
Abstract
Objective:
This discussion paper explores the intersection of cultural factors and Black women’s experiences with chronic pain and suicidality. It aims to inform the continued development of tailored pain interventions and culturally responsive psychiatric nursing care.
Methods:
Using existing literature, we identified six domains of cultural factors potentially influencing Black women’s pain experiences and suicide risk. The six domains were conceptually organized into two categories: culturally specific risk factors and culturally specific protective factors.
Results:
In terms of risk factors, the endorsement of the superwoman schema, intersectionality, and history of medical mistrust were identified. For protective factors, spirituality, culture, and reliance on social support were identified.
Conclusions:
Drawing on the disciplines of African American Studies, Black Psychology, and Clinical Health Psychology, we provide clear recommendations for the development of culturally tailored interventions that can uniquely address Black women’s pain and suicide-related experiences while receiving psychiatric nursing care.
Chronic Pain
Chronic pain is one of the most common reasons adults seek professional medical care, and approximately 100 million adults in the U.S. report experiencing chronic pain (Boyd, Chibueze, et al., 2024). Chronic pain is defined as pain that persists for at least 3 months (Boyd, Chibueze, et al., 2024) and is commonly associated with increased psychological distress and unpleasant emotional experiences (Baker et al., 2008). The economic impact due to chronic pain in the U.S. alone is estimated to range from $560 to $635 billion annually (Gaskin & Richard, 2012; Morales & Yong, 2021). The increasing prevalence of chronic pain and the economic demands of pain management have amplified the field’s focus on research for effective long-term management of pain (Morales & Yong, 2021). Pharmacological, physical therapy, and surgical approaches are commonly used for pain management (Imdad et al., 2025); however, there is an increasing trend to focus on non-pharmacological approaches due to their greater accessibility and reduced risk of adverse side effects (Shi & Wu, 2023).
Recently, there has also been a growing acknowledgment of the significant effects of chronic pain within racial and ethnic minority groups (Morales & Yong, 2021). Prior research shows that higher rates of chronic pain with greater severity have been documented among adults who identify as Black, Indigenous, and people of color (Boyd, Chibueze, et al., 2024) and that Black women are at a higher risk for experiencing significant chronic pain conditions (Baker et al., 2008). For example, according to Drazich et al. (2022), older Black women experience higher rates of pain but are more likely to be undertreated for their pain compared to non-Hispanic white adults. Black women are also at an increased risk for experiencing chronic pain conditions that are “more severe, physically debilitating, and undertreated when compared with men and white women” (Baker et al., 2008, p. 870). Black women often grapple with distinct forms of discrimination due to the intersection of their race, class, gender, and age (Crenshaw, 1989; Drazich et al., 2022). Few studies have closely examined sociocultural factors that play a role in not only Black women’s subjective pain experiences but also their objective pain outcomes and pain-related cognitions (Campbell & Edwards, 2012; C. R. Green et al., 2003; Meints et al., 2019; Rogger et al., 2023), resulting in a lack of contextual understanding of how they experience and cope with pain. Our poor understanding of this population’s unique pain experiences represents a significant challenge for pain measurement and treatment in this population. The limited research on culturally appropriate pain management interventions for Black women represents a glaring gap in the pain literature (Baker et al., 2008; Boyd, Quinn, et al., 2024; Drazich et al., 2022; Zis et al., 2017).
Chronic Pain and Suicidality
Chronic pain has also been consistently linked to elevated risk for suicidal ideation, a concern that is particularly salient for Black women who experience disproportionately high rates of pain-related conditions. Drazich et al. (2022) report that older Black women with comorbid pain and depression described a cycle where chronic pain exacerbated depressive symptoms, and in some cases contributed to suicidal thoughts. Prior research identifies a link between stressful pain experiences and suicide-related behaviors, with chronic pain often seen as a risk factor (Racine, 2018). Certain chronic pain conditions are reported to increase suicidality risk due to the adverse emotional response they can provoke (Chincholkar & Blackshaw, 2023; Hooley et al., 2014). As a result, it is imperative to focus on pain management among Black women as it can address both chronic pain and suicidality (Themelis & Tang, 2023). By addressing pain, interventions can potentially reduce the risk of suicide. To effectively support Black women’s experiences with chronic pain and associated suicide risk, it is important to develop comprehensive, interdisciplinary, and culturally relevant approaches.
Mental health conditions that co-occur with chronic pain pose a challenge for psychiatric nurses who must balance complex decisions about pain management and mental health treatment (Dewar et al., 2009).
Accordingly, we aimed to synthesize existing literature and provide concrete recommendations for psychiatric nurses caring for Black women who are at risk of co-occurring pain and mental health conditions, such as suicide risk. To do this, we explicitly highlighted culturally relevant risk and protective factors potentially influencing Black women’s pain and mental health experiences. A risk factor is conceptualized as a variable that can increase the likelihood of a person experiencing an adverse event, while a protective factor is a variable that decreases the likelihood of a person experiencing an adverse event. Drawing from the disciplines of African American Studies, Black Psychology, and Clinical Health Psychology, we provide clear health care recommendations for the development of culturally tailored interventions that can uniquely address Black women’s pain and suicide-related experiences.
This discussion paper involved a review that took place in two major searches. The search terms included combinations of “Black women,” “suicide risk,” “chronic pain,” “protective factors,” and “risk factors.” The first search focused on pain and chronic pain among Black women or Black adults, yielding 30 articles that met the inclusion criteria and informed the identification of six cultural domains. A second search explored each domain’s relation to suicide risk or protection among Black populations, including women, adults, and adolescents, yielding approximately 16 articles. Relevant data were extracted and organized in an Excel spreadsheet. This process informed the identification of the six cultural factors and their potential relationship with suicide risk, which are presented in the manuscript.
Culturally Specific Suicide Risk Factors
Superwoman Schema
Prior literature reveals that Black women’s endorsement of the superwoman schema may play a role in shaping their perceptions and coping mechanisms for pain (Thorpe et al., 2024) and may also serve as a significant risk factor for the onset of suicide ideation (Benson, 2024). The superwoman schema is a unique cultural factor that should be taken into consideration by psychiatric nurses to understand the specific factors influencing Black women’s pain cognitions, potential suicide risk, and may aid in developing effective culturally relevant pain treatments. Woods-Giscombe (2010) developed the concept of the superwoman schema (which can be used interchangeably with the Strong Black Woman Syndrome) to describe the distinct ways Black women primarily cope with distress. This concept contextualizes the cultural components integrated within Black women’s unique coping experiences and is deeply rooted in the fields of sociology, psychology, and Black feminist theory (Parks & Hayman, 2024). Woods-Giscombe (2010, p. 346) identified five primary coping strategies endorsed by Black women, which include: (a) manifesting strength, (b) suppressing emotions, (c) resisting dependence or vulnerability, (d) succeeding despite limited resources, and (e) putting others’ needs before their own.” Past research has established the endorsement of these strategies as risk factors for Black women, as it may lead to self-silencing and neglect for health concerns (Abrams et al., 2019).
Regarding suicide risk, prior research indicates that the superwoman schema has a significant indirect effect on suicide-related experiences among Black women, particularly through mechanisms of defeat and entrapment (Benson, 2024). Studies have also found that Black women endorsing superwoman schema characteristics as primary coping mechanisms (i.e., strength and affect regulation) report higher levels of depression and suicide ideation (B. N. Green, 2019). Qualitative studies echo these findings, consistently linking superwoman schema endorsement to suicide risk. For instance, analyses of magazines and blogs portraying the superwoman schema in Black women’s media reveal frequent associations with depression, suicidal thoughts, and exhaustion (Black & Peacock, 2011). These studies underscore the potential link between the endorsement of the superwoman schema and suicide risk among Black women.
In relation to coping with pain, Cousin et al. (2022) found that older Black women located in the southern parts of the United States endorsed all five components of the superwoman schema to cope with their experiences of chronic pain. Watson-Singleton (2017) explored the superwoman schema and psychological distress among 158 Black women and found that those who endorsed these cultural coping strategies were less likely to seek help, less likely to exhibit vulnerability, and more likely to experience psychological distress, all of which can contribute to worse chronic pain. The findings from Watson-Singleton’s (2017) study highlight how cultural factors such as the superwoman schema may influence the ways in which Black women cope with pain, rely on emotional support systems, and engage in help-seeking behavior, especially in the context of psychiatric care (Thorpe et al., 2024; Watson-Singleton, 2017).
Potential pain interventions incorporating the superwoman schema as a cultural risk factor may include psychoeducation about the importance of vulnerability and seeking help as forms of strength (rather than weakness), and the importance of communication as a pain management tool. Interventions can also include culturally sensitive assessment by using measures that account for the superwoman schema, such as the Superwoman Schema Questionnaire (Woods-Giscombe et al., 2019), to better understand Black women’s pain experiences and endorsement of this schema and, possibly, the addition of new items for existing pain coping measures that include culturally relevant domains. In addition, increasing representation to include more Black psychiatric nurses specializing in pain treatment for Black women can facilitate compassionate conversations and build trust around reducing suicide risk, chronic pain, and seeking help.
Intersectionality
Intersectionality is an additional cultural risk factor potentially influencing Black women’s pain experiences and associated suicide risk (Adams et al., 2023; Macgregor et al., 2023; Vance et al., 2025). Intersectionality is a theoretical framework coined by Kimberle Crenshaw (1989), which is used to describe the multiple layers of discrimination experienced by Black women and other marginalized populations. Variables contributing to multiple layers of discrimination often include race, class, gender, sexual orientation, religion, mental health status, and access to quality health care and education. Macgregor et al. (2023) argue for the use of intersectionality as a theoretical framework in chronic pain research to acknowledge how distinct populations often experience differing levels of privilege and oppression, which can impact pain treatment responsiveness, effectiveness, and relevance. Specifically, for Black women, psychiatric nurses must understand how intersectional experiences—such as racism, sexism, and other forms of oppression—can exacerbate health inequities, potentially shape pain perceptions, and influence help-seeking behaviors and engagement with chronic pain treatment (Wilson et al., 2024). There is great importance to evaluating the cultural relevance and effectiveness of pain treatment for Black women and whether these treatments take into consideration Black women’s intersectional experiences, which include their mental health experiences.
Intersectionality may play an important role in understanding Black women’s experiences with suicide risk associated with chronic pain. Researchers are incorporating intersectionality theory to develop culturally specific frameworks, such as the Vance-Wade Intersectional Suicide Risk Model, which explains how psychosocial risk factors, gendered racism, and the superwoman schema contribute to racialized gendered stress and may serve as predictors of suicide risk among Black women (Vance et al., 2025). Other models, like Opara et al.’s (2020) intersectional suicide risk model for Black children, highlight the interplay of factors such as racial discrimination, mental health, socioeconomic status, and sexual/gender minority status as leading suicide risk factors. These frameworks demonstrate that Black women’s experiences with suicide risk associated with chronic pain must be understood as complex and multilayered, underscoring the need for interventions that are equally comprehensive and tailored to address intersecting challenges.
Pain interventions that consider intersectionality for Black women must include a multilayered approach. First, providers must start by recognizing and acknowledging their own implicit biases regarding Black women’s pain experiences and openly communicating this awareness to their patients. Prior research indicates that empathy-based educational interventions implemented in medical training programs may be a valuable strategy for mitigating racial bias among future health care providers (Stensland et al., 2025). In addition, psychiatric nurses can actively aid in addressing health and mental health disparities by being knowledgeable about the intersectional factors affecting Black women and connecting Black women with supportive resources such as case management and community-based tools.
History of Medical Mistrust
In addition to the superwoman schema and the complex issue of intersectionality, medical mistrust is another cultural risk factor facing Black women, who have historically endorsed perceptions of mistrust in the health care system (Adams et al., 2023). Medical mistrust is described as suspicion and apprehension against medical professionals and medical systems (Adams et al., 2023). Medical mistrust among Black women is often rooted in awareness of historical atrocities, including a history of scientific racism embedded within medical systems. This can be seen in the surgical experimentation on enslaved Black women in the 1800s without anesthesia, the use of pseudoscience to justify categorizing Black individuals as psychologically distinct and inferior to white individuals, and the Tuskegee Syphilis Study, which refused to provide ethical care to Black men (Adams et al., 2023). Given the historical legacy of medical mistreatment and intentional exploitation of Black bodies, pain treatment must acknowledge this history when considering the development and implementation of pain and mental health management strategies for Black women in psychiatric care.
Medical mistrust may exacerbate Black women’s experiences with suicide risk associated with chronic pain, specifically by decreasing their willingness to seek mental health support (Boyd, Quinn, et al., 2024; Pederson, et al., 2025). For instance, Pederson et al. (2025) found that high levels of medical mistrust were associated with lower willingness to seek care from mental health professionals among 1,043 Black adults in the United States. Research also suggests a correlation between mental health seeking attitudes and suicide attempts and ideation. Specifically, Black young adults with positive mental health seeking attitudes were 34% less likely to attempt suicide and 35% less likely to experience suicide ideation (Boyd, Quinn, et al., 2024). These findings may imply that Black women’s experiences with suicide ideation can be worsened by a lower willingness to seek mental health support due to a history of medical mistrust, which further highlights the need for culturally sensitive care and efforts toward addressing inequities in health care.
Black women who are suffering in silence with their pain and mental health may continue to suffer if trust is not established or repaired among the medical systems. This can be particularly difficult when Black women present with chronic pain, given the subjective phenomenology of chronic pain and medical mistrust already implicit in the treatment of chronic pain regardless of cultural context (Mikesell & Bontempo, 2023). Potential pain interventions acknowledging the history of medical mistrust and Black women’s mental health require not only cultural awareness but also deliberate communication and genuine rapport building between medical professionals and Black female patients seeking and needing culturally relevant pain treatment. Effective communication about pain treatment is imperative as health care providers must ensure that information is accessible, clearly explained, empowering, and includes reassurance that pain complaints are believed and taken seriously. To aid in repairing trust within medical systems, it is also important that Black women understand the rationale and reasoning behind treatment recommendations. Black women should also be able to engage in collaborative discussions about their pain and mental health treatment by sharing their preferences and concerns, and feel empowered and motivated to participate in shared decision-making to determine the most effective treatment plan.
Culturally Specific Suicide Protective Factors
Spirituality
Though efforts to overcome treatment barriers often focus on mitigating risk factors, recognizing and strengthening protective factors can be equally important. Existing literature highlights three primary protective factors that can support Black women’s experience in pain management, including the endorsement of spirituality, conceptualizing culture as a resource, and leaning on social support (e.g., collectivistic orientation). These three protective factors have also been shown to reduce suicide risk among Black populations (Chatters et al., 2011; Fanegan et al., 2022; Street et al., 2012). Identifying and understanding culturally relevant protective factors specific to suicide risk associated with chronic pain may aid in informing the creation of culturally tailored interventions uniquely designed to support Black women.
Historically, spirituality has been regarded as a fundamental resource in supporting the well-being of Black communities (Kambon, 2012). The use of spirituality as a coping mechanism is often more accessible, culturally relevant, and a traditional practice that is passed down within African/Black communities (Kambon, 2012; Utsey et al., 2000). Black psychologists who specifically study culture and race-specific coping found that prayer and reliance on spirituality is often associated with improved quality of life for African Americans (Bakhshaie et al., 2022; Utsey et al., 2000). According to Bakhshaie et al. (2022), African Americans are also more likely to use spirituality (i.e., prayer) to cope with their pain experiences.
Spirituality may also serve as a culturally relevant protective factor by reducing Black women’s risk of suicide ideation associated with chronic pain. For example, Spates and Slatton (2023) examined existing literature to better understand factors that may protect Black women from suicide. Spirituality was found to be a protective factor, empowering Black women to believe in something greater than themselves. Similarly, Dorsey Holliman et al. (2018) used qualitative methods to identify suicide protective factors among Black women veterans. This study found that “faith in God, personal practices, and religious beliefs” were significant protective factors (p.1). A systematic review of religion’s relationship with suicidality among Black Americans found that religiosity may have a significant protective effect against suicidality but may also discourage the use of formal mental health services (Fanegan et al., 2022). Collectively, these studies highlight the important role that faith, spirituality, and religion can play in protecting Black women from suicide risk associated with chronic pain. However, additional research is needed to explore the specific relationship between spirituality, chronic pain, and suicidality among Black women.
As a result, effective pain and mental health treatment for Black women requires psychiatric nurses to acknowledge and incorporate the potential vital role of spirituality in their Black female patients, which begins with the inclusion of religion and spirituality as part of the chronic pain intake assessment. In addition to awareness, there is equal importance in thinking about deliberately integrating spirituality into pain interventions in practical and accessible ways, such as creating holistic pain management plans that incorporate spiritual care and ask about patients’ spiritual beliefs, practices, and values.
Culture
Black women’s culture may serve as a vital protective tool when coping with chronic pain and associated mental health conditions, such as suicide risk. Prior scholarship conceptualizes culture as a resource in pain management that inevitably influences the ways in which pain is communicated, as well as shapes the ways individuals experience, respond, and seek treatment for pain (Rogger et al., 2023). Pillay et al. (2014) explain that cultural identities can be a resource for individuals with chronic pain, because they provide a framework for meaning-making and include culturally based coping strategies (i.e., prayer). Literature in the field of Black psychology indicates that a positive perception of one’s culture is often linked with improved health outcomes for Black communities (Willis & Neblett, 2020).
Specific to suicide risk that may be associated with Black women’s chronic pain experiences, culture may serve as a protective factor. In the field of Black psychology, the impact of culture is often measured and operationalized through the construct of racial identity (Sellers et al., 1998). Racial identity is defined as the significance and importance one places on being Black and how it informs self-concept and cultural beliefs (Sellers et al., 1998). Higher levels of racial identity typically indicate greater connectedness to one’s culture and a positive perception of one’s culture (Sellers et al., 1998). Research supports the protective role of racial identity in suicide risk. Street et al. (2012) explored the impact of racial identity on reasons for living among 82 Black women with a recent suicide attempt, finding that women who viewed race as central to their identity had more reasons to live, citing community and cultural membership as key factors. Blassingame et al. (2023) similarly found that Black women with higher racial identity and more positive feelings about being Black reported greater reasons for living, well-being, and suicide resilience.
A strong racial identity is not only a marker of cultural connectedness but also a potential component of well-being among Black Americans. Black women experiencing suicide risk associated with chronic pain may benefit from the protective nature of cultural connection and higher racial identity. Using existing literature about the potential impact of culture, psychiatric nurses can better support Black women’s pain and mental health management by recognizing the interplay between culture, pain coping, suicide risk, and effective and adaptive pain treatment. Incorporating cultural values and practices into pain treatment for Black women may be beneficial, such as using spiritual practices like prayer and addressing cultural beliefs related to pain and illness. By honoring Black women’s culture, psychiatric nurses can create more personalized and humanizing pain and mental health management plans for Black women.
Collectivism
The endorsement of a collectivistic orientation (i.e., reliance on social support) has also been found to be a protective resource for pain experiences (Vina et al., 2013). Social support can facilitate an individual’s coping by leveraging social networks to provide psychological and material resources (Vina et al., 2013). Examples of psychological and material resources may include emotional support from family and friends, financial assistance with medical bills, and practical assistance (i.e., child care, house chores, and errands). Previous research shows that higher levels of social support are often correlated with improved patient decision-making, medication adherence, and other health-related behaviors (DiMatteo, 2004; Vina et al., 2013). Interestingly, although prior research highlights the protective effects of social support for pain, Black women may not commonly use social support (in the traditional ways) for their pain management. For example, in a study that assessed potential racial differences in social support among individuals coping with knee pain, the researchers found that “African Americans were less likely to have structural and functional support than white patients” (Vina et al., 2013, p. 1108). Social support may serve as a protective coping strategy for pain; however, Black women may not have accessible structures to facilitate pain support, which underscores the importance of the current research. Further exploration is needed to understand the unique cultural context of social support in Black women’s lives (i.e., roles of church, beauty salons, kinship networks) and how this support can appropriately be applied to Black women’s chronic pain experiences.
Specific to suicide risk that may accompany Black women’s pain experiences, it is essential to explore the unique ways social support can serve as a protective factor. Research has shown that social support is a protective factor for suicide risk (Holman & Williams, 2022). In the field of Black psychology, social support is often operationalized and measured through the construct of collectivism and collective coping (Kambon, 2012; Utsey et al., 2000). Studies have found that a strong sense of community is a significant protective factor against suicide risk among Black women (Borum, 2012); perceived supportive behaviors from family provide indirect protective effects on suicidal behaviors among Black American college students (Wang et al., 2013); and church-based social support is a protective factor for suicidality among Black Americans and Black Caribbeans (Chatters et al., 2011). Although some research suggests that Black women may not always use traditional support for pain management (Vina et al., 2013), Black women are engaging in social support as a coping strategy through culturally specific routes, such as the church. Therefore, social support may be a protective factor against suicide risk accompanying Black women’s pain experiences and warrants further exploration, particularly regarding culturally specific ways Black women engage in social support.
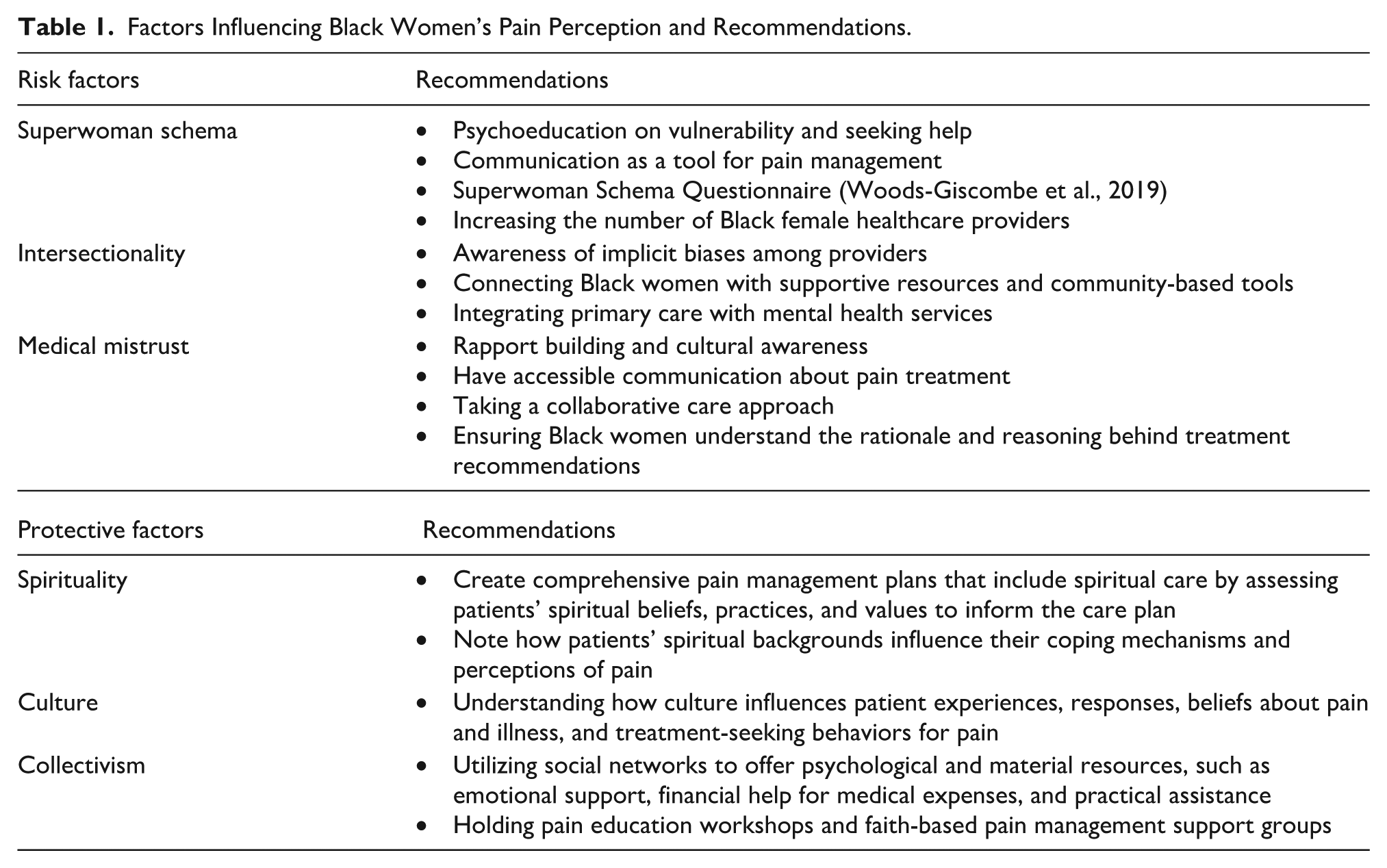
Psychiatric nurses must consider the complex and unique interplay between social support, suicide risk, cultural context, and pain treatment among Black women. Specifically, psychiatric nurses should acknowledge and lean on Black women’s accessible and culturally relevant social support resources to aid in developing more effective and personalized pain treatment plans. Practical examples of culturally relevant pain interventions using Black women’s unique social support systems may include faith-based pain management support groups in church, pain education workshops in accessible settings such as beauty salons, and community-based events (using food, education, and culturally relevant music) to aid in destigmatizing vulnerability and encourage help-seeking pain management. It may also be important to explore the ways in which Black women’s social support can be leveraged to mitigate the endorsement of the superwoman schema by encouraging vulnerability and help-seeking behaviors to manage pain. See Figure 1 and Table 1 for a display and explanation of the six cultural domains potentially influencing Black women’s pain experiences and associated suicide risk.
Risk and protective factors influencing pain perceptions among Black women.
Factors Influencing Black Women’s Pain Perception and Recommendations.
Conclusion
Overall, the current paper examined cultural factors influencing Black women’s pain and accompanying suicide risk to support psychiatric nurses in developing personalized pain interventions for Black women. Using existing literature, we identified six domains of cultural factors potentially influencing Black women’s chronic pain and suicide-related experiences. The six domains were conceptually organized into two categories, including culturally specific risk factors and culturally specific protective factors. In terms of risk factors, the endorsement of the superwoman schema, intersectionality, and a history of medical mistrust were identified. For protective factors, spirituality, culture, and reliance on social support were identified.
Focusing on Black women’s experiences with pain is needed, especially considering the current political climate in which diversity, equity, and inclusion efforts are being purposely dismantled (Clancy, 2025). Black women deserve to have their voices heard, their pain acknowledged, and their mental health prioritized. Equitable health care and personalized pain intervention are not about diverting attention away from others, but rather about honoring and addressing the unique needs of each individual. By taking a deliberate and holistic approach to pain and mental health intervention, psychiatric nurses can provide more effective support for healing and coping with comorbid conditions. By emphasizing the cultural determinants of pain experiences relevant to Black women, this discussion paper can inform personalized pain interventions and psychiatric nursing care to address the unique needs of Black women.
Footnotes
Author Contributions
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Vanessa Oliphant, Ph.D.
Gabriella Martinez, Ph.D.
Courtney Harold M.S.
De’ja Broyles, M.A.
Jennifer Williams, Ph.D.
Paul Nabity, Ph.D.
Donald McGeary, Ph.D.
Meredith Stensland, Ph.D., MSW2
The APNA planner and authors have no relevant financial relationships with ineligible companies or off label uses to disclose.
By the end of this article, the reader will be able to:
Explain risk and protective factors influencing chronic pain and suicide risk among Black women.
There is no fee for Nursing Continuing Professional Development (NCPD) contact hours.
Contact hour: To receive contact hours, you must read the entire article, complete a reflection activity, an evaluation, and the honor statement. Once you have completed the activity, evaluation, and honor statement, your nursing continuing professional development certificate will be generated online and available for immediate printing. Credit cannot be earned unless all components of the program are completed.
Go to apna.org/JAPNACEJuly2026 to access the reflection activity, evaluation, honor statement, and certificate.
The American Psychiatric Nurses Association is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center’s Commission on Accreditation.