
Abstract
Keywords
Introduction
Untenable levels of workplace violence, low mental-health resource use, and high job demands on nurses in general, and on psychiatric-mental health nurses (PMHNs) more specifically, can result in psychological and moral distress that increase risks of suicidal thoughts or intentions (Bambi et al., 2018; J. E. Davidson et al., 2020; Jansen et al., 2020; Leigh-Hunt et al., 2017; Pariona-Cabrera et al., 2020). Suicide is death caused by self-directed injurious behavior with the intent to die because of the behavior (U.S. Department of Health and Human Services, n.d.). In 2018, suicide was the tenth leading cause of death overall in the United States at a rate of 13/100,000 (Centers for Disease Control and Prevention [CDC], 2018). Post the COVID-19 pandemic, the issue of nurse suicide has received greater attention (Choflet et al., 2022; Jahan et al., 2021; Rahman & Plummer, 2020). Risk factors for nurse suicide include the knowledge and availability of life-ending means, undertreated depression, work-life stressors, tobacco use, and substance use (Alderson et al., 2015; Groves et al., 2023). Current estimates of suicide incidence among female nurses are 17.1 per 100,000 versus 8.6 per 100,000 in the general female population; the rate of suicide for male nurses is 39.8 contrasted to 28.2 in the male population (J. E. Davidson et al., 2019; Davis et al., 2021). With such high rates, nurses are particularly at risk and require concerted strategies to address the problem (Davis et al., 2021). However, there remains a gap in addressing nurse suicide among PMHNs.
Fortunately, several strategies to address suicide include self-care practices, education to build resilience, and proactive institutional screening with connections to mental health services (J. J. Davidson et al., 2018; J. E. Davidson et al., 2020; Heath & Woods, 2021; Rizzo, 2018). Of these strategies, educational interventions are highly effective and easily adopted (J. J. Davidson et al., 2018; Rizzo, 2018). Web-based suicide prevention training can increase knowledge (Kullberg et al., 2020; Lancaster et al., 2014; Peterson, 2020) and confidence (Bektas & Yardimci, 2018; Kerr et al., 2020) while decreasing suicidal thoughts and anxiety (Guille et al., 2015; Van Spijker et al., 2018). Yet few studies have examined such interventions among PMHNs.
As a guide for educational interventions, the Theory of Planned Behavior (TPB) contends that attitudes toward a behavior (i.e., the belief of whether it is good or bad), subjective norms toward the behavior (i.e., if the behavior is seen as normative), and perceived behavioral control (i.e., a person’s perception of their ability to carry out the behavior) each predict the intention to carry out the behavior (Ajzen, 1991). The TPB has been used to assess behavior change related to educational interventions with nurses on topics such as bedside rounding, organ donor promotion, and advocacy for intimate partner violence against women (Koştu & Toraman, 2022; Lin et al., 2014; Montgomery et al., 2016). Hence, the TPB can be a useful theory to guide educational interventions regarding nurse suicide prevention.
This pilot study aimed to evaluate the effectiveness of a web-based education module on changing knowledge, attitudes, subjective norms, perceived behavioral control, and help-seeking related to suicide prevention in PMHNs. The specific aims of this study were to examine:
Frequency of suicidal thoughts and use of support among psychiatric nurses, and
Following a suicide prevention education intervention, changes in (a) knowledge regarding suicide prevention, (b) attitudes, subjective norms, perceived behavioral control related to suicide prevention, and (c) intentions to engage in suicide preventive behavior.
Method
Design
This pilot study used a quasi-experimental one-group pretest-posttest design to examine changes in knowledge, attitudes, subjective norms, perceived behavioral control, and intentions to access suicide resources after engaging in a suicide prevention education module.
Sample
A convenience sample of 101 registered nurses from two hospital psychiatric units of an academic medical center and a 239-bed psychiatric hospital were invited to participate. Inclusion criteria were: (1) registered nurses, (2) at least a 3-month work tenure in the setting, and (3) full-time employees. We excluded nurses outside of the psychiatric setting and students.
Procedure
Approval was obtained from the hospital-affiliated University Institutional Review Board (IRB). Surveys were then sent to participants through the nursing staff listservs of the participating hospitals. The survey link included a cover letter outlining the study. After reading the cover letter, those choosing to participate clicked on a link and were directed to a Qualtrics survey comprising a pre-survey, web-based video, and post-survey. The pre-survey consisted of a 10-min questionnaire that evaluated knowledge of suicide risk and prevention, attitudes toward seeking help, subjective norms toward seeking help, perceived behavioral control toward seeking help, and intentions to seek help if needed. Then participants were directed to watch a 25-min web-based suicide risk and prevention educational module. Finally, after completing the module, participants completed a 10-min post-survey evaluating the same questions from the pre-survey. Participants who completed the pre-survey, web-based video, and post-survey could voluntarily “opt-in” for a chance to receive one of six $20 gift cards.
Intervention
The intervention was an investigator-developed 25-min web-based education module that presented content and topics identified in the Healer Education and Assessment and Referral (HEAR) program (J. J. Davidson, 2018). The content of the video included information to enhance understanding of current nurse suicide rates, nurse suicide risk factors, nurse burnout signs, methods of nurse suicide and recent trends, and available local and national resources for preventing nurse suicide and supporting nurses in mental health crises. The content of the educational module was reviewed by two certified suicide prevention trainers through the American Psychiatric Nursing Association (APNA) Competency Based Training for Suicide Prevention (CBTSP) and a PMHN practitioner trained in the Collaborative Assessment and Management of Suicidality and the APNA CBTSP (Jobes, 2012; Puntil et al., 2013).
Measures
Measures obtained from the electronic surveys included demographic information (age, sex, marital status, ethnicity/race, and education level), experiences of suicidal thoughts, and using psychiatric-mental health support services (e.g., “Have you ever experienced suicidal thoughts?” and “Have you accessed behavioral health support services because of suicidal thoughts?”), knowledge about suicide risk factors and prevention (five true/false questions assessing specific content provided through the web-based educational module), attitudes, subjective norms, perceived behavioral control, and intentions to access suicide prevention resources (a 15-item investigator-developed scale using guidelines by the developers of the TPB, Ajzen, 2011). The TPB questions were each based on a Likert-type scale of 1 (strongly disagree) to 7 (strongly agree). The reliability of the TPB items and scales has been supported in the literature (Okoli et al., 2017, 2018). Cronbach’s alpha for the TPB scale dimensions used in this study were as follows: attitudes, .88; subjective norms, .73; perceived behavioral control, .79; and intentions, .94.
Data Analysis
Twenty-nine of 101 (29%) invited nurses completed the pre-test, web-based education module, and post-test. Descriptive statistics were used to summarize demographic variables, including means and standard deviations or frequency with percentages as appropriate. The experiences of suicidal thoughts and using support services were summarized with frequencies and percentages. Paired sample t-tests were used to examine changes in the scores on knowledge about suicide risk factors and prevention and attitudes, subjective norms, perceived behavioral control, and intentions to access suicide prevention resources before and after the intervention. All analyses were conducted using IBM SPSS, version 28.
Results
Sample Description
Of the 101 eligible participants, 29 responded (28.7% response rate). The sample was mostly female (75.9%), White, non-Hispanic (89.7%), held a Bachelor of Science in Nursing degree (89.7%), married or in a cohabitating relationship (62.1%), and had a mean age of 43 (SD = 11.4) years. Sixty-two percent of the respondents were from the Psychiatric Hospital.
Prevalence of Suicidal Thoughts and Use of Psychiatric-Mental Health Support
Of the 29 nurses surveyed, 12 (41.4%) reported that they had experienced suicidal thoughts, and three (10.3%) reported prior use of psychiatric-mental health support services.
Changes in Knowledge About Suicide Risk Factors and Prevention
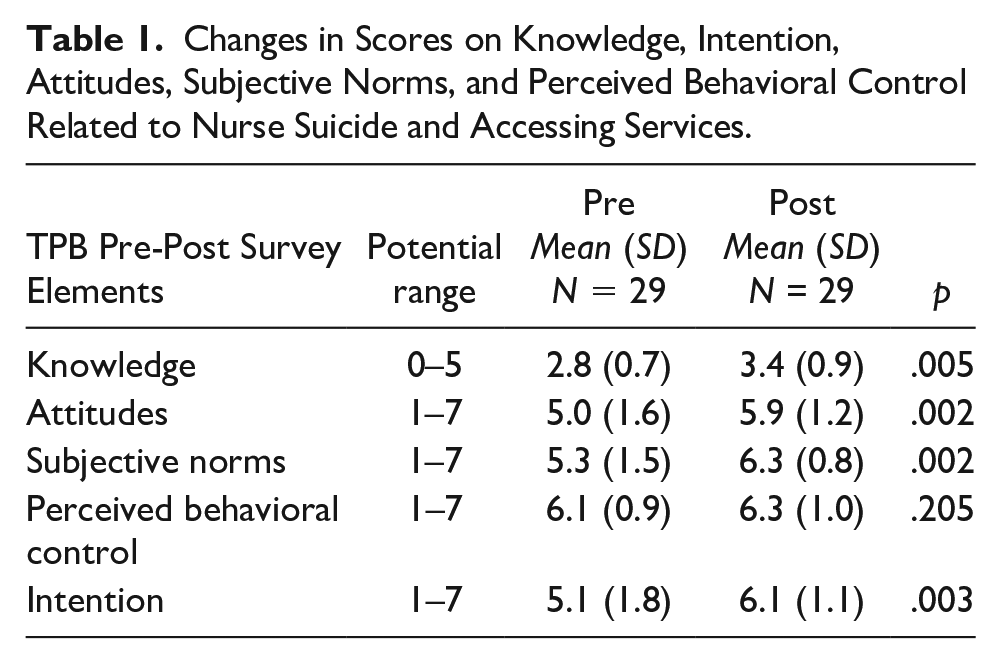
Participants’ knowledge related to nurse suicide and accessing available resources significantly (p = .005) improved after completing the web-based education module from a pre-test mean score of 2.8 (SD = 0.7) to a post-test score of 3.4 (SD = 0.9).
Changes in Attitudes, Subjective Norms, Perceived Behavioral Control, and Intentions to Access Suicide Prevention Resources
There were significant improvements in attitude scores (pre-test M = 5.0, SD = 1.6 to post-test M = 5.9, SD = 1.2; p = .002), subjective norms scores increased (pre-test M = 5.3, SD = 1.5 to post-test M = 6.3, SD = 0.8; p = .002), and intention scores (pre-test M = 5.1, SD = 1.8 to post-test M = 6.1, SD = 1.1; p = .003). However, changes in perceived behavioral control scores were not significant (pre-test M = 6.1, SD = 0.9 to post-test M = 6.3, SD = 1.0; p = .205; see Table 1).
Changes in Scores on Knowledge, Intention, Attitudes, Subjective Norms, and Perceived Behavioral Control Related to Nurse Suicide and Accessing Services.
Discussion
This study may represent the first to concentrate on nurse suicide within the PMHN subspecialty. Of note, more than 40% of the participants from this study reported having experienced suicidal thoughts. This rate is significantly higher than the 5.5% rate of suicidal ideations found in nurses in a recent study (Kelsey et al., 2021). However, we did not ask the duration of these suicidal thoughts (e.g., lifetime) or their frequency and severity (mild, moderate, or severe) in our study. Further qualitative analysis may be needed to better understand and guide efforts to ameliorate this elevated risk of suicide ideation in PMHNs.
Our findings using the TPB demonstrated improvements in attitudes, subjective norms, and intentions to access suicide prevention resources, but not behavioral control. This finding suggests that our web-based educational intervention may require some modification to also improve perceived behavioral control for PMHNs. Nevertheless, with appropriate modifications, such an intervention can also be targeted to nursing students to normalize mental health help-seeking attitudes, subjective norms, and intentions, particularly when experiencing suicidal ideations. Web-based interventions could be incorporated into the PMHN student curriculum to assess the risk of suicide and provide information about ways to seek help (Stubin, 2020). The TPB may continue to be used to guide such interventions to support help-seeking behavior.
Finally, our findings regarding the low rates of accessing mental health services relative to the high rates of suicidal thoughts suggest that organizations should support nurses’ access to proactive mental health services and help-seeking behaviors (Choflet et al., 2022). As nurses continue to experience high rates of depression, burnout, and suicidal ideation, organizational nurse leaders should advocate for and develop preventive system-level mental health initiatives that promote integration into a wellness culture (Melnyk et al., 2021).
Limitations
Some important limitations should be recognized when considering this study’s findings. The overall small sample size limits the generalizability of the results beyond the setting in which the study was completed. Also, the relatively low response rate may have introduced selection bias in the responses to our study. It is possible that individuals who perceived the content of the study as more salient to them were more likely to respond. Given the small sample size, a psychometric analysis could not be conducted to verify the reliability and validity of the specific instrument. However, other studies using TPB-based investigator-developed measures in mental health help-seeking behavior have been validated in the literature (Bohon et al., 2016; Logsdon et al., 2018). Finally, although we found a 40% prevalence of suicidal thoughts among our respondents, this rate may reflect a response bias. It is important to note that we did not assess actual suicide attempts, which may be a predictor of future suicides. Future studies may consider assessing previous suicide attempts.
Conclusion
Developing innovative programs that address nurse suicide is an essential aspect of evidence-based care and healthy clinical settings. Understanding the effectiveness of various modes of interventions can guide PMHN administrators in program development aimed at reducing suicide among nurses. Our web-based education intervention resulted in higher knowledge, attitudes, subjective norms, and intentions scores related to nurse suicide and access to mental health resources among nurses. Much is known about the benefits of training the nurse as a gatekeeper. However, there is a gap in the literature regarding the benefits of web-based training for the nurse as a consumer to complement a referral program. Thus, this pilot should be replicated to include nurses from various settings and specialties to evaluate the intervention on a broader scale and learn of differences in nurse subspecialties. Such research could provide valuable insights into the effectiveness of interventions to develop evidence-based and specialty-specific nurse suicide prevention strategies.
Footnotes
Acknowledgements
Marc Woods would like to thank the hospital administrations where the data were collected for their support.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript or critically revised the manuscript and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.