
Abstract

We have all likely experienced the shame, pain, and sting of being stigmatized at some point. Stigmatization appears in diverse forms—including derogatory comments about skin tone, hair texture, or body size; denial of resources due to social standing; and devaluation of persons because of sexual/gender identity, religious affiliation, or political preferences. Regardless of its form, stigmatization is never productive and poses a considerable threat to mental health and well-being.
In the Greek language, stigma alludes to the markings placed on an individual as a symbol of shame, chastisement, or humiliation (Economou et al., 2020). My earliest memory of stigmatization was at the tender age of 7, when a transfer student in my elementary school decided to bully me with constant taunts of “blackie.” Of course, once my teacher got wind of this, he was severely reprimanded and that put an end to any further problem. However, I still remember the sting of the ostensibly innocuous word, “blackie.” For the first time, I was introduced to the concept that my skin tone might be considered objectionable. This is the sting of stigma—to make something common appear undesirable. I imagine that at some time, each of you has felt the same sting in some form. As psychiatric-mental health (PMH) nurses, we are obligated to safeguard against stigmatization in any form, among the diverse individuals, families, and communities to whom we provide mental health care.
As the last column in this series on I.D.E.A.S., the focus is to describe types of stigmas, illustrate consequences of stigma in relation to mental health care, and discuss de-stigmatization approaches. It bears repeating from the first column of the series that stigma is like an “ink spot on a shirt” (Okoli, 2022). Ink is common and so is a white shirt; yet, communicating that ink on a shirt is undesirable stigmatizes the ink spot. The process of mental health stigmatization compromises inclusivity, limits diversity, fosters inequalities and inequities, and hinders health care access through typecasting (i.e., stereotypes), preconceived ideation (i.e., prejudices), and discriminatory behaviors (Fox et al., 2018; Okoli, 2023b, 2023c) (Figure 1). This stigmatization process can be conceived through three lenses—self (including stigma by association), public/social, and structural/institutional.
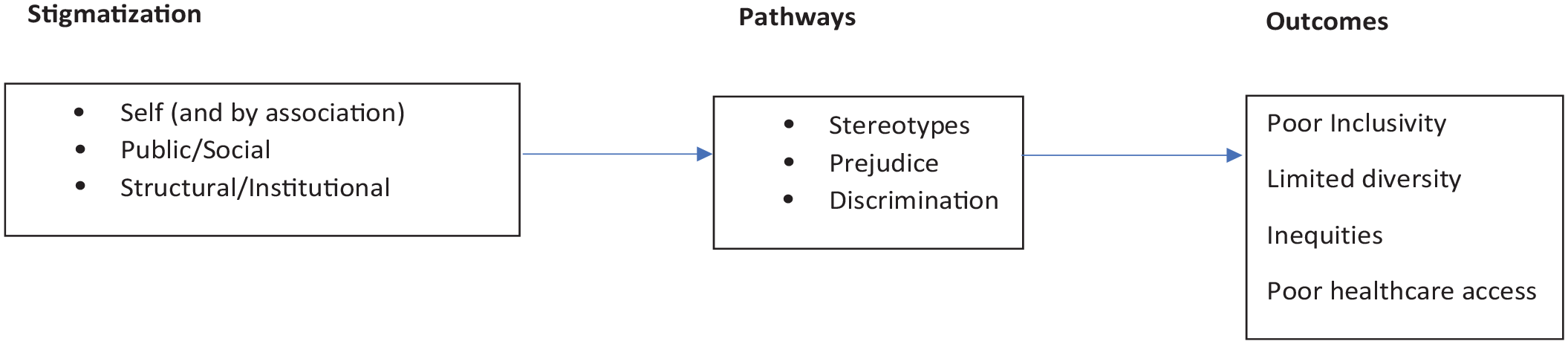
Conceptual Model of the Relationship Between Stigma, Inclusivity, Diversity, Equity, and Access
In the context of mental health, the first aspect of stigma, self-stigma, occurs when individuals living with mental health challenges internalize negative stereotypes related to their condition (Corrigan & Rao, 2012). When experienced by family members or close contacts, it becomes “stigma by association” (Thornicroft et al., 2022). These internalized negative stereotypes can lead to self-discrimination which undermines health care utilization, increases isolation, and results in poor self-esteem and quality of life (Corrigan & Rao, 2012; Corrigan & Watson, 2002a). The findings from a recent review suggest that nearly a third of individuals with serious mental illnesses have high rates of self-stigma, and these rates vary by geographic regions, cultural beliefs and practices, and degree of insight into an illness (Dubreucq et al., 2021). Conversely, stigma-resistance, self-efficacy, self-agency, and self-empowerment are protective factors against self-stigma (Dubreucq et al., 2021).
The second aspect of stigma, public (or social) stigma, is the general population’s response toward people with mental health challenges (Corrigan & Watson, 2002b). Perceived public stigma is the consciousness of negative characterizations (i.e., stereotypes) that are held against people with mental health challenges (Corrigan & Watson, 2002b). Perceived public stigma can increase the anticipation of encountering stigma from health care providers, and, thus, hinder treatment seeking among those for whom we care (Fox et al., 2018; Pattyn et al., 2014; Yu et al., 2021). On a positive note, findings from a recent longitudinal survey spanning 22 years (1996–2018) suggest an overall decrease in public stigma toward depressive disorders among U.S. adults; however, stigma toward people living with schizophrenia and substance use disorders persist (Pescosolido et al., 2021).
The third facet of stigma, structural (or institutional) stigmatization, results from practices or policies that disadvantage people with mental health challenges (Thornicroft et al., 2022). Structural stigma mainly reflects cultural standards, social circumstances, or formalized practices and policies (organizational and/or political) that disenfranchise those who are stigmatized (Hatzenbuehler & Link, 2014). For those with mental health challenges, structural stigma includes unfair hiring practices which limit employment opportunities, “diagnostic overshadowing” which compromises adequate care, and the underfunding, fragmentation, and poor re-imbursement for mental health care that impairs access to providers and needed treatments (Atkins et al., 2020; Brouwers, 2020; Charette-Dussault & Corbière, 2019; Hampson et al., 2020; Livingston, 2020; Okoli, 2023a).
Given the prevailing stigmatization of mental health, de-stigmatization efforts are a crucial part of our work in PMH education, practice, research, administration, and policy. Our de-stigmatization efforts should focus on mental health literacy, early detection of mental health challenges, and supporting recovery. As such, our work entails:
Promoting mental health literacy: One in five people in the United States has a current or prior experience with a mental health challenge (Substance Abuse and Mental Health Services Administration, 2022). Our key message is that although genetic vulnerabilities to mental disorders exist, these conditions are largely environmentally and socially determined. They cut across cultural, ethno-racial, socioeconomic, and religious groupings and impact a diverse range of individuals, families, and communities. Connecting individuals to peer-led programs can reduce self-stigma and empower them in their recovery journey (Dubreucq et al., 2021). As an example, the Honest, Open, and Proud (HOP) program, which empowers individuals in disclosing mental illnesses, shows promise in decreasing self-stigma and stigma stress among diverse populations with lived experience (Rüsch & Kösters, 2021). Moreover, leveraging media to provide positive messages about understanding mental illness and seeking treatment (e.g., A beautiful mind [2001] and Star Trek: Discovery—season four [November 18, 2021–March 17, 2022]), storytelling, and using educational vignettes are important strategies to improve awareness and reduce public stigma (Fong & Mak, 2022; Zhuang & Guidry, 2022). Finally, it is critical to directly address mental health challenges within workplaces to promote literacy, support care-seeking, and reduce stigma (Moll et al., 2018).
Normalizing mental health screening: Just as physical health screenings are crucial to anticipating health challenges, frequent mental health screening supports whole health and well-being. For those with an existing mental health challenge, our key message is that you are not alone—your challenges are real, can be understood, and are treatable (McGinty et al., 2015). For those without existing mental health challenges, our key message is that when detected, such challenges are treatable, and support exists for those who have such needs. We must make the case for “preventive psychiatry” to detect mental health challenges early and educate the public about maintaining well-being (Fusar-Poli et al., 2021). In this vein, programs such as Mental Health First Aid, Question Persuade Refer (QPR), and Psychological First Aid may be important avenues to reduce public stigma while supporting mental health seeking when needed (Hangartner et al., 2019; Morgan et al., 2018; Wang et al., 2021). Implementing such programs within workplaces can increase behavioral intentions toward helping colleagues and reduce mental health stigma (Reavley et al., 2021).
Supporting mental health recovery: We should advocate for person-centered, healing-oriented, and recovery-focused mental health care. Our key message for the public is that there are several ways to be part of the solution of reducing stigma by supporting recovery initiatives for individuals, families, and communities. Strategies include working with local and national organizations such as the National Alliance for Mental Illness (NAMI), The Trevor Project, the Substance Use and Mental Health Services Administration to support mental health and recovery. Participating can include volunteer opportunities, donations, membership on boards, and so on. Do not forget to engage in your local APNA chapter to promote mental health care and address de-stigmatization!
In combating mental health stigma, we must continue our efforts at de-stigmatization of mental health challenges, treatment seeking, and services. It is crucial that our recovery-oriented interactions with individuals, families, and communities are supportive of self-efficacy and self-agency to alleviate the effects of potential internalized stigma. To combat public stigma, tailored strategies such as educational platforms (e.g., books, movies, flyers, public service announcements), interpersonal contact with people who have lived experience, and cultural adaptations to care may be pursued (Ahad et al., 2023; Corrigan et al., 2012; Gronholm et al., 2023; Mascayano et al., 2020). Finally, as PMH nurses, we must advocate for change within institutions, at various levels, through our education, research, and practice. Our advocacy can expose structurally stigmatizing processes affecting our patients, their families, and communities. By engaging in the work of de-stigmatization, we are change agents and our collective voice can influence the change that is needed. And through our concerted efforts, we help others see the bigger picture: Without ink spots we could never appreciate the intricate beauty of a nice tie-dye shirt!