
Abstract
Background:
Long-acting injectable antipsychotics (LAIs) are unique and effective pharmacological treatment options for schizophrenia that are underutilized in clinical practice. Research surrounding prescriber barriers to the underuse of LAIs are limited to a few seminal studies which identified psychiatric prescriber barriers to the use of LAIs as knowledge deficits, uninformed attitudes, and poor prescribing practices. There is a gap in the literature regarding effective educational interventions to target the identified psychiatric prescriber barriers to the use of LAIs.
Aims:
The study aimed to develop a web-based educational toolkit that would positively affect the knowledge, attitudes, and practices of psychiatric prescribers regarding LAIs.
Methods:
A one-group, before and after design with a convenience, purposive sample of 17 psychiatric prescribers to assess the knowledge, attitudes, and practices (KAP) using a 20-item KAP questionnaire before and after a presentation of a web-based educational toolkit about LAIs was chosen.
Results:
The web-based educational toolkit slightly improved the total and three subscales KAP scores of psychiatric prescribers. However, only the difference in total KAP scores was found to be statistically significant.
Conclusions:
The developed and evaluated web-based educational toolkit could provide a foundation for positive change to psychiatric prescribers’ KAP regarding LAIs.
Keywords
Introduction
Long-acting injectable antipsychotics (LAIs) are unique and effective pharmacologic treatment options for those with schizophrenia, yet they are underutilized in clinical practice (Correll et al., 2016) by prescribers. Oral antipsychotics are the primary pharmacologic treatment for schizophrenia, but nonadherence is a common problem associated with relapse, rehospitalization, and worsening of the course of schizophrenia (Haddad et al., 2014; Patel & David, 2005). Medication nonadherence is a barrier to achieving positive outcomes for those with schizophrenia (Emsley, 2013), and prescribers frequently overestimate adherence with oral antipsychotics (Taylor et al., 2018). The percentage of individuals that are nonadherent to oral antipsychotics is high and varies between 40% and 90% (Agid et al., 2010, as cited in Taylor et al., 2018). Patients that are nonadherent to oral antipsychotic medication have five times the risk of relapse (Caseiro et al., 2012, as cited in Morrissette & Stahl, 2012).
Relapse in schizophrenia remains an enormous public health challenge and affects health care costs and life quality for those with schizophrenia (Kane et al., 1998). Prevention of relapse for those with schizophrenia requires uninterrupted, long-term pharmacological management with antipsychotic medication. LAIs assure continuous adherence with antipsychotic medication and serve as a practical solution to the common clinical issue of antipsychotic nonadherence in those with schizophrenia (Patel & David, 2005).
The underuse of LAIs denies those with schizophrenia of pharmacological treatment options that have been proven to improve adherence and decrease relapses, rehospitalizations, ER visits, and psychotic symptom severity (Buckley et al., 2015; Lafeulle et al., 2013; Lafeulle et al., 2016; Lin et al., 2019; Poloni et al., 2019; Subotnik et al., 2015). LAIs have the potential to decrease the personal suffering, family burden, and societal costs associated with schizophrenia.
The reasons for the underutilization of LAIs are not entirely understood. There is limited research regarding the barriers to the use of LAIs perpetuated by psychiatric prescribers. The existing research that examined the views psychiatric prescribers had of LAIs hypothesized that the knowledge deficits, uninformed attitudes, and poor prescribing practices among psychiatric prescribers were barriers to the use of LAIs (Ciglar et al., 2016; Correll et al., 2016; Heres et al., 2006; Iyer et al., 2013a, 2013b; Llorca et al., 2013; Miles et al., 2011; Patel et al., 2003; Patel et al., 2020; Sajatovic, Ross, Legacy, Byerly, et al., 2018; Sajatovic, Ross, Legacy, Correll, et al., 2018; Samalin et al., 2016; Weiden et al., 2015). There is a gap in the literature regarding effective educational interventions to target the knowledge deficits, uninformed attitudes, and poor prescribing practices of psychiatric prescribers that contribute to the underuse of LAIs. The purpose of this study was to develop and evaluate a web-based educational toolkit on the knowledge, attitudes, and practices (KAP) of psychiatric prescribers.
Review of Literature
There are only a few formative studies that investigated the psychiatric prescriber barriers that contribute to the underuse of LAIs in clinical practice. Those studies hypothesized that psychiatric prescriber barriers to the use of LAIs in clinical practice were related to knowledge deficits, uninformed attitudes, and poor prescribing practices (Ciglar et al., 2016; Correll et al., 2016; Heres et al., 2006; Iyer et al., 2013a, 2013b; Llorca et al., 2013; Miles et al., 2011; Patel et al., 2003; Patel et al., 2020; Sajatovic, Ross, Legacy, Byerly, et al., 2018; Sajatovic, Ross, Legacy, Correll, et al., 2018; Samalin et al., 2016; Weiden et al., 2015). Understanding the KAP of psychiatric prescribers regarding LAIs is instrumental in determining their influence on the use of LAIs so appropriate interventions to target those barriers can be created.
Heres et al. (2006) conducted a survey study on 246 psychiatrists that examined why LAIs were not chosen as a treatment option for those with schizophrenia or a schizoaffective disorder. Reasons for not prescribing LAIs included concern for extrapyramidal symptoms, patient refusal, and patient adherence to oral antipsychotic medication (Heres et al., 2006). The survey also revealed that 64.5% of the psychiatrists had never offered a LAI to eligible patients (Heres et al., 2006). Researchers concluded that the reported reasons for not prescribing LAIs were unsupported by evidence-based knowledge (Heres et al., 2006).
In a qualitative study by Iyer et al. (2013b), the attitudes of 24 psychiatrists from Canada regarding LAIs were explored through a questionnaire and focus group. Information gleaned from the questionnaire revealed that psychiatrists prescribed oral antipsychotics more than LAIs, did not frequently offer LAIs as a treatment option, had limited LAI prescribing experience, and would only prescribe a LAI if there were no other option (Iyer et al., 2013b). Psychiatrists reported believing that patients would refuse LAIs, be unconvinced about their benefits, fear pain, be aversive to needles, and interpret the suggestion of their use as a lack of trust by the psychiatrist (Iyer et al., 2013b). Researchers hypothesized that psychiatric prescribers’ lack of knowledge and experience with LAIs, lack of offering of LAIs to patients, and personal biases about LAIs might contribute to their underuse (Iyer et al., 2013b).
Miles et al. (2011) conducted a two-phase, qualitative study that examined psychiatrists’ attitudes and knowledge from New Zealand regarding the LAI Risperdal Consta and the impact of their attitudes on their prescribing practices. There were significant discrepancies in psychiatrists’ initiation, dosing, titration, and monitoring strategies, indicating that guidance on utilizing the Risperdal Consta was needed (Miles et al., 2011). Many psychiatrists reported negative perceptions of Risperdal Consta. They described it as a last resort option, which impaired the psychiatrist–patient relationship and was unpleasant due to needle administration (Miles et al., 2011). This study revealed the varied and limited knowledge, negative attitudes, and poor prescribing practices of psychiatric prescribers regarding the LAI Risperdal Consta.
Patel et al. (2020) conducted a questionnaire study to investigate the beliefs and attitudes of 136 European physicians regarding the acceptance and usage of LAIs for the treatment of schizophrenia. Physicians reported an increase in their utilization of LAIs within the past 5 years but reported offering oral antipsychotic treatment more than a LAI (Patel et al., 2020). The prescribing of LAIs was directly correlated to physician attitudes regarding LAIs (Patel et al., 2020). The researchers concluded that psychiatric prescribers’ poor attitudes regarding LAIs influence patient acceptance of LAIs and, ultimately, psychiatric prescriber usage (Patel et al., 2020).
The formative research studies that investigated the KAP of psychiatric prescribers regarding LAIs revealed valuable information about psychiatric prescriber barriers to the use of LAIs. Psychiatric prescribers’ knowledge, attitudes, and prescribing practices regarding LAIs greatly influence their patients’ acceptance of LAIs. Barriers to the use of LAIs are the knowledge deficits, uninformed attitudes, and poor prescribing practices of psychiatric prescribers.
A gap in the literature exists regarding interventions to alleviate the knowledge deficits, uninformed attitudes, and poor prescribing practices of psychiatric prescribers that are barriers to the use of LAIs in clinical practice. Psychiatric prescribers need education to improve their KAP regarding LAIs. The management of LAIs can be complicated and requires specific knowledge about practical issues such as dosing and switching to a LAI (Correll et al., 2016); there are insufficient data and recommendations within the literature (Llorca et al., 2013). “Tailored education about LAIs should be developed for different groups of professionals who interact with patients, including physicians, nurse practitioners, nurses, physician assistants, pharmacists, social workers, residents, peer counselors, and others” (Correll et al., 2016, p. 21). Psychiatric prescribers should have easy access and evidence-based education about LAIs to offer and prescribe them as a treatment option for those with schizophrenia. Development of education to address psychiatric prescribers’ knowledge deficits, uninformed attitudes, and poor prescribing practices that prevent LAIs from being utilized as a treatment option in those with schizophrenia is needed. Studies have indicated that the use of toolkits can facilitate translation of evidence into practice (Yamada et al., 2015), and web-based education has shown promise at improving the knowledge, attitudes, and practices of medical professionals (Madsen et al., 2014).
Theoretical Framework
The Knowledge to Action (KTA) Framework was the foundation of this study. Graham et al. (2006) developed the KTA Framework as a guide to optimizing the transfer of research findings into practice so patients could receive the best evidence-based treatment. It is composed of two concepts, knowledge creation and action (Graham et al., 2006).
The knowledge creation concept of the KTA Framework funnels through three phases: knowledge inquiry, knowledge creation, and knowledge tools. The phases represent synthesis of knowledge into a useful tool that meets identified needs (Graham et al., 2006). Within this study, the knowledge creation concept was illustrated by the development of a web-based educational toolkit regarding LAIs. The action cycle concept of the KTA Framework is a feedback loop that moves through activities leading to the implementation of the knowledge tool (Graham et al., 2006). The phases of the action cycle are identify the problem, adapt knowledge to the local context, assess barriers to knowledge use, select, tailor, and implement intervention; monitor knowledge use, evaluate outcomes, and sustain the knowledge use (Graham et al., 2006). The developed web-based educational toolkit regarding LAIs was tailored to target and overcome the knowledge deficits, impaired attitudes, and poor prescribing practices of psychiatric prescribers that contribute to the underutilization of LAIs. After implementation of the toolkit, its’ effectiveness was evaluated by measuring change in knowledge, attitudes, and practices of psychiatric prescribers. The KTA Framework and the concepts and phases which comprise it were utilized within the methods of this study to assist with the process of bringing evidence into practice.
Method
Study Design
The study was an interventional, one-group, before and after, quasi-experimental design. The web-based educational toolkit regarding LAIs and the accompanying presentation were developed using Microsoft PowerPoint. It was embedded in a seven-part module created using Moodle, an online open-source learning management system.
Institutional Review Board, Consent, and Ethical Considerations
The institutional review board reviewed the study before initiation and found it to be exempt. Permission was obtained from the organization that owns the online professional nursing membership forum where a recruitment announcement and invitation for participation in the study were posted. All participants were voluntary and online consent was obtained before participants viewed the web-based intervention. No risks or discomforts were anticipated for participants except for the time associated with participation, which was estimated to be approximately 30 minutes.
Setting
The setting was any location where participants could access and complete the web-based study. All components of the module were housed on Moodle.
Sample
A convenience, purposive sample of 17 psychiatric prescribers, recruited through word of mouth and via an online professional nursing organization member forum, was utilized. Inclusion criteria were a professional designation as a prescriber of psychiatric medication. The only exclusion was not being a prescriber of psychiatric medication.
Instrumentation
To study the impact of the web-based presentation of an educational toolkit on the knowledge, attitudes, and practices of psychiatric prescribers regarding LAIs, the following tools were developed:
A web-based educational LAI toolkit and presentation were created using PowerPoint and evidence-based information to enhance psychiatric prescribers’ knowledge, attitudes, and practices regarding LAIs. The toolkit was composed of the following elements: an overview of LAIs, review of evidence-based literature about LAIs, prescribing tables for each of the nine LAIs available in the United States based on information from the manufacturers, myths about LAIs, manufacturer websites, advantages of LAIs, disadvantages of LAIs, websites containing guidelines and an algorithm for the treatment of schizophrenia, resources for patients and psychiatric prescribers, and tips on how to engage patients in shared decision making conversations about LAIs. Content validity of the web-based educational toolkit was established by submission to experts for evaluation and was based on content, clarity, and organization. The experts were a board-certified psychiatrist and psychiatric mental health nurse practitioner with years of experience prescribing LAIs. The toolkit was finalized following suggested modifications from the consulted experts.
A 20-item KAP questionnaire was created using the content of the web-based educational LAI toolkit. The KAP questionnaire was composed of three subscales. The first subscale included 11 knowledge questions. The second subscale included six attitude questions. The third subscale included three practice questions. All questions were true or false. The 20-item KAP questionnaire was based on a 56-item, preexisting knowledge and attitudes questionnaire regarding LAIs. Eleven of the 20 items in the KAP questionnaire were directly used or modified from the preexisting knowledge and attitudes questionnaire. The 56-item questionnaire was based on and modified from a previous 44-item knowledge and attitudes questionnaire, which had excellent reliability based on the test–retest method and moderate internal reliability (Bawo et al., 2012). Permission was obtained from the author to utilize the knowledge and attitudes questionnaire. The content validity of the newly created 20-item KAP questionnaire was established by submission to the previously mentioned experts for suggestions and modifications. The questionnaire was tested for reliability before its use by the test–retest method with a 1-week interval and was found to have a good intraclass correlation coefficient.
A web-based module that consisted of seven parts was created using the online open-source learning management system, Moodle. Included in the web-based module was a brief description of the research project and intervention, a question to verify each participant as a prescriber of psychiatric medication with a yes or no option, a consent form with a yes or no option, multiple-choice demographic questions, the 20-item before KAP questionnaire, the presentation of the web-based educational LAI toolkit, and the 20-item after KAP questionnaire.
Data Collection
Data were collected using the web-based, 20-item KAP questionnaire administered before and after participants received access to the web-based educational toolkit presentation about LAIs. In the KAP questionnaire, there were 20 questions, all true or false, correct answers got 1 point, and incorrect answers got zero points. Knowledge questions were 1 to 11 (11 items), attitudes questions were 12 to 17 (six items), and practice questions were 18 to 20 (three items). The range for the total KAP score was 0 to 20, and the range for the three subscale scores were 0 to 11 for knowledge KAP subscale score, 0 to 6 for attitudes KAP subscale score, and 0 to 3 for attitudes KAP subscale score. Higher scores indicated better knowledge, more positive attitudes, and better prescribing practices of the psychiatric prescribers regarding LAIs. Demographic data were collected with five questions regarding age, sex, years prescribing medication, practice setting, and professional designation. All data were collected electronically by the web-based module created with and housed on Moodle.
The open announcement and invitation to participate in the study were posted on the online professional nursing organization member forum and sent via email to psychiatric prescribers found through word of mouth on July 24, 2020. Invitations were resent, and the open-announcement and invitation were reposted July 29, August 3, and August 10 of 2020. The announcement and invitation provided a URL link to the web-based module on the open-source learning platform, Moodle, which was available during the same 3-week time frame. Before accessing the web-based module on Moodle, participants were required to become a Moodle registered user, which necessitated consent to their user agreement and creation of a username and password. Data collection was concluded on August 17, 2020. Verification as a prescriber of psychiatric medication, consent, demographic data, and scores from each participant’s KAP questionnaire before and after viewing the web-based educational toolkit presentation were collected by and stored in the Moodle module. A personal email address identified each participant’s data. Email addresses were then deidentified by assigning each a unique numeric code from 1 to 17 before transferring the data to both a Microdoft Excel and a Statistical Package for Social Science (SPSS) file. All data were password protected.
Data Analysis
The purpose of the data analysis was twofold. The first was to determine if there were differences in the knowledge, attitudes, and practices of psychiatric prescribers (measured using the total and three subscales KAP scores) before and after the presentation of the web-based educational toolkit about LAIs. The second was to determine if there were associations between changes of knowledge, attitudes, and practices (measured as the differences in the after and before total and three subscales KAP scores) of psychiatric prescribers and any of their demographic factors. The data were imported into and analyzed using the Statistical Package for Social Science (SPSS) version 23 for Windows (IBM Corp).
Shapiro–Wilk tests were used to determine the normality of the data. As the data were not normally distributed, nonparametric procedures, including Wilcoxon signed-rank tests, were applied (Field, 2013). Wilcoxon signed-rank tests were performed to determine if there were differences in the knowledge, attitudes, and practices (measured using the total and three subscales KAP scores) of psychiatric prescribers before and then after the presentation of the web-based educational toolkit about LAIs. Mann–Whitney U tests (for categorical variables with two levels) and Kruskal–Wallis tests (for categorical variables with more than two levels) were used to determine if there were associations between changes of KAP (measured as the differences in the after the intervention and the before intervention total and three subscales KAP scores) of psychiatric prescribers and their demographic factors of age range, practice setting, professional designation, range of years prescribing medications, and sex. For all the utilized tests, a p value of less than .05 indicated statistical significance. All p values were two-sided.
Results
Power Analysis
A priori power analysis was conducted to determine the minimum number of participants required for a .80 power of finding statistically significant differences in the KAP of psychiatric prescribers before and after a presentation of the web-based educational toolkit about LAIs. The desired power of the study was .80. The power analysis was performed using G*power 3.1.9.4 (Faul et al., 2009) to determine the minimum sample size that was needed for this study. For a large effect size of 0.8 (Cohen, 1988, 1992) and an alpha level of .05, the minimum sample size needed to achieve a .80 power was 15 participants. The study recruited 17 participants, which was greater than the minimum sample size needed according to the power analysis to detect the effects hypothesized in this study, and hence this study had an adequate sample size.
Participant Demographics
A total of 25 participants registered for the study via Moodle. Out of the 25 participants that registered, eight were excluded from the data analysis. One participant completed the data collection but answered “no” to the question requesting consent to participate. Two participants did not answer all the demographic questions. Last, five participants did not complete the after KAP questionnaire. In the final data analysis, 17 participants were included after they consented to participate, verified themselves as a prescriber of psychiatric medication, viewed the intervention, and completed both the before and after the KAP questionnaire.
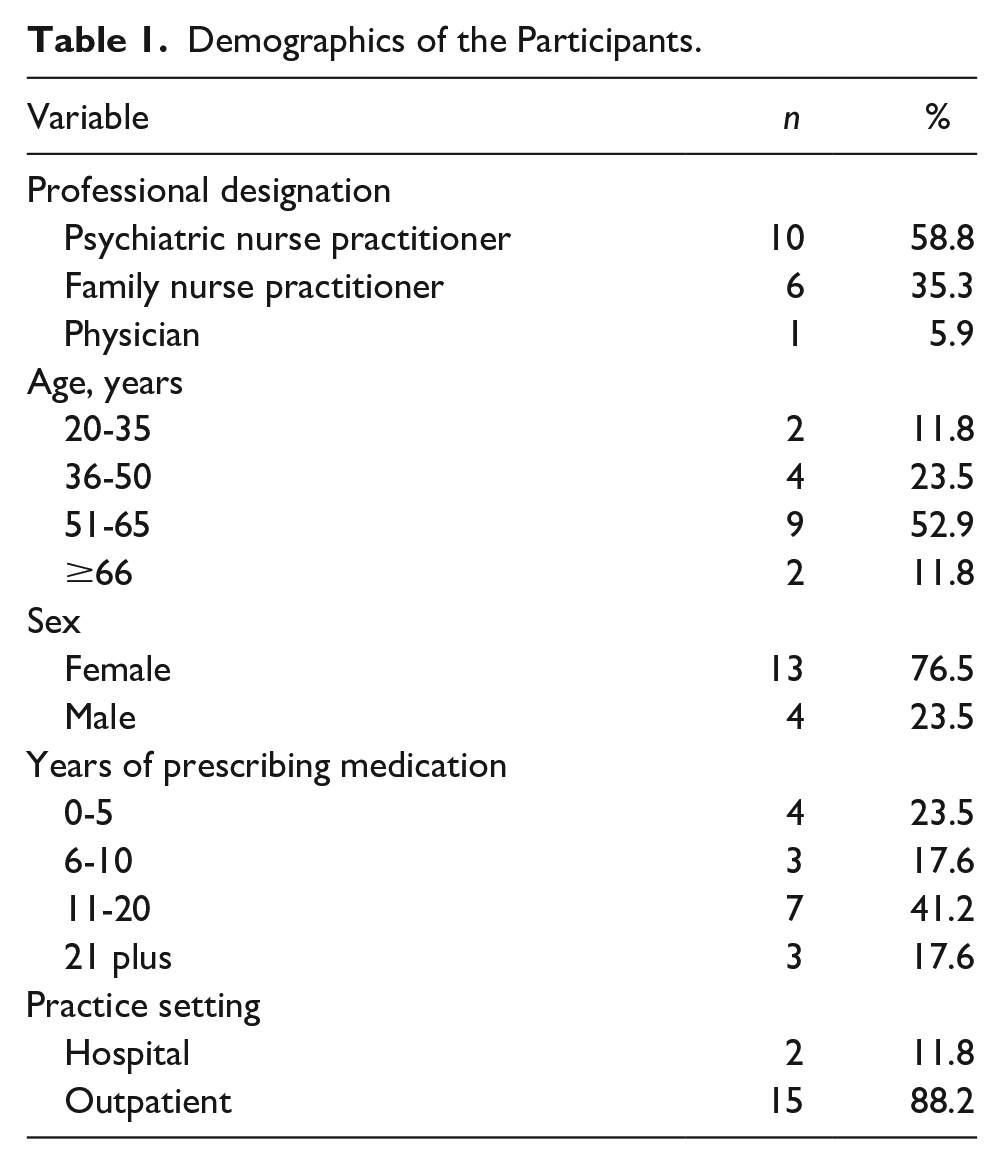
Table 1 shows the demographics of the participants. Nearly 60% of the participants (58.8%) were psychiatric nurse practitioners. Slightly over half of the participants (52.9%) were 51 to 65 years old. Most of the participants were female (76.5%) and practiced in outpatient settings (88.2%). Over 40% of the participants (41.2%) had prescribed medications for 11 to 20 years.
Demographics of the Participants.
Impact of the Web-Based Educational Toolkit on KAP Questionnaire Scores
Table 2 presents the descriptive statistics of the total and three KAP subscales scores before and after the presentation of the web-based educational toolkit about LAIs. The results of the Shapiro–Wilk tests indicated that except for the before total KAP scores (W = 0.919, p = .141), all the other data, including the before and the after knowledge KAP subscale scores, the before and after attitudes KAP subscale scores, the before and after practices KAP subscale scores, and the after total KAP scores, were not normally distributed (W ranged from 0.262 to 0.872, p < .05).
Descriptive Statistics of the Total KAP and Three KAP Subscales Scores.
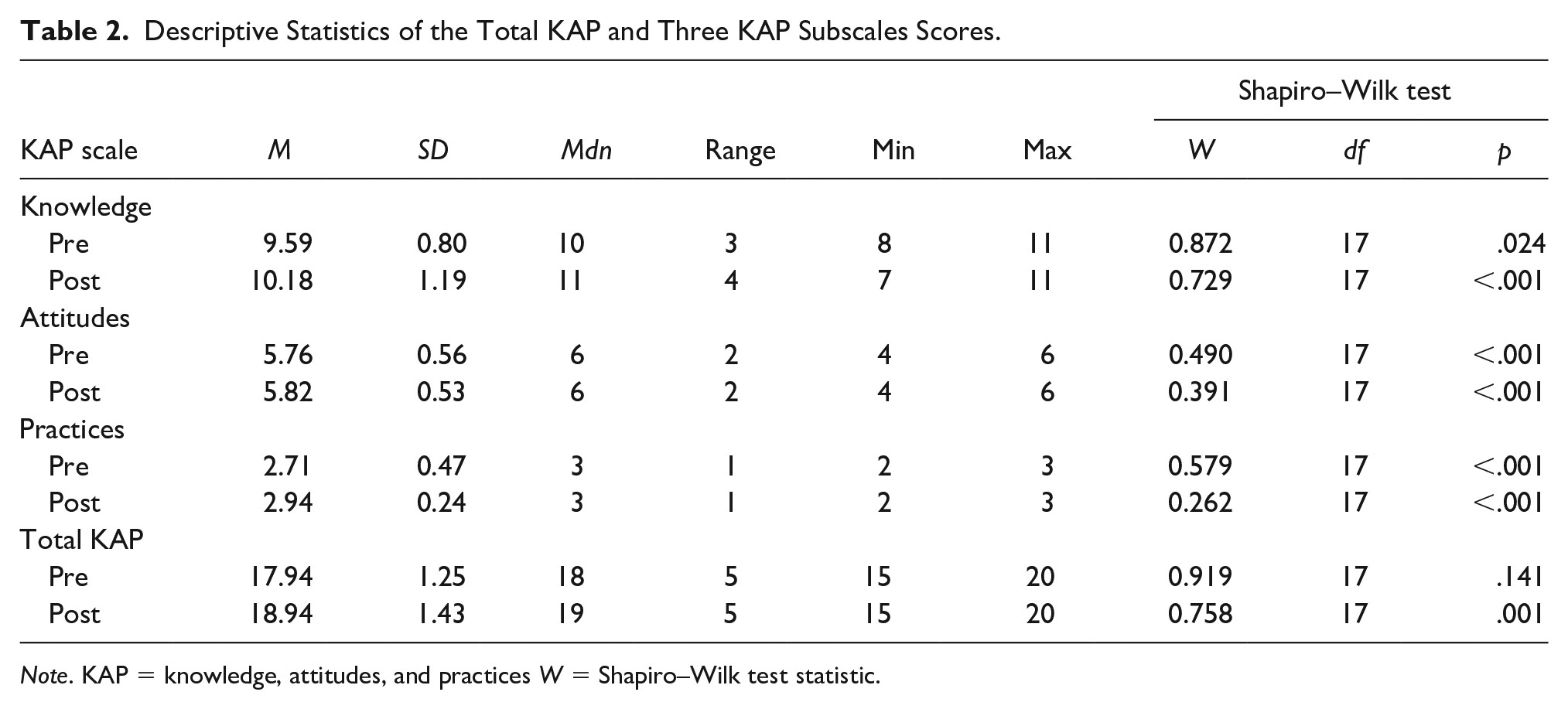
Note. KAP = knowledge, attitudes, and practices W = Shapiro–Wilk test statistic.
As not all the data were normally distributed, median and range were used to summarize the data. Median was used for the measure of central tendency, and the range was used for the measure of variation of the data. The median knowledge KAP subscale scores were 10 (range = 3) and 11 (range = 4) before and after the intervention, indicating participants had good knowledge regarding LAIs before and after the intervention. The median attitudes KAP subscale scores were 6 (range = 2) and 6 (range = 2) before and after the intervention, indicating participants had positive attitudes regarding LAIs before and after the intervention. The median practices KAP subscale scores were 3 (range = 1) and 3 (range = 1) before and after the intervention, indicating participants had good prescribing practices regarding LAIs before and after the intervention. The median total KAP scores were 18 (range = 5) and 19 (range = 5) before and after the intervention, indicating participants had good cumulative KAP regarding LAIs before and after the intervention.
Wilcoxon signed-rank tests were performed to determine if there were differences in knowledge, attitudes, and practices (measured using the total and three subscales scores of the KAP questionnaire) of psychiatric prescribers before and after the presentation of the web-based educational toolkit about LAIs. The results are presented in Table 3. There was no statistically significant difference in knowledge KAP subscale scores (T = 81.50, Z = 1.904, p = .057, r = .461), attitudes KAP subscale scores (T = 1.00, Z = 1.000, p = .317, r = .243), and practices KAP subscale scores (T = 1.00, Z = 1.000, p = .317, r = .243) before and after the presentation of the web-based educational toolkit about LAIs (Table 4). However, there was a statistically significant difference in the total KAP scores before and after the presentation of the web-based educational toolkit about LAIs (T = 110.00, Z = 2.933, p = .003, r = .711; Table 3). In particular, participants had statistically significant higher total KAP scores after the intervention (Mdn = 19, range = 5) than before the intervention (Mdn = 18, range = 5; Table 3).
Results of Wilcoxon Signed-Rank Tests.
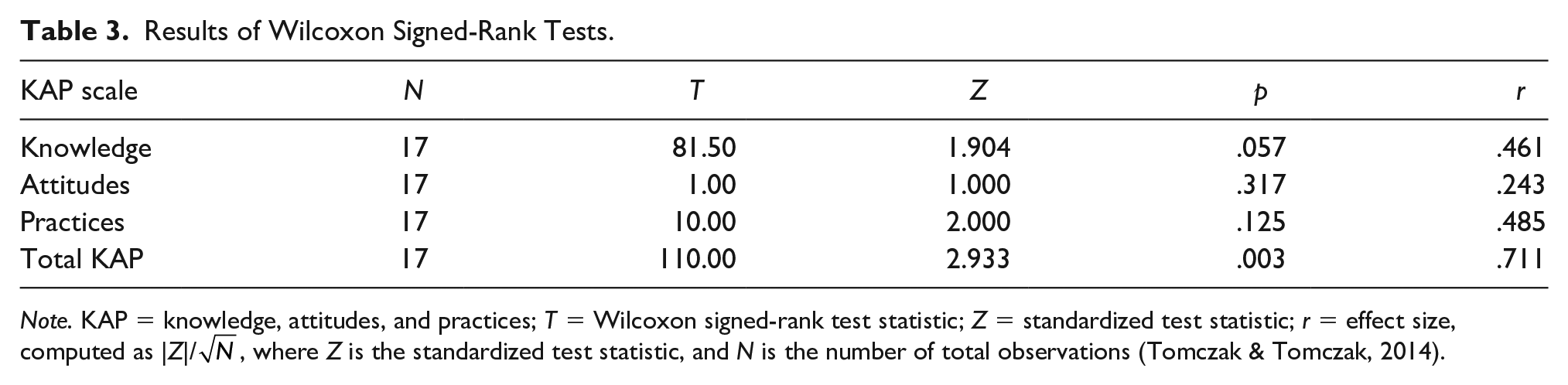
Note. KAP = knowledge, attitudes, and practices; T = Wilcoxon signed-rank test statistic; Z = standardized test statistic; r = effect size, computed as |Z|/
Results of Mann–Whitney U Tests for Determining if Differences in Total and Three Subscales KAP Scores (After–Before) Were Associated With Practice Setting.
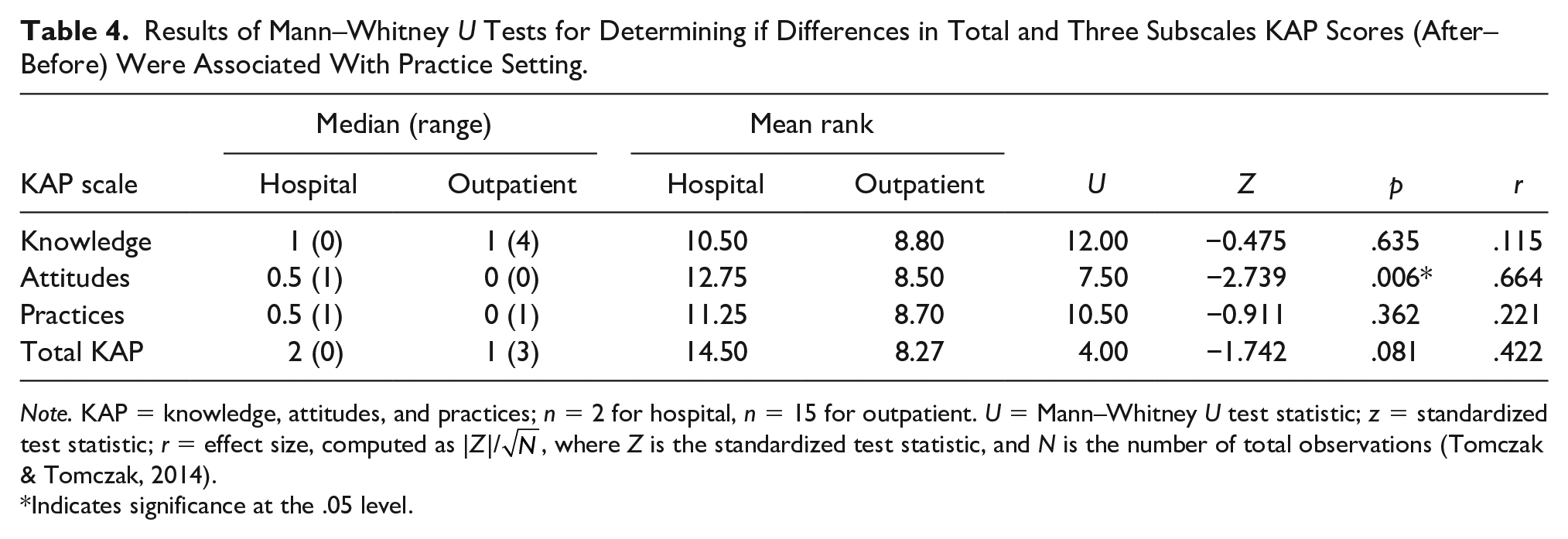
Note. KAP = knowledge, attitudes, and practices; n = 2 for hospital, n = 15 for outpatient. U = Mann–Whitney U test statistic; z = standardized test statistic; r = effect size, computed as |z|/
Indicates significance at the .05 level.
Association Between Change in KAP and Participant Demographics
Mann–Whitney U tests (for categorical variables with two levels) and Kruskal–Wallis tests (for categorical variables with more than two levels) were used to determine if there were a relationship between changes of KAP (measured as the differences in the after and the before intervention total and three subscales KAP scores) of psychiatric prescribers and demographic factors, such as age range, professional designation, range of years prescribing medication, practice setting, and sex. The median differences for the after and the before intervention attitudes KAP subscale scores were 0.5 (range = 1) and 0 (range = 0) for hospital and outpatient settings. There was an association between practice setting and differences in the after and the before attitudes KAP subscale scores (U = 7.50, Z = −2.739, p = .006, r = .664; Table 4). Those participants who practiced in hospitals had a statistically significant increase in attitude KAP subscale scores compared with the participants who practiced in outpatient settings.
Discussion
This study design was devised to develop and evaluate the impact of a web-based educational toolkit on psychiatric prescribers’ knowledge, attitudes, and practices regarding LAIs. The study aimed to develop a web-based educational toolkit for psychiatric prescribers to improve their knowledge, attitudes, and practices regarding LAIs. The research question of this study asked if the web-based educational toolkit would have an effect on the KAP of psychiatric prescribers regarding LAIs. The independent variable of this study was the presentation of the web-based educational toolkit regarding LAIs.
The dependent variables were the KAP of psychiatric prescribers. The outcome measures were the differences in the median total and three subscales KAP scores of participants before and after the presentation of the web-based educational toolkit regarding LAIs. This study’s analysis of the data revealed that the web-based educational toolkit regarding LAIs slightly improved the total and three subscales KAP scores of participants. It also showed that the total and three subscales KAP scores were adequate before and after the presentation of the web-based educational toolkit about LAIs (Table 2). The difference in the total KAP scores were statistically significant, with a p value of .003, but the differences in the three subscales KAP scores were not statistically significant (Table 3). Changes in the total and three subscales KAP scores from before to after the web-based educational toolkit presentation had no association with the participants’ demographic factors except for an association between practice setting and changes in attitudes KAP subscale scores of participants. Differences in the attitudes KAP subscale scores were statistically significant (p = .006) for participants working in hospitals compared with participants practicing in an outpatient setting (Table 4).
The web-based educational toolkit had a positive effect on the KAP of psychiatric prescribers regarding LAIs, as evidenced by the outcomes of the improved total and three subscales KAP scores. However, improvements were slight and only statistically significant when the totality of the improvements to KAP were combined as a total KAP score. Knowledge, attitudes, and practices are separate concepts but culminate to have an overall impact on the utilization of LAIs by psychiatric prescribers in clinical practice.
This study’s results both supported and contradicted aspects of the review of literature. The review of the literature revealed knowledge deficits, uninformed attitudes, and poor prescribing practices of psychiatric prescribers regarding LAIs (Ciglar et al., 2016; Correll et al., 2016; Heres et al., 2006; Iyer et al., 2013a, 2013b; Llorca et al., 2013; Miles et al., 2011; Patel et al., 2003; Patel et al., 2020; Sajatovic, Ross, Legacy, Byerly, et al., 2018; Sajatovic, Ross, Legacy, Correll, et al., 2018; Samalin et al., 2013; Weiden et al., 2015). The before total and three subscales KAP scores of participants revealed their baseline knowledge, attitudes, and practices regarding LAIs were adequate. Contrary to the review of literature, the psychiatric prescribers of this study had adequate KAP regarding LAIs, which may be related to the fact that the sample of psychiatric prescribers within the literature review were all psychiatrists. In this study, most participants were nurse practitioners. It raises questions about possible differences in education and training between psychiatrists and nurse practitioners regarding LAIs. Other confounding factors that may have contributed to the unexpected good baseline KAP of psychiatric prescribers regarding LAIs in this study include the date of and the various countries’ medical culture of the studies within the review of literature. This study was based on limited research from various countries conducted greater than 5 years ago. The time-lapse may have led to improved knowledge, attitudes, and practices of psychiatric prescribers. Compared with the medical culture of the United States, other countries’ medical culture could affect the differences in knowledge, attitudes, and practices regarding LAIs among psychiatric prescribers.
Limitations
There were several limitations associated with the design, process, and recruitment strategy of the study. The design of the study was not ideal since it was not a randomized controlled trial. The inclusion of a control group would have resulted in data fully representative of the intervention’s effectiveness. The one group, before and after design may have subjected participants to sensitization and not revealed the true effect of the web-based educational toolkit, but rather of the exposure to the KAP questionnaire.
The study’s process was complex and time consuming. Participants were required to access a computer with internet capabilities and register as a Moodle user. Independent completion of multiple steps by the participants were necessary to finish the module and all the data collection. Many participants were excluded from analysis of the data due to missing portions of the required data collection. This most likely occurred because participants were not automatically advanced but instead had to manually advance to the next portion of the data collection. Thus, making it easy to skip portions of the data collection inadvertently
Recruitment endeavors were unsuccessful and not representative of all psychiatric prescribers. Recruitment opportunities for psychiatric prescribers other than nurse practitioners were limited and resulted in a sample that was not diverse. In addition, the time frame and the specificity of the topic may have contributed to the lack of participation and resultant small sample size. Those who participated in the study were experienced prescribers, likely highly motivated, desirous of continuing education, and not fully representative of all psychiatric prescribers. Due to the lack of a control group, a limited number of participants, a complicated process, and the sample not being representative of all psychiatric prescribers, this study’s generalizability is limited.
Strengths
Though there were several limitations to this study that prevent generalization of results, it serves as the first step at addressing the gap in literature regarding the underuse of LAIs due to prescriber factors with the hope of mitigating those barriers in order to improve utilization. It further highlighted gaps in the literature regarding the use of LAIs by all psychiatric prescribers including nurse specialists, nurse practitioners, and physician assistants. Last, it supported the use of a web-based educational toolkit as a possible method to provide education to prescribers.
Implications for Future Research
This study serves as a catalyst for future research. To truly determine the effectiveness of the web-based educational toolkit on psychiatric prescribers’ KAP regarding LAIs it would have to part of a larger, randomized controlled trial study with a more inclusive sample of psychiatric prescribers. The web-based educational toolkit could be utilized in a performance improvement project to determine if the use of the toolkit translates into increased utilization of LAIs. Investigation is needed to determine the current factors that contribute to the underuse of LAIs in clinical practice by all psychiatric prescribers so they can be targeted and eliminated.
Conclusion
In conclusion, this study revealed that the developed and evaluated web-based educational toolkit could provide a foundation for positive change to psychiatric prescribers’ knowledge, attitudes, and practices regarding LAIs. However, the flaws within the design of the study prevent generalization of the findings. Still the study serves as an initial step in targeting prescriber barriers that contribute to the underuse of LAIs in clinical practice and in filling a gap in the literature.
Footnotes
Acknowledgements
Lisa Lewis would like to thank the psychiatric prescribers that volunteered their time to participate in this research.
Author Roles
LL and JR conceived the study and determined the methodology. LL collected the data and both authors analyzed the data. LL and JR wrote and organized the manuscript. Both authors reviewed the final manuscript before submitting for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Continuing Education
![]() to access the post-test, evaluation, and certificate.
to access the post-test, evaluation, and certificate.
The American Psychiatric Nurses Association is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.