
Abstract
Background:
Adolescent self-injurious behaviors (SIBs) present a global public health concern. Nurses, as frontline caregivers, play a crucial role in managing these cases, where their perceptions influence care quality. However, qualitative research deeply exploring these perceptions, particularly in the Zanjan, Iran context, remains scarce.
Aims:
To explore the perceptions and experiences of Zanjan nurses caring for adolescents with SIB.
Methods:
A qualitative content analysis study. Twelve nurses from general and psychiatric hospitals in Zanjan were purposively sampled. Data from in-depth, semi-structured interviews in Farsi were analyzed using the Graneheim and Lundman approach with MAXQDA software.
Results:
Analysis of the data generated 449 initial codes, from which three main categories emerged: (1) Conceptualizing Self-Harm: A Spectrum from Distress to Crisis, encompassing subthemes of persistent mental rumination, perceived precipitating factors, and profound emotional impact; (2) Systemic and Clinical Challenges in Care Delivery, comprising subthemes of organizational barriers, care complexities, and limitations in available treatments; and (3) Emotional and Cognitive Responses to the Adolescent, including subthemes of attributions about the person, perceptions of psychological suffering, and recognition of familial struggles.
Conclusion:
Nurses’ perceptions ranged from empathy to frustration. Notably, they often conceptualized non-suicidal self-injury and suicidal behaviors as interconnected expressions of distress rather than distinct phenomena. The findings highlight an urgent need for specialized nurse education, institutional support, and interdisciplinary collaboration to improve care. While insightful, the study’s focus on one Zanjan province and a small sample size suggests cautious interpretation and indicates a need for broader research.
Keywords
Introduction
Self-injurious behaviors (SIBs) among adolescents, encompassing both non-suicidal self-injury (NSSI) and suicidal behaviors, represent a significant global public health challenge (Ammerman et al., 2025). The critical distinction between these behaviors lies in the presence or absence of intent to die, a consensus highlighted in contemporary literature (Poudel et al., 2022). NSSI is defined as the direct, deliberate destruction of body tissue without suicidal intent, whereas suicidal self-injury involves self-harm with explicit intent to die. This study adopts this broad conceptualization of SIB, acknowledging the complex and often overlapping nature of these behaviors in clinical practice.
Adolescence (ages 10–19) is a vulnerable developmental period characterized by identity formation, emotional volatility, and heightened risk for psychopathology (Mastorci et al., 2024; de Neve-Enthoven et al., 2024). Within this group, SIB is prevalent and concerning. Global estimates indicate a lifetime prevalence of suicide attempts at approximately 6.0% and NSSI at 22.1% among adolescents, with trends showing a significant increase over the past decade (Haghish, 2025). The link between these behaviors is strong, with a substantial majority of adolescents who attempt suicide also reporting a history of NSSI, positioning NSSI as a major risk factor for subsequent suicidal behavior (Ammerman et al., 2025). Some studies in Iran report adolescent self-injury prevalence rates between 13% and 24.4%, noting an upward trend in suicide attempts and mortality (Abbasi-Ghahramanloo et al., 2024; Izakian et al., 2018; Mokhtari et al., 2019). These behaviors carry severe long-term consequences for mental and physical health, educational attainment, and social functioning.
Nurses, as frontline caregivers, play a pivotal role in managing adolescents who engage in SIB. Their perceptions, attitudes, and emotional responses significantly shape the therapeutic environment, the quality of care delivered, and ultimately, patient outcomes (Happell et al., 2019; Ribeiro Coimbra & Noakes, 2022). However, the hospital setting itself can present challenges, and nurses’ psychological well-being and performance are influenced by their exposure to and experiences with such complex phenomena (Fu et al., 2020; Neto et al., 2023). Understanding nurses’ subjective experiences—their thoughts, feelings, and the meanings they attribute to caring for this population—is therefore crucial. This understanding can illuminate systemic barriers, identify training needs, and foster more empathetic and effective care models (Tan et al., 2020).
While quantitative studies and attitude scales provide valuable data, they often fail to capture the depth, nuance, and context of human experience (Jamieson et al., 2023; Kandel, 2020). A qualitative approach is particularly well suited to explore the intricate perceptions and lived experiences of nurses, aligning with the philosophical foundations of nursing that value holistic understanding, empathy, and context (Wong & Bressington, 2022). Despite the clear importance of this topic, a review of available literature reveals a significant gap: no prior qualitative study has specifically and comprehensively explored the perceptions and experiences of nurses caring for adolescents with SIB in the Zanjan context. To address this gap, this study aimed to explore the perceptions and experiences of nurses in Zanjan who care for adolescents exhibiting self-injurious behaviors.
Method
Study Design and Setting
A qualitative study using conventional content analysis was conducted from November 2023 to November 2024. This approach is suited to obtain a rich, direct description of a phenomenon from participants with firsthand experience (Renjith et al., 2021). The study was set in general and psychiatric hospitals in Zanjan, Iran.
Participants and Sampling
A purposive sampling strategy, followed by snowball sampling, was used to recruit registered nurses. Inclusion criteria were: (a) at least 1 year of clinical experience, (b) direct experience in caring for an adolescent (aged 10–19 years) exhibiting SIB in the past year, and (c) willingness to participate. Sampling continued until data saturation was achieved, with no new substantive codes emerging after the 12th interview. The final sample comprised 12 nurses.
This study was approved by the Ethics Committee of Zanjan University of Medical Sciences (with the code No. IR.ZUMS.REC.1402.152). Written informed consent was obtained from all participants prior to the interviews. Participants were assured of the confidentiality and anonymity of their data; all identifiable information was removed, and they are referred to by codes in this report. Participation was voluntary and without compensation. Acknowledging the potentially distressing nature of the interview topics, all participants were informed about accessible, free psychological support services available through the university’s counseling center and were provided with the relevant contact information.
Data Collection
Data were collected through in-depth, semi-structured, individual, face-to-face interviews. An interview guide was developed based on the study objectives and a review of relevant literature. The guide included core, open-ended questions such as: (1) “Please describe your experience of caring for an adolescent who engaged in self-injurious behavior.” (2) “What were the main challenges or difficulties you faced while providing this care?” (3) “How did this experience affect you personally and professionally?” and (4) “What were your thoughts and feelings towards the adolescent during care?”
The interview process was iterative. While the core questions guided all interviews, follow-up and probing questions (e.g., “Can you give an example?,” “How did that make you feel?,” “What do you mean by that?”) were used flexibly based on participants’ responses and the ongoing analysis of previous interviews. This allowed for the exploration of emerging themes in subsequent interviews.
All interviews were conducted in Farsi, the native language of both the interviewer and all participants, to ensure depth of expression and avoid misinterpretation. Interviews were held in a private, pre-agreed room within the participant’s hospital to ensure comfort and minimize interruptions. Each interview lasted between 45 and 75 min. With the participant’s permission, all interviews were audio-recorded digitally.
Immediately after each interview, the researcher wrote detailed field notes. These notes captured contextual observations, non-verbal cues (e.g., tone, pauses, emotional expressions), and initial reflective thoughts, which later aided in contextualizing the verbal data during analysis.
Within 48 hr, the audio recordings were transcribed verbatim into Farsi by the primary researcher to ensure accuracy and familiarity with the data. The transcripts were then reviewed against the audio files for corrections. This process resulted in 12 complete interview transcripts for analysis.
Researcher Characteristics and Reflexivity
Reflexivity was maintained throughout the research process to manage the potential influence of researchers’ presuppositions. The primary interviewer (M.S.) was a male Master’s nursing student with clinical experience and prior research on self-harm. Because of his close proximity to the nursing field, he was able to build rapport and gain a deeper understanding of the participants’ challenges and jargon. However, during frequent peer-debriefing sessions with the supervisory team, his preconceptions were continuously discussed and challenged to reduce potential bias. Male and female professors with expertise in mental health and qualitative research made up the supervisors. They gave critical oversight during data collection and analysis, making sure that the codes and categories emerged from the data itself rather than the researchers’ assumptions. Also, during interviews, the researcher practiced bracketing by consciously setting aside his own beliefs to fully engage with the participants’ narratives.
Data Analysis
Concurrent data collection and analysis were performed using conventional qualitative content analysis as outlined by Graneheim and Lundman (2004). The analysis was an iterative process conducted primarily in the Farsi language to preserve the nuanced meaning of participants’ narratives.
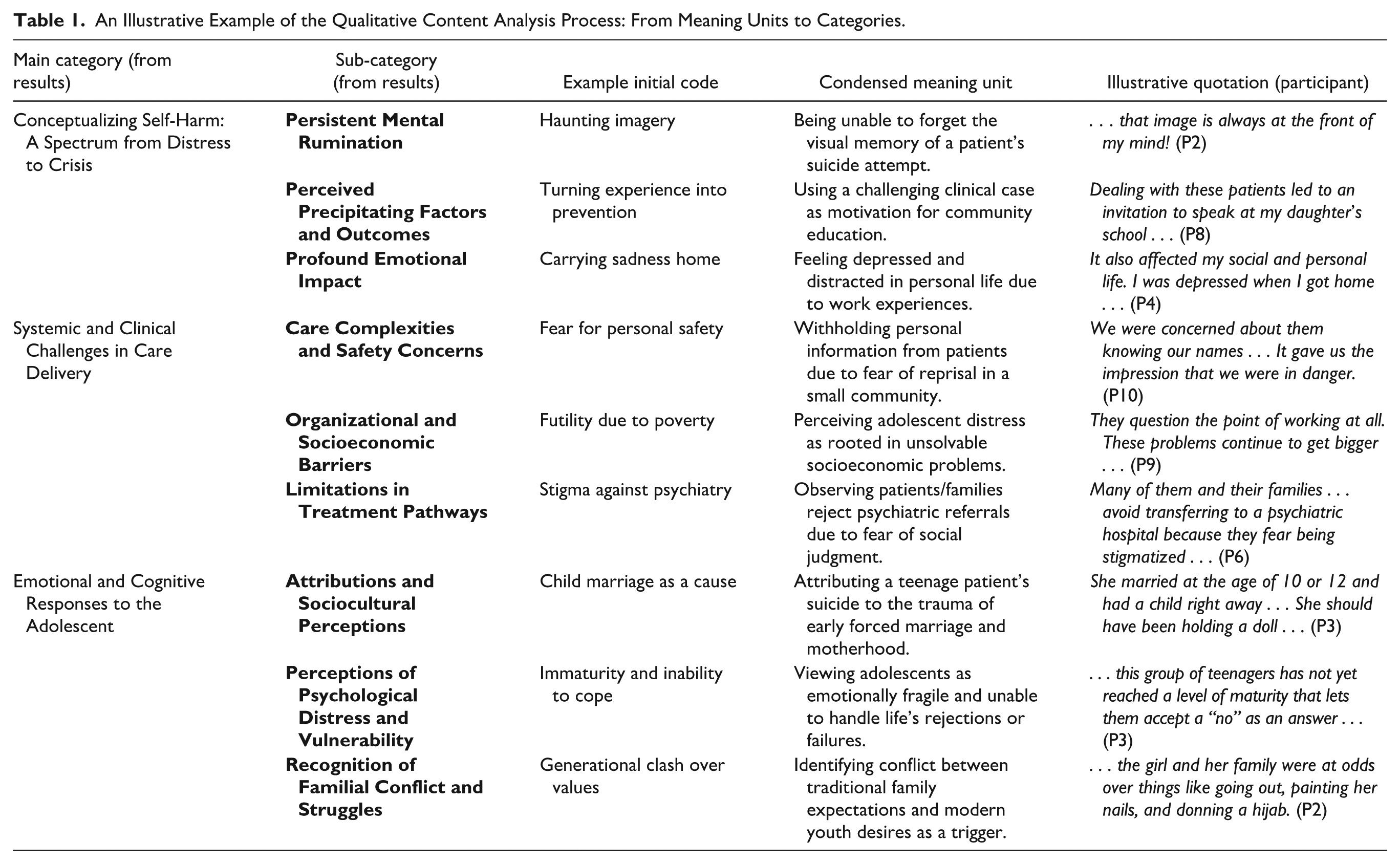
The analytical steps were as follows:
An Illustrative Example of the Qualitative Content Analysis Process: From Meaning Units to Categories.
Rigor (Trustworthiness)
The trustworthiness of this qualitative study was evaluated and ensured using Lincoln and Guba’s (1985) framework of credibility, dependability, confirmability, and transferability.
Credibility was established through multiple strategies: prolonged engagement (the study was conducted over 1 year to deeply understand the context), member checking (summaries of interviews and emerging themes were shared with participants for verification and feedback), and peer debriefing (the research team, including supervisors with qualitative expertise, regularly reviewed and challenged the coding process and interpretations during analysis sessions).
Dependability was achieved by maintaining an audit trail that documented all analytical decisions, from initial codes to final categories. Furthermore, an external audit was conducted where two independent qualitative research experts reviewed a sample of transcripts, codes, and the category structure to verify the consistency and logic of the analysis.
Confirmability was sought to ensure findings were rooted in the data, not researcher bias. This was addressed through practicing reflexivity and bracketing (as detailed in the “Researcher Characteristics” section), the triangulation of analysts via peer debriefing, and the external audit mentioned above.
Transferability, rather than generalizability, is the goal in qualitative research. To enable readers to assess the applicability of findings to other contexts, we have provided thick descriptions of the participants, the research setting (Zanjan, Iran), and a detailed account of the data collection and analysis process throughout this methods section.
Results
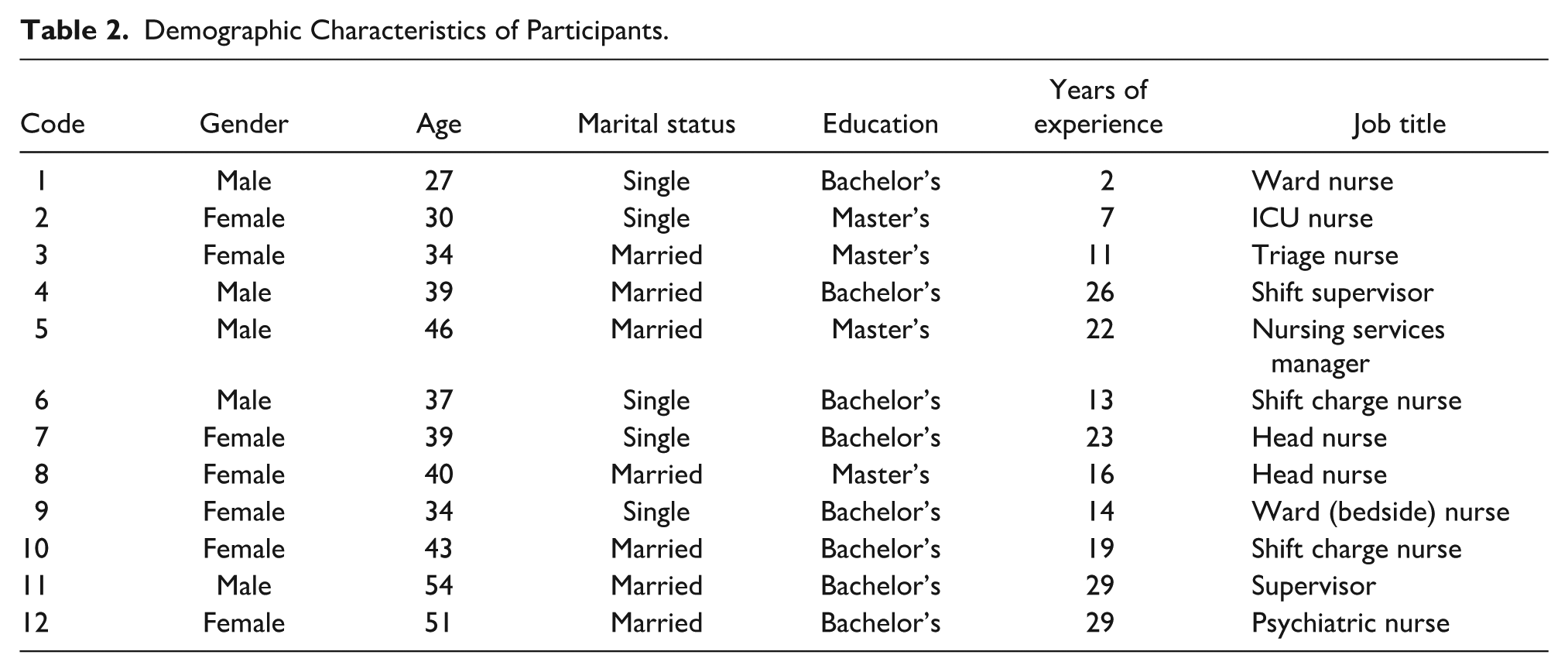
The study included 12 participants, comprising seven females and five males. Their ages ranged from 25 to 54 years. Three participants held a master’s degree, while the remainder had a bachelor’s degree. Detailed demographic characteristics are presented in Table 2.
Demographic Characteristics of Participants.
The analysis revealed that nurses’ perceptions and experiences were multifaceted, shaped by an interplay of their direct emotional encounters, the clinical and systemic contexts in which they worked, and their interpretations of the adolescents’ behaviors and backgrounds. The core findings were organized into three interconnected categories.
Following data analysis, 449 initial codes were generated. These codes were organized into nine subcategories and subsequently abstracted into three main categories: (1) Conceptualizing Self-Harm: A Spectrum from Distress to Crisis, (2) Systemic and Clinical Challenges in Care Delivery, and (3) Emotional and Cognitive Responses to the Adolescent.
Conceptualizing Self-Harm: A Spectrum From Distress to Crisis
This category captures how nurses conceptualized SIB among adolescents, ranging from NSSI to suicidal crises. It encompasses three subcategories: (1) Persistent Mental Rumination, (2) Perceived Precipitating Factors and Outcomes, and (3) Profound Emotional Impact.
Persistent Mental Rumination
This subcategory reflects the intrusive and prolonged psychological preoccupation nurses experienced following their care for adolescents who self-harm. Participants described how challenging these cases were and how they could dominate their thoughts long after the clinical encounter.
At times, certain experiences not only have a deep impact in terms of intensity, but they can also dominate a person’s thoughts for a prolonged period, especially the experience of the girl and her hanging; that image is always at the front of my mind! (Participant 2).
Perceived Precipitating Factors and Outcomes
Some nurses reframed adolescent self-harm not solely as a crisis, but as a potential turning point influenced by specific factors. They identified perceived triggers and, in some instances, opportunities for positive intervention that could lead to favorable outcomes, such as providing mentorship or developing specialized care approaches:
Dealing with these patients led to an invitation to speak at my daughter’s school, where I collaborated with teachers and gave advice. I have also found myself giving family, friends, and acquaintances similar advice because these behaviors are typical of students. (Participant 8)
Profound Emotional Impact
Caring for this population evoked strong emotional responses, predominantly sadness and pity, which nurses reported carrying beyond the workplace into their personal and social lives:
It also affected my social and personal life. I was depressed when I got home and found it hard to focus both at home and at work because my mind was overloaded. I found myself stunned by the experience, and I unintentionally passed on those negative feelings to my family. (Participant 4)
Systemic and Clinical Challenges in Care Delivery
This category encompasses the structural, organizational, and clinical barriers that nurses identified as impeding effective care for adolescents who self-harm. It consists of three subcategories: (1) Care Complexities and Safety Concerns, (2) Organizational and Socioeconomic Barriers, and (3) Limitations in Treatment Pathways.
Care Complexities and Safety Concerns
Nurses described significant challenges in maintaining a safe therapeutic environment, often reporting feelings of personal fear and insecurity. These concerns were amplified in close-knit community settings where anonymity was difficult to maintain:
Another issue we faced was that we didn’t share our names with the patients. This lack of etiquette felt challenging, as we were concerned about them knowing our names. We were more afraid of bad things happening to us because we lived in a small town. It gave us the impression that we were in danger. (Participant 10)
Organizational and Socioeconomic Barriers
Participants highlighted how broader systemic issues, including inadequate organizational support and deep-rooted socioeconomic inequalities, created fundamental obstacles to prevention and care. They perceived these factors as key drivers of distress among adolescents. Participant 9, while pointing to the juice provided by the interviewer to refresh him during the session, stated:
Look, I’m working here right now to make enough money to buy this juice, and we’re in a good enough spot financially that I can go to school. My parents support my education, but a lot of parents hold their kids back from pursuing their goals at school. Kids are dealing with complicated problems and they’re at a crossroads. Some of them start to wonder what the point of working even is. These problems can snowball and push a kid to a breaking point. I’ve seen it firsthand; one boy set himself on fire. He never went to the hospital—many kids don’t seek help at all.
Limitations in Treatment Pathways
A critical barrier identified was the fragmentation and incompleteness of treatment. Nurses pointed to structural deficiencies within the health care system and pervasive social stigma associated with mental illness, which together led many adolescents and families to disengage from essential psychiatric care:
I believe that this group of patients often ends up with incomplete treatment. There is room for improvement in this area. Many of them and their families come to the conclusion that they should avoid transferring to a psychiatric hospital because they fear being stigmatized as mentally ill. They tend to reject the idea of needing psychiatric help. Of course, we must acknowledge that this is Zanjan, and the circumstances are unique . . . (Participant 6)
Emotional and Cognitive Responses to the Adolescent
This category captures the complex emotional reactions and cognitive appraisals that nurses formed toward adolescents who self-harm, as well as their perceptions of the familial context. It comprises three subcategories: (1) Attributions and Sociocultural Perceptions, (2) Perceptions of Psychological Distress and Vulnerability, and (3) Recognition of Familial Conflict and Struggles.
Attributions and Sociocultural Perceptions
Nurses often made attributions about the causes of self-harm, linking them to specific sociocultural and gender-related factors. Some participants highlighted early marriage and motherhood as profound stressors uniquely affecting female adolescents in their context:
One of the women in our ward was born in 2005 and has a child who is eight years old! She died by suicide. It is evident that she married at the age of 10 or 12 and had a child right away. What is her knowledge of childbearing? What does she know about having a child? She should have been holding a doll by now, but she didn’t have time for this! (Participant 3) There was a girl who they wanted to force into pregnancy for her husband, and she had taken a rice pill and unfortunately passed away. (Participant 1)
Perceptions of Psychological Distress and Vulnerability
Adolescents who self-harmed were frequently perceived by nurses as being in a state of significant psychological distress and possessing a fragile mental state. Nurses described them as emotionally immature and ill-equipped to cope with life’s setbacks, which was sometimes attributed to a lack of prior adversity:
I sometimes believe that this group of teenagers has not yet reached a level of maturity that lets them accept a “no” as an answer, especially when it comes to emotional relationships. They may act drastically after hearing those words. Also, some people from wealthy backgrounds have never really grasped what life is all about. When faced with setbacks—like failing an entrance exam—they turn to self-harm or even suicide because they are accustomed to quickly getting what they want. They now navigate adolescence and adulthood with little hardship or difficulties. (Participant 3)
Recognition of Familial Conflict and Struggles
Nurses consistently identified intense family conflict, often arising from clashes between traditional values and modern youth norms, as a major contributing factor to adolescent self-harm. These conflicts typically centered around autonomy, behavior, and appearance:
About two months ago, a 16-year-old girl who was a patient in our ward [died by suicide] because of a number of problems that we subsequently discovered. A member of the kitchen crew who was acquainted with the girl and her family mentioned that the girl and her family were at odds over things like going out, painting her nails, and donning a hijab. (Participant 2)
Discussion
This qualitative study explored the perceptions and experiences of Zanjan nurses caring for adolescents with SIB. The analysis yielded three core themes that reflect a complex interplay between nurses’ personal responses and systemic constraints: (1) conceptualizing self-harm on a spectrum from distress to crisis, (2) navigating systemic and clinical challenges, and (3) managing emotional and cognitive labor. A key, cross-cutting finding was that nurses’ narratives often did not distinguish clearly between NSSI and suicidal behavior, instead perceiving them as interconnected expressions of profound adolescent crisis. This observation addresses a primary concern raised in the review regarding the need to clarify the relationship between these constructs in the data. The following discussion interprets these findings in light of the literature, emphasizes their implications for health equity and practice, and acknowledges the study’s limitations.
The first theme revealed that nurses conceptualize adolescent SIB not as a discrete act, but as a spectrum ranging from non-suicidal distress to acute suicidal crisis. Participants’ descriptions frequently intertwined self-harm with suicide, suggesting a clinical reality where these behaviors are perceived as fluid and related. This aligns with epidemiological evidence of their high co-occurrence. Within this spectrum, nurses described experiences of persistent mental rumination, where cases occupied their thoughts long after clinical encounters, leading to a profound emotional impact. These findings resonate with studies where nurses report significant anxiety, helplessness, and emotional burden in similar contexts (Leddie et al., 2022; Li et al., 2023). Notably, some nurses reframed these challenges by identifying perceived precipitating factors and potential for positive outcomes, finding opportunities for mentorship and community education. This adaptive coping mechanism, which can serve as a buffer against burnout, reflects a finding reported in a qualitative study of community nurses, where engaging in preventive education and advocacy provided a sense of purpose and mitigated feelings of helplessness when working with adolescents who self-harm (Leddie et al., 2022).
The second theme underscores the formidable systemic barriers that exacerbate the care crisis and directly relates to issues of health equity. Nurses faced immediate care complexities and safety concerns, often feeling vulnerable in close-knit communities. More critically, they identified deep-rooted organizational and socioeconomic barriers, alongside fragmented treatment pathways marked by stigma and resource limitations. These systemic failures are critically mediated by the local Zanjan context. Participants explicitly linked adolescent vulnerability—particularly among females—to specific sociocultural determinants of health such as child marriage, gender inequality, and economic disparity. This places our findings squarely within a health equity framework, demonstrating how power structures and access to resources shape both the adolescents’ risks and the nurses’ capacity to provide care. The nurses’ reported feelings of being underprepared and lacking specific expertise are a critical finding that underscores a widespread educational gap. This sentiment strongly echoes the conclusions of studies reviewing training needs, which call for the development and implementation of structured, evidence-based educational programs to better equip nurses for this complex care specialty (Singh-Weldon et al., 2022).
The third theme captured the intense emotional and cognitive labor involved in this care, which at times led to judgmental attitudes. The significant emotional toll described by participants, consistent with literature on caregiver burnout (López-López et al., 2019), is a well-documented challenge. Research specifically on psychiatric nurses highlights similar experiences of psychological strain and identifies systemic factors, such as high workload and inadequate support, as key contributors to this distress (Li et al., 2023). Nurses formed attributions about the causes of SIB, often pinpointing familial conflict and sociocultural stressors, and held perceptions of adolescents as psychologically vulnerable and immature. This significant emotional burden appeared to manifest in some instances as moralistic interpretations of self-harm. The perception of self-harm as a moral failing, while potentially a psychological coping strategy for nurses’ own feelings of helplessness, represents a critical point for intervention, as such attitudes risk perpetuating stigma and damaging therapeutic alliances (Cadorna et al., 2024; Zhao et al., 2023). This underscores the necessity for training that fosters reflexive practice to identify and manage these countertransference reactions.
When viewed together, these three themes illustrate a cycle influenced by health inequities. Systemic failures (Theme 2) exacerbate adolescent distress and limit care options, which in turn intensifies the emotional labor and moral distress of nurses (Theme 3), who may then struggle to conceptualize the behavior beyond crisis (Theme 1). This cycle is particularly pronounced in contexts like Iran, where structural determinants such as gender inequality and economic disparity directly shape both patient vulnerability and health care delivery. Addressing SIB, therefore, requires moving beyond individual-level interventions to tackle these root causes.
In an environment where unique cultural and religious norms directly affect both adolescent experiences and nursing care, this study provides a context-rich understanding. While challenges like organizational barriers and burnout are global, our research illustrates their specific manifestations within Iran’s health care and social systems. To break the cycle of stigma, burnout, and inadequate care, our findings highlight the imperative for specialized education programs that address the spectrum of SIB, structured institutional support for nurses’ well-being, and robust interdisciplinary, multi-sectoral collaboration that tackles the underlying social determinants of health. Future research should employ designs that can further disentangle care experiences for NSSI versus suicidal behavior, and quantitative studies are needed to measure the impact of targeted interventions on both nurse and patient outcomes.
Limitations and Recommendations
This study has several limitations that should be considered when interpreting the findings. First, the qualitative design and small, purposive sample of 12 nurses from Zanjan province, mean that the findings are rich in context but are not statistically generalizable to the broader population of all nurses in Zanjan province or other cultural settings. Second, despite employing strategies like reflexivity and peer debriefing to enhance trustworthiness, the interpretive nature of qualitative research entails an inherent degree of researcher subjectivity. Third, as the study aimed to explore broad perceptions, the interview guide did not explicitly differentiate between NSSI and suicidal behavior during questioning. Consequently, participants’ narratives often conflated these phenomena, which, while an important finding in itself regarding clinicians’ holistic perception of risk, means the data cannot delineate specific care experiences unique to each behavioral type. Finally, while demographic data were collected, the analysis did not deeply explore how specific religious or cultural beliefs of individual nurses may have shaped their responses, which could be a fruitful avenue for deeper inquiry.
These limitations suggest valuable directions for future research. Future qualitative studies could employ a more targeted interview approach to distinctly capture nurses’ experiences with NSSI versus suicidal crises. Quantitative surveys with larger, representative samples are needed to measure the prevalence of the attitudes and challenges identified here. Investigating how specific cultural, religious, or institutional factors moderate these perceptions and experiences would add significant depth. Finally, intervention studies are crucial to develop and test the efficacy of specialized training programs and support systems for nurses caring for this vulnerable adolescent population.
Conclusion
This qualitative study provides valuable, context-specific insights into the perceptions and experiences of nurses in Zanjan caring for adolescents with SIB. A key finding is that nurses often conceptualize these behaviors on a broad spectrum from non-suicidal distress to suicidal crisis, a perception that shapes their emotional and clinical responses. The results reveal a dual reality: significant emotional burden and systemic challenges—including inadequate training, organizational barriers, and sociocultural complexities like gender inequality—coexist with opportunities for professional growth and positive intervention.
The study underscores an urgent need for multifaceted strategies. At the practitioner level, specialized education and robust support systems are essential to equip nurses and safeguard their well-being. At the systemic level, effective prevention and care require dedicated mental health resources and genuine intersectoral collaboration across health care, education, and social services to address the root causes of adolescent distress. Ultimately, addressing this complex public health issue demands both empowering frontline nurses and enacting the structural changes necessary to support them in providing compassionate, effective care.
Relevance for Clinical Practice
This study offers vital information for nursing educators, health care administrators, and policymakers. To address the psychological strain identified and to move toward more equitable care, targeted interventions are needed. The results underscore the critical need for specialized, culturally sensitive training programs that equip nurses with advanced clinical skills and coping mechanisms for adolescent mental health care, including competencies in distinguishing between and managing non-suicidal self-injury and suicidal behavior. Health care organizations should establish structured support systems, such as clinical supervision and peer support groups, to mitigate long-term psychological impact on staff. Finally, to tackle the systemic and socioeconomic barriers identified, the study emphasizes the necessity for robust interdisciplinary collaboration and increased allocation of mental health resources to ensure complete, non-stigmatizing care for this vulnerable population.
Footnotes
Acknowledgements
We sincerely thank all the nurse participants who shared their experiences for this study. This work is part of a research project approved and supported by Zanjan University of Medical Sciences.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research and Technology Deputy of Zanjan University of Medical Sciences, Zanjan, Iran (Grant Number: A-11-86-28).
Ethical Considerations
This study was approved by the Ethics Committee of Zanjan University of Medical Sciences (with the code No. IR.ZUMS.REC.1402.152). Written informed consent was obtained from all participants prior to the interviews. Participants were assured of the confidentiality and anonymity of their data; all identifiable information was removed, and they are referred to by codes in this report.
Consent to Participate
Participation was voluntary and without compensation. Acknowledging the potentially distressing nature of the interview topics, all participants were informed about accessible, free psychological support services available through the university’s counseling center and were provided with the relevant contact information.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to the sensitive nature of the qualitative data and to protect participant confidentiality, but may be available from the corresponding author on reasonable request and with appropriate ethical approvals.