
Abstract
Objective:
Suicide is a significant public health crisis in Canada, claiming approximately 4,500 lives annually. Despite decades of localized efforts, Canada remains one of the few G7 nations without a national suicide prevention strategy until 2024. This discussion paper examines Canada’s newly launched National Suicide Prevention Action Plan (2024–2027) and provides a critique of its structural framework, collaborative mechanisms, and evidence-based approaches.
Methods:
The article outlines a brief historical overview of Canada’s development of the current National Suicide Prevention Action Plan. A review of the Plan’s four strategic pillars, specifically, data and monitoring, research and evaluation, support and services, and governance, reveals both progress and ongoing issues. The plan’s equity-focused approach, multisectoral collaboration, and integration of Indigenous perspectives mark notable achievements, whereas data infrastructure gaps, funding uncertainties, and implementation dependencies present ongoing concerns.
Results:
Drawing on successful Canadian and international policy models and provincial innovations, this paper provides concrete recommendations to strengthen implementation and ensure sustained impact on Canada’s persistent suicide rates.
Conclusion:
Canada’s National Suicide Prevention Action Plan (2024–2027) constitutes a significant federal milestone in addressing a persistent public health concern. However, to further enhance the current plan, specific details on evaluation, assessments, and outcome measures should be included. In addition, collaboration with provincial and territorial organizations that are currently involved in suicide prevention initiatives would strengthen the plan. More tailored approaches to support diverse groups within Canada and Indigenous populations are additional suggested improvements.
Keywords
Introduction
Suicide is one of the most urgent and complex public health challenges in society. In Canada, approximately 4,500 people die by suicide each year, roughly 12 per day, making it the ninth leading cause of death nationally and the second leading cause among those aged 15–34 (Public Health Agency of Canada, n.d.). Despite sustained advocacy and intervention efforts, Canada’s national suicide rate has changed little since 2006, underscoring the need for coordinated evidence-based policy responses that transcend fragmented regional approaches (Navaneelan, 2012).
The launch of Canada’s first National Suicide Prevention Action Plan in 2024 marks a major shift in federal public health policy. As one of the last G7 nations to formalize a national strategy, Canada’s plan reflects growing recognition that suicide prevention demands coordination across governments, sectors, and communities (Sinyor et al., 2014). This delay has also allowed policymakers to learn from international precedents and incorporate best practices, including trauma-informed care, distinction-based approaches for Indigenous populations, and innovative crisis-intervention technologies.
This discussion paper provides a brief historical overview of suicide prevention policy and advocacy at the federal level in Canada and a summary of the National Suicide Prevention Action Plan (2024–2027), examining its strategic framework, implementation, and potential impacts. The paper provides critiques and recommendations for improvements and cross-national learning, focusing on the implications for suicide prevention policy in Canada.
Historical Context of Development
Before discussing the National Suicide Prevention Action Plan, it is important to understand its historical context. There are a variety of reasons that contributed to the delay in its development, specifically jurisdictional issues and fragmentation, political hesitation, and a lack of dedicated funding. In Canada, health services are primarily a provincial/territorial responsibility, making federal leadership difficult without perceived overreach, leading to frameworks rather than mandates. In addition, efforts were scattered across different levels of government and organizations, and it was a challenge to develop a unified vision and coordination. From a political perspective, previous federal governments focused on a framework rather than a legally binding strategy and took few concrete actions, despite parliamentary support for a strategy (Eggertson & Patrick, 2016; Jones, 2016; Senate of Canada, 2006). In addition, initiatives often lacked the necessary financial commitment to implement effective, broad-reaching strategies, as noted by critics.
Canada first began to address suicide as a public health concern with recommendations developed by the Mental Health Commission of Canada in 2009 and 2012, which focused on improving the mental health and well-being of all Canadians (Mental Health Commission of Canada, 2012). Prior to these recommendations, many researchers, organizations, and individuals had advocated for a national approach to suicide prevention. The Canadian Association for Suicide Prevention (CASP, 2009) published a specific blueprint in 2004 and updated it in 2009 with clear direction and a coordinated campaign, which they brought before the Senate. Furthermore, the World Health Organization (WHO)’s (2014) Preventing Suicide: A Global Imperative report also contributed to the development of a framework in Canada. The Suicide Prevention Framework was created in 2016 and had three main objectives: “reduce stigma and raise public awareness, connect Canadians, information and resources, and accelerate the use of research and innovation in suicide prevention” (Public Health Agency of Canada, 2016). While the framework was established to align efforts, a 2023 Senate report found it has had no measurable effect on Canada’s overall suicide rate since 2016, prompting recommendations for improvement (Senate of Canada, 2023).
Provincial and Territorial Context
Before examining the national plan’s strategic pillars, understanding Canada’s existing provincial landscape is essential for assessing what federal coordination can realistically achieve. Provincial suicide prevention strategies differ substantially in approach, resources, and maturity, revealing both promising models and significant gaps that the national plan must address.
Saskatchewan’s “Pillars for Life” represents one of Canada’s most comprehensive provincial approaches, incorporating media guidelines for responsible suicide reporting, safe medication disposal programs to reduce lethal means access, peer support networks, targeted awareness campaigns, and systematic frontline worker training (Government of Saskatchewan, 2020). The media guidelines component alone demonstrates how provinces can implement evidence-based interventions that the national plan references but does not mandate. Quebec has invested in regional suicide prevention centers (Centres de prévention du suicide) that provide 24/7 crisis support, postvention services, and community education, creating an integrated infrastructure that other provinces lack. British Columbia has pioneered the integration of primary care and mental health services through collaborative care models, reducing barriers between physical and mental health systems (Lukey et al., 2022). The territory of Nunavut has a suicide prevention strategy that features collaboration with relevant organizations and develops specific Action Plans. The Inuusivut Anninaqtuq (United for Life) is the most recent multi-year plan developed through broad consultation and sets concrete actions, including strengthening mental health supports in schools and expanding cultural and community wellness initiatives (Government of Nunavut, 2025).
Overview of the National Suicide Prevention Action Plan (2024–2027)
Scope and Vision
The National Suicide Prevention Action Plan is a 3-year commitment from 2024 to 2027, designed as an “evergreen” framework intended to evolve iteratively through ongoing stakeholder collaboration and evidence accumulation (Public Health Agency of Canada, 2024). This adaptive approach recognizes suicide as a multifactorial phenomenon and stresses the need for a flexible policy that can incorporate emerging research, technological innovations, and community feedback (Canadian Mental Health Association, 2024).
Rather than replace provincial, territorial, or Indigenous-led initiatives, the plan positions federal action as a complementary force that connects local efforts through shared resources, knowledge exchange, and coordinated strategy (Public Health Agency of Canada, 2024). Its vision of “fewer lives lost to suicide and communities supported in their wellbeing” (Public Health Agency of Canada, 2024, p. 3) captures a dual emphasis on mortality reduction and community wellness. This framing reflects a contemporary understanding that effective suicide prevention extends beyond crisis intervention to encompass upstream determinants of mental health and social connections (Zalsman et al., 2016).
Strategic Pillars
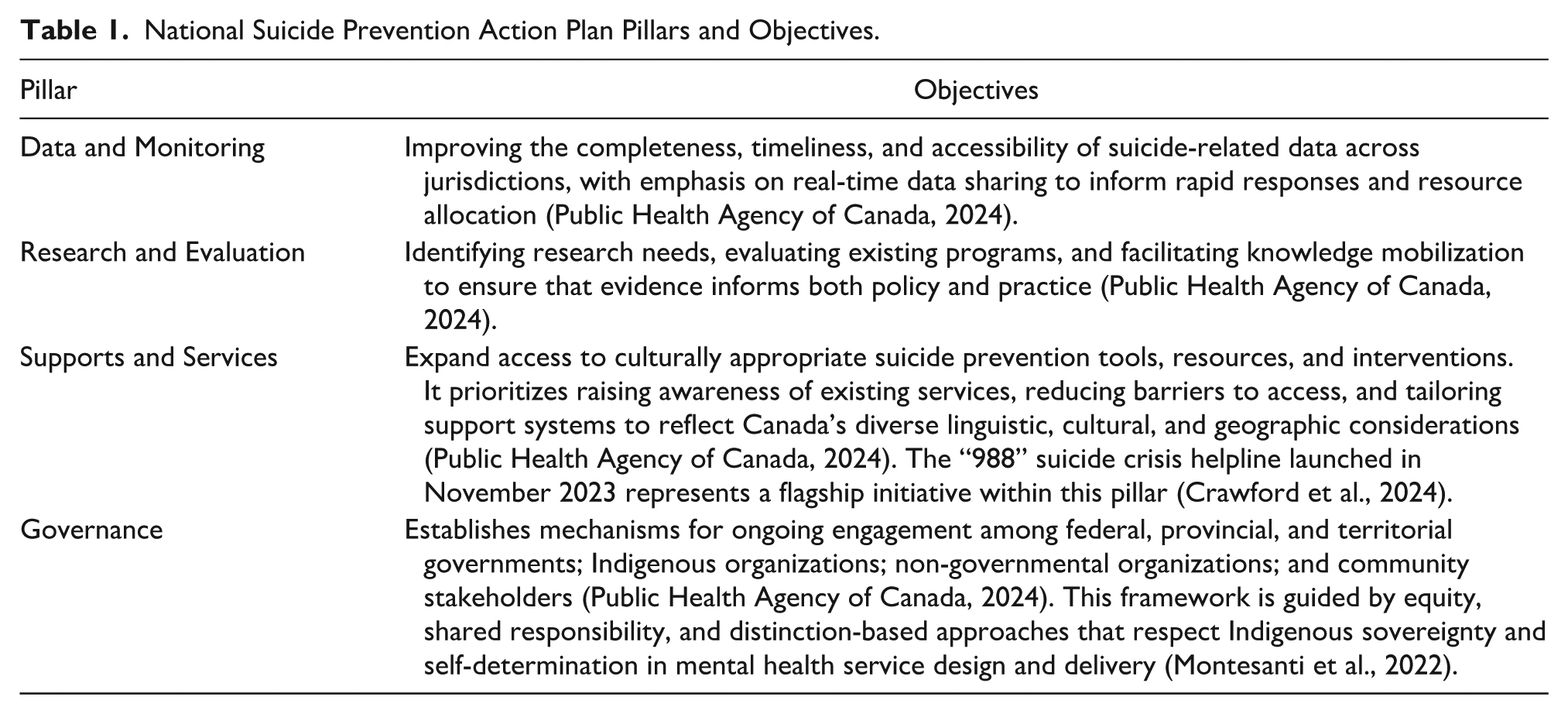
The plan’s operational framework relies on four interconnected strategic pillars, each addressing critical gaps in Canada’s existing suicide prevention infrastructure. Table 1 outlines the main objectives of each pillar.
National Suicide Prevention Action Plan Pillars and Objectives.
Implementation Principles
The implementation plan focuses on three overarching principles: First, evergreen adaptation commits to continuous refinement based on emerging evidence and feedback. It rejects static policies and remains flexible. Second, equity orientation centers on higher-risk populations, including Indigenous people, youth, 2SLGBTQI+ individuals (Two-Spirit, lesbian, gay, bisexual, transgender, queer, and intersex people, along with other sexually and gender-diverse individuals), and rural or remote communities. Third, momentum building leverages existing successes, such as the 988 helpline and growing public awareness, to accelerate progress rather than starting over (Public Health Agency of Canada, 2024). The National Suicide Prevention Plan highlights collaboration among numerous departments, including Health Canada, the Public Health Agency of Canada, Indigenous Services Canada, the Royal Canadian Mounted Police, and Statistics Canada (Public Health Agency of Canada, 2024). While it is laudable that the Canadian government is implementing evidence-based approaches, the Plan could be improved to ensure specific data collection, outreach, and initiatives are in place to ensure lasting changes.
Critique and Recommendations for Each Strategic Pillar
Strategic Pillar 1: Data and Monitoring
The plan identifies data deficiencies but lacks operational specifics. It calls for “complete, timely, and accessible” data without defining these terms. Current suicide data requires 18–24 months to appear in national databases (Navaneelan, 2012), yet the plan sets no improvement timeline. Provincial coroner offices use inconsistent classification systems, undermining interprovincial comparisons, but the plan offers no roadmap for harmonization or technical infrastructure specifications. The 2SLGBTQI+ data gap exemplifies this vagueness: the blueprint acknowledges the lack of sexual orientation and gender identity data but proposes no systematic mechanism for collection. Without operational details, these aspirations remain unfulfilled.
Recommendations for Pillar 1
Canada should establish a National Suicide Surveillance System modeled on the Canadian Chronic Disease Surveillance System (CCDSS), linking coroner data, emergency department visits, hospital admissions, and mental health service utilization for near-real-time monitoring (Public Health Agency of Canada, 2025). Implementation requires: mandatory 30-day reporting of suicide deaths to a federal database; standardized protocols capturing age, sex, Indigenous identity, method, location, prior service contact, and, where possible, sexual orientation and gender identity; and provincial funding tied to compliance, following health care wait-time reporting models. For 2SLGBTQI+ data, Statistics Canada’s survey protocols should extend to mortality investigations with culturally sensitive next-of-kin interviews and privacy protections.
Strategic Pillar 2: Research and Evaluation
The research pillar lacks implementation mechanisms and dedicated funding. Canada’s previous Framework for Suicide Prevention failed to generate robust evidence or effectively disseminate findings (Senate of Canada, 2023). The new plan risks repeating this by relying on Canadian Institutes of Health Research (CIHR) funding rather than specific research allocations. However, CIHR funding is highly competitive and not guaranteed to prioritize suicide prevention research. Without specific research funding, the plan’s research objectives become aspirational rather than operational.
The plan also lacks specificity about which interventions require evaluation. Saskatchewan’s media guidelines provide clear evidence-based impact on suicide rates (Pirkis et al., 2017), yet few other provinces have adopted them. Does the plan propose funding a multi-provincial trial to demonstrate effectiveness in the Canadian context and encourage adoption? Quebec’s regional prevention centers have operated for decades, but their outcomes relative to provinces without such infrastructure remain poorly documented. Should the plan fund comparative effectiveness research? The document provides no answers.
Most critically, the plan contains no mechanism for ensuring that research findings influence policy and practice. Knowledge mobilization is mentioned but not operationalized. Who is responsible for synthesizing research, translating it into practice guidelines, and disseminating it to provinces, health care providers, and community organizations? It identifies research priorities without specifying which interventions require evaluation.
Recommendations for Pillar 2
Based on Canada’s current federal funding agencies, it is recommended that the federal government establish a dedicated Suicide Prevention Research Fund through CIHR with US$10 million annually, modeled on the Canadian HIV Trials Network (Canadian Institutes of Health Research, 2023). The Canadian HIV Trials Network provides sustained, focused funding for a specific health priority. This fund would support pragmatic trials evaluating interventions in real-world Canadian settings, comparative effectiveness studies examining different provincial approaches, implementation research identifying barriers and facilitators to intervention adoption, and health economics research assessing cost-effectiveness to inform resource allocation.
Priority research areas should include: multi-provincial evaluation of media reporting guidelines to generate Canadian evidence supporting nationwide adoption; comparative analysis of Quebec’s regional prevention centers versus other provincial models to identify effective components; evaluation of cultural continuity interventions in Indigenous communities building on Chandler and Lalonde’s (1998) foundational work; and assessment of means restriction policies such as medication packaging changes and firearm storage requirements.
For knowledge mobilization, Canada should establish a National Suicide Prevention Knowledge Exchange Centre, similar to the National Collaborating Centres for Public Health or the Mental Health Commission of Canada’s knowledge exchange functions. This center would synthesize research evidence into practice guidelines, support provinces in implementing evidence-based interventions through technical assistance and training, maintain a public repository of evaluated programs and their outcomes, and convene annual forums bringing together researchers, policymakers, and practitioners to facilitate knowledge transfer. Funding of approximately US$5 million annually would support a small core team with the capacity to commission syntheses and support implementation. Priority research includes multi-provincial evaluation of media reporting guidelines, comparative analysis of Quebec’s prevention centers, cultural continuity interventions in Indigenous communities, and means restriction policy assessments.
Strategic Pillar 3: Supports and Services
The 988 helpline represents progress, but the plan problematically assumes awareness and access are primary barriers. Research shows awareness campaigns have a limited impact without addressing service quality, capacity, and continuity (Luxton et al., 2013). A critical gap is systematic follow-up care: evidence-based caring contact interventions and Zero Suicide frameworks demonstrate effectiveness (Brodsky et al., 2018; Luxton et al., 2013), yet the plan contains no provisions to mandate or fund these approaches. The plan lacks service standards and capacity requirements.
A critical gap is the absence of systematic follow-up care after crisis contact. Evidence from caring contact interventions, such as brief, regular outreach following suicide attempts or psychiatric hospitalization, demonstrates significant effectiveness in preventing subsequent attempts (Luxton et al., 2013). The Zero Suicide framework, emphasizing systematic screening, safety planning, counseling, and transition support, shows measurable impact when implemented comprehensively (Brodsky et al., 2018). However, the plan contains no provisions for mandating or funding these evidence-based follow-up approaches. The 988 helpline may connect individuals to immediate support, but without requirements that health care systems provide consistent follow-up, many callers will fall through gaps between crisis intervention and ongoing care.
The plan also lacks specificity about service standards and capacity requirements. It references “culturally appropriate” services but provides no definition or accountability mechanism. For Indigenous populations, culturally appropriate service might mean access to traditional healing practices, Elders, and land-based interventions, but the plan does not specify how provinces should ensure such access or how federal funding could support it. For francophone communities outside Quebec, culturally appropriate service requires French-language provision, yet the plan contains no mandate ensuring that crisis services beyond 988 operate in French.
Geographic equity presents another unaddressed challenge. Rural and remote communities face substantially longer wait times for mental health services and limited crisis intervention capacity (Barry et al., 2022). The plan acknowledges this but proposes only virtual care expansion as a solution. While telehealth can improve access, it cannot fully substitute for in-person crisis response, particularly in communities where internet connectivity remains unreliable. The plan does not address how rural emergency departments, often staffed by family physicians without psychiatric training, can be supported to provide competent suicide risk assessment and safety planning.
Recommendations for Pillar 3
Beyond the 988 helpline, the Canadian government should fund caring contact programs as a national standard to provide brief, non-demanding outreach following crisis contact that reduces subsequent attempts by 20% (Luxton et al., 2013; Ng et al., 2025). Federal funding could support provincial implementation through a model similar to the Canada Health Infoway, which provided targeted federal investment for specific health system improvements (electronic health records). A Caring Contacts National Implementation Fund would provide provinces with US$50 million over 3 years to establish infrastructure, train staff, and evaluate outcomes.
For Indigenous communities, the plan should specify that at least 30% of suicide prevention funding must support Indigenous-led, culturally grounded interventions. This approach follows the principle established in Budget 2021’s Indigenous Early Learning and Child Care Framework, which allocated dedicated funding percentages for distinction-based programs. Funding should explicitly support land-based healing programs, Elder involvement in crisis response, and Indigenous community-controlled mental health services. Research demonstrates that Indigenous cultural continuity and self-determination in service delivery are protective factors (Chandler & Lalonde, 1998), but as such, these cannot be realized without sustained, dedicated funding streams.
For rural service capacity, the plan should establish a Rural Suicide Prevention Infrastructure Fund modeled on the federal Rural Economic Development program. This fund would support rural emergency departments in hiring mental health specialists or establishing on-call psychiatric consultation services; community-based crisis response teams that can provide in-person assessment and support; and transportation supports enabling rural residents to access specialized services when needed. Allocation could be based on population density and existing mental health infrastructure, ensuring that the most underserved regions receive proportionally greater support.
Strategic Pillar 4: Governance
The governance pillar articulates admirable principles but lacks the structural specificity required for accountability. The plan describes a collaborative governance model involving multiple federal departments, all provinces and territories, and Indigenous partners. However, it does not establish formal accountability mechanisms, performance metrics, or consequences for non-participation or poor performance.
Federal-provincial coordination in Canadian health care has historically been challenging because constitutional jurisdiction over health delivery rests with the provinces (Flood et al., 2023). The Canada Health Act provides a model for federal leverage to encourage provincial compliance with national standards through funding conditions. However, the suicide prevention plan does not employ similar mechanisms. It proposes “collaboration” and “knowledge sharing” but creates no requirements to ensure provinces implement evidence-based practices, meet service standards, or report outcomes.
The plan’s Indigenous partnership framework similarly lacks operational detail. It correctly identifies the need for distinction-based approaches and references existing Indigenous mental wellness frameworks. However, it does not specify how Indigenous organizations will participate in governance beyond consultation. Will Indigenous partners have decision-making authority over resource allocation for Indigenous programs? Are Indigenous communities able to veto federal or provincial initiatives they view as culturally inappropriate? The plan suggests partnership, but does not define the power-sharing mechanisms that would make it meaningful.
A particularly problematic omission is the absence of defined performance metrics and evaluation timelines. Although plan commits to being “evergreen” or continuously updated based on evidence and feedback, it does not specify what evidence will trigger updates or who decides when changes are needed. Without clear success metrics (such as targeted reductions in suicide rates overall or for specific populations), the plan cannot be held accountable. Furthermore, the plan risks replicating the previous Framework’s failure to demonstrate impact without clear success metrics or accountability (Senate of Canada, 2023).
Recommendations for Pillar 4
The governance pillar articulates admirable principles, however it lacks structural accountability. The plan describes collaborative governance involving multiple federal departments, provinces, and Indigenous partners without establishing formal accountability mechanisms, performance metrics, or consequences for non-participation. While federal-provincial coordination in Canadian health care remains constitutionally challenging, the strategy does not employ Canada Health Act-style funding conditions to encourage provincial compliance with national standards. It proposes “collaboration” and “knowledge sharing” without requiring provinces to implement evidence-based practices, meet service standards, or report outcomes. Indigenous partnership lacks operational detail: the plan references distinction-based approaches but does not specify how Indigenous organizations participate beyond consultation, whether they hold decision-making authority over resource allocation, or if communities can veto inappropriate initiatives. The most problematic aspect is the absence of performance metrics and evaluation timelines.
Canada should establish formal Federal-Provincial-Territorial Suicide Prevention Agreements, modeled on bilateral health care agreements used for specific health priorities. These agreements would specify provincial commitments to implement minimum service standards such as 988 access, caring contact programs, and crisis follow-up protocols; data reporting requirements meeting national surveillance system standards; adoption of evidence-based practices such as means restriction and media guidelines; and participation in national evaluation efforts.
In exchange, provinces would receive dedicated federal suicide prevention funding beyond existing health transfers, technical support for implementation, and access to national knowledge mobilization resources. Agreements should include performance clauses: provinces failing to meet commitments would face graduated responses, including enhanced federal support, public reporting of non-compliance, and ultimately funding reductions for persistent non-performance.
For Indigenous governance, the plan should establish an Indigenous Suicide Prevention Council with real decision-making authority, modeled on the First Nations and Inuit Health Branch’s partnership structures. This Council would have binding authority over the allocation of federal funding for Indigenous suicide prevention, approval rights over federal initiatives affecting Indigenous communities, and responsibility for developing and enforcing cultural competency standards for non-Indigenous service providers working with Indigenous populations.
For performance metrics, the plan should establish specific, measurable targets following the Canadian Association for Suicide Prevention’s recommendations. These should include a national suicide rate reduction target of 20% by 2030 (a realistic goal based on international comparisons), population-specific targets acknowledging that different groups face different risks and may require longer timelines, such as 30% reduction in Indigenous youth suicide rates by 2032 and 25% reduction in suicide rates for 2SLGBTQI+ youth by 2030. Annual public reporting on progress toward these targets, disaggregated by province and population group, would create transparency and accountability. An independent evaluation of the plan’s implementation and impact should occur in 2027, informing the development of the next iteration and ensuring that the “evergreen” commitment translates into substantive rather than superficial updates.
Furthermore, Canada should establish formal mechanisms for shared learning through comparative reviews and participation in international suicide prevention networks, site visits, and exchanges with regions showing strong results (Zalsman et al., 2016). Attention should center on countries like Finland and Japan, which have reduced suicide rates, to understand context-specific success factors and judge their fit for Canadian use (Pirkis et al., 2017).
Canadian Association for Suicide Prevention (CASP) Advocacy
Many of the recommendations above correlate with an August 2025 press release from the Canadian Association for Suicide Prevention (CASP) and Dr. Allison Crawford. CASP is Canada’s national registered charity dedicated to suicide prevention, intervention, postvention, and life promotion initiatives across Canada. Dr. Allison Crawford is the Chief Medical Officer at 9-8-8. They strongly recommended that the federal government establish and fund a comprehensive National Suicide Prevention Strategy for 2025 to 2030 (CASP, 2025). Further recommendations include:
Introduce clear national and subpopulation reduction targets such as a “five-year suicide mortality reduction goal and specific sub-targets for priority populations such as youth, men, Indigenous peoples, and 2SLGBTQIA+ communities” (CASP, 2025, para.7).
“Create a national coordinating body with authority across federal departments, partnerships with provinces, territories, and Indigenous governments, and meaningful inclusion of people with lived and living experience” (CASP, 2025, para. 6).
Ensure an anti-racism and anti-ableism perspective and leadership within the equity discussion.
Establish ongoing funding for 9-8-8 (at least US$60 million).
Conclusion
Canada’s National Suicide Prevention Action Plan (2024–2027) represents an important federal benchmark for addressing one of the nation’s most persistent public health challenges. Its strength lies in broad collaboration across governments and sectors and a clear focus on equity for marginalized groups. It also applies distinction-based approaches and adds new tools such as the 988 helpline and youth mental health funding. The plan’s evergreen framework demonstrates an understanding that suicide prevention requires an adaptive, responsive policy capable of evolving with emerging evidence and changing population needs.
However, significant challenges persist that may limit its effectiveness and potential for meaningful impact on Canada’s steady suicide rate. Data infrastructure gaps undermine evidence-based policy development and program evaluation. Long-term funding commitments beyond youth-focused allocations remain unclear and raise sustainability concerns. Implementation depends heavily on the provincial capacity and commitment, creating the potential for geographic inequities. Research infrastructure and knowledge mobilization mechanisms require substantial strengthening to close the gap between evidence generation and practical applications.
The plan’s success depends on sustained political commitment, adequate resource allocation, effective federal-provincial-indigenous coordination, and genuine engagement with affected communities in ongoing adaptation and refinement. The regular evaluation of implementation progress, outcome achievement, and stakeholder satisfaction is essential for accountability and continuous improvement. The evergreen framework’s flexible design must yield concrete systems that ensure new evidence and community input shape future policy.
Consequently, the discussion paper outlined concrete recommendations for each pillar of the National Suicide Prevention Action Plan and encouraged the Canadian government to develop a tailored federal strategy with provincial and territorial collaboration, clear accountability, measurable targets, cross-sectoral coordination, and adequate funding.
Suicide prevention remains a complex, multifactorial challenge that requires sustained commitment across multiple systems, government levels, and societal sectors. Although no single policy can end suicide, coordinated national strategies may provide the structure to align resources, share knowledge, and keep attention on this urgent issue. Canada’s National Suicide Prevention Action Plan marks real progress, yet its impact will depend on turning vision into funded, effective, and well-assessed action.
Footnotes
Acknowledgements
Please note that Taylor and Francis author editing provided recommendations and edits on clarity and structure for the article. In addition, an artificial intelligence tool (Grammarly) was used for minor editorial support, including grammar correction, spelling, and formatting suggestions.
Data Availability Statement
NA.
Declaration of Conflicting Interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I am a Board member of the Canadian Association for Suicide Prevention (it is a voluntary position and I wrote this article of my own accord).
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
NA.
Informed Consent
NA.