
Abstract
Background:
The shortage of inpatient psychiatric mental health care nurses in Saudi Arabia represents an important health care challenge.
Aim:
The aim of this study was to illuminate perspectives of psychiatric mental health nurses employed in psychiatric inpatient settings about their employment experiences.
Method:
This study adopted an exploratory qualitative approach using thematic content analysis. Ten professional nurses with psychiatric inpatient caring experience participated in two focus groups composed of Master of Nursing students.
Results:
Four main themes emerged: inadequate professional skills and knowledge for psychiatric mental health care practice, negative public attitudes toward psychiatric/mental health nurses, concerns for personal safety, and alternatives and advantages. The findings of this study suggest that nurses’ lack of interest in working in psychiatric units is not merely personal but also social and organizational.
Conclusions:
The study findings may encourage managers and authorities to develop measures to attract more mental health nurses to work in psychiatric units. Such strategies may include modification of nurses’ skills, training, and professional knowledge, collegial supervision, mentoring, and working conditions and environment.
Introduction and Background
The recruitment and retention crisis in nursing has been extensively documented in recent years, with scholars, including Chapman et al. (2018) and Rice et al. (2019), among others, suggesting that the nursing profession is facing critical shortages around the world. Other researchers argue that these problems are nothing new for the psychiatric mental health (PMH) nursing profession, which has experienced issues in this regard for many years (Gabrielsson et al., 2021; Slaughter & Hoefer, 2019). Kaas (2020) argues that to manage this anticipated shortage, the nursing profession must recruit and train nurses and successfully transition them into their chosen careers. The future success of the PMH nursing profession thus relies, to some extent, on newly graduated nurses.
At face value, the simple solution to this shortage of nurses would be to increase the number of nursing training opportunities. However, the problem runs deeper than allowing more students to undertake nursing degrees. Ackerson and Stiles (2018) claim that there is already such a high attrition rate in nursing that the number of newly graduated nurses is currently not meeting the potential shortfall. Scholars, including Mabala et al. (2019) and Naseer et al. (2021), have investigated the reasons why so many newly qualified nurses leave the profession, citing factors such as poor organizational support, an unreasonable workload, toxic work environments, including negative interprofessional relationships, difficulties transitioning into practice, and general job stressors.
The MH care system in Saudi Arabia employs 10.7 mental health (MH) nurses in Saudi Arabia in practice per 100,000 people, compared with 23.2 in Europe Union countries (Al-Subaie et al., 2020). Saudi Arabia, with a population of 33 million people, spends 4% of its total health care budget on MH care. The Saudi National MH Survey was conducted in conjunction with a large scale health survey between 2011 and 2016 and reported in 2020 (Al-Subaie, 2020). However, the MH data which were employed in the final report of this survey was based on data from the Global Burden of Disease (GBD) Initiative and other small studies previously reported. Based on this study drug use disorders, depressive disorders, and anxiety disorders numbered third, fourth, and sixth leading causes of disability in Saudi Arabia (Al-Subaie, 2020).
Spending for MH care is largely for inpatient care, accounting for 80% of funds expended (Al-Subaie, 2020). The Saudi National MH Survey found that 20% of the sample had required MH care in the 12 months before the survey (Al-Subaie et al., 2020). However, the stigma of MH disorders is very strong, resulting in large numbers of those suffering from mental disorders failing to seek care or voluntarily forgoing treatment (Alattar et al., 2021).
About half (50%) of primary care patients in Saudi Arabia considered nerves, stress, and religious factors as a cause of their physical symptoms, so the effect of mental and emotional factors on illness is recognized by the population (Alqahtani & Salmon, 2008). However, MH is not freely discussed, and at times even immediate family members are unaware that this type of care is being accessed by the client. Punishment by God is considered one source of disturbed MH. People attribute other types of conditions to supernatural forces, such as witchcraft and the evil eye (Halligan, 2006). Awareness of these attitudes is important because clients are not likely to freely request care for MH problems from their health care practitioner.
Alluhidan et al. (2020), Gong et al. (2022), and Stolzman (2021) suggest that contemporary nursing graduates face important personal adjustment problems as they transition to clinical practice. Alluhidan et al. (2020) noted that Saudi nurses face challenges in coordination of family responsibilities, adjustment to work in contrast to student lifestyle, and adjustment to the reality of the nursing practice environment. These concerns are accompanied by fear of the nurses from violence during their practice. Stigma attached to being involved in MH care coming from family members and peers within the health care professions (Alyousef et al., 2020; Alhamidi & Alyousef, 2023; Alyousef et al., 2020).
Review of Related Literature
Peng et al. (2020) advise that MH and psychiatric problems are among the critical health care challenges of today due to their high prevalence and disease burden. Wang et al. (2020) cite a World Health Organization (WHO, 2020) report stating that 450 million people worldwide suffer from psychiatric/MH problems, with depression as the most frequently identified problem. The WHO (2020) report indicates that people may suffer from MH or psychiatric issues at any stage of life, while Tsegay et al. (2020) and Zareifopoulos et al. (2018) highlight that patients with these have a higher mortality risk due to comorbidities, including cognitive impairments and physical conditions, refusal to accept treatment, and the biases of health care providers. Delivering quality health care relies on the availability of committed, competent health care professionals including nurses. Phoenix (2019) advises that nurses are the largest group of health care providers in inpatient psychiatric units and PMH hospitals. Giorgi et al. (2020) support this, indicating that workforce surveys show that nurses are the largest occupational group working in MH, PMH, and addiction services.
According to Evans et al. (2019), the principal aim of nursing care in inpatient PMH hospitals is to work with patients to facilitate their recovery, promote their return to everyday life, and prevent them from being re-hospitalized (Larsen et al., 2021). Despite the powerful impact, PMH nurses can have in the psychiatric inpatient setting, scholars, including Kaas (2020), believe that the number of nurses available to deliver care are inadequate.
Samari et al. (2019) discussed a WHO report stating that worldwide in 2014, for every 100,000 patients in psychiatric settings, there were only 7.7 nurses and fewer than one psychiatrist, highlighting the staggering shortage of PMH staff. It is therefore critical to consider the reasons behind the shortage of nursing staff in inpatient psychiatric settings. Phoenix (2019) claims that MH nurses only choose to work in PMH settings when other work is unavailable, while Evans et al. (2019) cite nurses’ negative attitudes toward working in psychiatric settings. Kobayashi et al. (2020) highlight emotional burnout and stress as having a negative impact, which Foster et al. (2021) also found, advising that this was experienced by more than 50% of nurses in psychiatric/MH settings. Fukui et al.’s (2021) and Foster et al.’s (2021) examinations of occupational stress among MH nurses identified factors that included fear, despair, and burnout, as well as dissatisfaction with the job, all of which can negatively impact the quality of care they can provide patients. This was particularly marked during the first 15 months that MH nurses worked in psychiatric settings, citing the influence of stressors that led to emotional burnout. Itzhaki et al. (2018) found that negative public attitudes also impacted nursing students’ reluctance to work in psychiatric settings. Rio et al. (2020) found that MH nurses’ lack of engagement in psychiatric settings was also affected by a lack of technical nursing practice. Therefore, considerable academic attention has been paid to the shortage of PMH nurses, as well as how this affects the quality of nursing care that these providers can offer (Fukui et al., 2021; Itzhaki et al., 2018).
Kramer (1975) identified the phenomenon of “reality shock” in nursing over 40 years ago. Ko and Kim (2022) observed that this phenomenon still affects new nursing graduates transitioning into professional practice. Hartung et al. (2020) suggest that Kramer’s (1975) influential opinions remain pivotal to the modern understanding of how graduate nurses transition to professional practice across all clinical areas, including MH.
Objective
Perceptions about nurse employment in inpatient PMH nursing and their satisfaction in that career as viewed by qualified Saudi nurses is sparse. By examining contextual features of the experience of providing inpatient psychiatric nursing care, ways and means of ameliorating stresses and surrounding ecological factors that mitigate nurses’ participation in this area of nursing practice may be identified (Matua & Van Der Wal, 2015).
Thus, the objective of this study was to explore the views of PMH nurses employed in the inpatient PMH setting and identify factors that may mediate choices to be employed in this sector of nursing care.
Theoretical Foundations
This study is committed to the philosophy of social cognitive theory that change is possible and that social interaction based on responses to change is an important operating factor (Bandura, 1989). Therefore, awareness of causative phenomena that may explain patterns of behavior is an essential ingredient for the construction of best practices (Strauss & Corbin, 1990).
Social cognitive theory, as explained by Bandura (1989), is very useful in understanding and viewing the behavior of participants, clients, and social groups. An awareness of the importance of personal and social interaction and the effect of normative values on participants provides a perspective for data and a structure for its interpretation (Butts & Rich, 2011). Thus, exploratory qualitative data may provide insights of practicing PMH nurses and may contribute to a fuller understanding of the challenges faced in the provision of care. Information of this nature is needed as a prerequisite to understanding the sources of rewards, strengths, weaknesses, and challenges experienced by nurses and may assist in structuring experiences and programs that would enrich the MH caring experience.
Method
Study Design
This study used an interpretive qualitative approach to obtain detailed descriptions of the topic being investigated based on Dyar’s (2022) suggestion that a naturalistic, interpretative method of investigation is especially appropriate for studies that explore human experiences. Phenomena such as experiences, attitudes, and behaviors can be difficult to accurately capture quantitatively, whereas a qualitative approach allows participants to explain how, why, or what they are thinking, feeling, and experiencing (Tenny et al., 2022). The qualitative method employed in this study facilitated an in-depth investigation of the experiences and perceptions of a group of experienced professional MH nurses related to their work experience in that field.
Sample and Setting
Participants were recruited by broadcast of invitation to all students of The Master of Nursing—King Saud University program via Whatsapp social media (Meta Platforms, inc., Menlo Park, California). Inclusion criteria was students who were graduates of a BSN (Bachelor of Nursing) program and had been employed for a minimum of 2 years in direct inpatient care in public psychiatric units. The Office for Health Improvement and Disparities (UK) have recommended six to eight persons as an appropriate size for focus groups (Gov, 2020). Table 1 displays characteristics of the focus groups.
Participant Characteristics.
Data Collection
According to Ivanova et al. (2022), the focus group method of data collection has advantages over one-to-one interviews in that it allows the researcher to gather views from more participants. This not only has advantages in terms of time, but also enables more discourse and information sharing among the participants. Nyumba et al. (2018) also suggest that focus groups enable useful interaction between the researcher and the participants and provide a scenario in which concepts, perspectives, emotions, and experiences can be discussed. Bagiu et al. (2020) further add that focus groups allow researchers to use their analytical skills to draw out information from participants through theoretical sampling as the group interview progresses.
The data were collected through semistructured interviews in focus groups. Based on the size of the sample, two focus groups of five members each were formed and met simultaneously in the nursing graduate faculty of King Saud University. Each group was led by a moderator who was known to the participants as an undergraduate instructor. Kinalski et al. (2017) note that focus groups are highly instrumental in permitting participants to discuss health care experiences. The investigators initiated the discussion of feelings and experiences encountered during the provision of care to patients in the inpatient psychiatric setting. The meetings were approximately 2 hours in length. Although the projected amount was 90 minutes, additional time was occupied with member checking. The proceedings were digitally recorded and transcribed to form a Microsoft Word document. Identifying information was not included in the transcripts. The recordings and transcribed narratives were stored in a locked facility.
Open-ended questions were aimed at encouraging participants to express their opinions and feelings related to their practice (Kinalski et al., 2017). The initial probes were structured with an interview guide designed to elicit feelings about the participants’ caring experiences (Gioia et al., 2013). The focus group interviews began with open-ended questions displayed on Table 2. As interviews proceeded, theoretical sampling based on inductive data produced by the initial inquiries enabled the interviewer to structure probes to gain a greater understanding of the participants’ perceptions (Hennink et al., 2019). This process assisted the participants in providing thick descriptions of their experiences and associated feelings.
Interview Probes.
Each statement made by the participants was considered significant and treated as relevant. Cessation of emergence of novel inductive data was considered achievement of saturation (Kinalski et al., 2017; Strauss & Corbin, 1990). Member checking after achievement of saturation was employed to confer increased trustworthiness.
Data Tabulation and Analysis
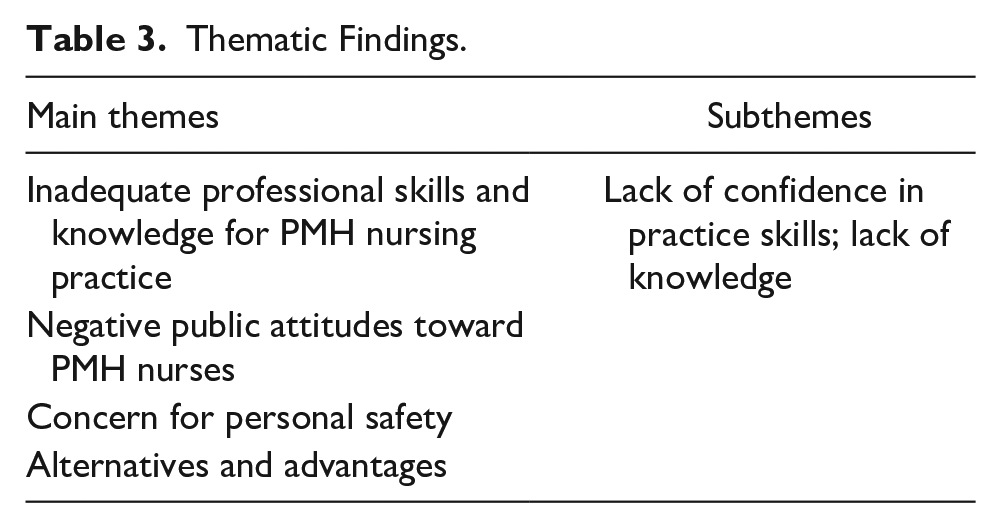
Based on Vignato et al. (2022) recommendations, the preliminary inductive data were processed via NVivo software, Lumivero.com, (2023) which assisted in identifying themes. As the thematic analysis progressed, the researchers identified emerging themes which are displayed on Table 3. The researchers identified additional subthemes and conversational threads in collaboration with an experienced peer researcher. Care was exercised to put their own views aside to avoid bias.
Thematic Findings.
Ethical Considerations
The research and interview process commenced after the ethics committee of the sponsoring University which approved procedures.
After being informed of the purpose of the research written and verbal informed consent were obtained from participants, including permission for digital recording of the interviews. The participants were assured that their contributions would be confidential and that they could withdraw from the study at any time. Participants were not paid nor received any tangible reward.
Rigor
Two researchers who had acted as moderators during data collection independently reviewed the data, codes, and themes. The depth which emerged during theoretical sampling of the experiences described by the participants directly impacted their dependability and potential for transferability. The data, codes, and classifications were also evaluated by two peer researchers to examine the sense, precision, and significance of the emergent data. Credibility was enhanced by the professional qualification and experience of participants, coupled with member checking for mutual understanding of the phenomena explored.
Findings
Participant reasons for low interest levels in employment in inpatient PMH units formed four main themes that were grouped into categories: inadequate professional skills and knowledge for PMH nursing practice, negative public attitudes toward PMH nurses, concerns for personal safety, and alternatives and advantages.
Theme One: Inadequate Professional Skills and Knowledge for Psychiatric Care Practice
Although participants had been employed in inpatient psychiatric settings, they were not confident of their skill sets and theoretical base. They perceived that there was discord between what they learned in their undergraduate curriculum concerning PMH care and the reality of caring for patients in the inpatient setting.
Subtheme 1: Lack of Confidence in Practice Skills
Most participants advised that their inadequate clinical skills in these settings were one of the main reasons that they were reluctant to join or continue with inpatient psychiatric nursing care. Nurse 6 noted, “I had chosen to work in a psychiatric/MH unit without having the right skills and knowledge. I was not sufficiently prepared for the reality of working in this setting.” This viewpoint was further expressed by Nurse 3, who said, “I don’t believe I have the right skills and nursing competencies to work in this setting.”
All the participants believed that working in PMH units was more complex than working in other hospital wards, citing the lack of enjoyment they found in this work due to their limited readiness for this type of care and compounded by their perceptions of insignificant patient recovery. Nurse 10 stated, “My lack of familiarity with working in PMH units causes me to be uncomfortable in my job [. . .] I do not enjoy this kind of work!” Nurse 8 agreed, basing her dissatisfaction on the lack of progress with patient outcomes.
Most participants felt that special competencies required for psychiatric care were not part of their skill set: “Working in psychiatric institutions is tougher than working in other clinical settings like medical or surgical wards” (Nurse 1).
Subtheme 2: Lack of Knowledge
The participants suggested that nurses who work in psychiatric wards require greater professional preparation and knowledge than nurses in other hospital settings. They cited the deficiencies in curricular content in MH, which adversely affected their abilities to function in practice.
Nurse 4 expressed the view that the theoretical content encountered during undergraduate training was incongruent with skills used during practice: “There is a wide gap between theory and practice in PMH units.” This perceived gap led participants to feel that they had not been properly prepared for psychiatric practice: “Most of us are unfamiliar with patients with MH problems” (Nurse 1). This situation left them feeling that they were not accomplishing constructive care. “Because I’m not familiar with these patients and their symptoms, I feel that I can’t do anything to help them and am not qualified to deliver the interventions they require to improve their situation” (Nurse 7).
Several other participants noted that the skills required in the inpatient unit varied little, limiting motivation to stay up to date in their skill levels: “The limited spectrum of cases we had on the unit meant that my interest in work dwindled. I felt that I had lost my nursing competency and fallen behind colleagues working on other hospital wards” (Nurse 6). Nurses 5 and 6 had a similar view.
A number of the MH nurses felt particularly stressed when patients exhibited symptoms with which they had not become familiar with during training and did not feel able to address. “I found it very stressful when faced with patients who suffered hallucinations and panic attacks because I was unfamiliar with how to address these conditions” (Nurses 9). Nurse 5 voiced the same concern.
Theme 2: Negative Public Attitudes Toward PMH Nurses
Negative public attitudes toward PMH nurses were another reason why the participants were not interested in working in PMH units. Most participants in the focus group argued that there were misconceptions and negative views about working in PMH hospitals units, not just among the public, but also among their own families (Nurses 2, 3, 6, 9, and 10). Some nurses noted that they are reluctant to mention that they work in an MH setting: “Despite my many years of experience working in PMH units, I still feel that I have to hide the name of my workplace from others because of the stigma associated with it” (Nurse 8). This was echoed by nurses 3 and 10.
Family members and colleagues attach a negative identity to PMH care, based on the belief that they are likely to be exposed to danger during employment: “Members of my family and many colleagues have a negative attitude toward PMH nursing. They fear that I will become mentally ill myself. I have encountered this attitude even among colleagues who have experience working in this type of setting” (Nurse 3). “Our families asked us not to work in MH and strongly advised me not to choose to work in an inpatient psychiatric MH setting when I started working” (Nurse 4).
Theme 3: Concern for Personal Safety
Participants expressed their dissatisfaction with psychiatric inpatient unit employment based on unsatisfactory relations with patients, whom they viewed as posing threats to their physical well-being: “My experience working in psychiatric units has been challenging, and I have had incidents where patients tried to harm me” (Nurse 9). This was also expressed by nurses 4 and 7. Physical violence was seen as a real threat, creating what the nurses considered a dangerous environment: “Nursing staff can be threatened and hurt by patients with MH problems when they become aggressive or irritable. This lack of safety puts me off working in MH units” (Nurse 10). Almost all the group members agreed: “When I was on duty in a MH unit, the nurses’ main concerns were protecting themselves from violence, such as harm by patients with delusions, hallucinations, or general irritability. It is a very stressful environment.”
Considering the shortage of professional psychiatric/MH nurses available and willing to accept assignment to inpatient psychiatric units, concerns expressed by the participants suggest that changes in professional preparation and ongoing support for nurses assuming this caring role may be predicated by an examination of the problem and introduction of innovative changes in unit practices.
Theme 4: Alternatives and Advantages
Discussing their experiences of working in psychiatric/MH units, most participants advised that they were attracted to work in such settings for various reasons, such as being recruited immediately after graduation without exploring other opportunities. For example, “The psychiatric department recruited us at an early stage” (Nurses 10 and 3). Other participants voiced their presence on the MH units as being a stop-gap measure until better work opportunities are available. Nurses 4 and 9 concurred that they felt they would always find a posting in the MH units: “There is always a shortage of nursing staff in psychiatric/MH units, so I will always get work there when I don’t have other options.”
Female nurses cited the demands of integrating their family duties with employment responsibilities via working hours and liberal leave: “Working in inpatient PMH units has certain advantages, such as fewer working hours. Because we have children, we cannot work nights, so this is a good option for me at this stage” (Nurses 2 and 5). “We get weekends off, which works well for me” (Nurse 9). “I have children and cannot work late at night. The psychiatric department gives me the flexibility to work during the day” (Nurse 10).
Additional employment benefits were cited by one participant as a reason for assignment in that unit. “PMH units often offer better money and more leave than other wards or hospitals” (Nurse 7).
Discussion
Studies concerning factors that may influence student or practicing nurses’ satisfaction with PMH as a career choice are limited (Çingöl et al., 2020; Hunter et al., 2015). The present inquiry found that nurses’ lack of interest in working within PMH settings was attributed by the participants to having inadequate professional skills for psychiatric care practice, negative public attitudes toward PMH nurses, concerns over personal safety, and availability of other alternatives and advantages which mediated the choice to practice in the inpatient PMH setting.
Selmon et al. (2020) found that student participation in undergraduate MH practicums constituted an important source of their decisions not to pursue a career in that area of nursing. Alhamidi and Alyousef (2023) found that undergraduate students in Saudi Arabia identified anxiety and stress related to contacting patients, stigmatization of MH care as a practice, and shortcomings in academic preparation as important factors in consideration of MH or PMH practice as a career choice.
This study’s findings align with those of Worringer et al. (2020) who found that staff shortages meant that PMH nurses often were expected by employers to begin their practice without receiving appropriate ward orientation. Labrague and McEnroe-Petitte (2018) found that many PMH nurses quit nursing in the first year after graduation due to the heavy workload and a poorly defined career structure, and Singh et al. (2020) highlighted the lack of experienced nurses for newly placed PMH nurses to model, possibly contributing to Rodrigues et al. (2021) who found that PMH nurses felt they lacked the specific knowledge and skills to be successful MH nurses. Adams et al.’s (2021) research found that nursing students’ and practicing nurses’ motivation at work was negatively affected by the feeling that they had insufficient education and knowledge.
Yılmaz’s (2017) study suggests that positive attitudes toward psychiatric nursing can be engendered by improving nursing students’ theoretical and practical knowledge. In keeping with Evans et al.’s (2019) opinion, it therefore follows that nurses’ interest in working within the PMH setting may be enhanced by providing them with educational content and experience which may give them feelings of increased confidence and competency. Mentoring may be instrumental in guiding the practitioner to avenues for acquisition of specialized skills and practice since the mentor has been down this track ahead of them. The use of experienced nurses to supervise and support novice nurses has been found to garner increased interest in working in psychiatric settings (Perkins et al., 2023).
Interestingly, Hwang et al. (2018) found that when PMH nurses developed closer professional relationships with patients, it led them to have a more positive attitude toward working in psychiatric wards. Formation of therapeutic alliances between nurses and their patients has been found to have a positive impact on treatment outcomes. Bordin (1979) was an early commentator on this aspect of PMH care, noting that commonality of goals and tasks as the basis of an alliance between patients and their health care providers augured for a more positive outcome.
Several scholars, including Palou et al. (2019), have identified the impact of stigma, advising that negative attitudes toward PMH nurses lead to nurses’ lack of interest in pursuing a career in the psychiatric setting. In this study, the participants advised that negative perceptions of PMH nurses among their families, colleagues, and the wider community, as well as their experiences of working in psychiatric care settings, influenced their lack of interest in pursuing a career in the sector. This is supported by Sari and Yuliastuti (2018) and Balingit (2019), who also reported that negative attitudes toward psychiatric nurses negatively affected their morale and interest in working in psychiatric settings. Rodrigues et al. (2021) also found that the social stigma associated with MH meant that psychiatric nurses could not share details of their career with their friends, families, and community about their workplace and career mirroring Saudi nurses’ comments.
Morgan et al. (2021) found that false perceptions and beliefs about mental disorders created the feeling that people believe that psychiatric patients are dangerous and unpredictable. These data are like those sentiments of participants in this study stated they encountered in their practice. Ring and Lawn (2019) point out that these misconceptions negatively affect the quality of PMH care, as well as the image of the profession as a career prospect. Moreover, Morgan et al. (2021) report that nurses’ previous experiences working in psychiatric settings mean that they retain anger toward patients or believe that these patients are not deserving of care and support.
Çingöl et al. (2020) believe that this might cause PMH nurses to become overly preoccupied with their work and develop negative feelings toward it, while Liu (2021) suggests that such negative feelings about work are not seen to the same extent in nurses who work in nonpsychiatric settings. Participants in this study also shared their fear of being harmed by patients, especially if they were unfamiliar with PMH units, advising that this was an important factor that affected their interest in working in PMH environments. This fear and anxiety led them to prefer working in different health care environments.
Singh et al.’s (2020) Iranian study found that stress over unexpected events and the fear of being afflicted by MH problems themselves made novice MH nurses unwilling to work in psychiatric/MH units. This sentiment was echoed by members of this study.
Crowe et al. (2021) highlighted an interesting finding that PMH nurses feared over-communicating with patients when attending PMH units, while Manzano-Bort et al. (2022) reported that nurses suffered from fear and stress because of patients’ aggressiveness and irritability, which led to feelings of insecurity. Fu et al. (2021) also found that psychiatric/MH nurses were frightened that patients would harm them, and similar concerns were expressed by participants in this study. These feelings contrast with nurses on medical wards, who were more fearful of harming patients by committing errors. Bingham and O’Brien (2018) found that many nurses believe that patients in psychiatric wards are dangerous, suggesting that it is critical to provide experiences that are well designed, supervised, and properly mentored to nursing students and those newly employed in MH units.
To address safety concerns, a purpose-built environment for PMH care is often considered to provide possibilities for increased nurse and patient safety. Elements such as tailoring the environment in psychiatric care areas with options for controlling patient interaction with each other, creation or use of positive distractions, individualization of patient personal space, removal of articles that might be used to do harm, creation of lines of vision and visibility, and maintaining ambient light and temperature may mediate threats to patient and nurse safety by reducing physical and mental stressors that may act as triggers to violence (Zadeh et al., 2018).
Moreover, attention by policymakers, stakeholders, and the media may be instrumental in assisting in changing public attitudes toward people with psychiatric problems and the health care providers who work to support them. Social media has been identified as a powerful influence in Saudi Arabia (Alyousef et al., 2020). Media fabrications may lead to the creation of false concepts and programs that do not accurately portray people with MH problems. Misunderstandings due to inaccurate information from the media about MH problems may contribute to the stigma experienced by nurses working in MH settings.
The enhancement or initiation of specific features of practice may require advanced specialized training and orientation for PMH nurses to benefit their patients and their own welfare (Cleary et al., 2009). Based on the findings of this study, improvement of these nurses’ skills through training and increased theoretical knowledge that employs exposure to literature and workshops, collegial mentoring by supervisory staff, and emphasis on best-practices rooted in evidence-based research as a foundation for undergraduate and continuing education teaching may be beneficial for the recruitment and retention of these badly needed professionals. However, these academic offerings need to be supplemented by real-life experiences because theoretical data retention among Saudi medical students from lectures and practice after 6 months has been found to be 5% and 75%, respectively (Colet et al., 2015).
Renewed evaluation of the inpatient psychiatric care delivery system may be a timely step. Efforts might be aimed at modification of the built environment of psychiatric inpatient units to enhance the safety of patients and employees alike. Furthermore, establishment of a clear-cut safety framework with a well-established protocol for addressing and preventing emergent situations involving potential harm to patients or staff, may provide increased confidence in safety among staff.
Based on the fourth theme which emerged from the data, additional attention may be required to retain PMH nurses in the psychiatric setting. Nurses reported that they elected to remain in the psychiatric setting because of personal expediencies. Recruitment of new graduates may need to include assessment of applicants’ knowledge and interest in psychiatric nursing as a practice specialty. Consideration of educational opportunities for personal and financial advancement and modification in team structure to meet personal needs in scheduling of shifts and vacations may be instrumental in retaining and recruiting committed PMH nurses in this area of practice as recommended by research conducted related to retention of Saudi nurses in the workforce (Alluhidan et al., 2020).
Strengths and Limitations
This study recruited a group of practicing PMH nurses in Saudi Arabia with previous experience in inpatient PMH care settings. Although the sample was small, it was characterized by participants who are experienced in inpatient PMH care which suggests that they are well suited to reflect on needs and problems in their environment, and care was taken to elicit their prespectices via thick description.
These findings reflect the publicly funded inpatient PMH environment, and conditions in privately funded facilities may differ. Furthermore, geographic locale may be a limiting factor, and needs to be considered if results are being applied in other settings.
Additional evidence-based qualitative and quantitative research may further illuminate the reasons contributing to the shortage of qualified staff nurses in MH institutions and be instrumental in providing solutions to this critical problem.
Conclusion
Nurses in PMH who participated in this study cited need for specialized education and training, stigma of MH care and caregivers in the professional health care environment and the community at large, and safety concerns as the principal obstacles to their participation in this field of practice.
These findings point to the need to ameliorate a variety of obstacles which need to be addressed to assure a stable group of specially trained PMH nurses ready to identify and establish themselves as professional practitioners in inpatient PMH settings. Based on this study, implementation of certain steps are required to be taken to arrive to this goal.
Appropriate training and orientation for nursing students in this specialized area coupled with continuing support to nurses already employed in these settings is an important beginning. The content of these experiences would be timely, evidence-based, and congruent with the milieu of the locale taking into consideration of the norms of the caregiving and patient population.
Community support is a critical element in overcoming stigma. Although MH stigma is deeply rooted in Saudi society, the pillars of Vision 2030 may be used through mass media to institute orientation of the general population regarding mental illness and its treatment (my.gov.sa, 2023).
Institutional changes in the inpatient PMH environment may assist in recruitment and retention of trained PMH specialist nurses. Attention to establishing a well-structured safety protocol, use or construction of specially built and furnished facilities aimed at safety for patients and their caregivers, availability of collegial mentoring and supervision, and continued use of administrative measures which provide incentives to seek and continue to participate in this area of care including opportunities for further education and modification of team structure and scheduling may assist in building workforce which is committed to provision of inpatient PMH care.
Footnotes
Acknowledgements
The author thanks her parent institution, King Saud University, for its support. She also thanks the reviewers and editor of this journal for their patience and expertise in the revision process.
Author’s Note
Health care managers can use the findings of this study, commissioners and authorities to improve the working environment of psychiatric/mental health nurses and thus increase the likelihood of these nurses choosing to work in psychiatric/mental health units. In particular, improving these nurses’ skills through training and a thorough orientation would be very beneficial. Staff nurses in psychiatric mental health should be provided with the competencies and knowledge specific to this sector, so it is critical to focus more on education programs and experience in the relevant clinical areas. Additional quantitative and qualitative research should be conducted to further explore the shortage of qualified staff nurses in mental health institutions. Moreover, authorities and health care providers should seek to develop media-based interventions to help to change public attitudes toward people with psychiatric problems and the health care providers who work to support them. This type of education should, over time, reduce stigma and increase nurses’ interest in working in psychiatric/mental health units, consequently impacting the quality of care in mental health services.
Author Roles
The author contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data, drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. The author agrees to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.