
Abstract
Objective
This paper updates the psychiatric mental health (PMH) nursing community regarding the progress of five recommendations for policy and practice to enhance workplace violence (WPV) prevention. This information should be useful to nurses in their efforts to advocate for workplace safety.
Methods
A comprehensive search of current literature, organizational action, and national policy relevant to the recommendations are reviewed and discussed to enhance WPV prevention and safety.
Results
Workplace safety is a critical concern for PMH nurses and has far-reaching implications in PMH nursing settings. While there has been implementation of state policy around WPV, federal legislation remains stalled. The national accreditation standards continue to provide individual institutions guidance around WPV data collection, reporting, and analysis, but these data do not inform national efforts particularly around defining requirements for mechanisms to support healthcare workplace protection. However, recent research continues to document both prevalence and associated conditions/quality metrics. While dashboards are now available for public reporting of select WPV data, nationally the public reporting standards remain the same. Organizing a nursing voice in WPV reporting resulted in interesting exemplars. Thus far, no data are available on efforts to include safety in nursing curricula.
Conclusions
The safety of nurses, particularly PMH nurses, is a multi-faceted problem that will require efforts in regulatory, organizational, educational, and personal behavior change.
Two years ago, a group of psychiatric mental health (PMH) nurse leaders developed a statement addressing the crisis of increased violence against healthcare workers. This topic is particularly salient to PMH nursing because of the increased risk of violence in the psychiatric setting (Alamri et al., 2023; El-Kass et al., 2025; Jang et al., 2022). They also initiated a policy dialogue proposing a holistic approach to workplace violence (WPV) prevention (American Academy of Nursing, 2023, 2024) with a separate policy paper published in Nursing Outlook (Schimmels et al., 2025). To achieve a wide dissemination of these ideas, including PMH nurses, recommendations to address WPV were published as a Health Affairs op-ed (Beeber et al., 2023). These recommendations were subsequently endorsed by the American Psychiatric Nurses Association (APNA) in their issue statement (APNA, 2023).
Since then, a variety of activities to disseminate these recommendations and garner support from other organizations have occurred (Delaney et al., 2024; Hauenstein et al., 2024; Schimmels et al., 2024), including the American Nurses Association’s (ANA) National WPV Prevention Committee representation. As PMH nurse leaders with continuing concern for nurse safety, and enduring advocacy for the recommendations, the purpose of this paper is to discuss updates and propose next steps using a comprehensive search of current literature, organizational action, and policy; thus keeping a focus on priority actions for PMH nursing to address WPV. A summary of recommendation updates is organized in Table 1, with one additional recommendation added, more specific guidance on unit training and education, particularly for PMH nurses.
2025 Urgent Recommendations and Action Steps for WPV Prevention.
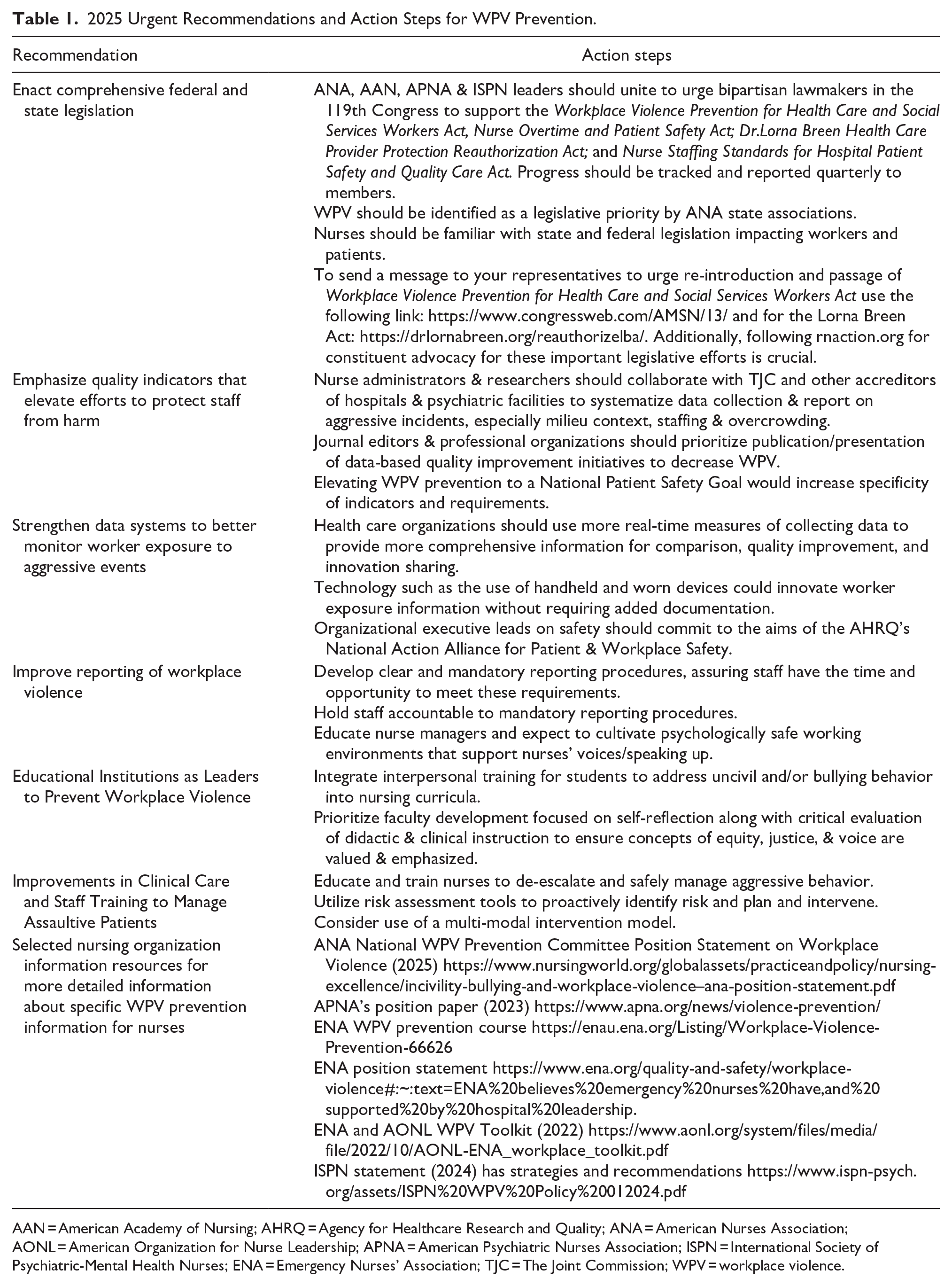
AAN = American Academy of Nursing; AHRQ = Agency for Healthcare Research and Quality; ANA = American Nurses Association; AONL = American Organization for Nurse Leadership; APNA = American Psychiatric Nurses Association; ISPN = International Society of Psychiatric-Mental Health Nurses; ENA = Emergency Nurses’ Association; TJC = The Joint Commission; WPV = workplace violence.
Background
The National Institute for Occupational Safety and Health (NIOSH) defines WPV as an act or threat of violence that ranges from verbal abuse to physical assaults that are directed toward people at work or on duty (NIOSH, 2024). Nurses should feel safe at work. In a recent meta-analysis of WPV prevalence involving nurses, the investigators reported that 35% of nurses experienced aggression from patients, family members, or visitors; a pooled prevalence rate from 37 studies, with the majority evaluating WPV within the past 12 months. The WPV prevalence was higher (59%) for nurses working in emergency departments, corrections, and psychiatric settings, with 50 to 97.6% of PMH nurses reporting exposure to WPV (Andersen et al., 2019; Jang et al., 2022; McLaughlin & Khemthong, 2024). A Bureau of Labor Statistics (BLS, U.S. Department of Labor, 2022) report attributes 13% of all missed workdays due to WPV. WPV contributes to poor mental health, burnout, moral injury, reduced productivity, turnover intention, staffing issues, higher risks for a variety of patient/client safety issues, and high costs related to time off and treatments (American Hospital Association, 2021; BLS, 2022; Jang et al., 2022; Konttila et al., 2021; Hsiao et al., 2022).
The safety of nurses is a multi-faceted problem that will take multi-factorial solutions. Several WPV risk factors include personal factors (e.g., inexperienced staff) as well as expectations of patients, families, inadequate manager skills, understaffing, rigid hierarchical work structures, wait times, shift work, high stress, poor teamwork, and job dissatisfaction (Lim et al., 2022; Pagnucci et al., 2022). Indeed, studies on WPV view it as a combination of staff, ward circumstances, and patient factors, including diagnosis (psychotic disorders), substance use disorder, and dementia (Salzmann-Erikson & Yifter; 2020; Weltens et al., 2021). But as Weltens et al. (2021) point out, the patient-related risk factor offers the fewest possibilities in WPV prevention efforts. In addition, too tight a focus on patient risk variables can prime staff to adopt a view of patients constricted to their risk characteristics (Deveau, 2024).
Educational interventions are insufficient by themselves (Amara & Hansen, 2024; Daguman et al., 2024; Mundey et al., 2023), and WPV is underreported with nurses’ fear of consequences, lack of visible changes after reporting, and lack of an efficient and user-friendly reporting system as reasons for not reporting (Spencer et al., 2023). There is a pressing need to mitigate WPV risk and to reinforce the ability of policymakers, nursing leaders, and healthcare administrators to ensure the safety of the PMH nursing workforce. The six recommendations are: enact comprehensive federal legislation, emphasize quality indicators, strengthen data systems, improve reporting, educational institutions as leaders to prevent WPV, and guidance on unit training and education, particularly for PMH nurses.
Enact Comprehensive Federal and State Legislation
Several key federal legislations focus on the work environment for nurses (ANA, 2025b; govtrack.us, 2023, 2024, 2025a, 2025b). Initially proposed in 2018, the Workplace Violence Prevention for Health Care and Social Services Workers Act failed to gain traction to become law after multiple reintroductions in Congress over the past 7 years (govtrack.us, 2025b). This comprehensive legislation creates a federal standard for nurses across the country to address WPV prevention, moving beyond best practices to make Occupational Safety and Health Administration (OSHA) guidelines the standard across healthcare (Collins, 2024; Solomon, 2024). Despite overwhelming nursing support for this legislation, including APNA, ISPN, and ANA (American Nurses Association, 2024), adversaries have expressed concerns about financial strain and additional burden on healthcare organizations (American Hospital Association, 2021; Petrino, 2022). The Nurse Overtime and Patient Safety Act limits mandatory overtime for nurses and offers protection for nurses filing complaints (govtrack.us, 2024b), while the Nurse Staffing Standards for Hospital Patient Safety and Quality Care Act requires a staffing plan with specified nurse-to-patient ratios based on unit (govtrack.us, 2023). The Dr. Lorna Breen Health Care Provider Protection Reauthorization Act (govtrack.us, 2025a) destigmatizes healthcare professionals from seeking mental health assistance.
While federal guidelines are pending, state-level policies have grown exponentially. Several states require comprehensive WPV prevention efforts in healthcare, such as procedure reviews, training, reporting, and post-incident services (LexisNexis, 2023; Livanos, 2023; Ninan et al., 2024). Mandating employer-run programs, identity protection, facility signage, and criminal penalties are among state-level policies that could lay the groundwork for much-needed national policy reform (Ninan et al., 2024).
Next Steps
It is advisable that the PMH nursing community takes immediate action to support the federal legislation mentioned above. Securing bipartisan support will be necessary to move legislation through Congress, an action that may respond to a united show of support from many nursing organizations. Links are listed in Table 1 to send messages to representatives and find out more about these pivotal policies. Additionally, understanding the proposed and in-place policies at the state level is crucial and warrants PMH nursing support.
Emphasize Quality Indicators That Elevate Efforts to Protect Staff From Harm
This recommendation arose from the lack of quality indicators for reporting incidents of WPV in the current inpatient quality/safety accreditation systems, such as The Joint Commission (TJC) or National Committee for Quality Assurance. Accreditation systems lack standardized, publicly available quality indicators to measure WPV incidents and gauge prevention efforts. Three recent trends around capturing quality indicators for injury/assault are noteworthy: one, the increase in public data of WPV incidents. Recent publications utilized structured reviews to pool estimates of violence against staff (McLaughlin et al., 2024; O’Brien et al., 2024) and available national data (Meese et al., 2024). Prevalence reports are emerging on hospital systems’ analysis (Doehring et al., 2024) and innovative methods to measure the rate of WPV, such as the use of nurse-held event counters, which recorded incidents in real time and later elaborated in Aggressive Incident and Management Logs (Iennaco, Molle, Allegra, et al., 2024). Kim & Kim (2023) demonstrated the effectiveness and acceptability of nurses documenting WPV using a Violent Event Severity Tool that lists six types of patient violence and severity indicators to improve the consistency and reporting of violence types and their severities.
A second trend is the examination of the organizational and system factors related to WPV (Lim et al., 2022). In a comprehensive literature review, Lyver et al. (2024) identified 229 indicators grouped via a Donabedian system into structural (e.g., organizational preparedness), process (e.g., occurrence frequency), and outcome measures (e.g., harm, post-incident intervention). This provides a guide for unit staff in systemizing data on the patterning of violence incidents and monitoring contributing environmental conditions (staffing, overcrowding) to gauge the success of prevention strategies.
A third promising trend involves staff teams using their WPV data for quality improvement. One initiative targeted improving staff therapeutic communication that reduced staff-directed violence by 75% (Amara et al., 2024). Similar efforts were evident at the 2024 APNA Annual Conference, where hospital teams reported on their WPV reduction efforts through a variety of strategies such as implementing reporting systems, training programs, and developing a crisis response team (Malone, 2024). Dialoging and publishing around WPV quality improvement efforts are critical for building data on risk, contextual factors, and effective strategies.
Next Steps
Systematizing data collection on aggressive incidents using structural and process indicators, particularly milieu context and shifting dynamics such as staffing and overcrowding, is recommended. Joint Commission standards should be utilized with authentic nursing participation in how data are gathered, what data are gathered, and worksite analysis. Elevating WPV prevention to a National Safety Goal would increase the specificity of indicators and requirements (e.g., TJC, 2019b). Continued research and public data reporting are needed to establish baselines of trends of WPV (Wright, 2024) and facilitate the evaluation of prevention strategies. Publication of an organization’s WPV data and quality initiatives will inform the field and build an evidence base for effective reduction strategies (e.g., Keller et al., 2022).
Strengthen Data Systems to Better Monitor Worker Exposure to Aggressive Events
Issues in data collection arise due to poor reporting and monitoring of WPV, and a lack of identification of prevalence to compare across settings. For example, TJC standards have been updated, but there are no specific tools or processes suggested to monitor incidents (TJC, 2023, 2024). Most reporting systems focus on WPV incidents rather than exposure, making identification of risks and consequences difficult. Additionally, data outside of patient/family, such as worker-on-worker violence, are not captured (Yusoff et al., 2023). Since information on exposure to aggression is only available with worker injuries using BLS data on time lost from work, reporting is grossly underestimated and impedes understanding of negative health consequences, work satisfaction, retention, or other outcomes. A recent study using a real-time measure of aggression in an inpatient medical setting identified 179 aggressive events where only two resulted in injury, showing current sources are missing many worker exposures (Iennaco, Molle, Allegra, et al., 2024). A variety of aggression measurement tools are available, including several observer-rated scales, which record information on an incident retrospectively, although most do not provide exposure information (for a review of aggression measurement tools, see Iennaco, Molle, Lauvrud, et al., 2024).
Technology to innovate future practice must be carefully evaluated. Real-time counter-measures and logs immediately after an event could reduce burden and recall bias (Iennaco, Molle, Allegra, et al., 2024). Wearable and real-time handheld devices could enhance exposure collection without requiring additional documentation (Siwicki, 2024). Innovations, including predictive analytics that use real-time data, the Internet of Things (IoT)-generated data, and machine learning algorithms to analyze large amounts of data, could identify a potential WPV incident. When added to wearable devices, IoT sensors can monitor vital signs and heart rate variability, enhancing decision-making (Whitley, 2023).
Next Steps
Strategies to improve data and systems to monitor, reduce, and prevent WPV are needed. Hospitals can improve their data by adhering to TJC definitions of WPV and increasing the specificity of information collected by shift, day, duration, and type (TJC, 2024). Data dashboards allow comparison of the prevalence and characteristics of WPV incidents across settings and institutions. The National Action Alliance for Patient and Workforce Safety site and National Healthcare Safety Dashboard are first steps toward public availability of information benchmarking WPV prevalence and data collection strategies (Agency for Healthcare Research and Quality [AHRQ], 2024). Additionally, the dashboard includes links to organizational self-assessment and existing sources of information on WPV, including existing OSHA reports, guidelines, and education as a centralized resource for information (AHRQ, 2025). Even though the information is limited now, expanding the data available and identifying the data sources will be an important strategy for improving workplace safety (AHRQ, 2025).
Improve Reporting WPV
Speaking up to report incidents of WPV is a professional nursing behavior essential to understanding the full scope of the problem for professional nursing and foundational in enacting improvements in workplace conditions at the local level. Violence toward the nursing workforce is maintained and exacerbated by actions (or inactions) of administrators that too frequently make it difficult for nurses to advocate for patients or themselves (Altmiller, 2024; Etchegaray et al., 2020; Levine et al., 2020; Okuyama et al., 2014). The literature shows that healthcare organizational policies and behaviors of individual nurses contribute to the unwillingness of nurses and other staff to speak up because these policies and behaviors promote psychologically unsafe environments and create fears of reprisal (Lee et al., 2022; Levine et al., 2020; Morrow et al., 2016a; Seo & Lee, 2022). Nurse-on-nurse bullying and incivility, including criticizing others publicly, withholding information, unfair assignments, and other insensitive behaviors, cause fear and unwillingness to report WPV (Anusiewicz et al., 2020; Hsiao et al., 2022; Pogue et al., 2022; Smith et al., 2016; Tedone, 2020). Attitudes such as nurses’ belief that aggression from patients is part of the job or that reporting is unimportant contribute to poor reporting because nurses believe their actions are not relevant to improving workplace conditions (Etchegaray et al., 2020; Huang et al., 2022; Jiang et al., 2018).
There has been some progress in recognizing the significance of nurses’ silence in perpetuating WPV. The ANA has launched a campaign to end the abuse of nurses, focusing on silence as an important contributor (ANA, 2025a). Nurses at Maine Medical Center and University Medical Center in New Orleans have organized “speak outs” to draw attention to safety concerns and highlight administrators’ inaction regarding WPV (National Nurses United, 2022, 2024). The Emergency Nurses Association founded the “No Silence on ED [Emergency Department] Violence” campaign for systemic organizational change for the safety of ED nurses, physicians, and staff. Major news outlets, including the New York Times, are beginning to publicize the extent of and negative outcomes from WPV (Ouyang et al., 2023). Leveraging the power of nurses’ collective voices underscores the importance of reporting WPV as a professional responsibility and is necessary to catalyze the cultural and organizational change needed to promote workplace safety.
Next Steps
Ideally, hospital administrators both set policies and provide incentives for reducing incidents of WPV. Its prevention is most likely to be achieved by well-trained nurse managers (Arnetz, 2022; Arnetz et al., 2019; Gillespie et al., 2015; Morrow et al., 2016b). Managers should be selected for leadership characteristics, receive supervision, and training to maintain positive interpersonal relationships with nurses (Arnetz et al., 2019; Asante, 2025; Gilbert et al., 2016). Nurse managers must provide “psychologically safe” nursing units where speaking up is considered an important professional behavior and where nurses are not fearful of reprisals from supervisors or peers (Arnetz et al., 2019; Asante, 2025; Wawersik et al., 2023). An important component of psychologically safe environments is “zero tolerance” of aggression, bullying, or incivility (Nachreiner et al., 2005; Spruce, 2014; St-Pierre & Holmes, 2008). Policies that provide a clear expectation of reporting incidents of violence, guidance about what is a reportable event, and ensuring reporting occurs during the nurses’ paid work time greatly improve WPV reporting (Huang et al., 2022; Levine et al., 2020; Seo & Lee, 2022).
Another step is obtaining a more nuanced, multi-vocal approach to engaging nurses to speak up to report WPV and improve conditions in their workplace. Speaking up is an agentic, prosocial voice that represents both a skill set and solid grounding in professionalism and experience (Hauenstein, 2025; Van Dyne et al., 2003). Even when nurses are emotionally and professionally prepared to speak up, their speaking-up behaviors must be cultivated through interpersonal skills training, values clarification, and simulation strategies (Sayre et al., 2012; Schwappach, 2018; Shanks et al., 2020). Ongoing professional development should be structured to provide a healthy work environment, education, and training, such as WPV prevention and management strategies (Maloney & Harper, 2022).
Educational Institutions as Leaders to Prevent WPV
Prevention of WPV begins in pre-licensure nursing education, focused on content as well as faculty role modeling. Nursing Essentials and ANA Code of Ethics doctrines provide students with a strong professional identity, a sense of equity, and an unwillingness to tolerate physical, verbal, non-verbal, and other forms of aggression and abuse in the workplace (American Association of Colleges of Nursing [AACN], 2021; ANA, 2025b; Burton et al., 2022; Burton, 2020; Croft & Cash, 2012; Huang et al., 2021; Roy et al., 2022). While there is evidence that faculty teach content relevant to WPV, there also is evidence that pre-licensure nursing students’ speaking-up behaviors decline over the course of their education (Altmiller, 2024; Bedgood & Mellott, 2021). These findings suggest faculty may not be providing the role modeling necessary for students to feel safe. Faculty may be ineffective in modeling speaking-up behaviors because there is also substantial evidence that many faculty are engaged in WPV as perpetrators and recipients of academic bullying (Beckmann et al., 2013; Condon, 2015; LaSala et al., 2016; Rutherford et al., 2019). Pre-licensure students both observe and are recipients of faculty bullying, undermining their confidence and willingness to speak up and advocate for themselves in future workplaces, and learn unhealthy and counterproductive communications and behaviors when they experience WPV (Mott, 2014; Rutherford et al., 2019; Seibel, 2014). Providing didactic education in WPV management and prevention is insufficient when students do not receive specific interpersonal skills training to address uncivil and bullying behavior from nurse managers or peers, or observe faculty practicing effective speaking-up and other professional communication behaviors (Cleary et al., 2012; Delker et al., 2020; Hauenstein & Schimmels, 2024; Lewis, 2006).
Next Steps
Faculty must begin to accept their responsibility for ensuring that graduates have the interpersonal skills and professional values to accept and act on their responsibility to prevent WPV. It is not possible, however, for nursing faculty to provide students with this knowledge and skills when incivility and bullying are tolerated in nursing academic settings (Kemp, 2024; O’Flynn-Magee et al., 2021). To lead in WPV prevention, academic nursing leaders need to engage in careful self-evaluation, implement zero tolerance policies, and provide faculty with didactic and simulated education designed to improve recognition of uncivil and bullying behavior, at all levels of the institution, and interpersonal skills training and support to enact changes in how faculty communicate (Beckmann et al., 2013; Dzurec, 2013; LaSala et al., 2016; Pattni et al., 2019; Rutherford et al., 2019; Spruce, 2014; Varty et al., 2024). Professional nursing organizations whose membership is populated by academic leaders are well-positioned to set policy, including zero tolerance policies, and to provide professional development opportunities to address this major problem.
Although it is important to ensure that the curriculum contains elements necessary to ensure that students possess knowledge about WPV and professional values that underlie integral professional practice, it is not operationalized in a way that would ensure that students receive communication skills training that would be effective in discordant situations (Goldsmith et al., 2022). Challenging uncivil behavior of peers, administrators, or faculty requires skills in conflict management and therapeutic interactions, both communication skill sets essential for changing behavior while maintaining relationships (Abadi, 2021; Kraatz et al., 2022; Monjaras-Gaytan et al., 2021). Effective communication skills cannot be integrated into the curriculum if nursing faculty do not have these skills, and instead model silence, incivility, and outright bullying of others. Similar to that seen in healthcare institutions, nursing faculty normalize and deny the extent of incivility and bullying, and the effects it has on themselves, peers, and students (Dzurec, 2013; Iyer et al., 2023).
New Addition: Improvements in Clinical Care and Staff Training to Manage Assaultive Patients
Organizations providing clinical care must integrate models that are shown to prevent and reduce aggression and violence in psychiatric settings. Implementation of effective strategies to engage with people exhibiting aggression and violence is critical to prevent, mediate, de-escalate, and reduce WPV. Strategies that integrate person-centered interventions, environmental and milieu management, and trauma-informed principles can be effective in reducing or eliminating violence as a safety risk in psychiatric settings (Gaynes et al., 2017). Several types of intervention are suggested: staff education and training, risk assessment, and intervention models (APNA, 2022a, 2022b).
Education and training offer skills to prevent, de-escalate, and safely manage aggressive behavior in clinical settings. The ANA (2025c) and APNA (2022a, 2022b) recommend that organizations provide annual training programs focused on the prevention of violence. Some models involve training staff to become in-house experts who can then educate other workers to prevent and manage violence, to integrate context-specific knowledge. Common principles used in WPV prevention training programs include therapeutic engagement, communication skills, conflict mediation, managing power dynamics, risk assessment, and trauma-informed care principles (ANA, 2025c; APNA, 2022a, 2022b). Nurses can also draw from WPV prevention strategies informed by several toolkits, online courses, and other resources (Emergency Nurses Association, 2022; NIOSH, 2013).
A variety of risk assessment tools are available for use in inpatient psychiatric settings (TJC, 2019a), facilitating proactive identification of risk, planning, and intervention. Risk Assessment tools include the Overt Aggression Scale (Silver & Yudofsky, 1991; Yudofsky et al., 1986), the Brøset Violence checklist (Almvik & Woods, 1998), and the Brief Rating of Aggression by Children and Adolescents (Barzman et al., 2011). Other risk assessment and aggression measurement tools are described in a recent text on Coercion and Violence in Mental Health Settings (Hallett et al., 2024).
Several evidence-based intervention models are available with multi-modal interventions designed to prevent and reduce aggressive behavior in psychiatric settings, well-known ones include: The Six Core Strategies (Huckshorn, 2004, 2006); Safewards (Bowers, 2014; Bowers et al., 2015, resources available at https://safewards.net); and a more recent model based on the Six Core Strategies is ReSTRAIN Yourself (Advancing Quality Alliance, 2023) including a toolkit for clinical settings. By offering open access to these models, organizations can readily make use of these available resources.
Next Steps
These resources are representative of several clinical care and training opportunities. Despite the presence of models for training, risk assessment, and multi-modal interventions to reduce aggression and violence in inpatient psychiatric settings, further research is needed to enhance the evidence base for preventing WPV in psychiatric settings.
Practical Tips From Peers
After presenting at APNA and ISPN in 2024, the team was excited to hear from peers about changes in practice. From that collective wisdom, three themes emerged: advocacy, connection, and integration. Advocacy: Many participants mentioned that they gained an understanding of policies, to pass information onto colleagues and discuss at staff venues is an important first step. Connection: Connection was voiced in terms of connecting with patients and connecting with leadership. Connection comes from being informed about TJC standards, regulations, policies, and awareness of management’s reaction and prioritization of procedures. Integration: Integration of safety in all aspects of nursing, from nursing curriculum that learners are exposed to at the beginning of their careers, to clinical partners, and making safety and nourishing places of work a priority. Instilling these values in training, recognizing vulnerabilities, and asking how decisions will impact staff safety and well-being are crucial.
Conclusions
The multifaceted problem of WPV significantly erodes safety in healthcare, detrimentally affecting PMH nursing. When minimized, poorly managed, or inadequately prioritized legislatively, WPV reflects a form of institutional betrayal (Brewer, 2021). Nurse leaders, administrators, educators, and policy advocates must engage in wide-ranging efforts described in this paper to protect the nursing workforce. These recommendations work as a platform of advocacy, connection, and integration. Advocacy is grounded in organizational policies and procedures supported by state and federal legislation and encourages organizational involvement and belonging. The connection between the efforts of local initiatives depends on standardized policies, procedures, reporting systems, processes, and training. Universal quality standards empower nurses to design and evaluate initiatives. Empowerment creates a culture of approachability and builds organizational trust (Spencer et al., 2023), consistent with a psychologically safe and supportive workplace, encouraging brave and courageous spaces (Andrews, 2020). Integration of safety in nursing curriculum promotes its importance and cultivates the commitment to prioritize safety and a nourishing place of work. This is an opportunity to see safety as a shared and professional value ingrained in all that PMH nursing does and is.
Footnotes
Author Contributions
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.