
Abstract
Objectives:
Tobacco use increases morbidity and mortality among its users. The rate of tobacco use is declining in the general adult population yet is two to three times higher for those experiencing mental health disorders, specifically those with serious mental illness (SMI). Psychiatric mental health nurse practitioners (PMHNPs) are well-positioned to treat tobacco use in patients with SMI, yet tobacco training during nursing education, both in amount of time spent and content delivered, is not well understood and can leave PMHNPs ill-prepared to intervene.
Methods:
A cross-sectional descriptive survey design was used to assess PMHNP programs nationwide to determine where tobacco treatment is located in the curriculum, the amount of time spent on tobacco treatment throughout the program, and program directors’ general attitude and beliefs about the importance of tobacco treatment related to the scope of practice and impact.
Results:
Program directors or their representatives responded (N = 34) across all program types. Respondents reported either agreement or strong agreement with the importance of tobacco treatment in PMHNP programs. Most spent less than 1 hour or between 1 and 3 hours on tobacco treatment, primarily in psychiatric assessment and psychopharmacology courses. Most agreed or strongly agreed that this was within the scope of practice, yet agreement was less when asked about impact on outcomes.
Conclusion:
PMHNP programs have an opportunity to improve perspectives on the impact psychiatric nurse practitioners can have on tobacco treatment outcomes and integrate curricular strategies to robustly integrate tobacco competencies.
Keywords
Introduction
More than 16 million Americans suffer from tobacco-related diseases, and almost half a million die annually from tobacco-associated sequelae (National Institute on Drug Abuse, 2023). The overall use of tobacco in the adult population is just under 20% and has been steadily declining over the past several years. Yet, almost 35% of people with mental health disorders use tobacco. In fact, the rate of tobacco-related morbidity and mortality, among patients with serious mental illness (SMI), is considerably higher than in the general population (Asharani et al., 2020; Evins et al., 2017; Sharma et al., 2016; Streck et al., 2024). For patients with a diagnosis of schizophrenia, tobacco use rates vary between 70% and 85%, and for people with bipolar disorder, they vary between 50% and 70% (NIDA, 2023). These patients also experience challenges with sustained abstinence and are less likely to be successful with a quit attempt. Further complicating the issue, more than 2.5 million adults living with SMI live below the poverty line, creating a powerful intersection of tobacco disparities (NIDA, 2023). In addition, racism and racial discrimination further complicate the issue of tobacco treatment and SMI, given the existing inequities in the provision of mental health care (National Alliance on Mental Illness [NAMI], 2021). There is a critical need to address tobacco use in people with SMI due to higher levels of use, reduced percentage of successful quits, and persistent disparities that are made worse by tobacco use.
Tobacco treatment can occur in any setting; however, given the number of people with SMI who use tobacco, the likelihood of psychiatric providers treating patients with these disorders is high. According to Cai et al. (2022), between 2011 and 2019, Medicare recipients experienced a 29% reduction in psychiatrist visits and a 113% increase in visits with a Psychiatric Mental Health Nurse Practitioner (PMHNP). As a rapidly growing group of providers, PMHNPs are well-positioned to be a part of addressing tobacco treatment and disparities. Although not well understood, barriers to tobacco treatment by nurse practitioners exist (Westmass et al., 2023). Limited data suggest that among the barriers reported are lack of knowledge, confidence, self-efficacy, resources, social context, and competing treatment priorities (Huddlestone et al., 2022; Westmass et al., 2023).
The need for well-prepared providers is essential to address tobacco use disorders (TUDs) and improve disparities in care, specifically for those with SMI. In 2020, the American Psychiatric Nurses Association (APNA, 2020a; Essenmacher et al. 2022) released a revised position statement and tobacco competencies recommending a central role in tobacco treatment for PMH nurses. However, there is a paucity of data available that describe how PMHNP educational programs integrate tobacco treatment. Efforts to integrate this information into PMHNP programs have been inconsistent and given lower priority (Boonstra & Spoelstra, 2024). The purpose of this research brief is to describe tobacco treatment education provided in PMHNP educational programs across the United States.
Method
Design, Sample, and Ethics
A cross-sectional survey design was used to query existing PMHNP program directors or their representatives related to tobacco treatment in their programs of study. A national publicly available listserv of PMHNP programs and director contacts available through the APNA website was used to recruit program directors from across the United States. Respondents were emailed with an initial opportunity to participate with two reminder emails sent over the course of a 1-month period. This study was approved by the Institutional Review Board at Rush University.
Data Collection Measures
A structured seven-item survey was created using the RedCap survey software to gather information related to the program type offered, time spent on tobacco treatment, and the location of tobacco treatment content in courses and clinical. In addition, questions sought program director perspectives on the importance, scope, impact, and value of educating PMHNPs on tobacco treatment. The measure was created by the research team, as no existing measure was available. The study was exploratory in nature, and the questions were designed to gather information to reflect the identified problem. Three research team members reviewed the items for face validity to ensure that the items reflected the information sought. Likert-type scale data were collected (1 = strongly disagree, 5 = strongly agree) on items related to importance, scope, and impact on practice. All questions were positively worded, with higher scores indicating stronger agreement with statements.
Data Analysis
Stata 18 was used to analyze the data. Exploratory data analyses were used to gain a greater understanding of the concept of interest, identify data patterns, and assess trends. Patterns in program type related to time spent on tobacco treatment were explored. The location of tobacco treatment content related to program type was also explored. General trends were analyzed with regard to perceptions of tobacco treatment education importance, scope of practice, and impact. In addition, because exploratory data analyses were conducted, both analysis of variance (ANOVA) and predictive statistical models were subsequently applied to the dataset to examine group differences and identify potential predictive relationships.
Results
Demographics
Invitations were sent to 174 programs with a total of 34 complete responses. Representatives from Master of Science in Nursing (MSN), Post-Master of Science in Nursing (P-MSN), and Doctor of Nursing Practice (DNP) PMHNP programs responded to the survey (N = 34). Several respondents offered more than one program type (see Table 1). The largest group of respondents (n = 9) came from programs that offered all three program types: MSN, P-MSN, and DNP, followed by DNP only (n = 5) and P-MSN and DNP (n = 6).
Demographic Characteristics.
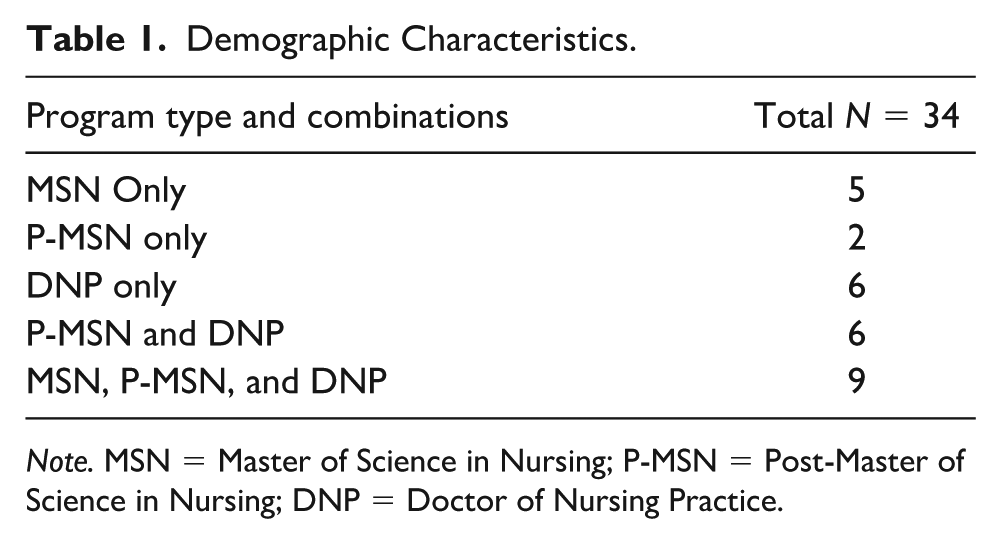
Note. MSN = Master of Science in Nursing; P-MSN = Post-Master of Science in Nursing; DNP = Doctor of Nursing Practice.
Across all programs, the importance of tobacco treatment was reported as 4.32, which indicates that most respondents either agree or strongly agree that tobacco treatment content in PMHNP programs is important with no significant difference based on program type (F = 0.84, p = .513). However, most programs spent less than 1 hour (n = 15) or 1 to 3 hours (n = 17) on tobacco content throughout the course of PMHNP training, and just over 70% of programs say they offered tobacco content specifically outside of other substance use disorder content. Although the type of program offered and agreement with importance were not significant predictors of time spent on tobacco treatment (p = .436), departments that offered all types of PMHNP programs were more likely to report a greater amount of time spent on tobacco treatment throughout the curriculum (1–3 hours), and programs that offered P-MSN only were more likely to report less time spent on tobacco treatment (less than 1 hour).
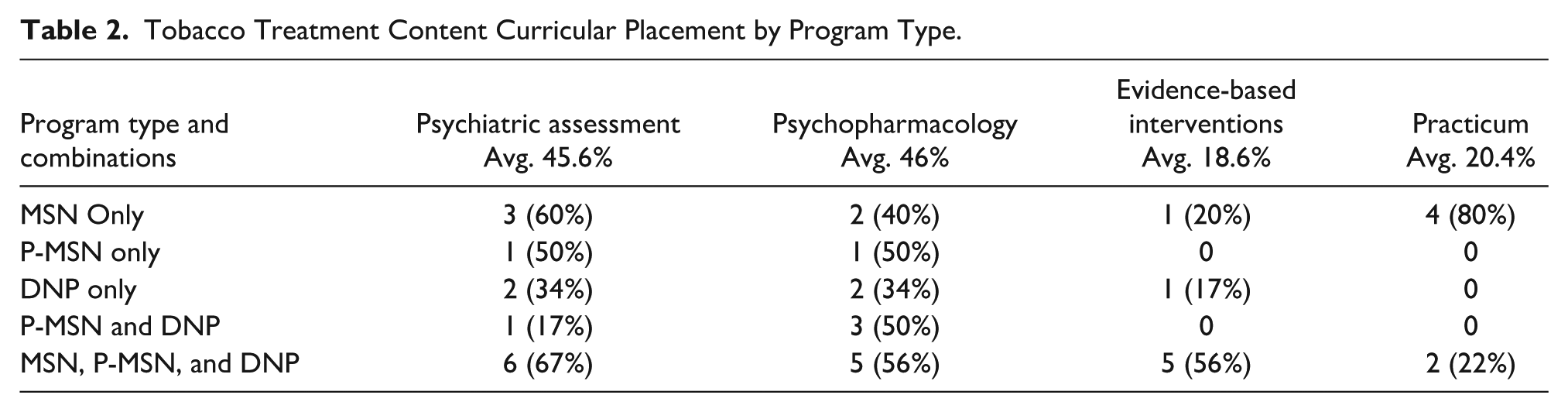
Most programs reported that tobacco treatment content was located primarily in psychopharmacology (46%) and psychiatric assessment (45.6%) courses (Table 2). A small percentage of programs indicated that tobacco treatment was included in practicum (20.4%) and evidence-based intervention (18.5%) courses.
Tobacco Treatment Content Curricular Placement by Program Type.
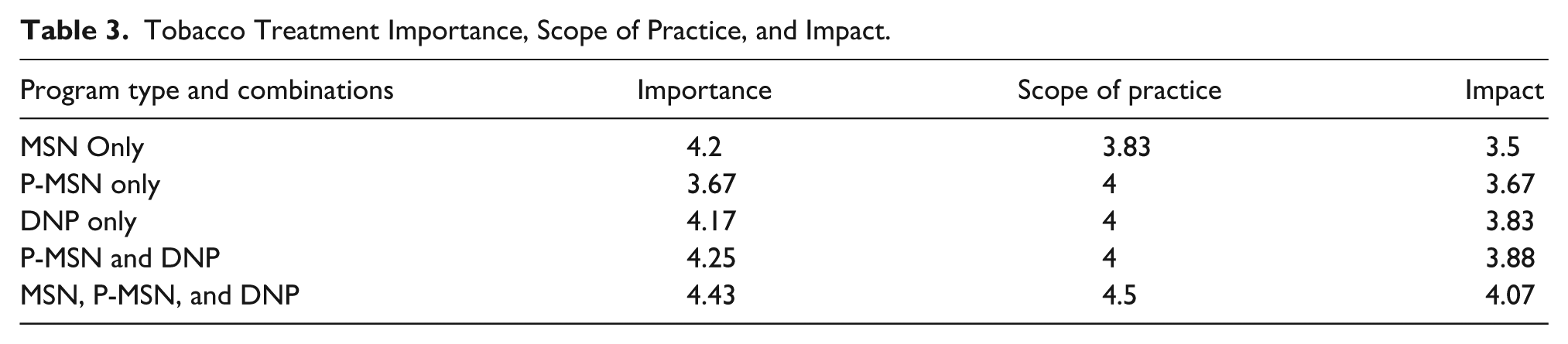
Program representatives were also asked to describe perceptions of the importance of tobacco treatment, whether tobacco treatment was within the PMHNP scope of practice, and the impact PMHNPs have on tobacco treatment outcomes (Table 3). Overall, when DNP programs were offered either independently or in combination with MSN and/or P-MSN programs, the importance of tobacco treatment scored higher as well as on the scope of practice and potential impact of PMHNP on treatment outcomes. The importance of tobacco treatment received the greatest agreement overall (4.14), followed by agreement that treatment was within the PMHNP scope of practice (4.06). However, the average rating by program directors on the impact of PMHNPs on tobacco treatment and outcomes was rated the lowest with an average of 3.79.
Tobacco Treatment Importance, Scope of Practice, and Impact.
Discussion
The results of this study support overall acceptance by PMHNP program directors of the importance of teaching TUD treatment to their students. Those directors also largely agree that treating this substance use disorder is within the scope of practice of a PMHNP. Perceptions of the impact their graduates can have on tobacco treatment and outcomes were less robust, which suggests there may be a disconnect somewhere on the continuum of training to practice. Research indicates that tailored and targeted tobacco training not only improves confidence in providers but also the intent to deliver tobacco treatment (Sheffer et al., 2021). Since these data reveal very little time spent on tobacco treatment in PMHNP programs, this begs the question of whether or not PMHNPs are prepared to deliver tobacco treatment. In addition, perceptions were reported that tobacco training in PMHNP programs has a less significant impact on outcomes, and this could be driving the degree of content inclusion and time spent on tobacco treatment in programs.
This discrepancy reveals an intention-action gap, which could indicate that program responses reflect the increasing attention paid in the literature to the impact of tobacco comorbidities in patients with SMI, as well as the 2020 release of the revised TUD position paper and competencies by a major professional organization for psychiatric mental health nurses (American Psychiatric Nurses Association [APNA], 2020b). However, the action needed to fully integrate training is lacking. Perceptions of impact are in alignment with nurse reports of personal ineffectiveness related to smoking cessation and negative attitudes about tobacco treatment (Boonstra & Spoelstra, 2024). In Rogers et al.’s (2018) exploration of perceptions of barriers to treating TUD, there was a mixed response to questions about whether TUD treatment was actually a mental health care responsibility. In addition, it is also often seen as a lifestyle modification rather than a medical treatment (Kleinman & Barnett, 2024).
Limitations
Several limitations were noted in the research. Although the survey was aimed at a broad audience, and the sample was representative of all program types, the sample was relatively small and unable to provide conclusive evidence on the state of tobacco treatment content in PMHNP programs in the United States. In addition, the number of P-MSN-only program responses was low (n = 2), which limits the ability to draw conclusions about this program type specifically, and conclusions may warrant further investigation.
Overall, 19.5% response rate was achieved, which is consistent with survey research (Dillman et al., 2014). The location of respondents within the United States is unknown, and therefore, conclusions cannot be drawn about region-specific implications. Non-experimental, cross-sectional research does not lend itself to determining causality. Programs willing to incorporate advanced and concentrated tobacco training compared with those who offer standard training could be studied to determine the impact on student outcomes and intent to prioritize tobacco treatment in practice.
Implications
Tobacco use is killing our patients with SMI. Beyond creating serious and exceptional harm to the people many psychiatric nurse practitioners treat, best practices for tobacco treatment are available. An academic approach to training PMHNPs in TUD treatment has not been fully realized and put into practice in many educational programs, despite the existence of clear guidance on necessary competencies from professional organizations. Peltier et al. (2025) describe integrating tobacco treatment into a family nurse practitioner program with noted improvements in knowledge, comfort, motivation, and confidence in providing information and helping people quit smoking. It follows, then, that improved TUD training in PMHNP education programs can improve these outcomes as well as the sense of priority rather than continuing to place treatment as secondary for an issue that is clearly a major predictor of morbidity and mortality among those with SMI.
As a start, all graduating PMHNPs should be aware that evidence shows that their patients who use tobacco and have schizophrenia or bipolar disorder who are maintained on varenicline beyond the standard 12-week course of varenicline are much more likely to avoid relapse (Evins et al., 2017). This could be included in psychopharmacology courses during the discussion of medications to treat substance use disorders. They should be prepared to use the “5 As” as soon as they start practicing. This evidence-based approach consists of five steps: (1) ask about the patient’s tobacco use, (2) advise the patient to quit, (3) assess their willingness for a quit attempt, (4) assist in a quit attempt (with counseling and/or medication), and (5) arrange for follow-up (Agency for Healthcare Research and Quality, n.d.). They should be as prepared to use the Fagerstrom test for Nicotine Dependence in assessing TUD as they are for using the Patient Health Questionnaire-9 item (PHQ-9) or Generalized Anxiety Disorder-7 item (GAD-7) for depression or anxiety (Sheikhattari et al., 2025). Brief motivational interviewing interventions can be used effectively to move patients toward willingness for a quit attempt as well as support conversations about accepting the use of pharmacotherapy as an effective component of tobacco treatment (Levounis et al., 2017). These basic components can be included in psychiatric assessment and intervention courses alongside content on assessment and interventions for other substance-use disorders. In addition, they should be ready to craft a treatment plan in collaboration with their patients who use tobacco as they would any collaborative effort to address a problem or diagnosis. The next logical steps would be to ensure the APNA tobacco competencies serve as an overarching outline to guide TUD curricular components, including broader systemic interventions and policy action.
Recommendations
A focus on the treatment of TUD in psychiatric as well as integrated health care settings has emerged in the literature by members of various mental health disciplines, along with the creation of academic and continuing education training programs to equip these clinicians to address the disorder (Peltier et al., 2025; Prochaska et al., 2009; Williams et al., 2020). Such efforts may provide guidance for the ongoing work of nurse practitioner programs to provide competency-based education in TUD treatment to reflect APNA calls to action, American Association of Colleges of Nursing (AACN) competency-based education, as well as the National Organization of Nurse Practitioner Faculties (NONPF) competencies. Including tobacco competencies in pre-licensure education would also improve the likelihood that such competencies would be reflected in post-graduation practice. Similarly, including TUD treatment content in evidence-based intervention and practicum courses in PMHNP programs, rather than only in the psychiatric assessment and psychopharmacology courses, as was more commonly reported by the program directors, would reinforce the necessity of incorporating the practices clinically, as persons with SMI are seen across the continuum of care. In addition, an assessment of faculty attitudes and confidence could be considered to determine whether programs that address TUD content effectively have a greater number of faculty who are comfortable presenting the content or who have specialized knowledge in this area.
Conclusions
Lifespan is shorter for those with SMI (Colton & Manderscheid, 2006), and this is exacerbated by the comorbidity of TUD. In people with SMI, the strongest predictor of mortality, after age, is tobacco smoking, with a dose-related effect (Dickerson et al., 2021). People with SMI often have fewer resources to support quit attempts, such as social support and access to health care. The high incidence and lethality of tobacco use in this population support a call to action for providers treating people with mental illness and TUD and for educators of these providers.
Ensuring that all graduating nurse practitioners, especially PMHNPs, possess the competencies in tobacco dependence treatment laid out by the APNA will, no doubt, require some curriculum revision in nurse practitioner education. It will be well worth it if, as a discipline, psychiatric nurse practitioners can help move the needle on tobacco use and resultant morbidity and mortality in the people for whom we care. We propose that the steady growth of PMHNPs treating people with SMI makes curricular change an essential component of improving patient outcomes.
Footnotes
Acknowledgements
Not applicable.
Author Contribution Statement
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Rush University College of Nursing Office of Nursing Research and Scholarship: PhD, DNP Collaboration Grant.
Ethical Approval
The ethical approval was obtained from the Rush University Institutional Review Board.