
Abstract
Background:
Cooperation between families of individuals with mental illnesses and mental health professionals is very important for the quality of mental health care, and there are many barriers to the establishment of cooperation between mental health professionals and families. It is highly important to identify/define barriers to cooperation between families and health professionals from a cultural perspective.
Aim:
The present study was aimed at identifying barriers to cooperation between mental health professionals and families from the perspectives of mental health professionals and family caregivers in Turkey.
Method:
In the sample of this descriptive qualitative study, 12 family caregivers and 11 health professionals were included.
Results:
The results of the study indicated seven themes regarding the perceptions of family caregivers and mental health professionals. The themes related to perceptions of family caregivers about barriers are as follows: “learning the process by living,” the perception of “my patient comes first,” and the perception of “being neglected.” The themes related to perceptions of mental health professionals about barriers are as follows: “lack of collaboration within the team,” “family itself as a barrier,” and “lack of education about working with families.” The common theme mentioned by both groups included the “patient-oriented service understanding.”
Conclusions:
The results obtained from this study are believed to be a guide for planning and implementing interventions to eliminate the barriers defined from the perspectives of both mental health professionals and family caregivers. Both mental health professionals and family caregivers need psychosocial interventions for strengthening “family cooperation.”
Introduction
The concepts of chronic mental illnesses and family cooperation have been among the most important mental health issues that have been on the agenda from the past to the present. Collaborative care is a care approach in which patients and their families work together systematically to provide patient-centered care (Lake & Turner, 2017). Supporting and maintaining the culture of collaboration is a key factor in the recovery of individuals with mental illnesses (Dirik et al., 2017). The collaborative approach also includes family involvement in care for mental illnesses. However, there are many barriers to family involvement in the care of individuals with mental illnesses (Landeweer et al., 2017).
Some of the developments in the field of mental health since the half of the 20th century include the dominance of the view that health professionals such as nurses and physicians are equal partners and the changes in the necessity of including both patients and family caregivers in care (Javed & Herrman, 2017). Family involvement in mental health care involves both cultural and structural changes. Such changes can be achieved through making it the common aim of each individual benefitting from the health service and the institution providing the service (Eassom et al., 2014). Although there are evidence-based results on families’ involvement in mental health care (McFarlane, 2016; Yesufu-Udechuku et al., 2015), in practice, families’ involvement is limited, and cooperation cannot be established at the desired level (Bucci et al., 2016; Javed & Herrman, 2017).
The definition of the current situation from the perspective of health professionals overlaps with the perspective of families. According to nurses providing care to people with mental illnesses, their primary responsibility is patients. Nurses establishing cooperation with patients is reported to be the cornerstone of nursing care. Although nurses think that the positive relationship between nurses and patients’ family members should be maintained, they also believe that this relationship should be secondary to patient care (Weimand et al., 2013). In their prospective and cross-sectional study investigating the expectations and actual experiences of family members regarding health professionals’ approaches in psychiatric care, Ewertzon et al. (2011) reported family members’ expectations in mental health professionals’ approaches as openness, confirmation, and cooperation (Ewertzon et al., 2011).
The first step in planning and providing health services for patients and families is the identification of “patient, family and service-related barriers” (Hamann & Heres, 2019). On the other hand, patient and family dynamics could demonstrate differences across the structure of different societies, cultures, and countries (Khan et al., 2019). Therefore, barriers to family cooperation in mental health services could also differ according to the perspectives of families and health professionals as well as cultures.
In a qualitative study conducted in Indonesia to identify the barriers to family involvement in mental health services, it was determined that affordability and usability were among the barriers (Tristiana et al., 2018). In a descriptive qualitative study conducted in Brazil, it was concluded that the family caregivers’ views about the nursing care in the inpatient psychiatry unit were generally positive and they did not have high expectations (Moll et al., 2018). In another study conducted in China regarding the barriers to implementing family-centered practices, it was reported that the family-centered approach did not develop in the clinical setting. Various perceptions of barriers to family-centered care were reported by nurses, which included psychiatry nurses’ identity and role perceptions, the gap between knowledge and practice, and the support of the administration (Wong, 2014). On the other hand, no studies were found to have defined perceptions of barriers to cooperation with families from a cultural perspective in mental health services in Turkish society.
In Turkey, health care regarding mental illnesses is carried out based on the community-hospital balance model. In this model, patients are provided with short hospitalizations and treatment during acute exacerbation periods, and they are expected to benefit from the community mental health centers in their regions and to be followed there (Bilge et al., 2016). However, cooperation with families, and interventions and continuous programs targeting families, both in the provision of community mental health services and during hospital stays are either insufficient or not available. Families of individuals with chronic mental illnesses cannot receive any educational or institutional support in this process (Ministry of Health, 2011).
Cooperation between individuals with chronic mental illnesses, their families, and mental health professionals is very important for the quality of mental health care. If what health professionals and families experience during the provision of these services is not clearly understood, it will be difficult for these services to meet such expectations. While family cooperation and barriers to this cooperation have been extensively investigated in the world literature, there is a gap in the literature about the studies on the barriers to family cooperation in Turkish society. Given the cultural dimension of ensuring cooperation with families, an identification of the perspectives of family caregivers and mental health professionals in Turkish society is believed to fill this gap in Turkish literature.
The results of the present study are believed to be a guide for forming the content and structure of the programs and psychosocial interventions to develop family cooperation in the presentation of mental health services. Therefore, the present study was aimed at identifying the barriers to cooperation with family caregivers of patients with chronic mental illnesses in Turkish society from the perspectives of family caregivers and health professionals working in the field of mental health.
Methods
Research Design and Participants
The present study is descriptive qualitative in nature. Descriptive qualitative research is a qualitative approach used in cases when the purpose is to define a phenomenon to be investigated and when a less theoretical relationship is offered compared with other qualitative approaches (Sandelowski, 2000).
In the present study, the maximum variation sampling method, one of the purposive sampling methods, was utilized (Yıldırım & Şimşek, 2013). The sample consisted of two groups. The purpose of including two groups (caregivers and health professionals) in the study is to identify the barriers to cooperation from the perspectives of both groups. While the first group was composed of family caregivers aged ≥ 18 years who had been providing care for individuals with chronic mental illnesses such as bipolar affective disorder and schizophrenia for at least 2 years, the second group included mental health professionals working in the field of mental health for at least 2 years (Table 1).
Inclusion and Exclusion Criteria.
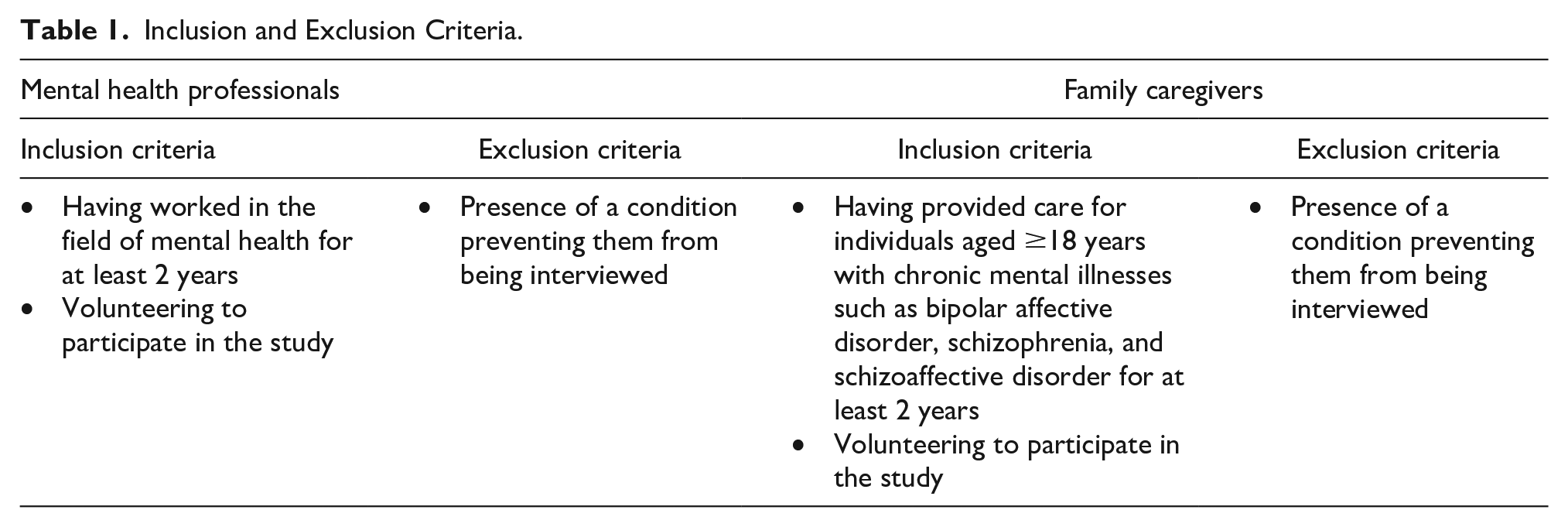
The participants were interviewed using the semistructured interview technique. The interviews were conducted individually. The study sample included 12 family caregivers and 11 health professionals. The individuals who were included in the sample were informed about the purpose of the study, but participation was on a voluntary basis in both groups. All the individuals in the caregiver group agreed to participate in the study.
Data Collection
Data were collected through individual and semistructured interviews conducted with the participants. The sociodemographic data were collected through the data collection forms that were prepared by the researchers in line with the pertinent literature. These forms provided descriptive information about caregivers and health professionals. While the caregivers’ descriptive data included information such as age, sex, education level, employment status, duration of caregiving, and degree of kinship, health professionals’ descriptive data included information such as age, sex, education level, working discipline, and duration of working.
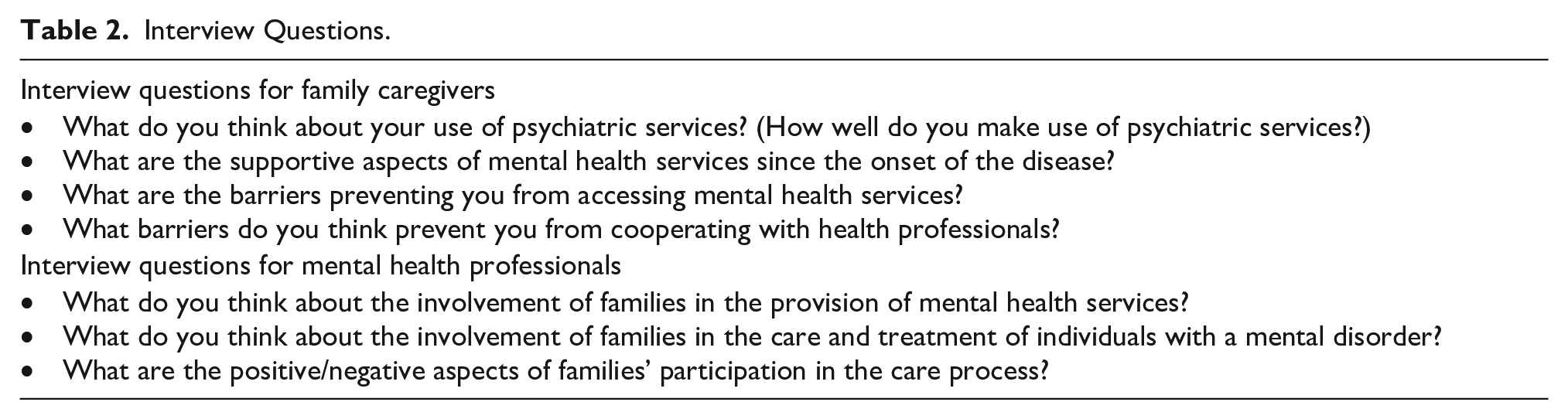
Interviews with volunteers who agreed to participate in the study were conducted in the interview rooms of the adult psychiatry clinic of a university hospital. The interviews were conducted only by the first researcher. Before the study was designed, the researchers received various courses and trainings on qualitative research. The researchers did not contact the family caregivers included in the study before the interviews. Prior to the interviews, each participant was informed about the purpose of the study. The researcher who held the interviews introduced herself to the participants. The interview questions were designed as semistructured (Table 2). Before the interviews were conducted, expert opinions were obtained from four experts specialized in mental illnesses. A pilot interview was conducted before the participants in both groups were interviewed. Those who were administered the pilot interview were not included in the sample. Each individual was interviewed once, and the interviews were not repeated. The interviews were audio-recorded. Short field notes were taken regarding the observations obtained during the interviews.
Interview Questions.
Interviews conducted with the family caregivers took a minimum of 13 minutes and a maximum of 44 minutes. Interviews conducted with the health professionals took a minimum of 11 minutes and a maximum of 23 minutes. The interviews were continued until the data obtained from the interviews started to repeat and no new data were obtained. The point when repeated data started to be obtained was identified as the saturation point, and the interviews were ended (Houghton et al., 2013; Streubert & Carpenter, 2011).
Analysis of the Data
The data obtained from the interviews were analyzed using content analysis methods. The transcription of the data obtained from the interviews was read several times, and then the data for both groups were coded. Coding was simultaneously conducted by the second and third researchers independently of each other. After the coding process was over, both researchers’ codings were compared. The consistency of the codes was evaluated by the experts. The researchers discussed the themes of coding. The most appropriate themes obtained from the codings were named, and the themes were given their final forms. No software programs were used in the analysis of the study data.
Rigor
The principles of credibility, transferability, consistency, and confirmability were used in the study. In line with the principle of credibility, the in-depth interview method was used to collect the data. The data collected were audio-recorded. The interviews were continued until the saturation point was reached. Expert opinions were obtained for the interview questions. The data diversification method is another method used for the principle of credibility. In line with this principle, diversity was ensured in characteristics such as professions, diagnoses of the patients for whom the family caregivers provided care, age, and sex.
In line with the principle of transferability, the purposive sampling method was used in sample selection, and the participants’ statements were directly quoted. To comply with the principle of consistency, the interviews were conducted by the same researcher. The data were coded by two researchers independently of each other. The consistency of the codings was evaluated by the experts. The Kappa test was used for the consistency evaluation of the themes obtained (Campbell et al., 2013; Creswell, 2013). The Kappa test evaluation by the three experts yielded excellent agreement (k = 1, p < .001).
Ethical Issues
Before the study was conducted, written permission (dated December 21, 2018, numbered 3693-GOA) was obtained from the non-interventional clinical research ethics committee of the university. After the participants were informed of the objectives and procedures of the study, their verbal and written informed consent was received. Permission was obtained from the administration of the institution where the study was conducted.
The individuals who agreed to participate were involved in the study, and participation was on a voluntary basis. The individuals who did not want to participate in the study were excluded from the sample. Those who participated were told that they could withdraw from the study at any stage. Particularly the caregiver group was told that participating in the study would not hinder the treatment or care processes at all, nor would they be affected negatively. It was also stated that the participants’ information would be kept confidential, and no names would be used when the study was reported. It was also stated that the participants’ voice recordings would be used merely for the study purposes, and the data would be stored and kept confidential, and would not be shared with the third parties. This information was also stated in the written consent form.
Results
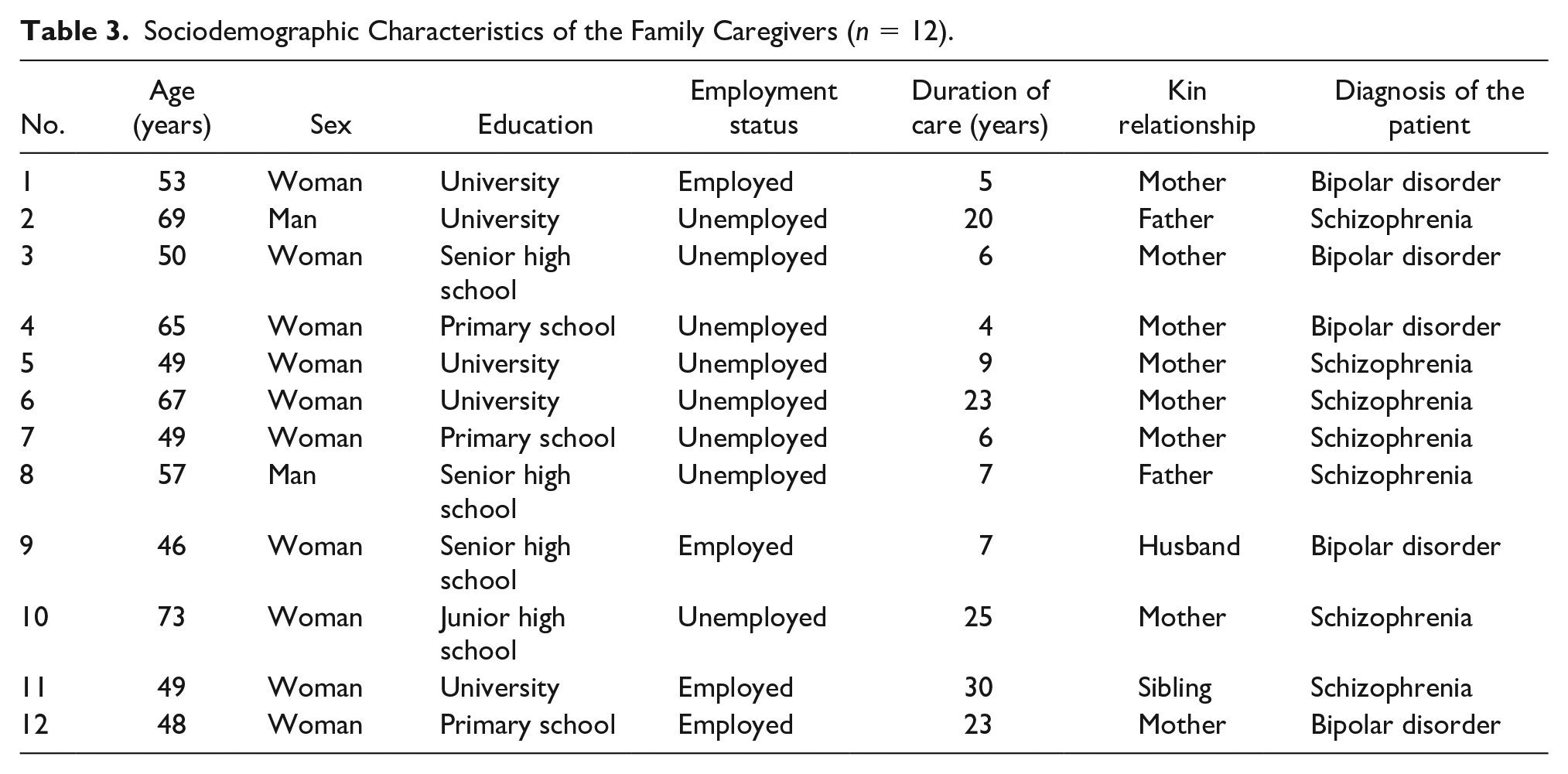
The mean age of the 12 participating caregivers was 56.25 ± 9.61 years (min: 46, max: 73). Of the family caregivers, 10 were women, and 2 were men. The mean duration of caregiving was 13.75 ± 9.56 years (min: 4, max: 30). Of the relatives of the family caregivers who received care, 7 were diagnosed with schizophrenia and 5 with bipolar disorder (Table 3).
Sociodemographic Characteristics of the Family Caregivers (n = 12).
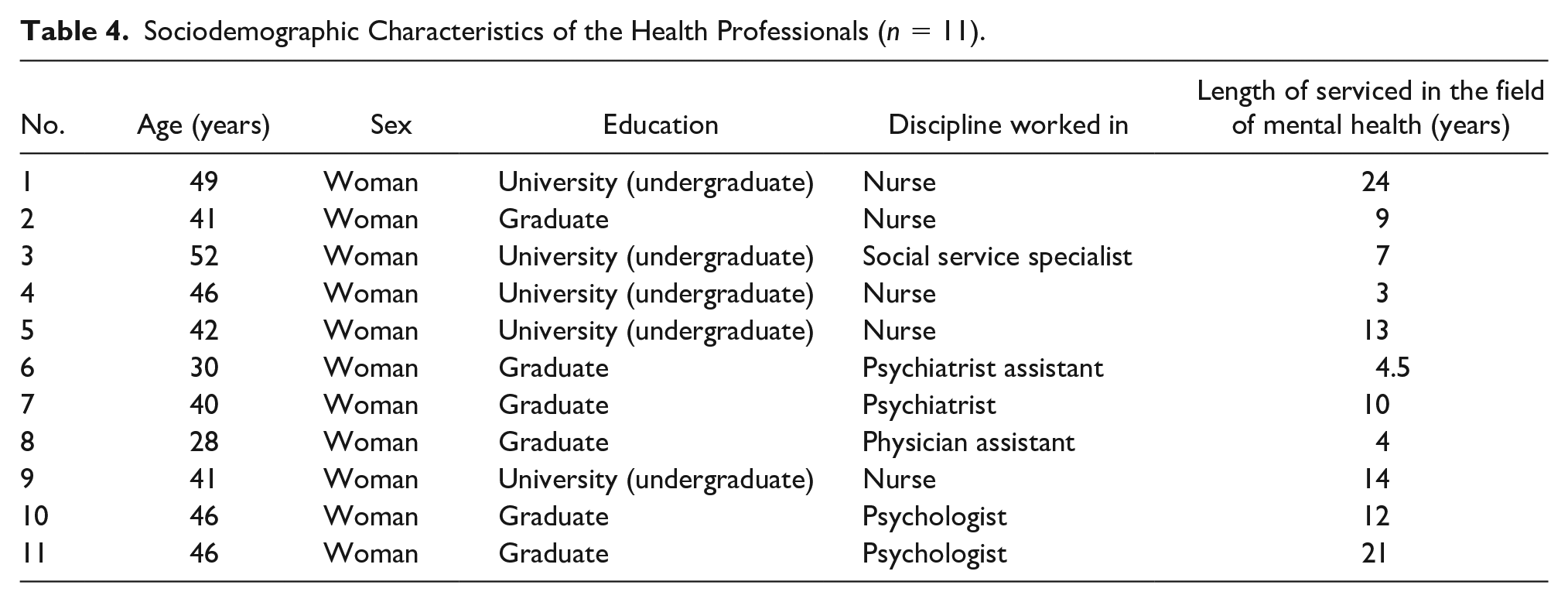
The mean age of the participating mental health professionals was 41.90 ± 7.36 years (min: 28, max: 52). All of them were women. Of the mental health professionals who participated in the study, five were university graduates, six had a postgraduate degree, five were nurses, one was a social worker, one was a psychiatrist, two were psychiatric assistants, and two were psychologists. Their mean length of employment in mental health services was 11.04 ± 6.77 years (min: 3, max: 24; Table 4).
Sociodemographic Characteristics of the Health Professionals (n = 11).
The results of the study indicated seven themes related to family caregivers’ and mental health professionals’ perceptions of barriers. These themes were grouped into three categories. While the themes about family caregivers included “learning the process by living,” “perception of my patient comes first,” and perception of “being neglected,” mental health professionals’ barrier perceptions included three themes: “lack of collaboration within the team,” “family itself as a barrier” and “lack of education about working with families.” The common theme of both groups was the “patient-oriented service understanding” (Figure 1).
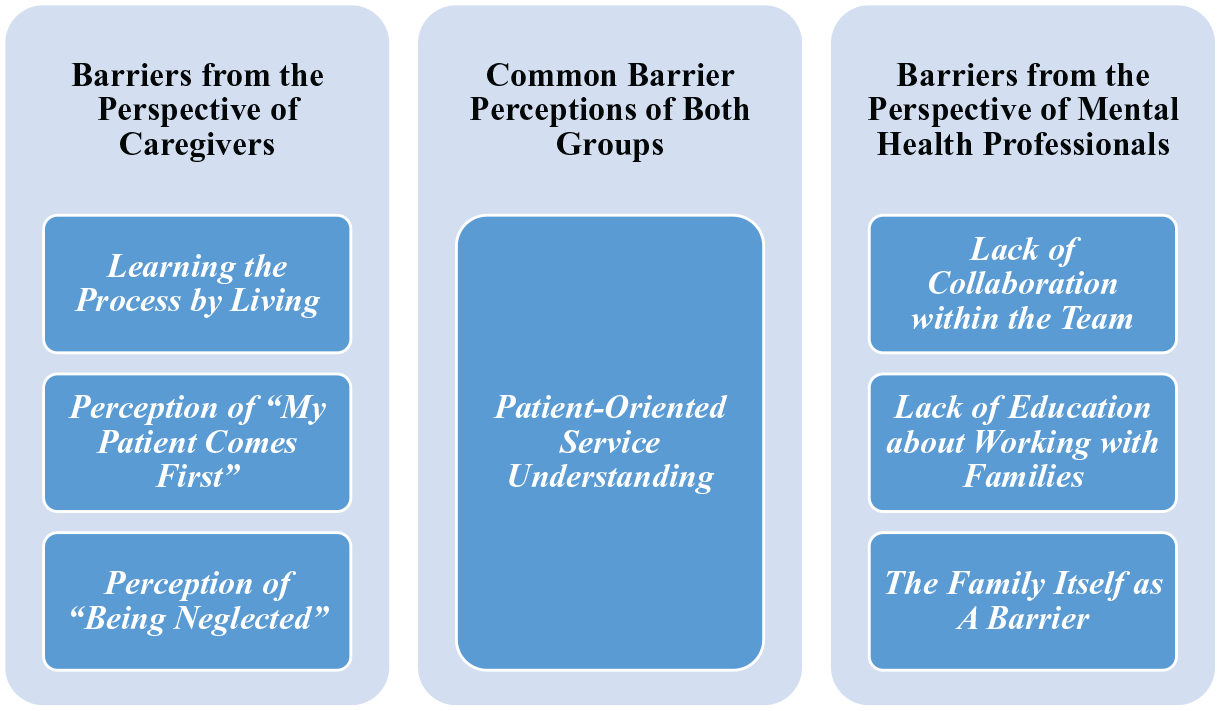
Barriers to cooperation between families and health professionals.
Barriers From the Perspective of Caregivers
Learning the Process by Living
Caregivers stated that they maintained the process of receiving the diagnosis of a mental illness and continuing care mainly by learning things with their own efforts. As a result of the positive and negative experiences with their patients, in time they learned how to approach the patient by themselves. One of the caregivers’ statements about this was as follows: Learning this has made us wiser within 6 years. It has taught us many things. It is not easy. However, if we had acted consciously . . . if we had felt that the attack periods were approaching and taken her to a clinic . . . I do not know if we had been supported . . . the process could have been easier for us. (3rd caregiver)
Perception of “My Patient Comes First.”
As family caregivers firstly thought of their patients, they reported that the priority was the patient, and thus they ignored their own needs. They stated that they ignored themselves because they thought of their patients and thus did not consult health services for themselves. The statement of a caregiver about this is as follows: At that moment, I only think of my patient. I mean, I say it is enough if the physician deals with my patient. I want my patient to get through the problem or the attack because I also feel relieved when it is over. (11th caregiver)
Perception of “Being Neglected.”
Family caregivers think that they are not given importance and their thoughts and experiences as patient relatives are not considered. Observations and experiences of the family caregivers regarding their patients reportedly were not given importance, and they were “put off.” An example of this theme is as follows: He is constantly talking to someone, fighting, getting up, and attacking. He sees someone. Do you think that’s okay? But the doctor says that’s not true. He says my wife refuses that. But I witnessed it. So now, they trust the patient, not me. But it is I who witness what’s going on. So this is a serious problem. (9th caregiver)
Barriers From the Perspective of Mental Health Professionals
Lack of Collaboration Within the Team
The mental health professionals mentioned a lack of collaboration within the team for the situations, preventing cooperation with families. They stated factors such as a lack of communication, conflicts due to communication problems, and lack of a team viewpoint in relation to this theme. The health professionals also mentioned that the circulation of physician assistant groups every 6 months and their change after 6 months was a negative aspect of the development of collaboration and a sense of belonging. A health professional’s views about this were as follows: We work here all the time, but the physician and assistant groups are changing constantly. There is circulation in this place. Maybe no one . . . sense of belonging . . . it is about a sense of belonging as well. As they are not here all the time, they may not need to develop such a program on their part. (2nd health professional)
Some factors preventing collaboration within the team were reported as the unwritten discrimination between “physicians” and “other mental health professionals” and the dominant role of physicians in the treatment. Health professionals other than the physicians stated that these factors caused the development of a hierarchical structure in the team. The professionals also stated that the problems experienced in the team collaboration caused them to experience uncertainties about who would take roles in involving family members in the process. An excerpt indicating this view is as follows: Everyone is expecting it from each other. The employment status is not that important. . . . It could be a psychologist, a nurse, or an assistant . . . I do not think that it could be an assistant because they are the temporary staff. I do not know. It could be a service specialist . . . s/he can organize such thing. (5th health professional)
Lack of Education About Working With Families
The mental health professionals stated that they lacked knowledge about how to work with families and how to establish cooperation with families. They thought that involving families in the care and providing education about patients also require education and stated that health professionals lacked knowledge about it. An expert’s statements reflecting this view are as follows: Of course. . . . Most of us know how mental patients and their families affect the treatment process positively or negatively, but we do not know how to prevent it. We just want it. We also lack training on it. I guess providing health professionals with a kind of training program could fill a great gap. (2nd health professional)
A health professional stated that structured trainings would be insufficient in meeting each individual’s needs and shared her experience with the inadequacy in helping caregivers about each individual’s needs as follows: Because everybody could ask something unexpected regarding, for example, the place they work in or maybe something about marriage life . . . so you need to address them as well. That’s why honestly, I am not so sure whether we could manage it as a group or in a structured way. (8th health professional)
The Family Itself as a Barrier
Mental health professionals stated that the family itself was an important barrier to providing cooperation. They also stated that involving a family caregiver in the process could affect the patient negatively, and some family members had negative effects on the treatment process. Mental health professionals said that some behaviors of family members could be a barrier to cooperation with professionals, and thus they considered the family itself as a “barrier” to cooperation. The preventive behaviors mentioned by professionals included overprotective family attitudes, indifferent family attitudes, interventional family attitudes, and the family member’s rejecting treatment. An excerpt’s statements were as follows: Because sometimes we have to deal with patient relatives who put us in a very difficult position and direct the treatment in the wrong way. I mean this is something related to patient relatives’ attitudes and it makes our job difficult. (1st health professional)
Another health professional’s statement is as follows: For instance, sometimes the patient relative is too much dependent on the patient . . . in a way to intervene with the treatment; namely, dependence at a pathological level. Or sometimes they are too indifferent and they see the patient as a burden; you can feel this from the way they approach the patient. Some people have high levels of expressed emotions; these kinds of people’s diseases cause them to have more frequent exacerbations. (5th health professional)
Common Barrier Perceptions of Both Groups
Patient-Oriented Service Understanding
Both caregivers and health professionals mentioned the patient-oriented service understanding as a barrier to cooperation. The caregivers stated that they saw the physician within the “15 minutes” allocated to the patient, and they could talk only about the patient within this limited time. They also stated that seeing the physician mainly included a medication-focused talk and that the service provided was treatment focused. The caregivers reportedly reported that they did not access the information they needed for their patients. An excerpt’s statements were as follows: How about us? We have not been provided with anything. We have been taking our patient to the physician. The physician has changed the medicine, written the report, and increased or decreased the dose of the medicine; we have been bringing our patient here. We have spent 30 years in this tiring process. (11th caregiver)
Mental health professionals also mentioned the barrier of the patient-oriented service understanding. In this theme, they mentioned that the system mainly was concerned with diagnosis and treatment for the patient and stated that there was no systematic output (financial benefit) of the interventions for the family. They stated that more importance is given to medication because the structure of the current system was mainly for the patient, and charging is based on this. They reportedly thought that the physicians’ treatment-oriented perspectives and psychiatry nurses’ focusing on conducting routine practices were the factors that caused barriers to the involvement of the family to the treatment and cooperation with the family. An expert’s statement about this is as follows: I think today one of the biggest problems in psychiatry is its turning to psychopharmacology. In other words, the support processes, psychotherapy processes, and interview processes have been given less importance. Here is a university hospital. However, to be honest, I do not think that visits or therapies are performed very regularly, nor can I see sufficient efforts shown for this. (10th health professional)
Discussion
Barriers From the Perspective of Caregivers
Barriers from the perspective of caregivers included the perception of “being neglected by professionals,” “perception of my patient comes first,” and “learning the caregiving process by living.” According to a qualitative study conducted by Ness et al. (2016), caregivers thought that health professionals did not see them as a source for cooperation and stated that good cooperation could be established by putting caregivers at the forefront (Ness et al., 2016). In another qualitative study, family caregivers were made to feel insignificant by health professionals, and they were marginalized from the care planning procedure; they reportedly had this feeling when health professionals were late for appointments, did not listen to them, or did not want to include them in the process (Cree et al., 2015).
Establishing cooperation with the family as early as possible creates a favorable environment for communication and partnership (Rusner et al., 2013). The perception that demonstrated differences in Turkish society is the perception of “my patient comes first.” Although caregivers learned many difficulties related to the process by themselves and continued the process with their efforts, they may give less importance to their own well-being. Due to the fatalistic structure of Turkish society, Turkish people put themselves in the background, bring the patient to the forefront, and hesitate to communicate with the health professionals. Perceiving the patient as the priority might be an indicator of caregivers’ perception of their own insignificance (Kaya & Bozkur, 2017).
Barriers From the Perspective of Mental Health Professionals
Barriers from the perspective of mental health professionals included “lack of collaboration within the team,” “lack of education about working with families,” and “the family itself as a barrier.” Inadequate training of health professionals is considered an important barrier (Bucci et al., 2016). In the National Mental Health Action Plan for Turkey (2011), it is stated that the labor force in the field of mental health in Turkey is well below the European region averages (Ministry of Health, 2011). The actions planned until 2013 were aimed at increasing the number of health workers working in the field of mental health. On the other hand, it is known that this goal has not been achieved yet (Karataş & Çalışkan, 2020).
Health professionals also state that families have negative effects on the process because they resort to some practices that discourage patients from taking medication, and this leads to the disruption of the treatment process. The participating professionals defined the caregivers’ attempts for intervening in the treatment as a barrier. This condition could be considered as two sided. While the professionals might unconsciously stigmatize family members, family members’ negative attitudes could affect the treatment process negatively (Cetinkaya Duman et al., 2015).
In the literature, findings that indicate caregivers’ feelings of being stigmatized by health professionals are reported (Tristiana et al., 2018). This study also found that family attitudes were defined as a direct barrier by health professionals. Trainings on health professionals’ stigmatizing attitudes toward families and on the involvement of families in the treatment process are believed to be an important intervention for cooperation with families in Turkish society.
The results of this study indicate that mental health professionals also do not have a common approach among themselves about this issue. Cooperation with families is facilitated through attitudes toward cooperation within the team and motivation for a common purpose and value (Shoesmith et al., 2020). Therefore, factors such as psychiatry nurses’ and mental health professionals’ focusing on a common purpose, explicit definitions of their roles, and communication between the individuals using the service and mental health professionals are of great importance for the establishment of cooperation with families (Biringer et al., 2020).
Common Barrier Perceptions of Both Groups
Both caregivers and health professionals saw the patient-oriented approach as a barrier to cooperation, indicating similarity with the results reported in the literature. Although mental health professionals were aware of the stress experienced by the family and the family’s need for support, they stated that their primary responsibility was to support and treat the patient (Wong, 2014).
The health system might contribute to family cooperation from different aspects. The cause as stated by both the family caregivers and the mental health professionals was that the health system lacks family services. In Turkey, the health system is mainly patient and treatment oriented (Cavmak & Cavmak, 2017). Within the health system, health professionals are not paid for the family-related interventions they perform, which is a barrier to the development of motivation for family cooperation. This result indicates that there is a need for revising the mental health system in terms of not only a treatment-oriented approach but also for the involvement of the family in the process.
Implications for Nursing Practice
The results obtained from this study are believed to be a guide for planning and implementing interventions to eliminate the barriers defined from the perspectives of both mental health professionals and family caregivers. The results obtained from a sample of Turkish society indicate that there is a need particularly for family interventions for strengthening family caregivers in the process of providing care for a mental illness. The caregivers should be identified and psychosocial interventions should be planned particularly in acute care and in cases when the first attack is experienced so that they can be provided with support. The difficulties experienced in the process and strengthening ways of coping are considered to raise awareness about the role of caregivers as much as that of patients in this process. There is also a need for providing health professionals with trainings on cooperation with families and sharing within the team to increase cooperation with families.
Strengths and Limitations of the Study
This study has some strengths and limitations. The strength is that the study aimed at investigating barriers to cooperation in mental health care included both family caregivers and mental health professionals in Turkish society. One of the limitations of the study is that the results cannot be generalized due to the nature of qualitative studies. Another limitation is similarly related to the purpose of the study. Explanations about the ethical issues of the study were made to family caregivers before the interviews. On the other hand, caregivers experiencing distress in expressing themselves regarding the services they receive and the potential difficulties is considered another limitation of the study.
Conclusion
The results of the present study revealed common and distinguishing perceptions of barriers to the cooperation between caregivers and mental health professionals. The barrier perception defined by both groups is the patient-oriented service understanding. Family caregivers providing care for a person with a mental illness stated that they learned the caregiving process by themselves through trial and error. Although family caregivers reported that they experienced difficulties in this process, they put the needs of their patients ahead of their own individual needs. They perceive themselves as insignificant while they are receiving mental health services. While a lack of collaboration among themselves as a team and a lack of education about working with families were reported as barriers by mental health professionals, another barrier was reported to be “caregivers.” Mental health professionals perceived caregivers as a barrier to cooperation.
Footnotes
Author Roles
All authors met at least one of the following criteria in each section: (1) The conception and design of the study, acquisition of data, or analysis and interpretation of data. (2) Drafting the article or revising it critically for important intellectual content. (3) Final approval of the version to be submitted and (4) agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.