
Abstract
Keywords
Introduction
More than 45,000 Americans over age 10 years died by suicide in 2016, making it the 10th leading cause of death in the United States (Centers for Disease Control and Prevention, 2018). Among adults who complete suicide, in the year prior to their death, approximately 20% to 25% have an emergency department (ED) visit for deliberate self-harm (Ahmedani et al., 2014; Ahmedani et al., 2015) and associated suicidality (hereafter referred to as DSH), which can include nonsuicidal self-injury. Because EDs are providing front-line suicide prevention services, improving the overall quality of ED mental health care for patients who present with DSH represents an opportunity to intervene with these high-risk patients. While previous studies have attempted to determine the quality of care in EDs for DSH patients, the literature is lacking in recent, U.S.-based research.
ED nursing managers were surveyed because of their broad knowledge of typical unit policies, practices, and staffing structure. In addition to providing management of frontline nurses, they also oversee the organizational structure of nursing treatment for DSH patients and are therefore well-positioned to shape the processes of care for these patients. Essential to improving this process is understanding the aspects of care that managers perceive as important to providing quality care, as well as the extent to which evidence-based practices (EBPs) have translated to the ED. For instance, after a DSH event, the provision of appropriate assessment and safety planning reduces risk for repeat DSH and suicide attempts (Boudreaux et al., 2016; Stanley et al., 2018). Safety planning is a brief behavioral intervention that can be performed by nurses in the ED that involves restricting access to lethal means, teaching coping skills, identifying a social and emergency network, and building motivation for continuing mental health treatment (Stanley et al., 2018). Despite the evidence supporting the efficacy of assessment and safety planning, it remains unknown how often these strategies are actually employed in EDs or the extent to which they improve the quality of care for DSH patients.
In order to assess the gap between research and practice in this area, a national survey of over 500 ED managers collected data on the extent to which EDs provide assessments, the elements of safety planning practices identified above, and mental health referrals on discharge. We then examined the extent to which implementation of these practices influenced ED nurse managers’ perceptions of the quality of care provided to DSH patients.
Methods
Between May 2017 and January 2018, we mailed an ED management of DSH survey to a random sample of 665 ED managers at hospitals with ≥5 self-harm visits in the prior year, as identified by national Medicaid claims data (Bridge et al., 2019). Deliberate self-harm was defined as an act of nonfatal self-poisoning or self-injury with or without suicidal intent (ICD-9: E950-E959). Although the survey was typically sent to ED nursing managers or directors, in some cases it was completed and returned by other hospital staff. Respondents were offered a $100 gift card in return for answering the survey, provided their hospital policy allowed for the acceptance of gifts. The response rate was 77.1% (n = 513). Voluntary completion of the survey constituted implied consent. The study was approved by the University of Pennsylvania Institutional Review Board.
The survey included components of two evidence-based interventions: The Patient Safety Screener (Boudreaux et al., 2016) and the Safety Planning Intervention, designated as a best practice by the Suicide Prevention Resource Center and American Foundation for Suicide Prevention (Stanley & Brown, 2012). Ten questions were used to understand how frequently each of these EBPs was used: “Never or rarely,” “Sometimes,” “Usually but not routinely,” and “On a routine basis.” These values were assigned a numeric scale of 0 to 3, with the possibility of another 0.5 added if the respondent reported use of a standardized template for the item in question (yes/no response). We created three subscales to assess the frequency with which “assessment” (3 questions), “safety planning” (6 questions), and “discharge planning” (1 question) were routinely provided to ED DSH patients. All of the assessment and discharge planning scores were dichotomized to represent the routine presence or absence of the practice using a cut-point of 2.5. For safety planning, scores were dichotomized using a cut-point of 2.0 since these (six) questions did not ask about the presence of a template. For all of the items, cut scores were set in order to delineate whether an ED was implementing a practice more often than not. The dependent variable of perceived quality of care was determined by a question that asked directors to “rate the overall quality of mental health care provided in your ED to DSH patients” given the options “poor,” “fair,” “good,” “very good,” and “excellent.” Perception of quality of care values were also assigned a scale of 1 to 5, with perception referring to the relatively subjective nature of the ratings.
Hospital Covariates
Given the research on perceived quality of care, mental health staffing levels were also included as a covariate (Innes, Morphet, O’Brien, & Munro, 2014). The survey asked about the availability of mental health professionals during various times—standard business hours, after standard business hours, on weekends, or not at all. EDs were considered “highly staffed” if they had either (a) mental health staff (adolescent and adult psychiatrists, psychologists, and psychiatric nurses) during and after standard weekday hours and on weekends or (b) a social worker during and after standard weekday hours and on weekends with a mental health staff member available at any of these times. Other structural characteristics were determined by linking survey data to the AHA hospital dataset and included hospital teaching status, urbanity (urban or rural), and hospital volume determined by dividing the survey responses to annual census into quartiles, with the mid-sized hospitals being the 25th to 75th percentiles (23,000 to 64,000; American Hospital Association, n.d.).
Analysis
A linear regression examined associations between the overall presence of the EBPs as independent variables and perceived quality of mental health care to DSH patients as the dependent variable, controlling for staffing status, hospital teaching status, size, and location. Survey weights were used to accommodate the sampling design that selected hospitals with probability proportional to their DSH patient volume and to produce representative estimates of the 2,228 EDs (weighted N) from which the random survey sample was drawn. All statistical analyses were conducted using SAS 9.4 (Cary, NC). Prior to commencing the study, a rigorous power analysis was conducted revealing that with our selected sample, we have 80% power with two-tailed test (α = .05) to detect effect sizes of Cohen’s d = 0.31.
Results
Nursing leadership contributed to the majority (78.4%) of the completed surveys; 59.8% of surveys were completed by only ED nursing directors or managers (n = 285) and 21.2% of surveys were completed by more than one individual in the ED (e.g., nursing director and social worker; of these, 88 of the 96 included nursing leadership). The remaining surveys were completed by ED medical directors (1.7%, n = 8); social workers (3.1%, n = 15); “others,” such as RNs or behavioral health directors (8.6%, n = 41); and 6.5% of respondents did not indicate their position (n = 31).
There was a broad distribution of characteristics of hospitals, in volume (26.5% low, 48.3% medium, and 23.5% high), urbanity (75.7% urban, 24.3% rural), teaching status (42.1% teaching, 57.9% nonteaching), and level of staffing (58.3% high staffed, 41.7% not high staffed). Frequency of routine provision of the examined EBPs was 69.1% for self-harm/suicide assessment, 50.1% for discharge planning care, and 46.0% for safety planning.
Approximately 8.5% of the ED directors rated the quality of their mental health care for DSH patients as “Poor,” 26.6% as “Fair,” 22.3% as “Good,” 33.0% as “Very Good,” and 9.6% as “Excellent,” for an overall mean quality rating of 3.09 (confidence interval = 2.96, 3.21). The unadjusted quality rating differed between routine and not-routine provision of discharge planning (3.45 vs. 2.72, p < .0001), self-harm assessment (3.17 vs. 2.88, p = .0470), and safety planning (3.45 vs. 2.72, p < .0001). The rating also differed between places with high and low mental health staffing levels (3.31 vs. 2.77, p < .0001) and teaching and nonteaching hospitals (3.31 vs. 2.92, p = .0025).
After controlling for hospital covariates, EDs that practiced routine discharge planning and safety planning were found to have a significantly higher quality rating (β = .488 and β = .736, respectively). High ED staffing levels and teaching status were also associated with higher quality ratings (β = .368, β = .319). In order to ensure that high mental health staffing levels were not driving the results, a sensitivity analysis was conducted. Excluding staffing levels did not change the original findings (Table 1).
Associations Between Selected Evidence-Based Mental Health Practices and Quality Rating by Emergency Department Directors (n = 513).
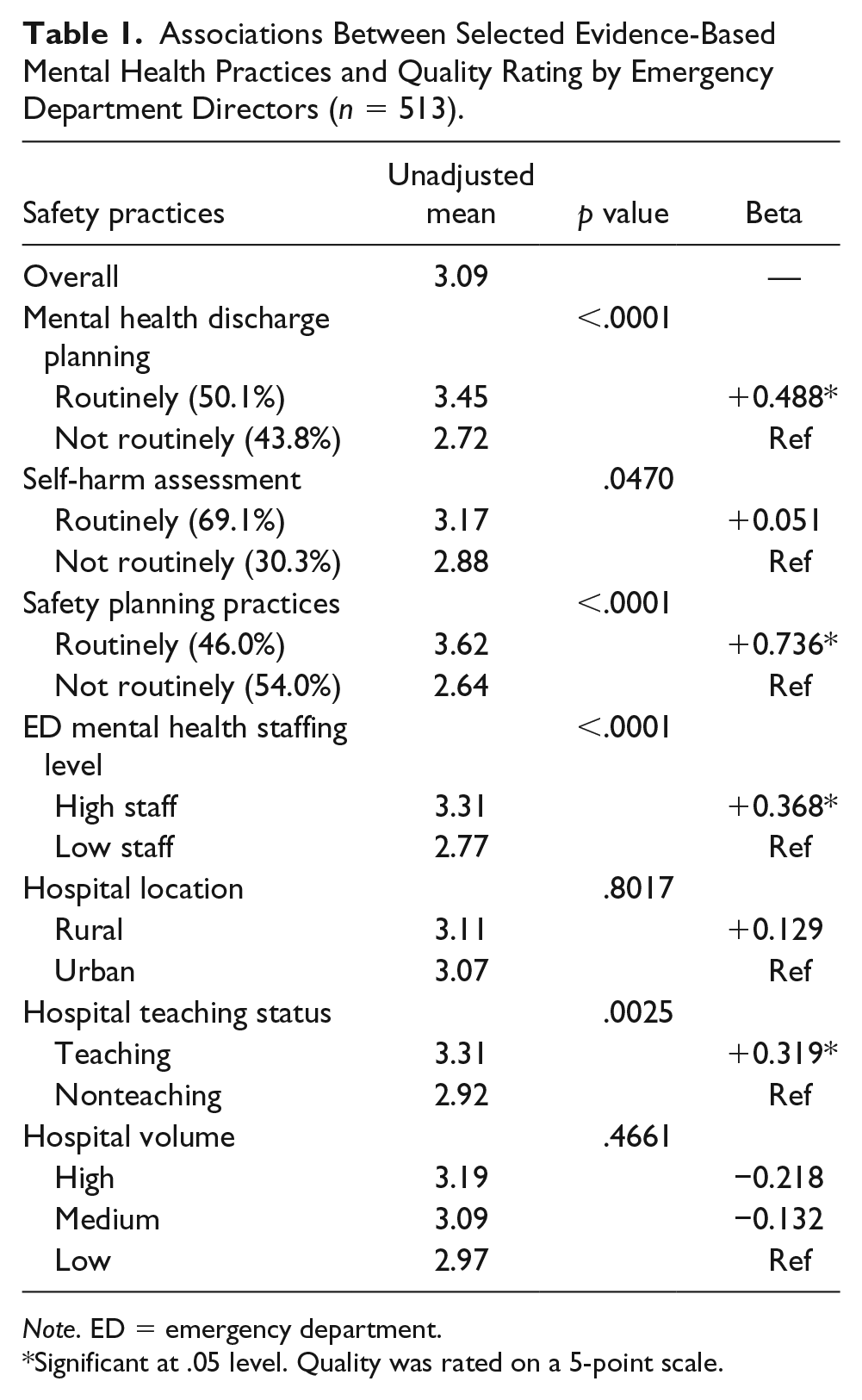
Note. ED = emergency department.
Significant at .05 level. Quality was rated on a 5-point scale.
Discussion
As compared with EDs that do not provide routine discharge planning and safety planning for DSH patients, EDs that routinely provide these services received significantly higher quality of care ratings from ED nursing leadership. More mental health staff support was also directly related to quality of mental health care ratings. However, routine assessment of DSH patients was not related to the quality of care ratings.
Given that higher levels of ED mental health staff and routine safety practices were associated with perceived quality of care suggests that ED leadership is well positioned to lead efforts to implement EBPs in the emergency mental health management of DSH patients. Unfortunately, many hospitals lack dedicated mental health staff in their EDs (Bridge et al., 2019) and hiring additional professionals may be cost prohibitive. Thus, future research should focus on ways to institutionalize staff training (including non–mental health staff) in safety planning and formalize linkages with outpatient services to ensure continuity of care, which together could improve the ED care for DSH patients while likely posing a lower burden on limited ED resources. In addition, drawing on techniques from implementation science (Williams, Glisson, Hemmelgarn, & Green, 2017) could provide an opportunity to engage leaders on incorporating these EBPs into practice at all EDs, with an eye toward customizing interventions that meet the specific needs of various types of hospitals, including underresourced and/or rural hospitals.
The findings offer an optimistic message that ED staff may be receptive to these strategies. There is always a concern that there may be a disconnect between research-based recommendations and the opinions of on-the-ground staff, but the fact that ED nurse managers reported that these evidence-supported practices were linked to favorable views of the quality of care for DSH patients is promising (Betz et al., 2013). Thus, nursing leaders may be well-poised to incorporate and teach EBPs to staff nurses and other ED staff using publicly available resources on assessment and safety planning, such as the recent National Association of State Mental Health Program Directors webinar on implementing safety planning 1 or the Suicide Prevention Resource Center’s Patient Safety Screener validated assessment tool. 2 These types of strategies which are available at little to no cost could be adopted by clinical staff even at the smallest, most rural, or resource-strained hospitals.
The study is limited in that despite a fairly high response rate (77.1%), there may nevertheless be nonresponse bias. While it may be considered a limitation that the study relied on self-report data, along with some subjective questions raising the possibility of response bias, this information also helps illuminate perceptions of ED leadership on the current quality of care provided for DSH patients. We also acknowledge that these findings are measuring perceptions (self-report) of the quality of the process rather than direct patient outcomes. Next, although survey development did not include formal item reliability testing, earlier versions were pilot tested with 22 respondents to improve item clarity. Finally, while responses were predominantly from nursing leadership whose perspective may differ from frontline nurses, they were targeted due to their knowledge and management of typical unit policies and practices.
ED managers are well positioned to influence and shape the processes of care that conform to their ideals of quality. These preliminary findings are promising in that they suggest that ED leaders are aware of the need for these changes. They also suggest that there may be a national institutional readiness for further implementation of EBPs for deliberate self-harm patients.
Footnotes
Author Roles
MO and SCM designed the study and obtained funding. AD, SWC, and SCM were responsible for acquiring data. AD performed the statistical design and drafted the article. All authors participated in the revision process.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Marcus reports receipt of consulting fees from Allergan, Alkermes, Johnson & Johnson, Sage, and Sunovion. No other disclosures were reported by other authors of the article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Grant R01-MH107452 from the National Institute of Mental Health (NIMH), National Institutes of Health (Marcus, Olfson, Multi-PIs).