
Abstract
Objective:
Intimate partner violence (IPV) is a serious public health threat in the United States, affecting millions of individuals and families. The American Association of Colleges of Nursing recommends that nursing programs, both baccalaureate and graduate, provide students didactic training and clinical experience in the assessment and management of IPV. Our goal was to expose Psychiatric Mental Health Nurse Practitioner (PMHNP) students and Family Nurse Practitioner (FNP) students to a simulated IPV scenario so they are prepared to respond appropriately to a survivor’s disclosure of IPV when they begin clinical practice.
Methods:
We integrated a patient simulation scenario into our PMHNP and FNP curriculum. A combined group of PMHNP and FNP students participated in a simulation in which the standardized patient provided an unlikely explanation for her injuries. If students inquired about abuse, the patient revealed that she had experienced IPV. A pre- and posttest survey was used to evaluate student knowledge gain before and after the participating in the scenario. A Related Samples Wilcoxon Signed Rank Test was used to evaluate the results.
Results:
Compared with pretest scores, students demonstrated improved confidence in screening for IPV as well as responding to a disclosure of IPV.
Conclusion:
Simulation provides a method to enhance student knowledge of incidence, risk, and best practices in relation to the screening, assessment and management of IPV.
Keywords
Introduction
Intimate partner violence (IPV) is a significant public health crisis in the United States. According to a survey completed by 88% of U.S. domestic violence shelters, there were more than 19,159 hot-line calls on September 12, 2019, alone (National Network to End Domestic Violence, 2020). The Centers for Disease Control and Prevention (CDC) defines IPV as violence that includes “physical violence, sexual violence, stalking and psychological aggression (including coercive tactics) by a current or former intimate partner (i.e., spouse, boyfriend/girlfriend, dating partner, or ongoing sexual partner)” (Breiding et al., 2015, p. 11).
IPV affects both men and women. In 2010, the CDC’s National Center for Injury Prevention and Control began a telephone survey to assess sexual violence, stalking and IPV in adult men and women in the United States. The latest survey, from 2015, reports that 5.5% of women (approximately 6.6 million women) and 5.2% of men (approximately 5.8 million men) in the United States experienced sexual violence, physical violence, and/or stalking by an intimate partner during the 12 months preceding the survey. About 25.1% of women and 10.9% of men in the United States experience contact sexual violence, physical violence, and/or stalking by an intimate partner during their lifetime and reported some form of IPV-related impact (being fearful, concerned for safety, injury, need for medical care, needed help from law enforcement, missed at least one day of work or school, experienced any posttraumatic stress disorder symptoms, need for housing services, need for victim advocate services; Smith et al., 2018).According to the Centers for Disease Control and Prevention, more than half of the 3,519 women and girls killed in the United States in 2015 were killed by a current or former intimate partner (Petrosky et al., 2017). While murder is obviously the most severe consequence of IPV, there are many others. Breiding et al. (2008) found that men and women who reported experiencing IPV during their lifetime were more likely to report a variety of chronic diseases, including asthma, joint disease, cardiovascular disease, and stroke. Depression symptoms and suicide attempts are also more common in those who have experienced IPV (Devries et al., 2013). Survivors of IPV had a higher incidence of sexually transmitted infections compared with women in nonabusive relationships (Hess et al., 2012). IPV is also associated with pregnancy coercion and birth control sabotage (Miller et al., 2010). Besides the physical and emotional costs of IPV, the financial costs are enormous. The lifetime economic burden of IPV was calculated at $103,767 for female survivors and $23,404 for male survivors. The population economic burden was more than $3.6 trillion over survivors’ lifetimes (Peterson et al., 2018). The COVID-19 pandemic may have produced a “perfect storm” environment for IPV to flourish. The upheaval of the labor market has contributed to financial stress and disruption of daily routines, increased drug and alcohol use, and a loss of outside contacts. The shelter-in-place orders, while decreasing the transmission of the virus, have led to social isolation with many people spending many more hours a day with their domestic partner with limited contact with the outside world. The National Domestic Violence Hotline (2020) reported a 9% increase in call volume from March 2020 to May 2020 compared with previous years.
The American Association of Colleges of Nursing (AACN) recognizes that IPV is a high prevalence public health crisis that requires intervention from health care providers. Specifically, AACN recommends that nursing programs, both baccalaureate and graduate, offer both didactic and clinical curricula that provides experience in dealing with this type of violence. The curricula competencies recommended by AACN include assessment skills related to the identification and documentation of abuse and its health effects, along with interventions to reduce vulnerability and increase safety (AACN, 1999). However, nurse practitioner students’ exposure to patients effected by IPV during clinical rotations is unpredictable and jeopardizes attainment of this competency. Simulation using standardized patients has been found to be an effective teaching method for both undergraduate and graduate nursing students (Kim et al., 2016). Goodman and Winter (2017) reviewed the use of standardized patients in psychiatric nursing education and reported a paucity of well-developed research studies demonstrating its effectiveness. Standardized patient simulation has been used to instruct undergraduate nursing students about IPV (Blumling et al., 2018; Johnson & Montgomery, 2017; Wood, 2016). There is limited published work on the use of standardized patient simulation in the instruction of psychiatric mental health nurse practitioner students in the management of a disclosure of IPV.
Method
Objectives
The purpose of this IPV simulation scenario was to evaluate whether participating psychiatric mental health nurse practitioner (PMHNP) students and family nurse practitioner (FNP) students would perceive enhanced confidence and competence in the assessment and management of a disclosure of IPV.
Theoretic Framework
The theoretical framework for this study was Kolb’s theory of experiential learning (Kolb & Kolb, 2017). The foundation of this theory is that competence arises as experiences are transformed by a cyclical process of active conceptualization, concrete experiences, reflexive observations, and active experimentation. These four components of the learning cycle build on each other to create deeper understanding and further insight.
Scenario Development
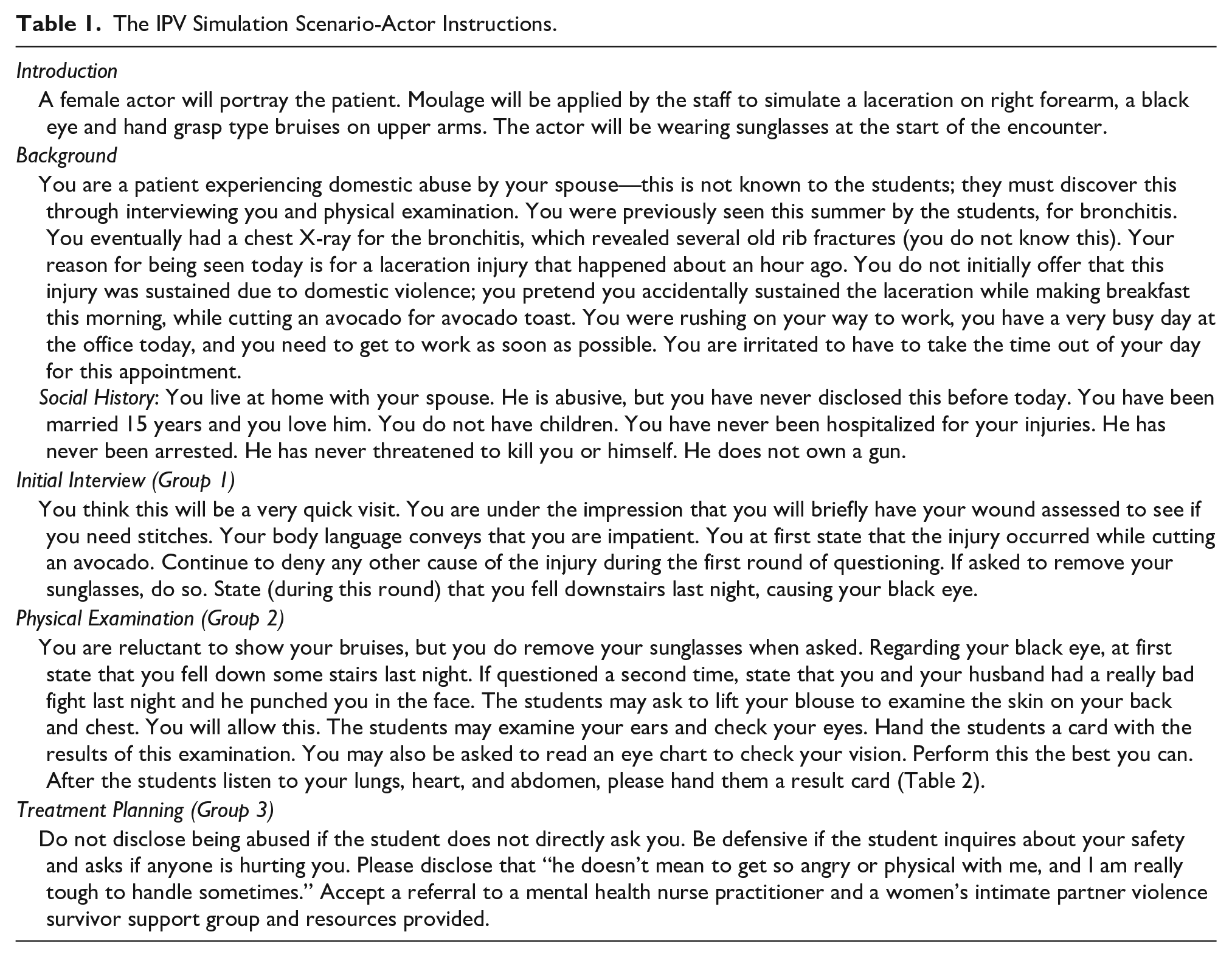
The International Nursing Association for Clinical Simulation and Learning standards of best practice were used as a checklist for development of the scenario (International Nursing Association for Clinical Simulation and Learning Standards Committee, 2016).The scenario was developed jointly by two faculty. One faculty member had completed an in-house training program that was developed by a certified health care simulation educator. This four-module program (Introduction to Simulation, Principles of Simulation, Debriefing, and Evaluation) was developed to provide a thorough foundation for faculty who planned to work in the simulation arena. The other faculty member has had extensive work with promoting screening, assessment and referral for IPV patients at her clinical sites. The scenario took place at a large publicly funded Midwestern University in the United States. The objectives of the simulation were the following: (1) obtain a focused patient history, (2) examine, diagnose and treat injuries, (3) develop an in-clinic management plan, including a hand-off to a PMHNP, (4) discuss safety planning, and (5) develop a follow-up plan for the patient, which includes a referral for counseling (Table 1 here).
The IPV Simulation Scenario-Actor Instructions.
Participants
As part of a clinical practicum course, PMHNP students and FNP students were required to participate in a Simulation Day experience. Fifty students (12 PMHNP and 38 FNP) participated over 2 days. The simulation day comprised four scenarios, all of which had both a psychiatric and primary care component. The other scenarios were a telephone call for a controlled substance (Woroch et al., 2018), a transgender teenager, and a patient presenting for a follow up for his severe mental illness. Each day, the faculty randomly divided the students into four groups. Groups comprised roughly five FNP students and one PMHNP student. The students rotated between the different scenarios. Working in pairs, the students were assigned to work either on the history, physical examination, or the management plan. Students were instructed to make a “time-out” sign if they wished to put the scenario on hold and consult their peers as to the next steps. The actor did not participate during time-outs and continued as though they did not hear the conversation that occurred during the time-out. Each scenario was allotted 75 minutes, 45 minutes for the scenario and 30 minutes for the debriefing.
Actor
The simulation center maintains a roster of local improvisational actors. The actor was hired based on her age, physical characteristics, and acting experience. The scenario was reviewed with her prior to the scenario, with an emphasis on actor demeanor. On her arrival to the simulation center, make-up was applied to mimic a forearm laceration, a periorbital hematoma, and upper arm ecchymosis. She was also provided with sunglasses to wear. She was provided with cards to hand to students which contained detailed physical examination results (Table 2).
Physical Examination Cards.
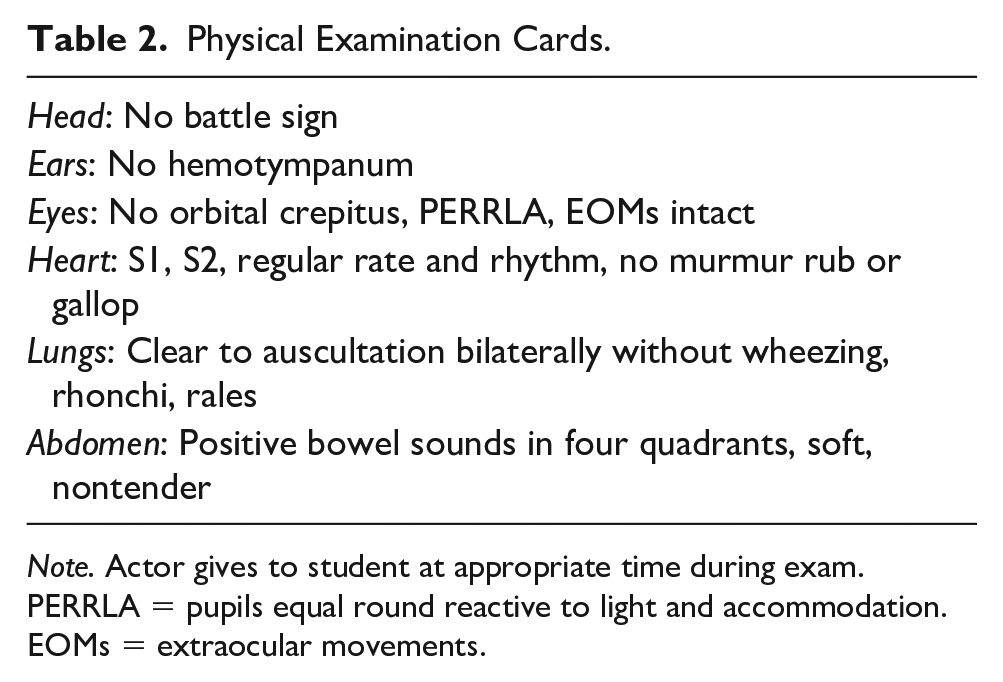
Note. Actor gives to student at appropriate time during exam. PERRLA = pupils equal round reactive to light and accommodation. EOMs = extraocular movements.
Tool
Prior to participation in the simulation scenario, students confidentially completed a 10-question pretest survey about barriers to screening for IPV. They placed a confidential, self-chosen 4-digit number on the survey, which enabled posttest result correlation. The survey tool utilized a 5-point Likert-type scale (1 =strongly disagree, 5 =strongly agree) designed to examine barriers to assessing for IPV (Table 3). This tool was adapted for brevity and for student simulation from The Physician Readiness to Manage Intimate Partner Violence (PREMIS), which has been used to assess IPV knowledge, training, behaviors and attitudes of health care providers (Short et al., 2006). The PREMIS tool is a reliable, comprehensive 15-minute survey that measures physician readiness to manage IPV clinically. The tool measures perceived preparation for IPV situations, perceived knowledge, actual knowledge, and provider opinions about IPV related topics. Provider opinions include perceived barriers, practice issues, victim safety and autonomy, self-efficacy, legal requirements, and perceived preparation. The publicly available PREMIS tool can be used to measure the effectiveness of IPV educational programs. The pre- and posttest that was adapted for this simulation scenario measured family and psychiatric nurse practitioner students’ opinions including perceived preparation, self-efficacy, victim safety and autonomy, practice issues, and barriers. The scenario received an exemption from further review from the university’s institutional review board.
Comparison of Pre- and Posttest Survey Results (p = .05).
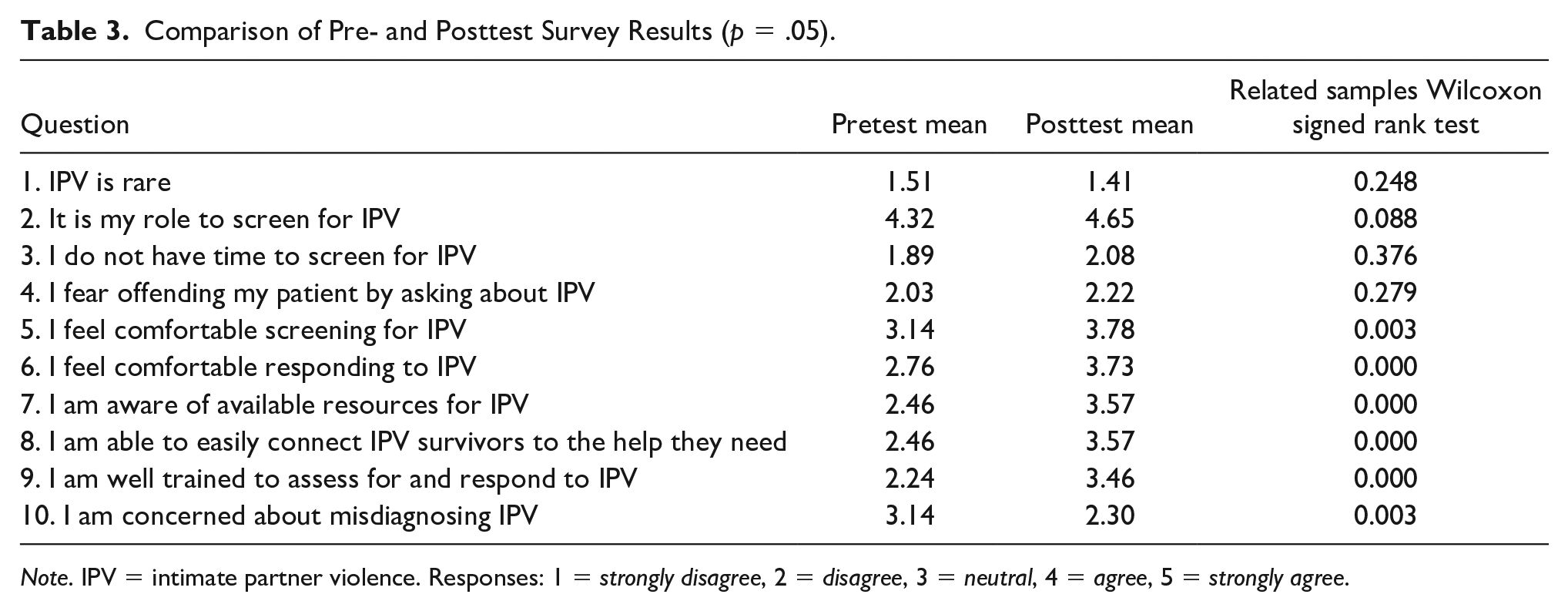
Note. IPV = intimate partner violence. Responses: 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree.
Prebriefing and Debriefing
Prior to the start of the scenario students were given permission to leave the room if the scenario triggered any unwelcome response or became too intense for them. Although no student left the scenario, faculty was prepared with counseling and other resources should this need have arisen. After the scenario was completed, the students, actor and faculty discussed the encounter. The 3D model of debriefing (Zigmont et al., 2011) builds on Kolb’s experiential learning theory. This model emphasizes defusing (exploring the emotional impact of the experience), discovering (gentle probing the learner about their thought processes during the scenario), and deepening (how can what was learned be connected to actual practice). The students used reflexive observation to consider their roles as advanced practice registered nursing students and the importance of empathy is a situation such as this. Dealing with a stressful situation and an emotionally painful encounter were also frequent themes in the debriefing. The actor provided feedback on how she felt as the “patient” and whether or not she felt the student was empathetic.
Results
Of the 50 participants, 37 completed both the pre- and posttests. Thirteen students either declined to complete the survey, completed the pretest but not the posttest, or did not include a matching number on the posttest for correlating the results with the pretest. The pre- and posttest data were analyzed using a matching pairs Wilcoxon signed-rank test via SPSS software. Result analysis showed that the simulation scenario produced statistically significant improvement in questions 5, 6, 7, 8, 9, and 10 on our survey. The students indicated that, after participating in the scenario, they felt more confident screening and responding to a disclosure of IPV. After the simulation they were more aware of, and readily able to connect survivors to, available local IPV resources. Resources included mental health, financial, legal, shelter, career support, and safety planning. Students felt well trained to respond to IPV postsimulation compared with before the training. Students felt less concerned about misdiagnosing IPV postsimulation. There was not a statistically significant change in Questions 1, 2, 3, and 4. The students acknowledge it is their role to screen for IPV both before and after participating in the scenario. Each participant disagreed or strongly disagreed that IPV was rare before and after the simulation. They disagreed or strongly disagreed that there is not enough time to screen for IPV. They were not concerned about offending patients by inquiring about IPV (Table 3).
Discussion
In their landmark qualitative study, Rodriguez et al. (1996, p. 156) quoted a woman who had been hospitalized with injuries: When I was physically hurt, I was put in the hospital and the physicians there did absolutely nothing to help me realize I was battered—or took time to talk to me. They just took care of what the injury was at the time and that’s it.
The provider may not have felt comfortable discussing IPV or was afraid of misdiagnosing it. As IPV is more prevalent than diabetes in our society, it is important that providers are able to knowledgably yet gently ask patients about their injuries and provide resources, such as a safety plan, to those in need. Students are unlikely to encounter IPV survivors in their clinical site, as the patients may be even more unlikely to disclose such information to a student. Providing advanced practice registered nursing (APRN) students the opportunity to participate in a simulated IPV scenario prepares them to identify and address IPV clinically. They will forever recognize the importance of screening by asking gentle probing questions, listening without judgement, and providing safe and timely resources for the patient to pursue.
Limitations
The fact that the scenario was a face-to-face encounter may be considered either a limitation or an advantage as the pandemic has forced many previous in-person encounters to be transitioned to telehealth. The scenario can easily be adapted to a telehealth platform. The participants in our simulation were APRN students, although undergraduates may also encounter IPV in certain settings. We limited our scenario to IPV. Other types of abuse, such as elder abuse and child abuse could also be brought to the simulation suite. A more complex scenario would involve children in the home and a discussion on consulting with child protective services. A disadvantage to our study was that 13 of 50 participants failed to accurately complete both the pre- and posttest surveys. Assuring that matching legible identifiers were on both surveys would have increased our response rate.
Conclusions
Unfortunately, IPV is common in our society. It is becoming more common with emotional and financial stressors and the need to “shelter-in-place” due to the COVID-19 pandemic. APRN students need to be able to diagnose IPV, assess and manage patients’-related injuries, discuss safety planning, refer the survivor to mental health provider, and provide resources to survivors. These skills do not come without experience. PMHNP and FNP students who engaged in a simulated IPV scenario in their clinical practicum course demonstrated increased self-efficacy, competence, and confidence in addressing this violence. They also became familiar with the safety-centered, empathic, and gentle yet persistent response necessary to address both the physical injuries and the emotional and safety needs of the patient.
Footnotes
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.