
Abstract
Background:
Using long-acting injectable (LAI) antipsychotic medications can improve the outcomes of patients with schizophrenia, such as reducing symptom severity and hospitalization risk. However, the outcomes of switching from oral to LAI antipsychotic medications are unclear.
Aims:
The purpose of this review is to provide a summary of the clinical, quality of life, and health care utilization outcomes of switching from oral to LAI antipsychotics among patients with Schizophrenia Spectrum Disorder.
Methods:
We thoroughly searched the PubMed, Scopus, PsycInfo, and CINAHL databases. To conduct the meta-analysis, we used the Comprehensive Meta-Analysis Program.
Results:
Forty-one articles met our inclusion criteria. After switching to LAIs, symptom severity, the number of rehospitalizations, emergency department visits, and overall health care costs were reduced. Also, social functioning significantly improved. However, no differences were observed in the frequency of outpatient visits. Pharmacy costs were increased between pre- and post-LAI initiation.
Conclusion:
Our findings support evidence that changing the route of administration of antipsychotic medications from oral to long-acting intramuscular injections can improve the clinical, quality of life, and health care utilization outcomes in people with schizophrenia. Health care practitioners might consider encouraging LAI use earlier during treatment for schizophrenia for better clinical outcomes and to reduce health care utilization associated with treatment.
The primary goal of using antipsychotic medications to treat those living with schizophrenia spectrum disorder is to decrease symptom severity, prevent relapse, and improve overall clinical outcomes (Keepers et al., 2020). A persistent challenge in treating people with schizophrenia is to maintain the continuity of effective, well-tolerated antipsychotic therapy that provides adequate symptom control and clinical stability (Haddad et al., 2014). In fact, non-adherence to antipsychotic medications varies widely, ranging from 11.0% to 71.9% (Ljungdalh, 2017; Yaegashi et al., 2020). Moreover, relapse after the first episode of psychosis ranges from 19.4% to 97.0% among people with schizophrenia (Bowtell et al., 2018). Given these varying rates of non-adherence and relapse, finding ways to support medication management is essential.
Medication management for symptoms of schizophrenia currently involves two main formulations of antipsychotic medications: oral and long-acting injectables (LAIs). After initiating an oral antipsychotic medication, it is not uncommon for people to switch to another. Studies have explained that patients switch between antipsychotic medications because of inconsistent adherence and poor tolerance of side effects (Huang et al., 2021; Keks et al., 2019; Newcomer et al., 2013). LAIs are considered an important means of supporting adherence and preventing symptom relapse with similar tolerability and efficacy profiles between first-generation and second-generation formulations (Biagi et al., 2017; Rubio et al., 2020; Uribe et al., 2020; Zolezzi et al., 2021). When considering initiating an LAI, expert consensus panels emphasize consideration of oral efficacy and tolerability as well as the potential use of LAIs earlier in the course of schizophrenia (Sajatovic et al., 2018a, 2018b). Moreover, providers, who practice from a patient-centered, recovery-oriented approach, view LAI initiation as crucial in further preventing functional declines, desocialization, reduced mortality, and promoting adherence to medications (Fang et al., 2022; Pietrini et al., 2019). Hence, it is important to examine both clinical and recovery-centered outcomes of LAI initiation for people with schizophrenia. Recent studies have reported possible advantages of using LAIs early in the course of schizophrenia treatment. In particular, they suggested that early LAI initiation within the first year of schizophrenia episodes may benefit treatment management, adherence, relapse rates, and other outcomes, resulting in lower hospitalization rates and health care expenditures (Kane et al., 2023; Munday et al., 2019).
Previous reviews have also investigated the impact of switching from oral to LAIs among schizophrenia patients. These reviews examined the effect of LAIs on medication adherence, hospitalization risks, relapse, emergency department (ED) visits/admission, or health care costs compared to oral antipsychotic medications (Kishimoto et al., 2013, 2021; Lin et al., 2021). In general, these studies determined that LAIs are often superior to oral drugs in terms of medication adherence, hospitalizations, and ED visits, but not health care costs. However, no known published studies have conducted a comprehensive review and meta-analysis on the effect of switching the administration route of antipsychotic medications from oral to intramuscular injections on both clinical and recovery-focused (e.g., quality of life) outcomes. Our current review includes recent research updates and includes additional outcomes of importance, including symptom severity and social functioning, which have not been included in prior meta-analyses.
Therefore, the purpose of this review was to synthesize the known studies that have examined the effect of switching the administration route of antipsychotic medications from oral to intramuscular injections in people with schizophrenia spectrum disorder. Specifically, we (a) conducted a systematic review on the effectiveness of switching from orals to LAIs on clinical outcomes (i.e., symptom severity, rehospitalization, outpatient, and ED visits), quality of life (i.e., social functioning), and health care utilization (i.e., health care costs) as primary outcomes and (b) performed a meta-analysis on the effectiveness of changing antipsychotic administration route on clinical, quality of life, and health care utilization.
Methods
The preregistered protocol for this systematic review was submitted to PROSPERO (registration number CRD42021249844). Our process was guided by the Preferred Reporting Item for Systematic Reviews and Meta-Analyses (PRISMA) (Page et al., 2021). We searched for indexed studies in the PsycInfo, CINAHL, Scopus, and PubMed databases. The following sets of keywords were used: “Fluphenazine Decanoate AND Haloperidol Decanoate AND Aripiprazole Monohydrate AND Aripiprazole Lauroxil AND Olanzapine Pamoate AND Paliperidone Palmitate AND Risperidone Microspheres,” “Adherence AND Outpatient Visit AND Hospitalization AND Incarceration AND Readmission,” and “Schizophrenia OR Schizoaffective OR Psychotic disorder.” All articles that matched our inclusion criteria were included in our search.
Inclusion and Exclusion Criteria
We included English-language studies published before August 2020 from peer-reviewed journals that compared outcomes before and after changing antipsychotic administration route from an oral to an LAI. We excluded meta-analyses, review articles, and non-quantitative studies.
Study Selection
Two authors (Authors 1 and 2) conducted the searches and initial screening of articles. The EndNote program was used to pool the retrieved articles, and all duplicates were removed. To select relevant articles, titles were initially screened, then, abstracts were assessed, and finally, the full texts of the retrieved articles were examined. The screeners produced a final list of relevant articles, and any disagreements over an article’s eligibility were resolved through discussion with another reviewer (Author 4).
Appraisal of Methodological Quality
Independent reviewers screened all included articles (Authors 1, 2, and 3). Two different quantitative checklists were used for critical appraisal that assess similar aspects of studies (Kmet et al., 2004; Ma et al., 2020). The first checklist was rated on a three-point scale (0 = No, 1 = Partial, and 2 = Yes). The total score for all 14 items was added and then divided by 28 (the highest number to be given) to calculate the summary score for each paper (Kmet et al., 2004). The second checklist was by the National Institutes of Health (NIH), which assessed the quality of pre-post studies (Ma et al., 2020). It includes 12 items rated as 0 = No or 1 = Yes. Results of the critical appraisal were presented in both quantitative and narrative forms. SPSS Version 28 was used to assess the inter-rater reliability among raters.
Data Extraction
Two reviewers independently (Authors 1 and 2) extracted the data. The data extraction forms included author and publication year, country where the study was conducted, design, participant characteristics, main outcomes, time points of study outcomes, and main findings.
Main Outcome Measures
Symptom severity was assessed using the Positive and Negative Syndrome Scale (PANSS), Global Assessment of Functioning (GAF), and Clinical Global Impression (CGI) scales. The PANSS includes 30 items rated from 1 (absent) to 7 (extreme). It is divided into three subscales: positive symptoms, negative symptoms, and general psychopathology. The PANSS has good inter-rater reliability and adequate construct validity (Kay et al., 1987, 1988). The second scale was the GAF, which measures mental health by rating the patient’s psychological, social, and occupational functioning on a scale of 0 to 100. The validity of assigned GAF ratings often correlates more strongly with the intensity of symptoms than with degree of impairment, especially when the severity and degree of functional impairment are incongruent (Endicott et al., 2008; Schwartz, 2007). Also, the CGI was used to measure symptom severity and treatment efficacy and has good reliability and moderate validity. The CGI is rated on a seven-point scale and includes three subscales: illness severity, global improvement, and therapeutic response (Allen et al., 2012; Ventura et al., 2008).
The Personal and Social Performance (PSP) Scale was used to assess social functioning. The PSP is a six-point Likert-type scale that includes four domains: social activities, personal and social relationships, self-care, and disturbing and aggressive behaviors. Different studies have supported the validity and reliability of the PSP scale (Nafees et al., 2012; Nasrallah et al., 2008).
To assess hospitalizations and outpatient and ED visits, we used the mean number of visits. The examining studies assessed outpatient and ED visits by collecting data from the year before (pre-LAI period) and the year after the index date (the start of the LAI period) and determining the mean number of visits. Health care and pharmacy costs were determined at the patient level as an average monthly cost before and after LAI.
We pooled the effect from studies that used the same statistical approaches and measurements. The Comprehensive Meta-Analysis (CMA) software Version 3 was used to analyze the data (Borenstein et al., 2013). Random-effects modeling was used to determine overall effect sizes as well as standardized mean differences (SMDs) and associated 95% confidence intervals (CIs). An SMD less than zero with p < .05 indicates a significant difference between treatment conditions. The heterogeneity of true effects was tested using prediction intervals for outcomes involving at least 10 studies, and
We used the Joanna Briggs Institute (JBI) System for the Unified Management, Evaluation, and Review of Information to conduct a narrative synthesis (Moola et al., 2017). The key findings from each study were then classified based on our primary outcomes of interest (symptom remission, rehospitalizations, outpatient and ED visits, health care costs, and social functioning).
Results
Studies Description
Initially, 1,587 articles were found in the research (see PRISMA flow chart, Supplementary Figure S1). Excluding duplicates, 41 studies met all inclusion criteria. Based on the two raters, the mean score of the included studies (using the NIH tool) was 8.720 (intraclass correlation coefficient r = .464, p = .023), and the average score for the included studies using the Kmet tool was 18.488 (intraclass correlation coefficient r = .808, p = .001). The quality of all included studies (N = 41) was graded as fair, with a bias risk due to the absence of blinding and not using the interrupted time series design to measure the outcomes of interest.
The total number of patients with schizophrenia who switched from oral to LAIs in the included studies was 15,754. The mean sample size of all included studies was 384.24 (range = 21–3,094). The following narrative and meta-analysis results are categorized according to the primary outcomes of interest.
Narrative Analysis
Symptom Remission
Ten studies measured PANSS scores from before to after LAI treatment. From the baseline of each study to its endpoint, the PANSS total score significantly declined (Table 1). Also, 10 studies reported significant reductions in the CGI scores after switching to LAIs (see Table 1). Finally, five studies reported that the GAF scores were significantly improved from baseline to endpoint (Table 1).
Characteristics of Included Studies.

Data for the meta-analysis was derived from an abstract presentation with the following citation: Beauclair et al. (2005).
Rehospitalization
All except one (Bourin et al., 1998) of the 36 studies that reported rehospitalizations found a decrease in the number of rehospitalizations after switching to an LAI (Table 1).
Outpatient and ED Visits
Eight studies reported the number of outpatient visits pre- and post-LAI initiation (Table 1). Two studies showed no differences (Fefeu et al., 2018; Patel, Emond, et al., 2020), while two showed decreases in the number of outpatient visits (Lee et al., 2020; Zhdanava et al., 2021). However, four studies showed an increase in the number of outpatient visits/claims between pre- and post-LAI initiation (Chang et al., 2012; Fuller et al., 2009; Patel, El Khoury, et al., 2020; Ren et al., 2011). Also, five (Crivera et al., 2011; Hsia et al., 2017; Koczerginski & Arshoff, 2011; Patel, Emond, et al., 2020; Zhdanava et al., 2021) of eight studies reported significant reductions in the number of ED visits upon initiation of LAIs (Table 1).
Health Care Costs
Twelve studies compared the health care costs pre- and post-LAI initiation (Table 1). Ten studies reported reductions in overall health care costs after LAI initiation (Fefeu et al., 2018; Kamat et al., 2015; Lee et al., 2020; Mahlich et al., 2020; Olivares et al., 2008; Patel, El Khoury, et al., 2020; Patel, Emond, et al., 2020; Peng et al., 2011; Willis et al., 2010; Zhdanava et al., 2021). However, after switching to LAIs, six studies reported an increase in pharmacy costs (Chang et al., 2012; Fuller et al., 2009; Olivares et al., 2008; Patel, Emond, et al., 2020; Willis et al., 2010; Zhdanava et al., 2021), four studies found increases in outpatient costs (Chang et al., 2012; Fuller et al., 2009; Mahlich et al., 2020; Patel, Emond, et al., 2020), and one study found a decrease in the outpatient costs (Lee et al., 2020) (Table 1).
Social Functioning
Four of five studies showed significant improvements in PSP scores from the oral to the LAI treatment period (Devrimci-Ozguven et al., 2019; Emsley et al., 2017; Kwon et al., 2015; Li et al., 2019; Si et al., 2016) (Table 1).
Meta-Analysis
Meta-analyses were conducted to pool the results of studies on symptom remission, rehospitalizations, outpatient and ED visits, and social functioning. Heterogeneity varied across models; therefore, a random effects model was used. Studies that provided data related to health care costs used different statistical approaches. Thus, the pooled effect size could not be calculated.
Symptom Remission
The pooled analysis of the studies showed LAIs were superior in decreasing the PANSS score compared to the oral antipsychotic treatment period (n = 2,622, effect size = −0.225, 95% CIs = [−0.286, −0.164], p < .001; I2 = 50.52%, p = .033) (Figure 1). Also, the forest plot showed significant differences in the mean CGI score when switching from oral to LAI (n = 2,319, effect size = −0.262, 95% CIs = [−0.335, −0.188], p < .001; I2 = 60.755%, p = .006) (Figure 2). The effect size for mean GAF scores could not be calculated because the studies varied widely in the statistical approaches to analyzing this outcome.
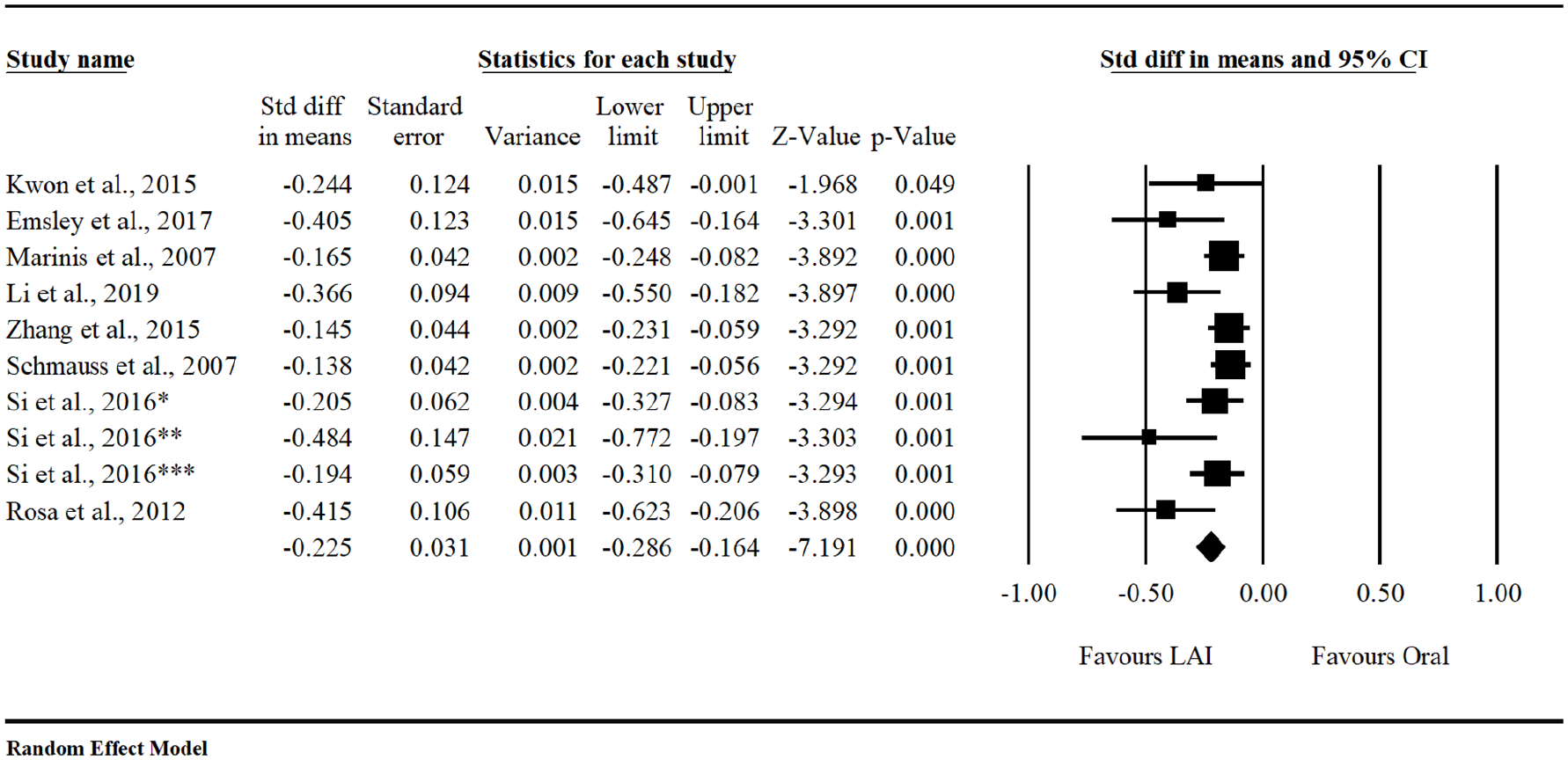
Forest Plot of the Change Between LAIs and Orals in the Mean PANSS Score.
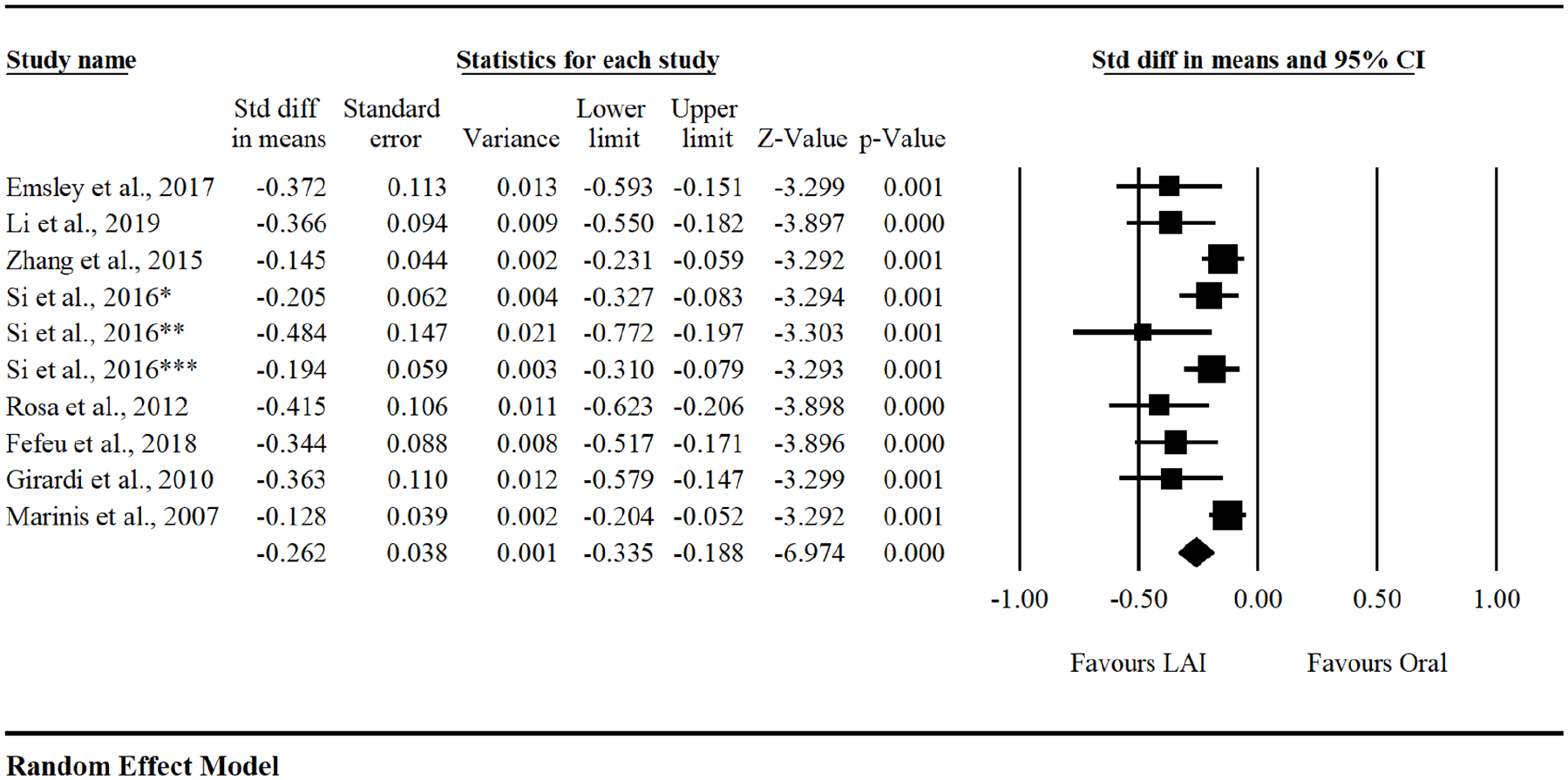
Forest Plot of the Change Between LAIs and Orals in the Mean CGI Score.
Rehospitalization
The forest plot showed a significant reduction in the mean number of rehospitalizations when patients switched from an oral to LAI antipsychotic (n = 5,038, effect size = −0.224, 95% CIs = [−0.318, −0.131], p < .001; I2 = 82.10%, p < .001) (Figure 3).
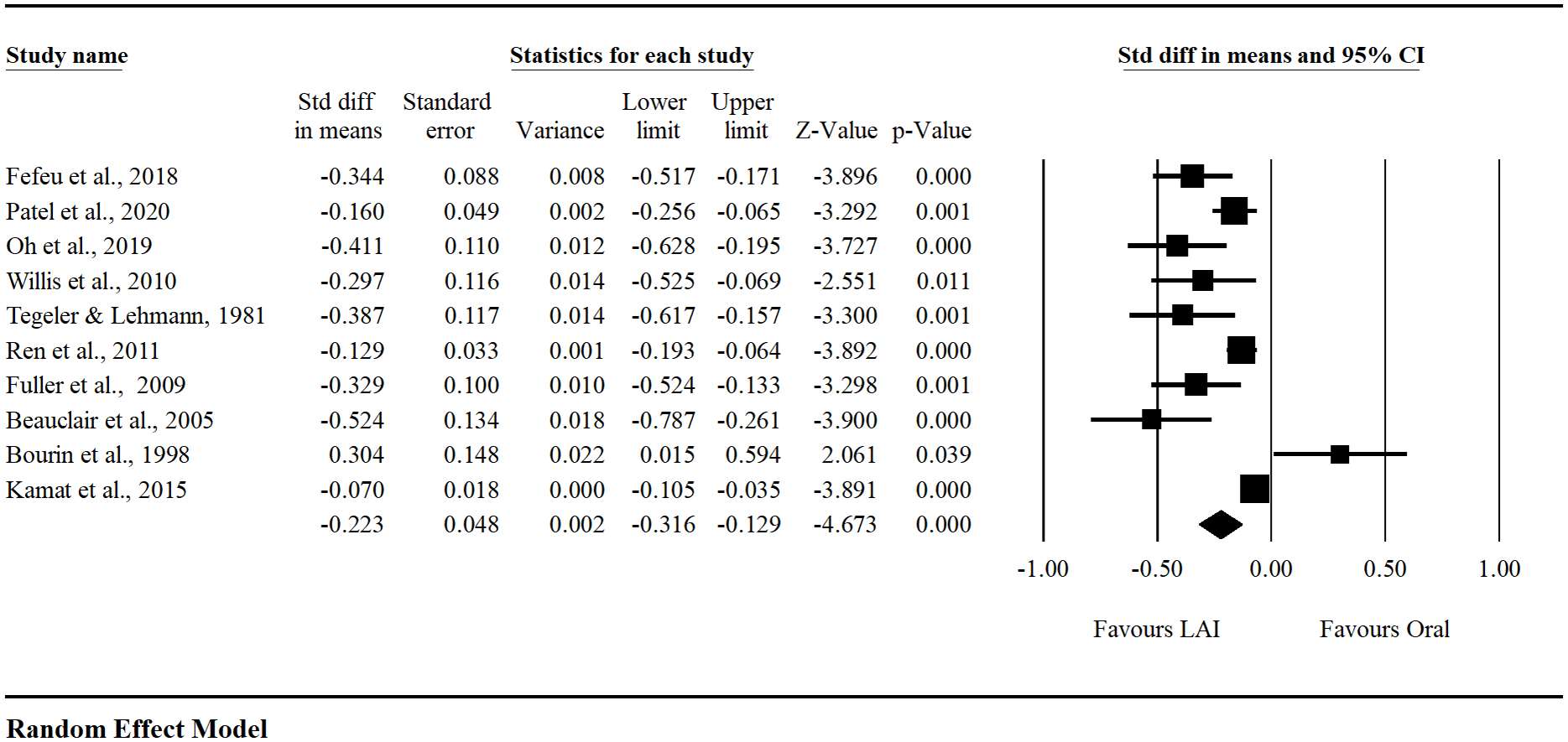
Forest Plot of the Changes Between LAIs and Orals in the Mean Number of Rehospitalizations.
Outpatient and ED Visits
We calculated the pooled effect size of switching from oral to LAI on the mean number of ED visits for only five of eight studies that used similar statistical approaches for outpatient visits. The pooled analysis of these five studies found no differences in switching from oral to LAI on the mean number of outpatient visits (n = 3,570, effect size = −0.022, 95% CIs = [−0.112 to 0.068], p < .628; I2 = 78.769%, p < .001) (Figure 4). However, the pooled effect size of switching from oral to LAI on the mean number of ED visits was not calculated because these studies used different statistical approaches.
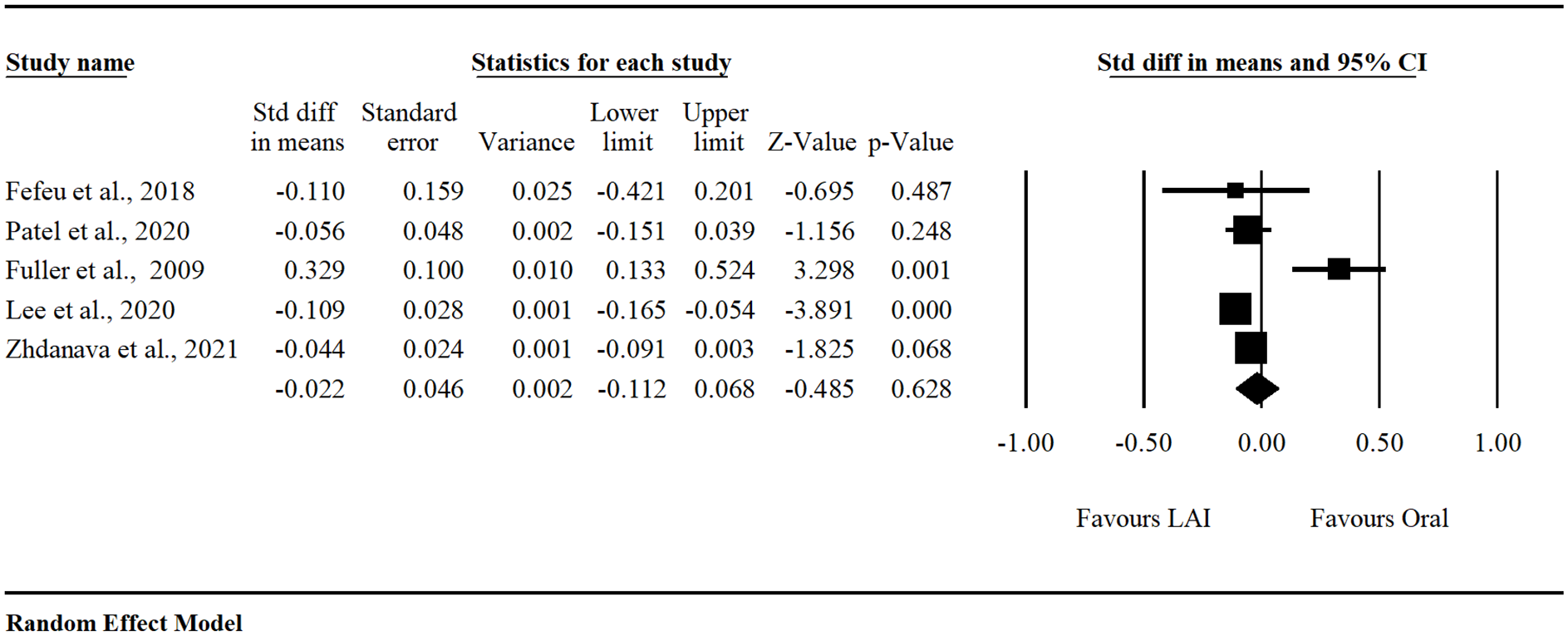
Forest Plot of the Changes Between LAIs and Orals in the Mean Number of Outpatient Visits.
Social Functioning
Four studies found that switching from an oral to LAI antipsychotic resulted in significantly increased PSP mean scores (n = 2,892, effect size = 0.432, 95% CIs = [0.324, 0.539], p < .001; I2 = 0.00%, p < .001) (Figure 5).
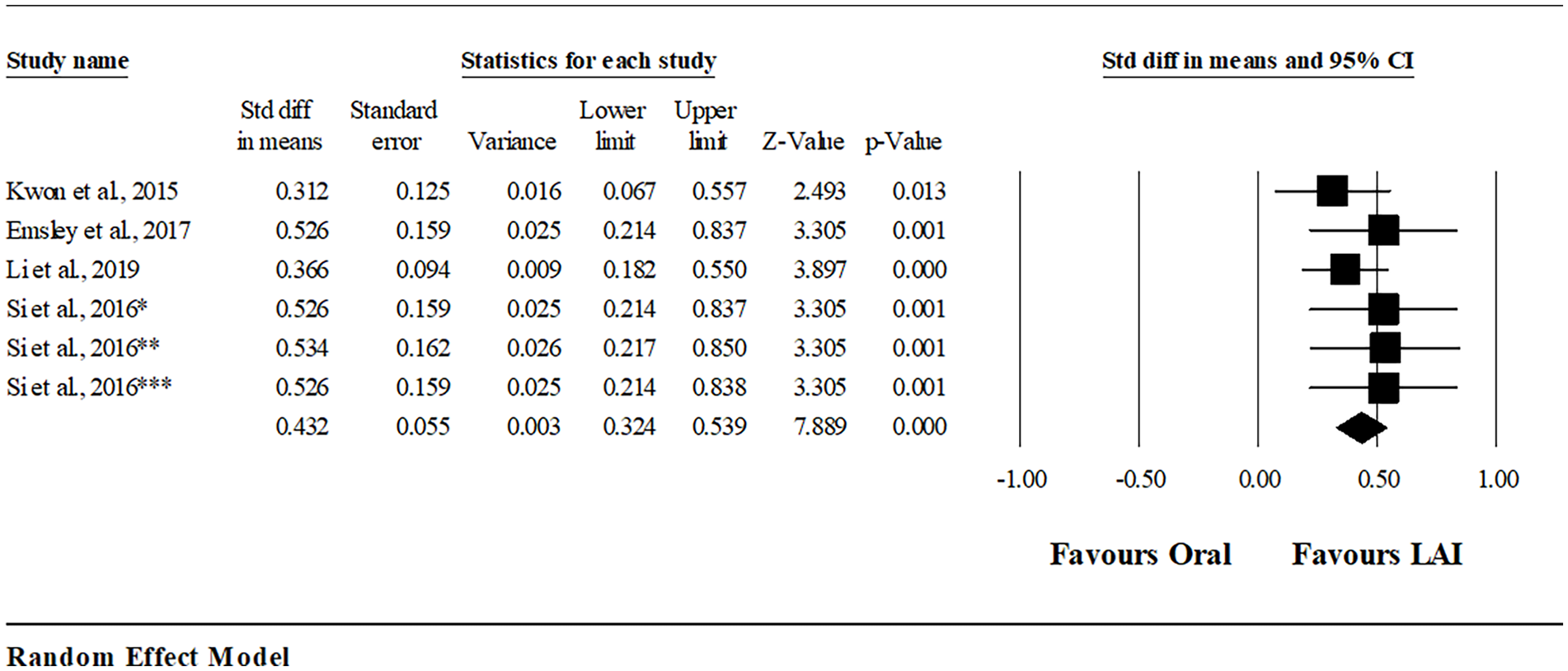
Forest Plot of the Changes Between LAIs and Orals in the Mean PSP Score.
Publication Bias
We used funnel plots, Egger’s regression test, and Duval and Tweedie’s trim and fill methods to assess publication bias. The PANSS, CGI, and rehospitalizations outcomes were reported in at least 10 studies; therefore, publication bias for these outcomes was evaluated. The three funnel plots were asymmetrical. The effect sizes were somewhat altered after applying the trim and fill procedure to correct for any publishing biases. The point estimate for the PANSS was −0.16476 (95% CIs = [−0.23367, −0.09584]), the CGI was −0.20394 (95% CIs = [−0.27612, −0.13176]), and the rehospitalizations were −0.18050 (95% CIs = [−0.26848, to −0.09252]). Hence, these results suggested little evidence for publication bias.
Discussion
The purpose of this systematic review was to synthesize the evidence regarding the effect of switching from oral to LAI antipsychotics on patient outcomes. Our findings, indicating that switching from an oral to LAI resulted in greater symptom remission (PANSS, CGI, and GAF), are similar to the results of a recent meta-analysis (Kishimoto et al., 2021) and are supported by new additional studies (Lee, 2021; Strunoiu et al., 2021). Recent studies indicate that patients might experience symptom improvement associated with LAI use as a result of improved medication adherence (Kishimoto et al., 2021; Okoli et al., 2022). Similarly, the greater reductions in rehospitalizations and ED visits and improvements in social functioning because of switching to LAIs might also be enhanced by improved medication adherence (Lin et al., 2021; Magliocco et al., 2020). Thus, these findings lend support for switching to LAIs when indicated to support recovery among those with schizophrenia.
In addition, our findings demonstrated that switching to LAIs was linked to lower overall medical care costs compared to treatment with oral antipsychotics. However, pharmacy costs increased after switching to LAIs. In a recent meta-analysis of U.S. studies, Lin et al. (2021) similarly reported increases in pharmacy costs after switching from an oral to an LAI. However, the study also found decreases in rehospitalizations and overall medical care costs. In other words, although switching to LAIs may result in increased pharmacy-related costs, these costs might be offset by overall lower medical costs. Hence, taken together, switching to LAIs might have an additional benefit of reduced health care utilization apart from pharmacy costs.
The present findings have some limitations. First, the effect of changing antipsychotic administration route on patient adherence outcomes was not investigated in this study because few studies have reported this phenomenon. Second, the types of LAIs and oral antipsychotics were different (e.g., first-generation vs. second-generation) in most of the included studies. Thus, future studies may examine the effect of switching between specific antipsychotic types on clinical outcomes. Third, this review could not account for variations in patient characteristics or clinical settings prior to and after switching to an LAI, which might have introduced biases affecting our primary outcomes.
Despite the limitations inherent in the studies included in our review, we found that changing antipsychotic administration route can be beneficial for clinical, quality of life, and health care utilization outcomes among people with schizophrenia spectrum disorder. Total pharmacy costs may increase, but this increase may be offset by decreases in medical care costs and fewer rehospitalizations. Future research is needed to examine the effectiveness of changing antipsychotic administration route on adherence, as well as ways to improve accessibility while lowering pharmacy costs. Such studies will provide evidence to support clinical outcomes associated with treatment for schizophrenia.
Implications for Practice
Mental health providers who have the authority to prescribe treatment should clearly communicate with patients and caregivers about the risks of long-acting injectable antipsychotic medications, for example, pain at injection site, extrapyramidal side effects, and weight gain. Also, mental health providers should discuss the benefits of switching to LAIs as part of evidence-based decision-making, for instance, decreased frequency of medication administration, lower risks of rehospitalization, and improved quality of life.
Conclusion
The outcomes of this systematic review demonstrated that after switching to an LAI, patients with schizophrenia spectrum disorder may experience improvements in clinical, quality of life, and health care utilization outcomes. However, there were inconsistencies in the findings related to changes in outpatient visits. Moreover, half of the reviewed studies reported increases in pharmacy costs following the switch to an LAI. In addition, the findings that switching from an oral to an LAI improved symptom remission, social functioning, and decreased rehospitalizations were supported by the pooled analysis. These findings are important in guiding future research and informing evidence-based practice related to the use of antipsychotics for patients with schizophrenia spectrum disorder.
Supplemental Material
sj-pdf-1-jap-10.1177_10783903241279605 – Supplemental material for Clinical, Quality of Life, and Health Care Utilization Outcomes of Switching the Administration Route of Antipsychotic Medications Among People With Schizophrenia Spectrum Disorder: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-1-jap-10.1177_10783903241279605 for Clinical, Quality of Life, and Health Care Utilization Outcomes of Switching the Administration Route of Antipsychotic Medications Among People With Schizophrenia Spectrum Disorder: A Systematic Review and Meta-Analysis by Amani Kappi, Tianyi Wang, Bassema Abu farsakh and Chizimuzo T. C. Okoli in Journal of the American Psychiatric Nurses Association
Footnotes
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported, in part, by the Cabinet for Health and Family Services, Department for Medicaid Services under Agreement titled “Assessing the Impact of Long-Acting Injectables on Psychiatric Treatment Outcomes among Medicaid Beneficiaries.”
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.