
Abstract
BACKGROUND:
Restraint and seclusion in an inpatient child and adolescent psychiatric population adversely affects the overall value and safety of care. Due to adverse events, negative outcomes, and associated costs, inpatient psychiatric hospitals must strive to reduce and ultimately eliminate restraint and seclusion with innovative, data-driven approaches.
AIM:
To identify patterns of client characteristics that are associated with restraint and seclusion in an inpatient child and adolescent psychiatric population.
METHOD:
A machine learning application of fast-and-frugal tree modeling was used to analyze the sample.
RESULTS:
The need for restraint and seclusion were correctly predicted for 73% of clients at risk (sensitivity), and 76% of clients were correctly predicted as negative or low risk (specificity), for needing restraint and seclusion based on the following characteristics: having a disruptive mood dysregulation disorder and/or attention-deficit hyperactivity disorder diagnosis, being 12 years old or younger, and not having a depressive and/or bipolar disorder diagnosis.
CONCLUSIONS:
The client characteristics identified in the predictive algorithm should be reviewed on admission to recognize clients at risk for restraint and seclusion. For those at risk, interventions should be developed into an individualized client treatment plan to facilitate a proactive approach in preventing behavioral emergencies requiring restraint and seclusion.
Keywords
Background
Restraint and seclusion in an inpatient child and adolescent psychiatric population adversely affects the overall value and safety of care (American Psychiatric Nurses Association [APNA], 2018; Substance Abuse and Mental Health Services Administration [SAMHSA], 2011). Untoward outcomes have occurred when responding to behavioral emergencies with restraint and seclusion (Hert et al., 2011). All institutions that provide services to inpatient child and adolescent psychiatric populations must strive to reduce, with the intent to eliminate restraint and seclusion with innovative, data-driven methods.
Problem
With the growing evidence base in the literature, restraint and seclusion have been found to be far from therapeutic in many instances (APNA, 2018; World Health Organization, 2017), even causing adverse client outcomes (Ye et al., 2019). Psychiatric hospitals have long used restraint and seclusion as an intervention for maintaining safety during behavioral crises. Dating back to the 1800s, those in support of the Moral Treatment approach, including the leaders of this practice, French physician, Philippe Pinel, and English Quaker philanthropist, William Tuke, advocated for the elimination of restraint, as they deemed them immoral (APNA, 2018; Charland, 2015). The Moral Treatment approach focused on providing compassionate, humane care to those suffering from mental illness, with an additional emphasis on reducing inhumane interventions, such as restraints (Charland, 2015). Unfortunately, even though the elimination of restraints has been advocated for since the 1800s, the United States has not been able to accomplish that to date, as some believe they are a safety measure to prevent injury and decrease tension (APNA, 2018).
The research study’s organization has identified consistent excessive use of restraint and seclusion in their inpatient child and adolescent psychiatric population. There were no true patterns or trends identified in using restraint and seclusion in this population. Excessive use of restraint and seclusion in this population has led nurses to identify the need for further attention, awareness, and exploration as to the causes. As more evidence is realized around restraint and seclusion in this population, there is a growing body of literature that relate negative outcomes with use of restraint and seclusion.
A variety of adverse outcomes have been related to the use of restraint and seclusion. Some have included client injury, human rights violations, increased length of hospitalization, psychological trauma such as post-traumatic stress disorder, and staff injury, burnout, ethical dilemmas, and turnover, among others (American Nurses Association, 2012; APNA, 2018; Chien et al., 2005; Chieze, Hurst, Kaiser, & Sentissi, 2019; Kamel et al., 2007; SAMHSA, 2011; Unruh et al., 2007; Ye et al., 2019). Restraint and seclusion have proven to increase organizational costs, negatively influence the client experience (Chien et al., 2005; Kamel et al., 2007; SAMHSA, 2011), and cause an invisible impact on clients and organizations (Ye et al., 2019). The term invisible impact is used, as mental health professionals and organizations may not always be aware of the future impact that restraint and seclusion have on their clients or the magnitude of lost prospective clients due to reputation by word of mouth.
Clients have shared feelings of shame, guilt, and humiliation during and after being restrained and secluded (Larue et al., 2013). They have also identified psychological trauma and stress (Larue et al., 2013). Loss of autonomy also resonated with many clients, among other negative emotional states, such as rejection and fear (Ling et al., 2015). The invisible impact on clients has included long-term effects that developed following an episode of restraint and seclusion, such as retraumatization, lack of trust in health care professionals, and recurrent nightmares (Mohr & Pumariega, 2001). The invisible impact on organizations results from reputation by word of mouth from those who have experienced or witnessed others being restrained and secluded. This may result in reduced access to care if clients choose not to seek services. Lost income for facilities also may occur.
The emerging awareness of associated negative outcomes and costs have sparked the continued need to find innovative approaches to reduce and ultimately eliminate restraint and seclusion (APNA, 2018; Magnowski & Cleveland, 2019). However, before staff can identify escalation and provide early intervention, it would be most helpful to understand which clients are more at risk for restraint and seclusion to provide targeted assessment and monitoring (American Nurses Association, 2012). Targeted assessment and monitoring can better help staff prevent restraint and seclusion through increased structure, awareness, and individualized treatment plans.
A study conducted by Allen et al. (2020) found a statistically significant reduction in the duration of mechanical restraint episodes by implementing increased registered nurse assessment and surveillance. Their results highlight the importance of individualized client assessment and surveillance to improve outcomes associated with mechanical restraint. Although the goal on any acute care psychiatric unit is to prevent restraint and seclusion from occurring, but when prevention is not obtainable, minimizing the duration of restraint and seclusion should be the next focus and priority. Targeted and individualized assessment and monitoring of clients are needed to promote safety and ensure positive client outcomes.
This study seeks to identify which patterns of client characteristics are associated with restraint and seclusion in an inpatient child and adolescent psychiatric population.
Significance
The APNA (2018) recommends that psychiatric facilities reduce restraint and seclusion, with the long-term goal of elimination. The APNA (2018) suggests early identification and intervention of client escalation and aggression as an effective approach in preventing restraint and seclusion. Under most clinical circumstances, early identification and intervention of escalation and aggression can be achieved; however, there are times when escalation and aggression happen too rapidly in this population, leading to an immediate restraint and seclusion. If staff only focus on intervening at first signs of escalation, that sole approach does not provide an opportunity to identify those more at risk for escalation or aggression. Being able to identify clients at risk for restraint and seclusion assists staff in developing more individualized treatment interventions that may reduce the likelihood of a behavioral crisis.
Many factors have been identified in the literature as risks or even predictors of restraint and seclusion in the inpatient child and adolescent psychiatric population. The risk factors identified in this section reflect both restraint and seclusion. The primary identified antecedent to restraint and seclusion was aggression (Allen et al., 2014; Baeza et al., 2013; Dean et al., 2007; Delaney & Fogg, 2005; Hert et al., 2011; Valenkamp et al., 2014). Ultimately, the goal is to deescalate a client at the earliest signs of escalation and aggression to prevent restraint and seclusion from occurring. However, aggression can be hard to measure consistently and prior to escalation, as aggression can intensify so quickly that early identification and intervention are not always possible, and thus, restraint and seclusion are pursued.
Additionally, restraint and seclusion tend to be needed more on locked psychiatric units (Schneeberger et al., 2017), such as the units in this study. This, in part, can be contributed to the extent and frequency of aggression seen on locked, inpatient psychiatric units (Iozzino et al., 2015; Schneeberger et al., 2017). For example, Iozzino et al. (2015) identified that approximately one in five clients admitted to an inpatient psychiatric unit may demonstrate some type of aggression or violence. Other risks or predictors found in the literature included abuse and/or trauma history (Dean et al., 2008; Hammer et al., 2011), previous hospitalization (Baeza et al., 2013; Dean et al., 2008; Delaney & Fogg, 2005; Furre et al., 2017), the approximate age of around 13.9 years old (Dean, et al., 2008; Delaney & Fogg, 2005), diagnosis of mood disorder (Baeza et al., 2013; Dean et al., 2008), and more than one psychiatric diagnosis (Dean et al., 2008).
Currently, there is little evidence in the nursing literature identifying how predictive analytics, defined as using statistical modeling to estimate future outcomes, can aid in restraint and seclusion prevention and elimination. Incorporating a predictive analytics approach may be helpful in identifying clients who are more susceptible to restraint and seclusion based on their individual risk factors. Predictive analytics provide the ability for clinicians to identify clients who are more likely to have a specific treatment outcome, such as the need for restraint and seclusion, and thus, can provide valuable information to support decision making based on individual client characteristics (Van Calster et al., 2019). These predicted outcomes help provide information to make decisions with foresight instead of hindsight and help nurses identify those at risk for a specific outcome (Raab & Gigerenzer, 2015).
Early identification can be used to determine those at risk for being restrained and secluded from the application of a fast-and-frugal tree (FFT). Eliminating the use of restraint and seclusion may benefit clients and lower inpatient costs. Identifying which client factors, individually and/or combined, with help from an FFT, may be useful in mitigating the need for restraint and seclusion, and could prevent a behavioral emergency from occurring altogether. The research question is, “Which patterns of client characteristics are associated with restraint and seclusion in an inpatient child and adolescent psychiatric population?”
Method
Restraint is defined as any type of manual method, either physical or mechanical, that impairs or restricts a client’s ability to move his or her body or limbs freely (Centers for Medicare and Medicaid [CMS], 2008). Seclusion is defined as the “involuntary confinement of a client in a room or area from which the client is physically prevented from leaving” (CMS, 2008, p. 96). The rationale for combining both restraint and seclusion in this algorithm is based on the premise that the decision to use restraint and seclusion is dependent on the same guideline, active or imminent danger to self or others, stemming from a comprehensive individual client assessment (CMS, 2008). A client displaying active or imminent danger could progress to the need for restraint and seclusion depending on the individual nurse’s assessment and clinical judgment. In addition, from the literature reviewed and applied to this study, the search targeted both restraint and seclusion, versus restraint or seclusion individually.
Analysis
To estimate the predictive algorithm, the FFTrees package in R Statistics 3.5.1 was used; it implemented cost sensitivity within FFT model classification (Phillips et al., 2017, 2018; R Core Team, 2018). As stated earlier, data-driven methods must be deployed in the health care setting to reduce, with the intent to ultimately eliminate restraint and seclusion. Data-driven methods, such as FFTs, can help identify clients more at risk for certain events or outcomes (Raab & Gigerenzer, 2015), including the use of restraint and seclusion. This type of methodology, from a predictive standpoint, applied to the clinical setting is just starting to emerge. There are currently a limited number of studies that have focused on predictive factors for restraint and seclusion in this population (Hert et al., 2011).
An FFT is a machine learning algorithm that can be defined as a set of hierarchical rules for making decisions based on very little information. They are transparent strategies for binary decisions and can be easily implemented for real-world decision tasks. They are both prescriptive (how people ought to make decisions) and descriptive (how people do make decisions) in their nature. A relatively simple method for algorithmic prediction, FFTs emphasize both speed and frugality in classification. Speed refers to the mean number of basic operations used for classifying an individual point, and frugality is the mean number of cues (also referred to as aspects, nodes, dimensions, or features) used across objects for classification (Martignon et al., 2008). Cues are presented sequentially, and each cue in an FFT is a decision point based off exit conditions to make classifications, rather than classifying based on weighted nodes throughout a sprawling tree (Luan et al., 2011).
By definition, FFTs are decision trees that have m + 1 exit: one exit for each of the first m − 1 cues and two exits for the last cue, with exit conditions typically defined as if–then statements (Luan et al., 2011). To make classifications, FFTs check an object’s value on each cue to see if an exit condition has been met (i.e., having a decision made). If an exit condition has not been met, the FFT considers the subsequent cue and continues sequentially until an exit condition is satisfied. Relative to other models, FFTs have advantages in terms of frugality (due to their singular decision points), as well as comprehensibility since the decision points can be conveyed without in depth knowledge of the underlying process.
Often, a lack of transparency leads to resistance in utilizing models; this is minimized with FFT models (Luan et al., 2011). Important, simplicity does not necessitate lesser performance, as FFTs have been shown to be competitive with more complex models, such as logistic regressions and random forests, in terms of predictive ability for a binary class (Phillips et al., 2017). Due to the inherent simplicity and relatively strong predictive performance of an FFT, this method would provide the most utility for real-world clinical implementation. The algorithmic logic is clear and comprehensible, providing opportunity to check for theoretical soundness. Additionally, these simple decision trees are easily communicated to clinicians and direct caregivers.
Sample Data
The sample consisted of 1,437 inpatient children and adolescent clients discharged from Rogers Behavioral Health between January 1, 2019 and July 31, 2019. Rogers Behavioral Health is a private, not-for-profit, behavioral health organization, located in the Midwest. These encounters came from all three inpatient locations at Rogers Behavioral Health: Brown Deer (n = 483), Oconomowoc (n = 413), and West Allis (n = 541). At any given time, the Brown Deer location can have up to a total of 28 inpatient child and adolescent clients, 22 at Oconomowoc, and 22 at West Allis. The child and adolescent inpatient units were locked units. Typical admission criteria consisted of danger to self or others. Clients with potential active medical issues needed to obtain medical clearance prior to being admitted. The inpatient child and adolescent units define a child client between five and 12 years old and an adolescent client between 13 and 18 years old (18 years old only if still in high school).
The data used were retrospective and collected as part of the standard treatment process. There was no additional impact to clients in obtaining the discussed data. Research analyses were approved by the Rogers Behavioral Health Institutional Review Board.
After a thorough review of the literature, key variables were identified as potential risk factors for restraint and seclusion during an inpatient stay. These key variables included demographic factors, abuse history, and diagnoses, and provided the foundation for client characteristics to be considered in the algorithm (Baeza et al., 2013; Dean et al., 2008; Delaney & Fogg, 2005; Hammer et al., 2011). Independent variables were selected based on predictive factors outlined in the literature. The outcome identified which predictive factors (independent variables) were associated with restraint and seclusion (dependent variable). RS Occur was the dependent variable that identified whether a client was restrained and secluded during their hospitalization.
The following variables were input into the FFT algorithm as a pool for potential predictors:
Female flags the client if of biologic female gender
Age is years of the client
LOS is length of stay, calculated as number of days between admission and discharge for a client’s encounter
Daily Census is the average number of clients on a unit during a client’s stay
Additionally, flags were given for specific diagnoses suggested in the literature, including
PDD for pervasive developmental disorder
Autism for autism spectrum disorder
DMDD for disruptive mood dysregulation disorder
Anxiety for any anxiety disorder
ADHD for attention-deficit hyperactivity disorder
Mood Disorder for depressive and/or bipolar disorders
Sexual Abuse, Physical Abuse, and Emotional Abuse were flagged if the client reported a history of these abuses. Table 1 has basic summary statistics for these variables.
Sample Demographics.
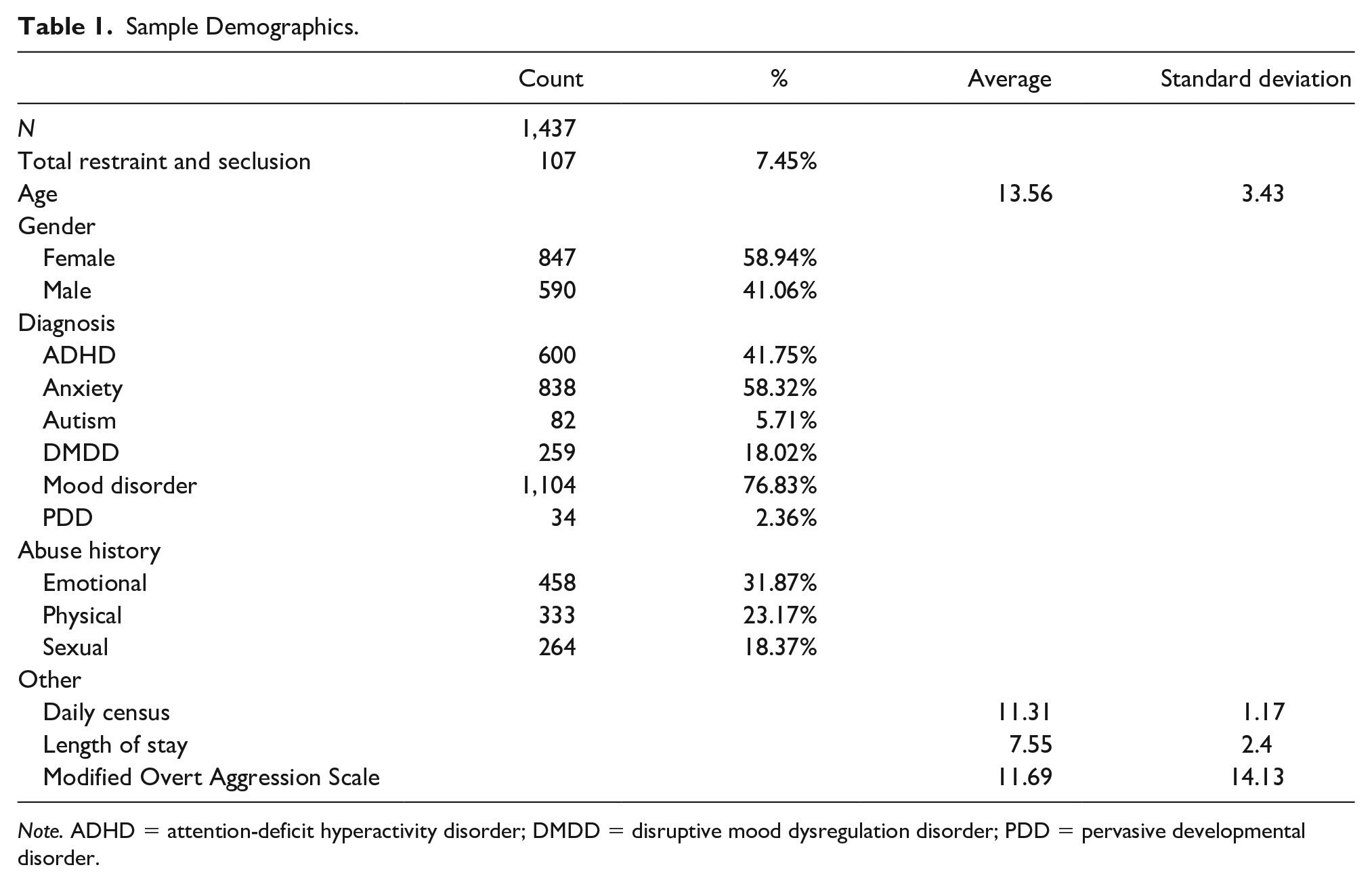
Note. ADHD = attention-deficit hyperactivity disorder; DMDD = disruptive mood dysregulation disorder; PDD = pervasive developmental disorder.
This algorithm will be implemented in inpatient settings primarily for quality care and safety purposes. The organization has identified potential risks of implementing this for quality purposes that are discussed below. There are no current anticipated risks of sharing this algorithm with the scientific community in a research publication.
In the future, when this algorithm is implemented into practice, the only foreseeable direct risk is that the algorithm will indicate that some clients are higher risk for restraint and seclusion than others. This could potentially lead to closer monitoring and quicker and/or more frequent interventions from staff for that client, while reducing monitoring and intervention for other clients. Additionally, there is a possibility for the algorithm to miss a client who is potentially high-risk; meaning, the risk level determined by the algorithm does not provide any additional benefit for that client. The benefits of leveraging data science to identify at risk clients, which might not have otherwise been identified as higher risk, outweigh these mentioned risks.
Results
The results section consists of the FFT algorithm and model performance and specification. Sample demographics are listed in Table 1. The FFT algorithm is shown in Figure 1.
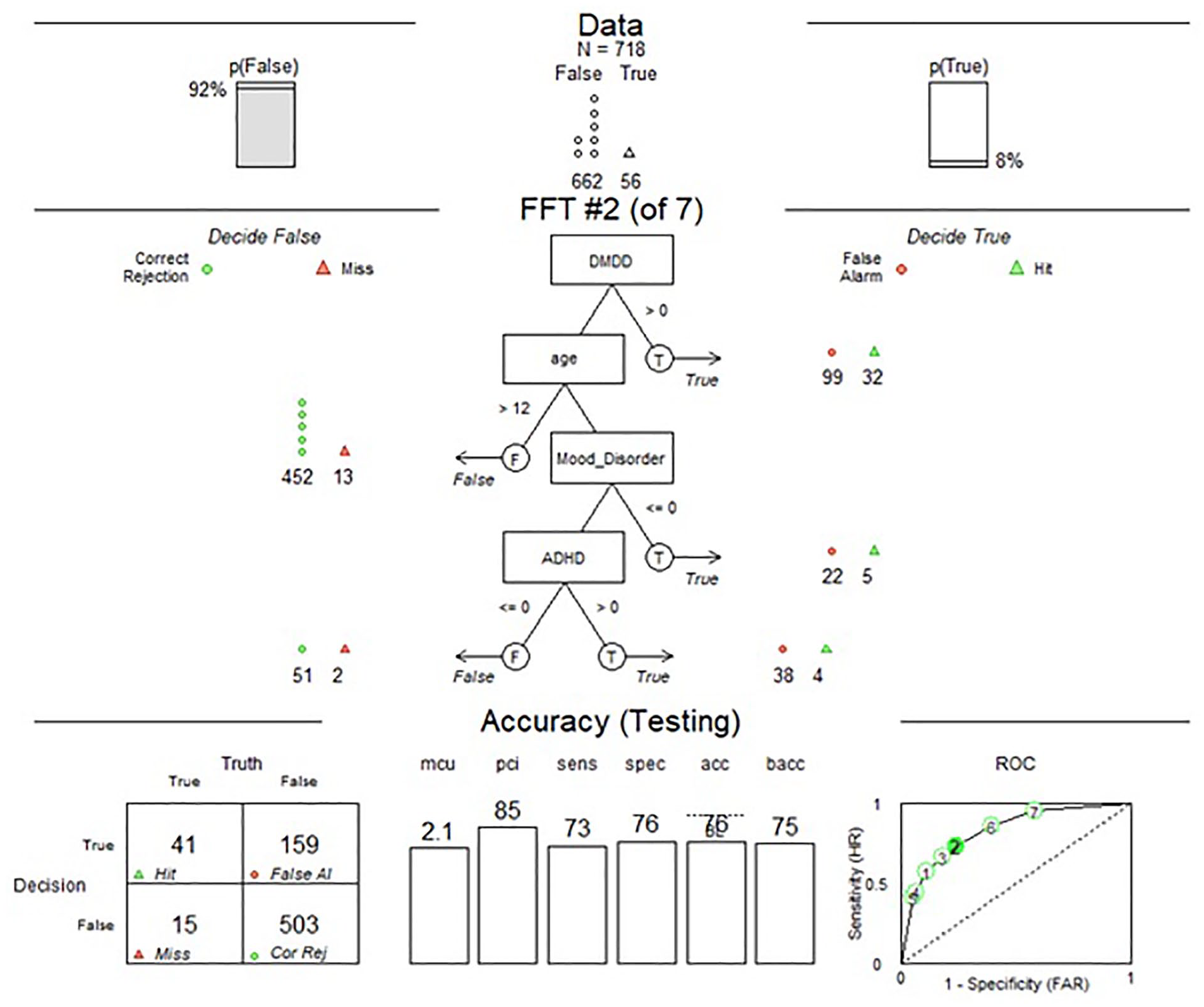
FFT Restraint and Seclusion Predictive Algorithm.
Algorithm
Upon analysis of the algorithm output, it was determined that a false negative is much costlier than a false positive. The rationale for a false negative being much costlier than a false positive is related to clients receiving a low-risk prediction when they are high-risk, providing staff no opportunity to put the preventive measures in place. However, it would be of little consequence to a client’s outcome if he or she was to be considered high-risk, when he or she was in fact low-risk. From a treatment team perspective, there is a risk that assigning too much cost to false negatives will result in too many to provide a useful amount of differentiation across classifications. Thus, our cost matrix was created with the intent of finding balance in predicted outcomes.
Results are interpreted in a tree algorithm where each decision point in the tree is referred to as a cue. Results suggest that the following assessment questions can be good cue indictors for clients needing restraint and seclusion while in treatment:
Cue 1: DMDD present A flag if a client had a disruptive mood dysregulation disorder diagnosis: A yes would indicate high-risk for a restraint and seclusion episode; a no would indicate a move to the subsequent cue.
Cue 2: Age—If no DMDD present Client age in years: Being older than 12 would indicate a lower risk for a restraint and seclusion episode; being 12 or younger would indicate a move to the subsequent cue.
Cue 3: Mood Disorder—If 12 or younger A flag if a client had a depressive and/or bipolar disorder diagnosis: A no would indicate high-risk for a restraint and seclusion episode; a yes would indicate a move to the subsequent cue.
Cue 4: ADHD—If no mood disorder present A flag if a client had an ADHD diagnosis: A yes would indicate high-risk for a restraint and seclusion episode; a no would indicate a client is low-risk since this is the last decision point.
Figure 1 represents the FFT algorithm, with the cues being decision points on the tree. The results of these decisions on the test sample are visually shown by the “True” and “False” branch exits with the conditional tests listed above these branches. The key results are highlighted from this figure in the next section.
Model Performance and Specification
The formula used 50% of the data set for training and 50% for testing, resulting in n = 1,437 in the FFT results. In total, 107 clients required restraint and seclusion and 1,330 did not. The performance of the FFT testing set is reported at the bottom of Figure 1 and can be interpreted as 41 cases correctly hit. This indicated that 41 positive criterion values (required restraint and seclusion) were correctly predicted to be positive, while 503 cases with negative criterion were correctly predicted to be negative. The hit rate (sensitivity) of the training data set is 73, which indicates 73% of the positive criterion values (required restraint and seclusion) were correctly predicted by the algorithm. The specificity of the model is 76, indicating 76% of negative cases were correctly predicted as negative.
The overall accuracy percentage of 76% can be misleading because it ignores the difference between hits and correct rejections. The section labeled receiver operating curve can be interpreted as having the true positive rate along the y-axis and the false positive rate along the x-axis. The receiver operating curve is used to determine the relationship between sensitivity and specificity related to a group of screening characteristics through graphical presentation (Safari et al., 2016). Thus, a point in the top left corner would have predicted all true positives correctly and no false positives. Meaning, the closer the point is to that corner, the more balanced accuracy the specific tree has. The bolded number on the curve represents the best algorithm, while the other numbers represent other algorithms that were considered.
The average number of cue values used in making classifications was 2.1, while the percentage of cues ignored when classifying cases was 65. The nature of FFTs is to use little information to make predictions so that a low number of cue values are used, and a high percentage of cues ignored is common. Overall, our algorithm appears to be reasonably strong at correctly predicting both individuals at risk for requiring restraint and seclusion and individuals who are not at risk.
Discussion
With the identified client characteristics of having a DMDD or an ADHD diagnosis, being 12 years old or younger, and not having a depressive and/or bipolar disorder diagnosis, approximately three out of four clients were correctly predicted as either having or not having a restraint and seclusion. Relating these characteristics or risk factors to current literature, there were some similarities, as well as differences. Delaney and Fogg (2005) found that clients around the age of 13.9 years old were more at risk for being restrained and secluded, which is close in comparison to what the algorithm indicated, identifying 12 years old and younger as being at risk.
Baeza et al. (2013) and Dean et al. (2008) found that a mood disorder diagnosis indicated higher risk for restraint and seclusion. Our algorithm found that clients with a disruptive mood disorder diagnosis increased and a diagnosis of depression and/or bipolar decreased the likelihood that a restraint and seclusion would occur. Additionally, our algorithm found that a diagnosis of ADHD increased the risk of restraint and seclusion in this population. This was a result not found in the literature. These findings should be taken into consideration when reviewing a client’s past and current psychiatric history related to his or her increased (DMDD and ADHD diagnoses) or decreased (depression and/or bipolar diagnosis) restraint and seclusion risk potential.
Risk factors found in the literature that were associated with higher prevalence of restraint and seclusion, but did not appear in the algorithm were abuse and trauma history (Dean et al., 2008; Hammer et al., 2011) and history of previous hospitalization (Baeza et al., 2013; Dean et al., 2008; Delaney & Fogg, 2005; Furre et al., 2017). Although these characteristics did not pull through in our best FFT, this does not necessarily mean that they are not predictive of risk of restraint and seclusion. Studies should be done that look at the predictive value of other restraint and seclusion risk factors in this population with the use of an FFT.
An interesting point to highlight is that aggression is heavily cited within the literature as being the number one predictor of restraint and seclusion (Allen et al., 2014; Baeza et al., 2013; Dean et al., 2007; Dean et al., 2008; Delaney & Fogg, 2005; Hert et al., 2011; Valenkamp et al., 2014). One commonly used instrument to measure aggression is the Modified Overt Aggression Scale (MOAS), which was the tool of choice at the organization during the time this study took place. What was found when reviewing the MOAS scores of clients restrained and secluded was that they were low before and high following restraint and seclusion.
This resulted in the inability to be able to apply the average scores in a meaningful way to this algorithm since many of the scores did not indicate an issue with aggression at the time the MOAS assessment was completed—prior to restraint and seclusion. Although the scores may be high following restraint and seclusion, having a lower score initially does not help staff identify those more at risk. In addition, escalation and aggression can happen quite rapidly in this population and can occur due to an unexpected trigger or impulse. This limits the ability of staff to identify escalation and aggression to be able to prevent restraint and seclusion.
Limitations
There are five noteworthy limitations to this study. First, since data are collected at a client stay level, it was not possible to predict on a dynamic, day-to-day basis. More specifically, the time of day could be a theoretically relevant predictor. However, since there was no daily information for each client encounter, we could not implement this into our algorithm. Daily census could potentially vary drastically during a client’s stay, but an average across individual client stays was used, since we did not have information for all days on all clients. Second, this model is lacking a variable for variation in client interactions across treatment teams or staff. We did not have insight into how avoidable each of the restraint and seclusion episodes in our sample may or may not have been. In other words, it is plausible that there were situations likely to end in restraint and seclusion that were caused by adept handling from staff, and others likely to end in restraint and seclusion that were escalated by improper handling from staff. Having some way to account for staff behavior may improve a model’s predictive ability.
Third, since this algorithm found diagnoses to be factors in predicting risk, this may limit one’s ability to use the algorithm for immediate risk evaluation. However, there are admitting diagnoses that can be taken into consideration that apply to this algorithm. Fourth, we used an FFT to keep the algorithm easily comprehendible and implementable, and by design, pulled out only a small number of decision points. Other samples, such as data from other organizations or treatment settings may contain different nuances in population attributes that could result in variations of the optimal tree. Last, since aggression is the primary risk factor of restraint and seclusion (Allen et al., 2014; Baeza et al., 2013), potential sequelae of reducing restraint and seclusion could be an increase in client or staff injury or even the use of chemical restraints or medications used during restraint. Future research should seek to understand client and organizational outcomes, such as staff injury and frequency of chemical restraints or medications, associated with restraint and seclusion in this population.
Implications
The restraint and seclusion predictive algorithm can influence client outcomes positively and improve the value and safety of care in an inpatient child and adolescent psychiatric population. Using this algorithm to identify clients more at risk for restraint and seclusion can assist in the development of individualized treatment plans to prevent a behavioral emergency. Staff will also be better prepared to efficiently focus their time, monitoring, and intervention for identified clients who need more structure or redirection to prevent aggression and escalation.
Further studies, emphasizing the inpatient child and adolescent psychiatric population should focus on the following: (a) applying this algorithm to future clients to compare predictive power and statistical methods for risk identification and restraint and seclusion reduction; (b) identifying historical patterns and trends of clients who have been restrained and secluded and compare them to what has been published in the literature from units with similar demographics; and (c) exploring aggression scores of clients prior to restraint and seclusion as a possible predictive factor.
Ideally, a sample representative of the population on a national scale would be used to identify a comprehensive predictive algorithm. This study, to an extent, is generalizable, as it used data from three different inpatient child and adolescent psychiatric units within three different hospitals. However, the three different hospitals were from the same organization. Thus, to be more generalizable, the recommendation would be to study the characteristics of this population from different organizations nationwide. Outcomes associated with reduced restraint and seclusion, such as staff turnover, injuries, and the client experience should also be reviewed and studied.
Conclusions
There were both positive and negative client characteristics that collectively revealed a high predictive power for restraint and seclusion in an inpatient child and adolescent psychiatric population. The positive predictive outcomes were having a diagnosis of disruptive mood dysregulation disorder or ADHD and being 12 years old or younger. The negative predictive outcome included not having a depressive and/or bipolar disorder diagnosis.
Existing literature also confirms that these characteristics increase a client’s risk for restraint and seclusion (Baeza et al., 2013; Dean et al., 2008; Delaney & Fogg, 2005). These characteristics should be reviewed on admission, and if all identified characteristics from the algorithm are present, an individualized treatment plan should be created that aims to prevent a behavioral emergency. In doing so, the overall value and safety of care increases, as prevention and awareness of at risk clients become the focus. Ultimately, this algorithm could help reduce, with the intent to ultimately eliminate, restraint and seclusion in the inpatient child and adolescent psychiatric population.
Footnotes
Author Roles
All authors conceived the study and determined the methodology. SRM collected and organized the data and DK, JC, and BK analyzed the data. SRM took the lead in writing and organizing the manuscript. DK and JC wrote the methods and results sections, and SRM wrote the introduction, discussion, and conclusion sections. BK critically appraised the study. All authors reviewed the final manuscript before submitting for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.