
Abstract
Background:
Tobacco continues to have a deleterious impact on health outcomes in the United States. Professional nurses at all levels of practice have an opportunity to be a part of the solution. The development of nurse-specific competencies for treating tobacco use disorder (TUD) disorder is long overdue. A task force of American Psychiatric Nurses Association (APNA) subject matter experts was assembled to engage in the process of reviewing the available peer-reviewed literature and additional evidence-based resources (e.g., professional organization position statement, toolkits, national survey results) to create the Nursing Competencies for Treating Tobacco Use Disorders.
Objective:
The aim of this article is ultimately to improve patient access to quality, evidence-based TUD nursing care by all nurses who are competent, full partners in TUD multidisciplinary care.
Method:
Search terms were defined and a scoping search and review of the TUD literature and resources was performed from November 2018 to November 2020.
Results:
Over 300 articles and evidence-based resources (e.g., professional organization position statements, toolkits, etc.) were discovered. Thirteen competencies were developed and were internally and externally reviewed prior to APNA Board of Director’s approval.
Conclusion:
TUD competencies have the potential to guide nursing education, practice, and research, allowing nurses to be full partners in the design, development, and implementation of effective TUD treatment.
Tobacco use disorder (TUD) continues to claim almost a half-million lives annually in the United States. Additionally, 16 million more are living with serious medical illnesses due to smoking. Although some progress has been made in reducing smoking rates, high levels of morbidity and mortality remain. According to the Centers for Disease Control and Prevention (CDC, 2019e), the current rate of overall smoking in the general population of the United States is 14.0%. Evidence-based practices (EBP) are available for treating TUD, however, intricacies of treatment and limited accessibility create barriers to implementation (Sheffer et al., 2021). Adding further complexity, existing data on trends in tobacco use do not always include issues associated with novel tobacco use devices such as electronic nicotine delivery systems (ENDS; i.e., Vape pens, JUUL, ENDS; Substance Abuse and Mental Health Services Administration, 2019; U.S. Department of Health and Human Services, 2020). These issues may confound understanding of tobacco use and treatment options.
Tobacco-related health disparities disproportionately cause health problems for vulnerable populations, including people who experience mental health disorders. Thirty-five percentage of people diagnosed with mental health disorders report using tobacco (CDC, 2019h). Myths and misperceptions related to how quitting may affect psychiatric symptoms leads to missed opportunities to address TUD (Malone et al., 2018; Sheals et al., 2016).
Improving the lives of persons living with mental illnesses has long been the focus of many nurses who provide mental health care. The American Psychiatric Nurses Association (APNA) has supported and supplied continuing nursing TUD treatment education. In 2008 APNA, in collaboration with the Smoking Cessation Leadership Center, facilitated an initiative drawing attention to nursing education and training for treating TUD. By 2014, APNA efforts coalesced around restructuring member activities about addictions care. The Addictions Council was formed and member efforts on treating tobacco use was organized as the Tobacco Dependence Branch of the Addictions Council. In 2018, in response to a white paper on the need for standards of TUD nursing care, APNA formed a task force (TF) to focus on improving nursing engagement in treating TUD.
This article has three main purposes: (1) to describe the TF processes in constructing the competencies, (2) to provide the reader with a glimpse of key evidence that supports each competency, and (3) to provide the reader with an overview of the gaps in the literature and next steps to take. Table 1 contains the list of approved competencies. A link to the competencies and supportive statements can be found free of charge by nurses and other clinicians regardless of membership status, on the APNA resource page (see Table 2). Readers of this article are encouraged to refer to the large body of research from evidence-based literature, professional organizational policy and position statements, research findings in national databases, and input from subject matter experts (SME) with the understanding that this evidence was foundational in creating each competency.
Nursing Competencies for Treating Tobacco Use Disorders (TUD).
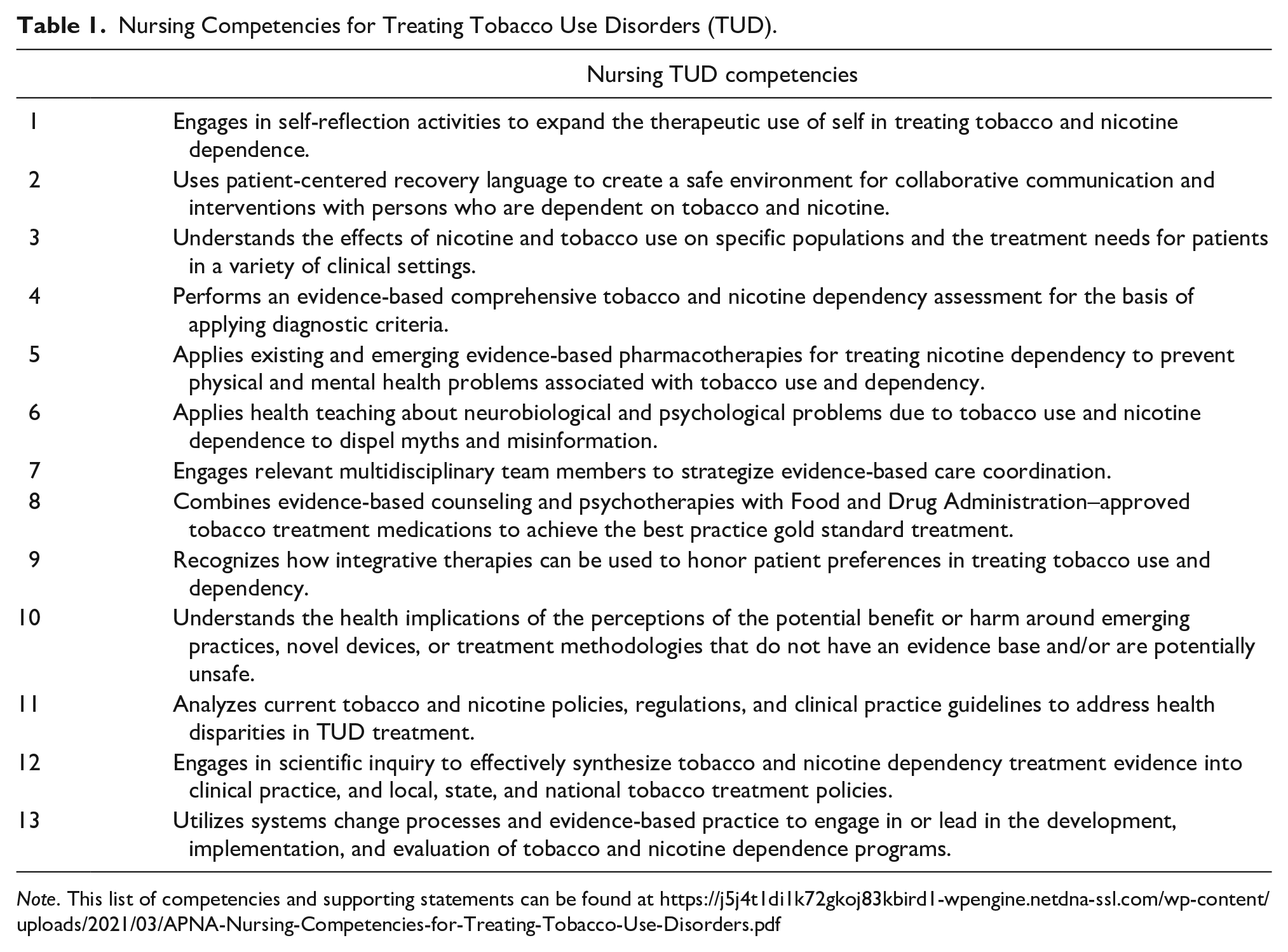
Note. This list of competencies and supporting statements can be found at https://j5j4t1di1k72gkoj83kbird1-wpengine.netdna-ssl.com/wp-content/uploads/2021/03/APNA-Nursing-Competencies-for-Treating-Tobacco-Use-Disorders.pdf
Helpful Links for Accessing Additional Tobacco Use Disorder (TUD) Resources.
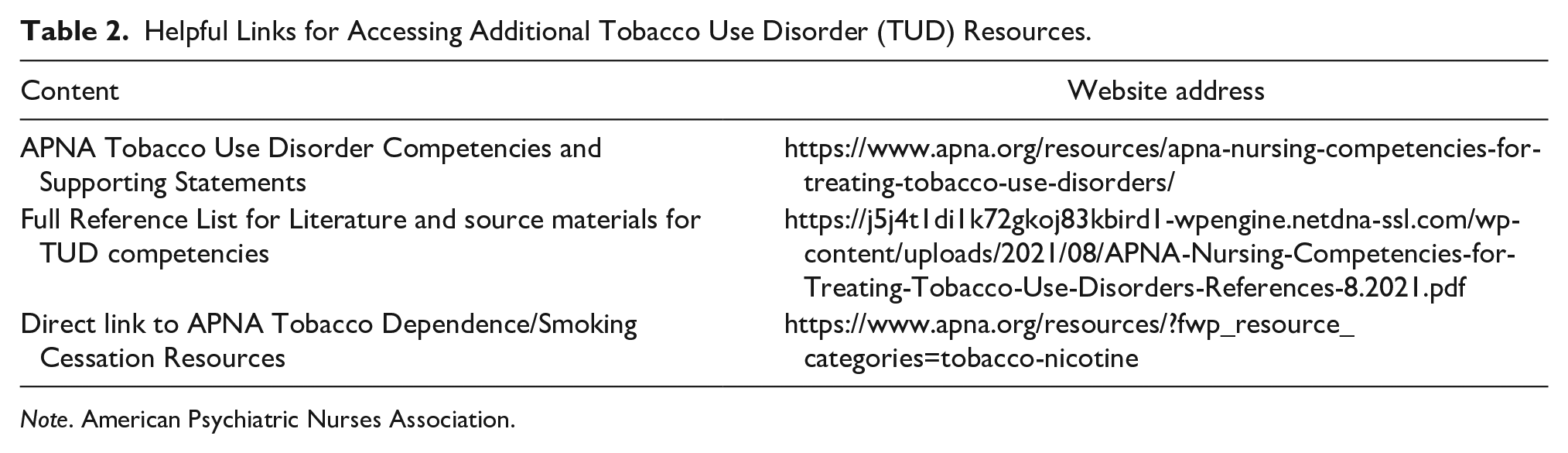
Note. American Psychiatric Nurses Association.
Task Force Processes, Methods, and Results
Processes
During the initial weekly meetings, TF members sought to define the parameters of the groups’ efforts and the general standards that would guide the group’s work and outcomes. It was clear from the onset that any resulting recommendations should support safe nursing practice within the psychiatric mental health nursing (PMH RN/ PMH APRN) scope and standards of nursing practice (American Nurses Association et al., 2014). Themes such as those contained in the nursing process, ethics, education, EBP, quality of practice, communication, leadership, collaboration, professional practice evaluation, resource utilization, and the environment of health were evaluated as applicable to TUD nursing care.
To further maximize TF efforts, developmental processes similar to those used by other APNA committees who developed other competencies and education were examined. Methods employed to search for and collect existing evidence were discussed. The TF members agreed to meet weekly to work on this project, beginning in November, 2018.
While being mindful of the terminology to be used, a distinction by the TF members between nursing competencies and nursing guidelines helped clarify efforts. Guidelines serve as treatment recommendations, steps to follow, and tasks to be completed (Fukada, 2018). Competencies integrate knowledge, values, attitudes, professional judgment, and skills (Fukada, 2018) and serve as a foundation to promote scholarship through translation of evidence into clinical practice. Nursing guidelines (Registered Nurses’ Association of Ontario, 2017) and competencies (i.e., Association for the Treatment of Tobacco Use and Dependence [ATTUD], Rx for Change) already exist. ATTUD has a certificate program available to multidisciplinary clinicians meeting application criteria. However, no current nursing-specific TUD competencies are found in the literature. TF members sought to create parameters for TUD nursing care that would go beyond steps to follow and tasks to be completed. While being careful to adhere to standards of nursing practice TF members sought to create opportunities for nursing leadership and innovation. Therefore, development of nursing specific TUD competencies validated by objective information and scientific inquiry is warranted.
Initially, the most challenging work of the TF was to describe a phenomenon observed when working with patients—noted as anecdotal evidence that eludes clear explanation. This phenomenon is described as a lagging sense of TUD treatment urgency and limited adoption of current evidence-based TUD treatment information by nurses. Multiple factors likely contribute to this, one of which may be that it can take decades for adverse health issues to emerge from smoking. This leads to a sense that there is time to treat TUD later—to a point that TUD is then not addressed until a devastating health issue occurs (Choi & Stommel, 2017). Another factor contributing to this lagging sense of urgency may be a false belief that TUD is a personal choice and not an addiction (Hughes et al., 2018). Adding to the problem is the common occurrence of treatment failure, which many falsely attribute to patients not being motivated to want to quit when evidence shows patients are very interested in quitting (Chaiton et al., 2016).
Additionally, nurses are taught to screen for TUD, provide a brief intervention, and refer the patient to treatment (i.e., screening, brief intervention, and referral to treatment [SBIRT]; Schwindt et al., 2019). The TF discussed the possible unintended outcomes of this approach. SBIRT may influence TUD nursing care by giving nurses the impression that because they will be referring the patient to another clinician, there is little need for them to add to their busy practices by spending time learning more about TUD treatment. This information served as an additional impetus to ensure that effective treatment of TUD became a standard part of nursing care and thus the development of nursing competencies.
Methods
The TF engaged in an initial comprehensive review of the published and in-press literature and digital media starting in November, 2018. Data were discovered via CINAHL, PubMed, and Medline. Search terms included key concepts from standards identified in the 2014 Psychiatric–Mental Health Scope and Standards of Practice (i.e., assessment, diagnosis, outcomes, etc.). Also included were a variety of terms related to TUD (i.e., nicotine, smoking, smokeless tobacco, noncombustible tobacco, e-cigarettes, ENDS, JUULS, etc.). The type of literature found in peer-reviewed journal articles and textbooks was evaluated using the Johns Hopkins Evidence Level and Quality Guide (Dang & Dearholt, 2018).
Early TF efforts led to the recognition that other evidence-based literature should be considered. Search efforts expanded into a scoping review of multiple sources of information. These sources included materials from SME discussion boards (e.g., ATTUD, Society for Research on Nicotine and Tobacco, Global Bridges). Sources include qualitative and quantitative research, clinical practice guidelines (CPGs), policy statements, professional organization toolkits, consensus opinions, and findings from national committees. Also included were TUD treatment works completed by a wide variety of professional national, and international health care organizations such as the American Society of Addiction Medicine, American Heart Association, American Lung Association, the CDC, and others. Inclusion of valid literature and materials was ongoing until time of submission of competencies to APNA Board of Directors in November, 2020. The competencies were approved by the APNA Board of Directors after being internally reviewed by APNA SME and then was externally reviewed by key stakeholders (e.g., CDC, Smoking Cessation Leadership Center). Updating the existing literature is ongoing as effects of ENDS use and COVID-19 unfold and new TUD evidence emerges daily.
Results
Over 315 literature sources were discovered. Using the Johns Hopkins Evidence Level and Quality Guide (2018) to describe the types of source materials found, there were 29 Level I peer-reviewed studies (i.e., randomized controlled trials [RCT], mixed methods, systematic reviews of RCTs, etc.) included in the literature search. Twenty-four Level II sources (i.e., quasi-experimental, systematic reviews of combination RCT and quasi, etc.) were examined. Level III studies (nonexperimental reviews of RCTs, qualitative analyses, etc.) made up the largest portion of literature with 131 sources. There were 53 Level IV studies (opinion of respected authorities, CPGs, consensus and position statements) included. Seventy-eight Level V sources were included (nonresearch evidence, experiential, integrative reviews, QI program evaluations, etc.). Effort was devoted to understanding the potential causes and identifying specific areas where nurses should become competent in treating TUD. As evidence was collected and reviewed, the TF recognized the value of structuring the competencies in an order that focused on maximizing the potential effect of a specific competency on nursing practice. Discussion centered on what specific competency would support maximum patient benefit while being mindful of the already busy nurses in practice. The TF was also mindful of the limited availability of TF member volunteer time, funding, and resources that would be required to integrate TUD content into nursing education and practice.
Overview of Key Research Influencing TUD Nursing Competency Development
After lengthy discussion about the order of competencies, the consensus was that to maximize efforts, it is necessary for nurses to examine and resolve biases, myths, and misinformation about TUD and TUD treatment. The delivery of effective treatment starts with recognizing the likely harmful nature of TUD and consistently and accurately assessing for it. Discussions about the current state of TUD nursing knowledge led TF members to a metaphoric description.
Competency 1
Analogous to pulling a thread on an old sweater, the risk of inadequately assessing the importance and need for TUD treatment increases the risk of inconsistent quality of care delivery. The therapeutic relationship and safe recovery environment may not be consistently developed. This may lead to limited, or no TUD treatment occurring. Subsequently, there may be a lack of TUD treatment supportive systems and structures put into place. Continuing with the pulled thread metaphor, without prioritizing TUD nursing education and its consistent delivery, research efforts may get stymied. As a result, TUD policies, guidelines, and regulation may lag behind needed guidance. Therefore, the first competency focuses on literature about self-reflection to expand therapeutic use of self once personal biases are recognized and addressed.
The literature focuses attention to deleterious effects of inconsistent individual and institutional attention and commitment to effective TUD treatment. A more thorough explanation of these inconsistencies may be possible but are beyond the scope of this article. While mindful of other possible influences, the inconsistencies are described by the TF as a form of bias.
Bias is a common thread (Bowes et al., 2020; Buetow, 2019) that runs through TUD care, leading patients to feel stigmatized and unwelcome in accessing care, specifically for members of vulnerable populations (Ashford et al., 2019; Hammet et al., 2018). Inconsistent attention to bias, an overconfidence in skills bias, and misperceptions (Cassam, 2017; Krosnick et al., 2017) about the primary importance of TUD treatment contributes to missed teachable/reachable treatment opportunities. Unbiased nursing efforts are needed to improve population health outcomes, update policies, guidelines, and set educational academic and clinical TUD treatment standards.
Institutional bias is apparent on a larger scale. Health care facilities overtly demonstrate attention bias in the selection of the national performance measures they will monitor. Sarna et al. (2020) concisely describes this, observing that the nation’s top hospitals have not voluntarily selected to monitor tobacco treatment episodes of care as a standard measurement despite the Joint Commission recommendations to do so. Facilities not monitoring and inconsistently making TUD treatment a priority may result in facility nurses being inadequately educated. Treating tobacco use as a secondary need and misperceptions that TUD is a personal choice, rather than a physical addiction that requires a recovery-oriented approach, may be one potential explanation (Sheals et al., 2016).
Competency 2
Increasing amount of literature sources drew TF attention to the importance of creating an effective recovery environment. Therefore, the next (second) competency focuses on recovery language to create a safe, effective, and accessible treatment environment. TUD treatment success improves as individuals feel safe to accurately self-disclose their tobacco use. Coffey et al. (2019) conducted a cross-national comparative study of the values of a recovery-focused environment, finding that increasing emphasis on recovery ideas and language increases therapeutic contact time. This promotes personalized recovery care planning. Therapeutic use of self is crucial for creating hope when patients become so discouraged about past failures, they are resistant to trying yet another quit attempt. A valuable, validated therapeutic approach that is taught and used by some nurses is motivational interviewing;
Blame-laden language used in terms of treating TUD is deeply engrained in our culture and nomenclature (Lefebvre et al., 2020; Wilson, 2020). One prime example is the use of the term “smoking cessation.” This terminology implies a scenario wherein the delivery of one treatment episode or series should mean the patient quits forever. This is not usually the case—it takes multiple quit attempts to achieve long-term quitting success (Piper et al., 2020). As a result, nurses become frustrated with the (erroneous) perception of patient resistance or lack of motivation. Meanwhile, the person who relapsed is embarrassed or ashamed to be forthcoming, and reluctant to return for assistance. When they do finally return, they are often sicker and more discouraged. Using a neutral term such as “tobacco treatment” more accurately reflects the reality of quitting challenges. Yet it is difficult to change this linguistic habit even amongst seasoned TUD treatment professionals.
Using recovery-oriented language to treat TUD expands possibilities of improving population health outcomes related to TUD. A gap in the literature exists about recovery as a central focus of a TUD treatment environment beyond concepts and use of recovery-oriented, unbiased language. Recovery competent nurses are better prepared when caring for vulnerable populations who may have difficulty accessing care.
Competency 3
A plethora of literature about who smokes provided the impetus for the next competency, as it became clear that vulnerable populations were at higher risk (CDC, 2019a, 2019b, 2019c, 2019d, 2019e, 2019f, 2019g, 2019h). Competency three addresses the unique challenges of vulnerable populations. These population cohorts are reflective of social determinants of health that test the delivery of TUD treatment (CDC, 2018; 2019a, 2019b, 2019c, 2019d, 2019e, 2019f, 2019g, 2019h; Drope et al., 2018; Weinberger et al., 2017). A small sampling of literature sources describing the distinct challenges experienced is provided here and the reader is encouraged to access the body of knowledge cited on the APNA resources page (see Table 2).
Vulnerable populations and some of their unique TUD challenges include (but are not limited to): persons living with mental illnesses (Okoli et al., 2017), persons of racial and ethnic minorities (CDC, 2019b; Giovanni et al., 2015; Mills et al., 2018), and members of the lower socioeconomic populations and those with less education (CDC, 2019c, 2019e, 2019f, 2019g, 2019h; Jahnel et al., 2019; O’Keefe et al., 2019; van Wijk et al., 2019). Persons who identify as LGBTQ (lesbian, gay, bisexual, transgender, and queer) make up about 3% of the U.S. population yet approximately 20.5% reported smoking cigarettes (CDC, 2019g). These individuals experience both internalized stressors and external stressors related to discrimination and stigma, putting them at higher risk to smoke (American Lung Association, n.d. 2020; U.S. Food and Drug Administration, 2019).
A myriad contributing factors also sabotage access to care. The role of chronic stress in vulnerable populations complicates development and implementation of effective evidence-based treatments. Social inequality, stigma, and chronic stress is associated with discrimination and must be addressed to improve successful treatment. Inconsistencies in TUD education and training of mental health professionals and lack of high-level evidence continues to perpetuate tobacco-related treatment disparities (Prochaska et al., 2017). It is important for nurses to become competent in the nuances adversely affecting vulnerable populations (Patnode et al., 2021).
Competency 4
For treatment to be effective for any health condition, interventions must be based on a thorough evidence-based assessment and subsequent application of diagnostic criteria. A growing body of literature supported this as the focus of the fourth competency. Nurses are taught to do the “5As” (Ask, Advise, Assess, Assist, and Arrange) to screen for tobacco use. While intentions are good, these strategies are habitually delivered without much intent of going beyond initial close-ended tobacco use screening. Advice to quit is obligatory and nurses proceed to inadequately assess, assist, and arrange TUD treatment. Nurses are generally unaware of quitting resources for patients beyond the national quitline (1-800-QUITNOW; Bialous et al., 2017).
As previously discussed, the SBIRT is a referral to treatment to another clinician, usually at a different location. This missed nursing opportunity adds extra steps for the patient to complete, and for modestly motivated patients this is a bridge too far. The unspoken message to the nurse is, “someone else will do this, there is little reason for me to learn more about this.” Assessment for TUD may be further minimized by its inclusion in a larger assessment (i.e., screening tools for other substances used; Gryczynski et al., 2017). TUD care could be improved when nurses reach competency in performing a thorough TUD assessment.
As the TF acquired literature about pharmacotherapy, it became clear that less effective TUD assessments leads to less than effective TUD treatment and outcomes. This unfortunate scenario gains momentum as nurses erroneously assume they are adequately assessing TUD, then treatment (pharmacotherapy and counseling) lacks specificity. TUD pharmacotherapy then often fails, which contributes to TUD medications being ordered at abysmally low rates (Sarna et al., 2020). Poor health outcomes are sustained, care takes longer than it should, and nurses become less sure of what to do because their treatment efforts have not been successful.
Competency 5
Thus, the fifth competency concentrates on pharmacotherapy interventions for treating TUD. When nurses practice to the full scope and standards of their graduate or undergraduate education and training, treatment is more likely to be successful. Medications used appropriately have long been shown to improve quit rates (Fiore et al., 2008). Understanding how nicotine (the addictive chemical in all forms of tobacco) works (Preedy, 2019) is essential to successful TUD pharmacotherapy. Medications such as nicotine replacement therapy (NRT) are often either not prescribed at all, are under prescribed, or are not prescribed for a long enough time frame to support successful quitting (Gupta et al., 2019; Umesh & Nagesh, 2016).
Unchallenged myths held by some nurses include mistaken beliefs that nicotine causes cancer (it does not). Nurses often lack awareness about the nicotine content in tobacco products and the treatment implications related to nicotine content and individual metabolism (Fucito et al., 2014). Nurses may be unaware of novel uses of TUD pharmacotherapies, that is, progressive patch dosing prior to quitting (Przulj et al., 2018), and ordering NRT as something precontemplative patients have to “opt out” of leads to successfully quitting (Cheung et al., 2015). It is noteworthy that one category of TUD treatment medications, NRT, is available in three over-the-counter formulations. Yet nurses are inconsistently educated on standard NRT dosing (Malone et al., 2019).
Important practice distinctions are made in translating medication information into clinical practice. The TF recognizes that there are differences that stem from the scope and standards of undergraduate- versus graduate-level nursing practice and licensure regulations. Graduate nurse practitioners must possess competency of pharmacokinetics and pharmacodynamics of medications, the metabolism and excretion systems, implications of specific diseases affecting medication metabolism, and side effects. Nurses with prescriptive privileges and TUD treatment education can offer other FDA-approved medications, such as bupropion or varenicline (Cunningham et al., 2016). Competent nurses can effectively teach and answer patient (and colleague) questions, safely and effectively pass and/or prescribe TUD medications precisely to the individual’s needs. This delivers a sizable solution to problems with stagnating quit rates.
Competency 6
In the search of literature and resources, the TF discovered an abundance of information on knowledge about effective TUD treatment. Health teaching of both nurses and patients is the emphasis of the sixth competency. Due to heavy workloads and limited TUD content in academia nurses may not be aware of literature with pragmatic, clinically useful information. The Surgeon General’s Report (U. S. Department of Health and Human Services, 2020) confirms TUD comorbidities that nurses have recognized for years (i.e., lung cancer, severe respiratory diseases, heart disease, etc.). However, nurses may not know that smoking is now confirmed as an independent risk factor for devastating diseases such as type 2 diabetes, macular degeneration, several types of cancer (not just lung cancer), and ectopic pregnancies (Preedy, 2019; U. S Department of Health and Human Services Surgeon General’s Report, 2020).
Nurses who are engaged in public health education can help reduce adverse health and economic outcomes of TUD-related diseases. The multiple physiological effects of nicotine, its legal availability, and corporate marketing to promote sustained use contribute to misinformation and myths about cigarettes and ENDS. These include the belief that “cold turkey” is the best cessation method; use of NRT prolongs addiction, and that ENDS are not addictive (Prochnow, 2017). A systematic review (Ye et al., 2017) found that providing nicotine and tobacco education and interventions resulted in improvement in health care provider’s knowledge, attitudes, behaviors, and skills (Ye et al., 2017).
As trusted health care providers, PMH RNs and PMH APRNs can inform patients and families that TUD is a chronic health condition best treated with a combination of pharmacotherapy and behavioral health counseling. Nurses are ideally situated in clinical positions to provide long-term, consistent support during the treatment process despite slips or relapses. Health teaching occurs in an array of settings via a variety of delivery methods. Teaching occurs in moments when nurses provide valid brief interventions (Lepage et al., 2015) during teachable moments and includes opportunities yet conceived by future nurses.
Competency 7
Competency 7, the role of nursing in multidisciplinary teams is inconsistently defined in the literature. The TF coalesced around the importance of nurses having a “full partnership seat at the table” for the opportunities to advocate for TUD treatment priority. Rosell et al. (2018) advocates for improved role clarity of team members and increasing focus on whole patient care as a means of improving outcomes. Innovative nursing interventions such as guided self-help strategies (Simmons et al., 2018) and nurse-led community teams (Shishani et al., 2019) demonstrate long-term success presenting and nursing opportunities (Binnal et al., 2018). Nurses can use the treatment team meetings to dispel myths and misinformation as they arise before they can perpetuate and negatively affect patient outcomes.
Competency 8
The evidence was found on what is known as the gold standard of TUD treatment; pharmacotherapy and supportive counseling, which is the eighth competency. In 2008, a revision of the CPG for treating TUD was published (Fiore et al., 2008) providing clinicians with access to knowledge of effective TUD treatment. This information was and still is not consistently conveyed to graduate and undergraduate nurses (Savage et al., 2018; VanDevanter et al., 2017). This results in chronic inconsistency of quality and delivery of TUD care and poor population health outcomes.
It is unclear why nurses inconsistently use CPGs. A targeted search of the literature falls short in finding current studies on the lack of widespread nursing adoption of the 2008 TUD treatment CPGs. It has been the observation of several TF members and other SME that nurses, especially prescribing nurses, are often unaware of 2008 TUD CPG treatment recommendations, or are skeptical (show bias) about TUD treatment efficacy. If the gold standards of TUD treatment are not taught, implemented, and evaluated in general practice setting, treatment opportunities will be missed especially among the most vulnerable.
Competency 9
Despite receiving gold standard TUD care, a return to using tobacco is not uncommon (Piper et al., 2020). In their quest to find what works for them, patients seek out treatments that can be integrated into their physical and mental health care. Evidence found on this topic (Eaves et al., 2017; Jang et al., 2019) is the focus of the ninth competency. Such treatments are commonly referred to as “alternative” or “complementary” or “integrative” therapies (National Center for Complementary and Integrative Health, 2021). These therapies have not been evaluated as extensively or rigorously as conventional medicine (Muramoto et al., 2016). Many nurses receive extra training in and use complementary therapies as part of their holistic nursing practice to reduce stress and anxiety (Barnes et al., 2019: Frisch & Rabinowitsch, 2019). This may be useful as many patients smoke to manage anxiety and stress.
Evidence shows that nurses generally have a favorable view of the use of alternative, integrative, or holistic nursing practices (Balouchi et al., 2018). Nurses need to be informed about complementary approaches that are monitored by but do not have current FDA approval. The evidence for use of integrative or complementary therapies for TUD is mixed and also confounded by the placebo effect phenomenon, which is difficult to confirm in integrative therapy studies. Some evidence supports the effectiveness of complementary therapy when combined with empirically valid treatment, such as auricular acupuncture combined with NRT (Hyun et al., 2018). To respect and honor patient autonomy in choosing TUD treatment, nurses need to answer patients’ questions about alternative or complementary interventions with scientific evidence, including caution for use, while refraining from influencing decisions based on nurses’ opinion or experience.
Competency 10
Literature emerges nearly daily on new products such as ENDS and other novel products such as “heat not burn” products (Auer et al., 2017; Lee et al., 2020). TF members realized that nurses need competency about the use of these products to provide information and support to patients and colleagues, therefore this became the 10th competency. The public is being inundated with mixed messages on potential benefits or harms around emerging practices, novel devices, and treatment methodologies (Chest Foundation, 2021; Shiffman & Auguston, 2021). There is a plethora of existing and emerging literature (see Table 2 for link to evidence) expressing strongly held pro/con opinions among TUD treatment professional about the use of these devices and the potential harm from them. Since the introduction of ENDS the industry has grown exponentially, devices have been refined, and evolved to a fourth generation of products. ENDS contains nicotine, colors, flavors, aromas, other chemicals, including those causing cancer (Jensen et al., 2017).
Many illicit substances have been synthesized or liquefied and added to e-liquid or “juice” to increase appeal (McDonald et al., 2016). Unregulated commercial ENDS vendors can keep secret the list of varying chemicals in devices and product labels are not always correct (Nguyen & Aamodt, 2018; Prochnow, 2017). Achieving competency of this area requires ongoing updates. The long-term results of using novel products such as ENDS is closely monitored. The CDC (2020) continues to investigate, finding cases of severe pulmonary disease, referred to as e-cigarette, or vaping, product use-associated lung injury (EVALI). As of 2020, there were 2,478 reported cases of EVALI with 64 cases resulting in death (CDC, 2020).
New nicotine delivery systems, such as “heat not burn” products (Auer et al., 2017; Lee et al., 2020), are being created and used without oversight. It is important to consider risks and harms associated with ENDS. The clear harms from ENDS are made more alarming because of inconsistent regulation of chemical contents, laws and policies restricting sales to minors, and lack of clear and consistent treatment guidelines (Cardenas et al., 2016; Jenssen et al., 2019). It will require effort for nurses to sustain accurate knowledge of these devices and products due to the rapidity of emerging evidence. Nurses must have a role in creation of ENDS-related policies and treatment guidelines.
Competency 11
In the evidence collected by the TF, there was a growing body of knowledge about policy development as being critical to support treatment and regulation. This became the 11th competency. To deliver evidence-based TUD interventions that benefit patients, nurses benefit from understanding and using TUD health care policies, regulation, and CPGs (CDC, 2018; CDC, 2019a). Research suggests, however, that most nurses are inconsistently competent in implementing EBP (Melnyk et al., 2018; Pereira et al., 2018). Barriers to implementing TUD nursing interventions include lack of training (Meijer et al., 2019) and biases that hinder adherence to TUD treatment CPG and policies (Evers-Casey et al., 2019).
An area of potential for nurses to lead is related to the observations made by Sarna et al. (2020), who found that TUD treatment national performance measures are infrequently adopted even by top-rated health care facilities (2.7% in 2018 and 1.9% in 2019). In top hospitals monitoring provision of treatment, just 40.4% of patients in 2018 and 38.7% in 2019 received TUD care recommended by the Joint Commission (Sarna et al., 2020). The responsibility to lead is within the nursing scope and standards of practice and nurses can advocate to have health care systems that monitor and make improvements in patient TUD programming, based on nationally recognized standards.
As nurses become more knowledgeable about policymaking, opportunities emerge to challenge the status quo and engage in shaping TUD facility policies. Graduate-level nurses engaged in policy management can mentor other nurses on the importance of policies and policymaking. Nurses are in unique position to identify and address issues with public’s health, collect data, support policy development or change, advocate for laws, and implement guidelines (Fairchild et al., 2019; Jenssen et al., 2019; Prochnow, 2017). Nurses who analyze policies, regulations, and CPGs can create individualized, recovery oriented, unbiased TUD nursing interventions to address health disparities.
Competency 12
The TF search yielded an expanding body of literature on the importance of scientific inquiry in TUD use and treatment issues. This became the focus of the 12th competency. Understanding and communicating evidence is a crucial part of nursing as a scientific discipline. Nurses who understand the science about TUD and TUD treatment have an opportunity to engage in policy, regulation, and CPG development. Charania et al. (2019) emphasized the importance of incorporating EPB in clinical assignments to improve outcomes and promote undergraduate nursing students’ professional self-concept. Nursing engagement in the use and practice of scientific inquiry to address TUD issues and treatment sends a powerful message to stakeholders (i.e., patients, employers, government researchers, and policy makers) that nurses can lead TUD treatment in a comprehensive and systematic way.
To practice at full scope and standards of education and licensure (AMERSA, 2018), nurses have the opportunity and professional obligation to regularly read, discuss, understand, utilize, test, and implement TUD interventions. Reading, understanding, and applying TUD-related research has become more complex over time. For example, tobacco and pharmaceutical company sponsor studies, which may or may not include bias about a product. A recent example of this practice is the special issue of the American Journal of Health Behavior (Shiffman & Augustson, 2021), that was financially sponsored by the company who manufacturers the ENDS product named JUUL. To competently use research findings in practice, nurses need to learn how to objectively examine and critique scientific literature addressing TUD and TUD treatment.
Competency 13
The last, 13th competency utilizes the significant amount of evidence found on systems-level changes needed to improve TUD treatment (Malone et al., 2018; Malone et al., 2019). A systems-level opportunity exists for improved TUD health outcomes with enhanced knowledge of TUD treatment strategies among all nurses. Nurses who are motivated could obtain expertise to champion continuous updates and dissemination of TUD issues and TUD treatment. Having TUD treatment nurses readily available could result in significant improvements in access to quality treatment. This can lead to improved population health especially among persons who experience tobacco-related chronic illness (CDC, 2019d). Nurses who are competent in TUD treatment, research, and policy development can answer the invitation to engender systematic changes improving health care practices, outcomes, and the quality of life of Americans.
Nunn et al. (2020) assert that 5% of U.S. citizens accounted for half of all U.S. health care spending in 2017 and costs are higher among people living in poverty—often related to chronic diseases. People who use tobacco are often poor and suffer more chronic illnesses (CDC, 2019d), which are costly in time, money, and effort to treat. Nurses competent in TUD treatment, research, and policy development can answer the invitation to engender systematic changes improving health care practices, outcomes, and the quality of life of Americans.
Limitations
Structural factors (i.e., TF meetings occurred across several time zones, no prior defined process instructions) may have contributed to some of the limitations of this study and article. Limitations include the decision to keep literature searches within 5 years (note that TF activities started in November, 2018 and proceeding until November, 2020). The resulting TF work may have missed influential or older, foundational sources. Literature searches were expanded beyond the established systematic review and scoping review standards to capture a representation of the enormous amounts of information on TUD and TUD treatment resources. This effort may not have secured and considered all available evidence. Accurately describing and searching for rationale for lagging adoption of up-to-date TUD treatment was challenging and may not fully represent true reasons behind inconsistent adoption of tobacco treatment practices by nurses.
Implications for Nurses and Next Steps
The American Association of Colleges of Nursing (AACN; 2021) recently published an update of the essential domains and competencies for graduate and undergraduate nurses. The new AACN essentials embrace competency-based education, stating, “Achieving a specific competency gives meaning to the theoretical and assists in understanding and taking on a professional identity” (AACN, 2021, p. 4). This philosophy aligns with early decisions by the TF to pursue the creation of competencies rather than guidelines—using nursing theories (e.g., Benner’s novice to expert) and health behavior change theories, to guide the individual nurse’s judgement, attitude, and application of theory supporting practice.
Sheffer et al. (2021) studied effects of specialized education and training and noted improvements in consistency, quality, and access to TUD care. Nursing credentialing organizations and other specialty organizations provide for undergraduate-level certification (e.g., ambulatory care, addiction, psychiatric, care-coordination, etc.) and several graduate-level nurse practitioner certifications. The nursing competencies for treating tobacco use and dependency may serve as a critical part of the curriculum for a future certification for nurses. Having a high percentage of certified nurses assists health care systems meet criteria to achieve sought after “Magnet” status. For nurses practicing in the clinical setting, intensive education and training serve as a foundation for nurses to develop TUD treatment expertise. These “champions” can then disseminate and role model competent TUD nursing practice, education, and research—perhaps facilitating a “grassroots” normalization of consistent evidence-based TUD treatment. Dedicated TUD treatment nurse champions can increase advocacy for sustained, timely treatment to, “every patient, in every setting, every time” (APNA Tobacco Treatment Mission Statement).
The aim of the competencies is to improve patient access to quality, evidence-based TUD nursing care. Development of nursing-specific TUD education reflecting the competencies is an obvious next step. Competency educational activities provide opportunities to exchange misinformation that perpetuate poor health outcomes. TUD treatment competent nurses can translate evidence into practice during teachable/reachable moments. Competencies can open doors for improved knowledge, skills, and attitudes for every nurse of any academic preparation. Opportunities open for nurses seeking advanced, specialized TUD knowledge to champion TUD initiatives in practice with individuals, and families.
Nurses comprise one of the largest health care disciplines and can lead improvements in population health outcomes (MacKinnon et al., 2020). Moving forward, opportunities for nursing innovation emerge as nurse champions engage in novel use of media and other resources to deliver pragmatic TUD education and treatment. Nurses in TUD treatment strategies can provide a cohesive, unified nursing “voice” serving in multidisciplinary activities. Disseminating nursing TUD treatment knowledge raises discipline visibility and credibility. Since nurses are increasingly welcomed at local, state, and national policy development organizations, a logical progression would include nurses contributing to policy change. These recommendations are the next steps to take in succession or simultaneously to translate TUD treatment nursing competencies into practice.
Conclusions
The available evidence and pertinent literature support the value of discipline-specific TUD education and training (Meijer et al., 2019). TUD is inconsistently treated by nurses. The reasons for this are complex and may include the near constant flow of new TUD information, persistent misperceptions, and the already overburdened nurses in practice. Compounding these problems is the inconsistent integration of evidence-based TUD treatment strategies in nursing education. The purpose of this article was to describe the rationale and processes used by the TF to examine current evidence on the need for competencies and the subsequent development of evidence into the Nursing Competencies for Treating Tobacco Use and Dependence. The recommended next steps include developing and empirically testing curriculum for disseminating the competency curriculum options. Nurses are invited to use this opportunity to integrate TUD competencies into education for practice to change the trajectory of health outcomes.
Footnotes
Author Roles
CE, CB, JH, and MRS conceived the project, determined the methodology, critically discussed implications of the collected literature, and designed the TUD competencies. SA critically discussed implications of the collected literature, contributed significantly to the writing of select competencies, and designed the TUD competencies. CE took the lead in writing and organizing the manuscript. All coauthors contributed significantly to the project and writing of the manuscript. All coauthors reviewed the final manuscript before submitting for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.