
Abstract
Introduction:
Affecting more than 3.9 million Americans, the hepatitis C virus (HCV) attacks the liver by causing inflammation. Left untreated, HCV can lead to serious consequences. Targeting high-risk individuals in the inpatient psychiatric setting can lead to increased testing and referral.
Aims:
This quality improvement project determined whether an intervention—consisting of a pretest, educational session, posttest, and screening implementation—increased staff knowledge about HCV screening recommendations, identified at-risk individuals, and increased the number of patients screened and referred for treatment.
Method:
An online HCV educational session was provided to 30 staff at a Midwest regional psychiatric unit. An online pre/posttest was conducted to determine staff knowledge and understanding prior to and after the educational session. An HCV screening tool checklist was incorporated into the electronic health record (EHR) system. A 3-month pre/post-intervention chart review was completed to determine the number of patients identified and screened for HCV.
Results:
A comparison of the 30 staff members’ mean pre/posttest scores were calculated using an unpaired t test, showing a prescore mean of 55.15 ± 19.09 and a postscore mean of 85.75 ± 13.44, p < .001. A chi-square analysis indicated that there was a statistically significant post-intervention increase in the percentage of high-risk patients identified (5.6%–36.4%, p < .001) and screened (5.6%–31.4%, p < .001) for HCV compared with pre-intervention.
Conclusion:
The study intervention increased staff knowledge of HCV guidelines and the number of at-risk patients identified and screened for the disease.
Introduction
Problem Description
Hepatitis C virus (HCV) infection is a major public health concern, affecting more than 3.9 million Americans (Manjelievskaia et al., 2017). While HCV rates in the United States have been declining, statistics show it is on the rise again in young adults, mainly due to increasing intravenous drug use ( IVDU; Centers for Disease Control and Prevention [CDC], 2018). HCV is a blood-borne pathogen that can lead to acute or chronic liver disease, which can be prevented with routine HCV screening. According to a study by Girardin et al. (2021), patients who are hospitalized for a mental health illness have many risk factors for contracting HCV. HCV screening is often overlooked in psychiatric patients. By targeting individuals in the inpatient psychiatric setting, high-risk individuals can be identified, which would lead to increased testing and referral for treatment. Authors hypothesize that there is a low clinician adherence to screening for HCV due to lack of knowledge of CDC screening guidelines and treatment regimens. Given that the inpatient psychiatric unit was not routinely screening for HCV, project directors created a quality improvement project which screened this vulnerable population.
Available Knowledge
HCV is a serious, but often treatable health concern. HCV screening is crucial, as it can identify patients at earlier stages of the disease. Early identification of HCV increases treatment options, allows for the use of less expensive treatments that are effective prior to HCV progression, and helps reduce transmission risk. While HCV screening kits are cost-effective and readily available, they are not being used routinely by all health care agencies (American Association for the Study of Liver Diseases [AASLD], 2019). Since targeting only certain high-risk patients, such as those born between 1945 and 1965, will not necessarily increase HCV screening rates, the U.S. Preventive Services Task Force (USPSTF, 2000) expanded their recommendations to include all individuals at high risk for infection. While HCV screening is slowly increasing, the gains are not substantial, leaving ample room for improvement. In their serial, cross-sectional analysis of the National Health Interview Survey Population from 2013 to 2015, Kasting et al. (2018) determined that only 11.5%–12.8% of baby boomers were being screened for HCV. Another population at high risk for contracting HCV are individuals with mental health diagnoses, as they often engage in risky behaviors that increase their chances of contracting HCV.
A literature review was conducted to identify quality improvement studies related to HCV screening. Overall, the studies indicated the need to screen high-risk individuals for HCV to reduce long-term disease progression. Moreno et al. (2017) emphasized the fact that, despite it being asymptomatic in the early stages, HCV can lead to serious liver complications such as cirrhosis and hepatocellular carcinoma. These authors determined that the most common and significant form of transmission is through IVDU, with an alarming 54% to 77% of new cases being intravenous drug users (Moreno et al., 2017).
In addition to screening individuals with IVDU, those born between the years of 1945 to 1965 should also be screened. Nili et al. (2018) noted that approximately 75% of HCV infections and 75% of HCV deaths in the United States are among baby boomers. Those infected with human immunodeficiency virus (HIV) are also at risk for HCV. Mocroft et al. (2019) stated that 2.3 million of the 36.7 million individuals with HIV are coinfected with HCV. Another high-risk population are individuals on hemodialysis (Nguyen et al., 2019). In addition, Schreiner et al. (2019) determined that individuals who have either consecutively elevated liver enzymes or patterns of abnormality in these tests also should be screened for HCV.
Initially, HCV screening strategies were based on identifying potentially stigmatizing risk factors such as a history of IVDU or unprotected sex with multiple partners. However, Dan and Kaplowitz (2019) expanded screening recommendations to include those who have received blood, blood products, or an organ transplant prior to July 1992, as well as individuals who received blood from a donor who later tested HCV positive. They also recommend screening for health care, emergency medical, and public safety workers who have been exposed to HCV-positive blood.
Rationale
Thomson et al. (2016) found that, despite being aware of current screening recommendations, few providers routinely screen patients in practice or feel comfortable treating HCV. Clearly, interventions are necessary to overcome screening barriers and maximize infected individuals’ access to treatment options.
The cited studies have shown the importance of screening for HCV in a variety of settings. In one study, Younossi et al. (2016) estimated that only 20% of HCV patients were identified and less than 10% of that 20% were treated. To improve these numbers and successfully treat and care for patients infected with HCV, it is important to screen appropriately for HCV as well as link individuals with HCV to suitable care providers. Testing, recognition, and referral for appropriate treatment are highly encouraged given the 300% increase in HCV cases from 2010 and 2015 (Cos et al., 2019).
Promoting provider HCV engagement requires a cost-effective, timely, and easy-to-implement education strategy (Buller-Taylor et al., 2018). Therefore, Buller-Taylor et al. (2018) developed a 1-h online course with a pre/posttest to measure knowledge gains. Shek and Zhu (2018) stated that “developers in education research may also use the pre/posttest design to determine the effectiveness of an education intervention program” (p. 2).
Furthermore, Trinh and Turner (2018) assessed HCV screening rates by reviewing charts of patients’ annual or new visits over a 3-year period. Their results indicated that the study intervention (a provider knowledge survey, screening education for providers, an electronic health record [EHR] screening tool, automated EHR prompts, and an audit of provider screening rates) significantly increased screening rates from 24% to 90% (Trinh & Turner, 2018).
Jones et al. (2019) indicated that electronic screening tools can increase HCV screening, referrals, and treatment, allowing physicians to identify asymptomatic patients and reduce overall HCV morbidity and deaths. Overall, the reviewed studies indicated the importance of screening at-risk individuals for HCV.
Specific Aims
The specific aims of this quality improvement project were to determine whether an intervention—consisting of a pretest, educational session, posttest, and implementation of a screening checklist—increased staff knowledge about HCV screening recommendations, identified at-risk individuals, and increased the number of patients screened and referred for treatment.
Methods
Context
This quality improvement project was performed on a 15-bed inpatient psychiatric unit in a Midwest regional medical center in Northeastern Michigan. To accommodate social distancing recommendations due to the coronavirus pandemic, a virtual online educational module was conducted among 30 staff members which included one first-year nurse practitioner, four psychiatrists with more than 20 years of experience, five social workers ranging from 2 to 9 years of experience, and 20 registered nurses with a variable experience range of 1 to 18 years of experience. Chart review was based on adults (age 18 years and older) who were admitted to the inpatient psychiatric unit. Inclusion criteria consisted of those charts which indicated patients were born between 1945 and 1965, had a blood transfusion or organ transplant before 1992, were currently using (or had previously used) intravenous drugs, were on long-term hemodialysis, experienced persistently abnormal alanine aminotransferase (ALT) levels, had received clotting factor concentrates produced before 1987, had an HIV diagnosis, or had been exposed to HCV-positive blood (i.e., via needle sticks, sharps, or mucosal exposure) while working in the health care, emergency medicine, or public safety fields. Patients with existing HCV positive and/or neurocognitive impairment diagnoses were excluded from chart reviews along with those that had no other identified risk factors, or were below the age of 18.
Intervention
The educational module, which was developed by the project directors, consisted of a modified, condensed version of the publication, A guide to comprehensive hepatitis C counseling and testing (CDC, n.d.). The module included screening recommendations, high-risk populations, and an HCV flowchart for ordering appropriate lab work. This project employed two assessments. First, a knowledge test (Figure 1; developed by the project directors based on information provided from A guide to comprehensive hepatitis C counseling and testing) was used to evaluate staff understanding of HCV screening benefits before and after the educational session. Pre/posttest scores were compared with evaluate whether a change occurred in staff knowledge following the educational intervention. Staff were receptive to the educational session.
Hepatitis C Virus (HCV)—Pre/Post Survey.
Second, a checklist was created based on CDC screening guidelines. This checklist used to identify patients at high risk for HCV—was incorporated into the EHR system to be used on all patients admitted to the unit for a period of 3 months. Staff were unable to bypass the screening checklist, unless patients were neurocognitively impaired at the time of admission. When high-risk factors were identified according to the CDC criterion, the checklist requested patient permission to perform HCV screening. After receiving verbal patient screening approval, the providers ordered an anti-HCV blood level test to determine the possibility of disease at which time a referral would be made to their primary care physician. EHR data about HCV screening were collected for the 3 months before and the 3 months following the educational session.
Measures
Data were collected using a self-created data extraction tool, developed by the project directors, which included patient gender, race, identified HCV risk factors, whether antibody labs were ordered and came back positive, and whether follow-up to the patients’ PCP was established. This tool covered all parts of the subjects it aimed to measure, addressing content validity. Furthermore, face validity was addressed as it showed a good representation of what the project directors were trying to gather.
Data were collected from the pre/posttest administered to staff members, including job description, gender, race, and academic background. The pre/posttest consisted of 11 questions to determine overall staff knowledge of HCV screening.
EHR data were collected from all admissions, totaling 77 charts in the 3 months prior to the intervention and from 127 admission charts in the 3 months after the intervention. These data were used to determine the number of patients identified as at risk based on inclusion criteria, screened for HCV, and referred for treatment, both pre- and post-intervention.
Analysis
Scores from 30 staff members’ pre- and posttests were analyzed. The mean pretest scores were compared to the mean posttest scores using an unpaired t test to determine whether there was an improvement in staff understanding of the need to screen high-risk individuals for HCV. EHR data were then accessed to determine whether or not an HCV screen was completed on a high-risk patient. A chi-square analysis was used to determine whether there was a statistically significant change in the number of high-risk patients identified and screened for HCV before and after the educational intervention.
Ethical Considerations
The Program for Education and Evaluation in Responsible Research and Scholarship (PEERRS) training, a requirement for all students through the University of Michigan-Flint was completed prior to the study. After review for human subject considerations through the institutional review board (IRB), this project was classified as exempt (#1574138-1) by the site where it took place and was not regulated (ID HUM00177845) by the University.
Results
Following the virtual educational session, there was a statistically significant increase in staff mean knowledge scores. The prescore mean was 55.15 ± 19.09 and the postscore mean was 85.75 ± 13.44, p < .001. The results represent a 30.6 percentage point increase in staff knowledge of HCV screening guidelines.
The analysis determined that during the pre-intervention phase, 72 out of the 77 individuals would have been appropriate for HCV antibodies screening using the HCV questionnaire. Four charts indicated that the patient was cognitively impaired, and one chart showed the patient was HCV positive; therefore, these charts would have been excluded. Of the 72 charts that would have met HCV screening criteria, only four patients were actually screened for HCV (Figure 2) (three males and one female) based on one with previous hemodialysis treatment, one with past IVDU, and two with elevated ALT/AST levels. Of these four patients screened for HCV (Figure 2), due to negative HCV antibody labs, none were referred to their PCP.
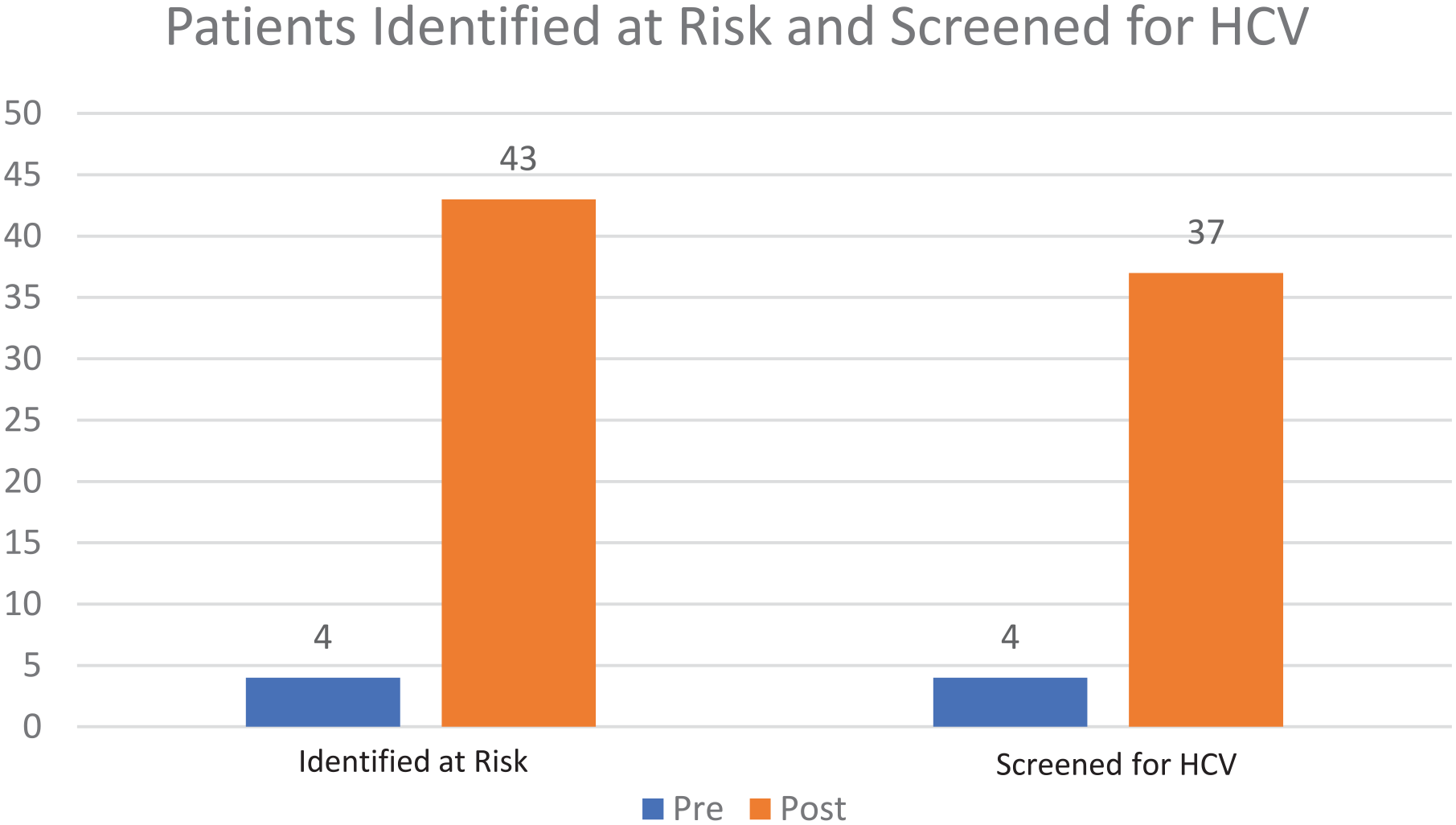
Hepatitis C Virus (HCV)—Bar Graph, Patients Screened, and Identified at Risk.
During the post-intervention period, 118 out of 127 patients received HCV screening through the risk assessment questionnaire. Of the nine patients who were not screened, three charts indicated the patient already had an HCV diagnosis and therefore did not qualify for the HCV questionnaire. Furthermore, six patients were not asked the CDC recommended questions by the staff due to neurocognitive impairment or psychosis at time of admission. Of the remaining 118 patients eligible to be screened for HCV, 43 met the HCV screening criteria (49% male and 51% female) and were considered to be high risk for HCV. Among patients identified as high risk, the most commonly reported criteria were being born between 1945 and 1965 (60%), past or current IVDU (26%), history of receiving blood products prior to 1992 (7%), and multiple criteria (7%). Of the 43 individuals identified as high risk, 37 consented to HCV antibody screening and six refused it (Figure 2). No individuals who completed the HCV antibody testing had positive antibody results. Therefore, none of the patients required a PCP referral for further treatment. Chi-square analysis indicated that there was a statistically significant increase in the proportion of patients who were identified as high risk from the pre (5.6%) to the post (36.4%, p < .001) periods, as well as those who received HCV antibody screening from the pre (5.6%) to the post (31.4%, p < .001) periods.
Discussion
Interpretation
The results of this quality improvement project identified an increase in staff HCV screening knowledge after completion of an online educational session. Overall, the results indicated that there was an increase in screening for HCV risk factors from four of 72 patients’ pre-intervention to 118 of 127 patients’ post-intervention. This ultimately led to 43 patients being identified as high risk, with 37 of those patients agreeing to HCV antibody screening post-intervention. Likely due to the small sample size, there were no positive HCV tests requiring referral to PCP for treatment options.
As early detection is the key to reducing HCV morbidity and mortality, the aim of this project was to increase staff knowledge of HCV screening recommendations, identification of individuals at risk for having HCV, and the number of patients screened and referred for treatment to their PCP. Using an online educational module for staff members that included a pre- and posttests, the current project’s results demonstrated an increase in staff HCV screening knowledge similar to those of the studies completed by Buller-Taylor et al. (2018), and Shek and Zhu (2018).
The HCV screening checklist (prompting staff to screen high-risk patients) implemented in the EHR for the current project was supported by Jones et al. (2019). It was determined that one of the most effective screening techniques for HCV was incorporating it into the EHR for staff to be prompted to assess for HCV criteria at the time of admission.
Prior to adding the screening checklist to the health system’s EHR, permission to do so was obtained from additional subsidiary hospitals within the same health system. At the conclusion of this project, the findings were presented to the hospital leadership team for a new policy proposal and implementation. The authors agreed to share the educational session and screening checklist with the other MidMichigan subsidiary hospitals for the purposes of a quality improvement project replication. A major strength of the quality improvement project was that a protocol was presented to continue screening those at risk for HCV upon admission. Another strength of this project was there was minimal cost involved as authors were able to create an online learning module and therefore did not need a space to deliver the educational session to the staff.
Limitations
This project had several limitations. First, the recent coronavirus pandemic led to a decreased sample size due to low unit census. Next, because the educational session could not be conducted face-to-face, participants could not ask questions about the content. However, an online educational module was created for the staff and questions were encouraged via email. Of note, due to pandemic-related lay-offs, this created time constraints when obtaining pre/posttests results.
While not pandemic-related, study validity may have been limited by patients being unwilling to admit to IVDU. Another limitation for this quality improvement project was not being able to have everyone in the same room, completing the educational session at the same time. This created difficulties for the authors as they needed to remind staff frequently to complete the pre/posttest and educational module.
Conclusion
Despite providing care for many individuals who may be at high risk for HCV, many staff and providers in mental health facilities do not complete routine HCV screening. HCV can be treatable and transmission risks can be reduced by identifying the virus early (AASLD, 2019). Without routine screening, the number of HCV patients will continue to increase substantially. As staff and health care providers, it is important to identify and provide screening to individuals at risk for this disease. The project’s educational session increased unit staff’s knowledge of HCV guidelines and increased the number of high-risk patients identified and screened for HCV. By incorporating a policy regarding HCV screening, the quality improvement project will maintain sustainability. Further studies with larger sample sizes are needed to confirm and extend these findings, although the authors are confident that this quality improvement project would produce similar results if replicated in a similar setting.
Footnotes
Acknowledgements
The authors would like to thank the staff for their participation and support at the hospital where the data were collected and Jenny LaChance, statistician.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.