators should present information about ways nursing students and newly licensed nurses can positively cope with stress, psychological trauma, and exhaustion to avoid maladaptive coping through substances. While there are signs that a nurse may be impaired, those signs and symptoms may not be apparent. Our data indicate that when discovery of SU results in a nurse’s unexpected removal from patient care, the entire unit’s staff should be debriefed in a session that follows institutional policies and protects the suspected-impaired nurse’s confidential information. The interplay and tensions between human dynamics of addiction, legal implications of licensure, safe patient care, and peer relationships need to be recognized.
The American Nurses Association (ANA) supports legislation and initiatives toward healthy work environments and flexible, safe staffing levels (ANA, 2015). The ANA links safe staffing to decreased nurse fatigue and burnout and increased job satisfaction and retention (ANA, 2015). Our data provide preliminary support that substances, particularly alcohol, are being used as a way to cope with professional stress, which may be associated with staffing levels and resource allocations. Future research is needed to further explore this finding.
Increasing literature emphasizes the organization’s role in ensuring nurses with SUDs are treated with compassion as well as the stress inherent in the nurses’ roles (Kunyk et al., 2016; Ross et al., 2018). Regulatory actions taken by state boards of nursing assume the nurse is making choices surrounding addiction in a rational manner and that such actions will be effective in reducing substance usage (Kunyk et al., 2016). Again, the implicit bias toward moral character flaws rather than SUD seen as a treatable, chronic disease needs to be discussed in open, transparent ways. Reentry of the nurse in recovery should be supported by nurse managers who are willing to document monitoring agreements and reports, reduce or allow no overtime, and continue insurance so that the nurse may enter into treatment (Bettinardi-Angres & Garcia, 2015). One of three new priorities for 2019 to 2020 of the American Academy of Nursing is to “Reduce Patient, Provider, & System Burden.” The American Academy of Nursing (2019) policy priority states, “In order to achieve the goal of placing the patient at the center of care delivery, policies must equally support providers and systems” (n.p.). Supporting the nurse with an SUD, the peer, and the supervisor within various systems can be derived from this policy priority and expands the locus of control beyond the individual to the system level. This policy speaks to the duality of needs of patients and the nurses rendering care within a system context.
Discussion
In the current study, we revealed four themes related to SU in nurses: differing social network proximity to SU; an individual process, from vulnerability to outcomes; bedside, system, and organizational spaces and effects; and no exposure to SU in nursing. Firsthand accounts of personal SU, as well as nurses who reported experiences with SU in peers and associates, provided detailed descriptions with consistent themes threaded throughout the data. Certain clinical specialty areas either create an environment that places the nurse at risk for SU (e.g., ICU; Trinkoff & Storr, 1998) or being a repository for nurses seeking employment after leaving acute care (e.g., long-term care). Nurses who are impaired vary in presentation, from those with obvious symptoms, such as being in a daze or sleepiness, to those who were able to function without suspicious symptoms of SU. One novel finding from the data surrounds how nurses’ SU influences organizations and systems and, simultaneously, is influenced by such organizations and systems.
SU in nurses influence organizations and systems. Nurses’ termination or abrupt departure related to SU generates emotional and operational fallout. Organizational policies that require termination if drug screening is refused allows the nurse to continue to work in an unsafe manner, unsafe for the individual and patients. Also, peers, interdisciplinary team members, supervisors, and human resource representatives may be faced with questions surrounding the nurse’s departure. Peers may experience additional workloads and myriad emotional responses (e.g., relief, anger, sadness, guilt, and negative biases/stigma). Staff debriefings may be helpful in ascertaining what questions and concerns remain after the nurse’s departure. Debriefing models such as the critical incident stress management (Everly, Flannery, & Mitchell, 2000; Flannery & Everly, 2004) or the resilience in stressful events (Edrees et al., 2016) may be used to support staff; these models may be implemented based on the extent of the trauma/distress experienced by the peers of the nurse. To the extent possible and depending on the circumstances, the impaired nurses’ right to confidentiality must be honored. In alignment with the aim of providing safe, effective patient care, quality improvement projects may surround root cause analysis of how suspected diversion went unreported. The American Association of Nurse Anesthetists has developed a list of drug diversion prevention strategies (American Association of Nurse Anesthetists, 2016) that could be translated to other clinical areas to prevent diversion activities. The NCSBN (2019) offers a variety of educational resources for nurses and nurse managers, including a video and a guide for nurse managers.
Organizational and system factors influence nurses’ SU, factors that create stress and a need to cope with these stressors. Job-related factors were threaded through the data: increased stress, anxiety, depression, feeling inadequate at the job, heavy workloads with insufficient staffing, a lack of support, and workplace bullying. An inconclusive but, nonetheless, important finding is the apparent direct relationship between professional stress and increase SU in nurses. In an attempt to understand the lived experience of the nurse with SU addiction, Burton (2014) interviewed 14 nurses who were “addicted to substances” (p. 151). Themes such as guilt, shame and embarrassment, and poor coping were discovered and are in alignment with the current study findings. Yet there were novel findings uncovered by Burton (2014): Nurses felt a need to control their environment and a central belief that they were immune to becoming addicted. The need for control is often cited as an outcome of past trauma, and such control may be elusive in high-acuity specialty units, such as ICU.
While some nurses had reported SU in peers, others were taken by surprise. Cares, Pace, Denious, and Crane (2015) surveyed nurses who had been enrolled in a peer health assistance program. Findings from 302 anonymous surveys of nurses indicate that 48% had used drugs or alcohol at work, and more than 67% thought their problem could have been recognized sooner. Barriers to treatment included fear, embarrassment, and the threat of losing their license (Cares et al., 2015). Recognizing signs of impairment sooner was recommended by Cares et al. (2015). However, in the current study and in select cases, even when nurses reported suspected SU, system failures allowed nurses to continue to practice.
Conclusions
Nurses who use substances should be viewed as individuals with a chronic disease, which may be accompanied by dual diagnoses, such as a combination of depression, anxiety, and posttraumatic stress disorder. Organizations may need to assume culpability in producing environments that lend nurses susceptible to poor coping choices, such as the use of substances to offset stress. The peers and units where these nurses reside should also be viewed as affected by the nurses’ SU. Nurses’ SU must be in the context of a systems perspective; that is, in identification of impaired nurses, policies that support rapid intervention and support, including removal or limited practice, debriefing of peers and colleagues and open discussions of the impact to the unit, and diligent efforts to create an environment where nursing care is rendered with appropriate staffing, prevention of workplace violence, and supportive leadership.
Footnotes
Acknowledgements
Karen J. Foli would like to thank the nurses who contributed responses to the survey.
Author Roles
KJF and LZ conceived the study; KJF determined the methodology. KJF, LZ, and BR collected the data, and KJF, BR, and KK analyzed the data. KJF took the lead in writing and organizing the manuscript. LZ took the lead in preparing the comparator table with assistance from BR. All four authors reviewed the final manuscript before submitting for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Council of State Boards of Nursing, Center for Regulatory Excellence (Project: R101011).