
Abstract
Background:
Methylphenidate is a first-line psychostimulant widely prescribed for the treatment of attention-deficit/hyperactivity disorder (ADHD). Although its therapeutic efficacy is well established, concerns remain regarding its potential effects on cardiovascular regulation, particularly on autonomic nervous system balance.
Aims:
To evaluate the effect of methylphenidate on heart rate variability (HRV) in ADHD children and adolescents.
Methods:
Our review included children and adolescents diagnosed with ADHD, studies wherein the intervention group should receive short- or long-term methylphenidate treatment, studies that evaluated participants under conventional treatment except methylphenidate, single or double-blind, non-blind randomized or non-randomized control studies.
Results:
No significant changes were observed in time- and frequency-domain HRV indices, with all outcomes presenting very low certainty of evidence.
Conclusions:
Our results indicate that methylphenidate does not significantly affect resting heart rate HRV in ADHD children and adolescents. The very low certainty of this review’s evidence level and high risk of bias warrant further studies to provide stronger scientific and statistical evidence.
Introduction
Methylphenidate is a pharmacological psychostimulant prescribed for treating children and adults with attention-deficit/hyperactivity disorder (ADHD). It is similarly prescribed for narcolepsy, refractory depression in the elderly, fatigue in individuals with cancer, cognitive performance (e.g., memory), and lethargy in Alzheimer’s disease (Verghese et al., 2024). Methylphenidate blocks norepinephrine and dopamine reuptake in presynaptic neurons, inhibiting these neurotransmitter transporters and elevating their concentrations in the synaptic cleft. This pharmacological mechanism induces a stimulant effect in the central nervous system, predominantly in the prefrontal cortex (Shellenberg et al., 2020).
Given the extensive use of methylphenidate during childhood and adolescence and ongoing concerns regarding its cardiovascular and autonomic effects, the present synthesis aimed to systematically evaluate the effects of methylphenidate on heart rate variability (HRV) in children with ADHD through a systematic review and meta-analysis.
Methylphenidate has substantial public health relevance, as approximately 7 million children in the United States are prescribed this medication for ADHD management (Zablotsky & Terlizzi, 2020). Given the scale of exposure during critical periods of growth and neurodevelopment, even modest benefits or adverse effects may have meaningful population-level implications. Therefore, generating robust evidence on the broader effects of stimulant therapy is essential to inform clinical decision-making, optimize risk–benefit assessments, and support safer prescribing and monitoring strategies in pediatric ADHD care (Raman et al., 2018).
Earlier studies have demonstrated a cardiovascular dysfunction risk associated with medications prescribed for ADHD (Torres-Acosta et al., 2020; Zhang et al., 2022). This relationship was highlighted in a Review Topic of the Week because of its relevance (Torres-Acosta et al., 2020). The American College of Cardiology Guidelines recommended that physicians lessen the dosage of sympathomimetic amines or terminate these pharmacotherapies altogether in hypertensive individuals with ADHD, as it may increase blood pressure further (Whelton et al., 2018). The interaction between psychostimulants and the autonomic nervous system has raised additional concerns (Torres-Acosta et al., 2020). Sympathetic activation may increase resting blood pressure and heart rate, promote vasoconstriction, and contribute to arrhythmogenic risk. Sympathetic stimulation induced by psychostimulants could promote hypertension, increasing cardiovascular mortality and the possibility of myocardial infarction (Thayer et al., 2010).
In addition, of late, ADHD has been linked with cardiovascular disorders (Thapar et al., 2023). A prospective cohort study (Thapar et al., 2023) reported that adults with childhood ADHD problems presented important cardiovascular risk factors, with higher body mass index, triglyceride levels, and systolic and diastolic blood pressures.
In this situation, HRV is a reliable non-invasive method that estimates autonomic nervous system (ANS) function through analysis of interbeat interval oscillations (Vanderlei et al., 2009). The scientific research literature presents robust evidence indicating HRV as a dependable technique to detect physiological, cardiovascular, and metabolic risk factors (da Silva et al., 2014; de Andrade et al., 2017; Ferreira et al., 2015; Speer et al., 2024) and to predict diseases (Adam et al., 2023; Aftyka et al., 2023; Ranpuria et al., 2008; Singh Solorzano et al., 2022).
Heart rate variability (HRV) is the natural variation in the time interval between consecutive heartbeats and is considered a non-invasive marker of autonomic nervous system regulation. In general, higher HRV indicates better autonomic flexibility, stronger parasympathetic activity, good recovery capacity, better cardiorespiratory fitness, and greater resilience to physical or psychological stress. In contrast, lower HRV may suggest reduced autonomic adaptability and can be associated with stress, poor sleep, fatigue, illness, overtraining, inflammation, anxiety, cardiometabolic conditions, autonomic dysfunction, or cardiovascular disease. However, HRV is highly individual and influenced by age, sex, fitness level, medications, sleep, alcohol intake, hydration, respiratory pattern, and measurement method. Therefore, HRV should preferably be interpreted as a trend over time within the same person rather than as an isolated value, and it should complement, not replace, clinical assessment (Garner et al., 2025; Salatini et al., 2022).
Despite the growing recognition of HRV as a clinically meaningful marker of autonomic and cardiovascular health, its modulation in individuals with ADHD undergoing pharmacological treatment remains insufficiently characterized. Existing studies evaluating the effects of methylphenidate on HRV have reported heterogeneous and, at times, conflicting findings, with variations in study design, sample size, age groups, treatment duration, dosing regimens, and HRV assessment protocols. Moreover, many investigations are limited by small cohorts, cross-sectional designs, or lack of appropriate control groups, restricting the ability to draw robust conclusions regarding causality and clinical relevance (Buchhorn, 2014; Buchhorn & Christian, 2014; Buchhorn, Conzelmann et al., 2012; Buchhorn, Müller et al., 2012; Buchhorn et al., 2020; Shim et al., 2015; Negrao et al., 2011). Importantly, no consensus has been established on whether methylphenidate induces sustained alterations in autonomic balance or whether observed HRV changes translate into meaningful cardiovascular risk over time. To date, the absence of a comprehensive systematic synthesis and quantitative meta-analytic evaluation of available evidence represents a critical gap in the literature, hindering evidence-based clinical decision-making and long-term cardiovascular monitoring strategies for individuals with ADHD.
Based on the aforesaid, we highlighted the following questions: Does methylphenidate affect HRV in children and adolescents with ADHD? Is there strong enough evidence to support an ADHD treatment plan? So, we assessed the effect of methylphenidate on HRV in children and adolescents with ADHD via a systematic review and meta-analysis.
Method
Registration
Our systematic review was reported based on the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Page et al., 2021; Raimundo, 2026) and is registered in the PROSPERO database (CRD42024524865).
Search Strategy and Study Selection
A comprehensive and systematic literature search was conducted in the EMBASE, MEDLINE/PubMed (via National Library of Medicine), Cochrane Library, CINAHL, Scopus, and Web of Science databases from inception to January 2026. No restrictions regarding publication status were applied. Searches were limited to studies published in English.
The search strategy combined controlled vocabulary terms (when applicable) and free-text keywords related to methylphenidate, ADHD, and cardiac autonomic function. The core search terms included:
(“Methylphenidate” OR “Metadate” OR “Equasym” OR “Centedrin” OR “Tsentedrin” OR “Ritalin SR” OR “Methylin” OR “Concerta” OR “Daytrana” OR “Phenidylate” OR “Ritalin”) And (“ADHD” OR “Attention Deficit Hyperactivity Disorder” OR “Attention Deficit Disorder” OR “Hyperkinetic Syndrome”) And (“heart rate variability” OR “RR variability” OR “heart period variability” OR “vagal” OR “autonomic nervous system” OR “ANS”).
Search strategies were adapted as necessary for each database to account for differences in indexing and syntax. The complete search strings for all databases are provided in the Supplementary Material.
All retrieved records were exported to Rayyan QCRI (Qatar Computing Research Institute, Doha, Qatar) for duplicate removal. Two independent reviewers (SHSG and AAP) screened titles and abstracts for eligibility. Full-text articles were then independently assessed for inclusion by the same reviewers. Any disagreements were resolved through discussion, and when consensus could not be reached, a third senior reviewer (VEV) made the final decision. In addition, the reference lists of all included studies and relevant review articles were manually screened to identify potentially eligible studies not captured in the electronic search.
Eligibility Criteria
The inclusion and exclusion criteria were consistent with the PICOS (Population, Intervention, Comparison, Outcomes, and Study Design) elements, including:
(P) Children and adolescents with a formal diagnosis of ADHD, established according to standardized diagnostic criteria (e.g., DSM or ICD). We excluded studies with adults (≥18 years of age), participants without a confirmed diagnosis of ADHD, studies including participants with major cardiovascular diseases, congenital heart disease, or clinically relevant arrhythmias at baseline, unless these conditions were explicitly controlled for in the study design;
(I) Methylphenidate administered as monotherapy, regardless of formulation, dose, route of administration, or treatment duration (short-term or long-term). We excluded studies that combined pharmacological interventions in which methylphenidate was administered together with other psychostimulants or cardiovascular-active drugs, non-pharmacological interventions, or multimodal treatments where the isolated effect of methylphenidate could not be determined.
(C) Comparison groups included: (1) control participants; (2) children and adolescents with ADHD not receiving methylphenidate; or (3) the same participants assessed before methylphenidate initiation (within-participant comparison);
(O) HRV indices were the results of interest;
(S) We included randomized controlled trials, non-randomized controlled studies, and observational before–and–after studies that evaluated the effects of methylphenidate on HRV in children and adolescents with ADHD. Given the limited availability of randomized trials in this field, non-randomized and observational designs were also considered eligible. This study was restricted to articles published in peer-reviewed journals and written in English. We excluded conference papers, master’s theses, doctoral dissertations, descriptive studies, case studies, editorials, and reviews.
Data Extraction
Data related to the authors, study design, characteristics of the study participants and treatment were extracted from primary references and presented in Table 1. Absent data were solicited by contacting the appropriate study’s authors. This phase was completed independently by at least two investigators (SHSG, AAP, RDR, ISS). If the corresponding author did not respond, the Web Plot Digitizer® was required to extract the graph’s data. The HRV parameters were charted as means and standard deviations (SD). Values with “confidence intervals” (CI) or “standard error” in the references were converted to SD.
Description of the Characteristics of the Study Population of Articles by Author and Year, Sample, Age (Years), Intervention, Control and Outcomes.
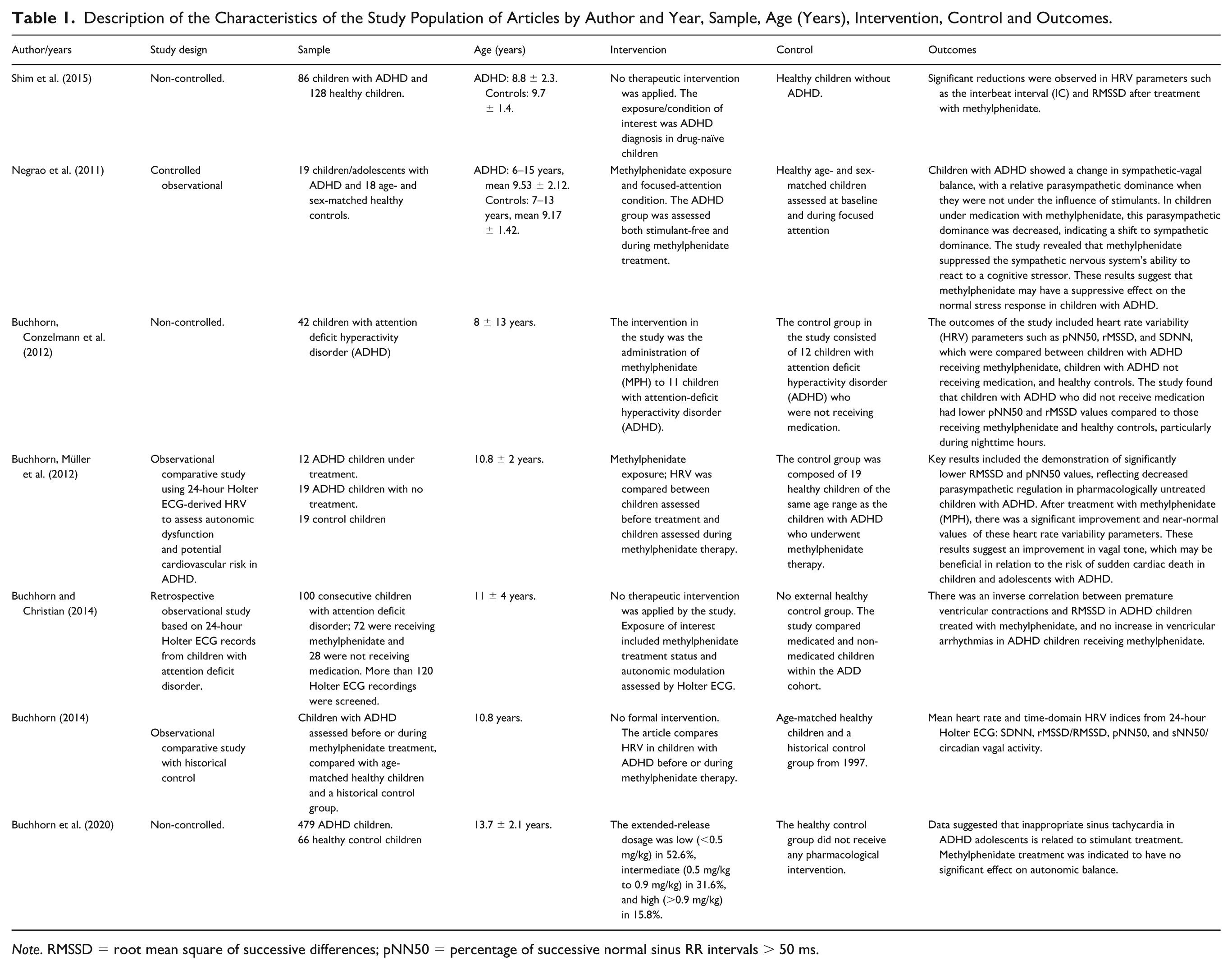
Note. RMSSD = root mean square of successive differences; pNN50 = percentage of successive normal sinus RR intervals > 50 ms.
The HRV indices extracted and analyzed included the standard deviation of normal-to-normal intervals (SDNN), root mean square of successive differences between normal heartbeats (RMSSD), percentage of adjacent normal-to-normal intervals differing by more than 50 ms (pNN50), low-frequency power (LF), high-frequency power (HF), Poincaré plot standard deviation perpendicular to the line of identity (SD1), Poincaré plot standard deviation along the line of identity (SD2), and the RR triangular index.
Assessment of the Risk of Bias in Individual Studies and Across Studies
The bias assessment for the included studies was conducted using the ROBINS-I tool (Risk of Bias in Non-Randomized Studies of Interventions), developed by the Cochrane Methods Group (Sterne et al., 2016). ROBINS-I assesses risk of bias across seven methodological domains: “Bias due to confounding,” “Bias in selection of participants,” “Bias in classification of interventions,” “Bias due to deviations from intended interventions,” “Bias due to missing data,” “Bias in measurement of outcomes,” and “Bias in selection of the reported results.”
Each domain was judged according to standardized criteria and categorized into one of the following levels: low risk, moderate risk, serious risk, critical risk, or no information. Our judgments followed the guidance presented in the “ROBINS-I: Detailed Guidance” documents, specifically the section “Reviewers’ Judgments and Criteria for Judgment” (Sterne et al., 2016). The risk-of-bias assessment was independently performed by two reviewers. In cases of disagreement, a third reviewer resolved the discrepancies.
We also examined potential factors that could impact the overall body of evidence, including publication bias, selective outcome reporting, and inconsistencies within studies. All assessors underwent dedicated training sessions to ensure proper use of the ROBINS-I tool and consistency in evaluations.
GRADE (Levels of Evidence)
The Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) framework was used to assess the certainty of the evidence. This evaluation included the study design (strong evidence). We considered study quality (detailed study methods and conduct) and limitations in the strength of evidence (Meader et al., 2014). We used the GRADEpro GDT v4® (McMaster University, Ontario, Canada) to create the summary of the findings table.
Qualitative Analysis (Systematic Review)
We performed a narrative synthesis to describe data regarding how each study was completed. Details for the selected references were offered in texts and tables. Results of the qualitative analysis were obtained by analyzing HRV indices for the intervention or control protocols.
Quantitative Analysis (Meta-Analysis)
A meta-analysis was conducted when at least two studies reported comparable HRV outcomes using equivalent metrics and provided sufficient quantitative data (mean and standard deviation) to allow effect size calculation. When available, pre- and post-intervention values were extracted; for studies with different comparison structures, effect estimates were calculated accordingly. Only HRV indices consistently reported across studies were pooled.
Given the methodological and clinical diversity among the included studies—particularly with respect to study design (intergroup vs. intragroup comparisons), participant characteristics, methylphenidate dose, and intervention duration—a random-effects model was applied a priori. This approach was chosen to account for both within-study and between-study variability and to enhance the generalizability of the pooled estimates.
Statistical heterogeneity was assessed using the I2 statistic, with values >50% interpreted as indicating substantial heterogeneity, in accordance with established guidelines (Higgins & Thompson, 2002). When substantial heterogeneity was detected, its potential sources were explored through pre-specified subgroup analyses, separating studies according to comparison type (intergroup versus intragroup designs). This strategy was adopted to minimize methodological heterogeneity and to improve the interpretability of the pooled results.
Effect sizes were expressed as mean differences (MDs) with corresponding 95% confidence intervals (CIs). Statistical significance for the overall effect was defined as p < .05. All meta-analyses, heterogeneity assessments, and forest plots were generated using Review Manager software (RevMan®, version 5.4.1). Forest plots were used to visually present individual study effects, pooled estimates, 95% confidence intervals, and heterogeneity statistics for each HRV outcome included in the meta-analysis.
Results
Description of Studies
We documented 4,193 references through searches in the databases. We eliminated duplicates (n = 232), and 3,961 references were screened for inclusion criteria. Among the publications, 3836 records were omitted after reviewing the title or abstract. Thirteen studies were excluded as they were reviews, 72 references were deleted as they were unrelated to methylphenidate, and 26 were removed for the reason that they did not present the outcome of interest. A further seven were excluded since they were letters.
There remained seven studies that were assigned for full-text reading, qualitative analysis, risk of bias assessment, GRADE analysis, and meta-analysis possibility (Buchhorn, 2014; Buchhorn & Christian, 2014; Buchhorn, Conzelmann et al., 2012; Buchhorn, Müller et al., 2012; Buchhorn et al., 2020; Shim et al., 2015; Negrao et al., 2011). Six publications (Buchhorn, 2014; Buchhorn, Conzelmann et al., 2012; Buchhorn, Müller et al., 2012; Buchhorn et al., 2020; Shim et al., 2015; Negrao et al, 2011) were included for the meta-analysis. All search methods and selection stages followed the PRISMA statement flow diagram (Figure 1). Additional details about the publications are provided in Table 1. All studies included in this systematic review were conducted in accordance with the Declaration of Helsinki and reported approval by an institutional review board or ethics committee, as well as informed consent obtained from participants or their legal guardians when applicable.
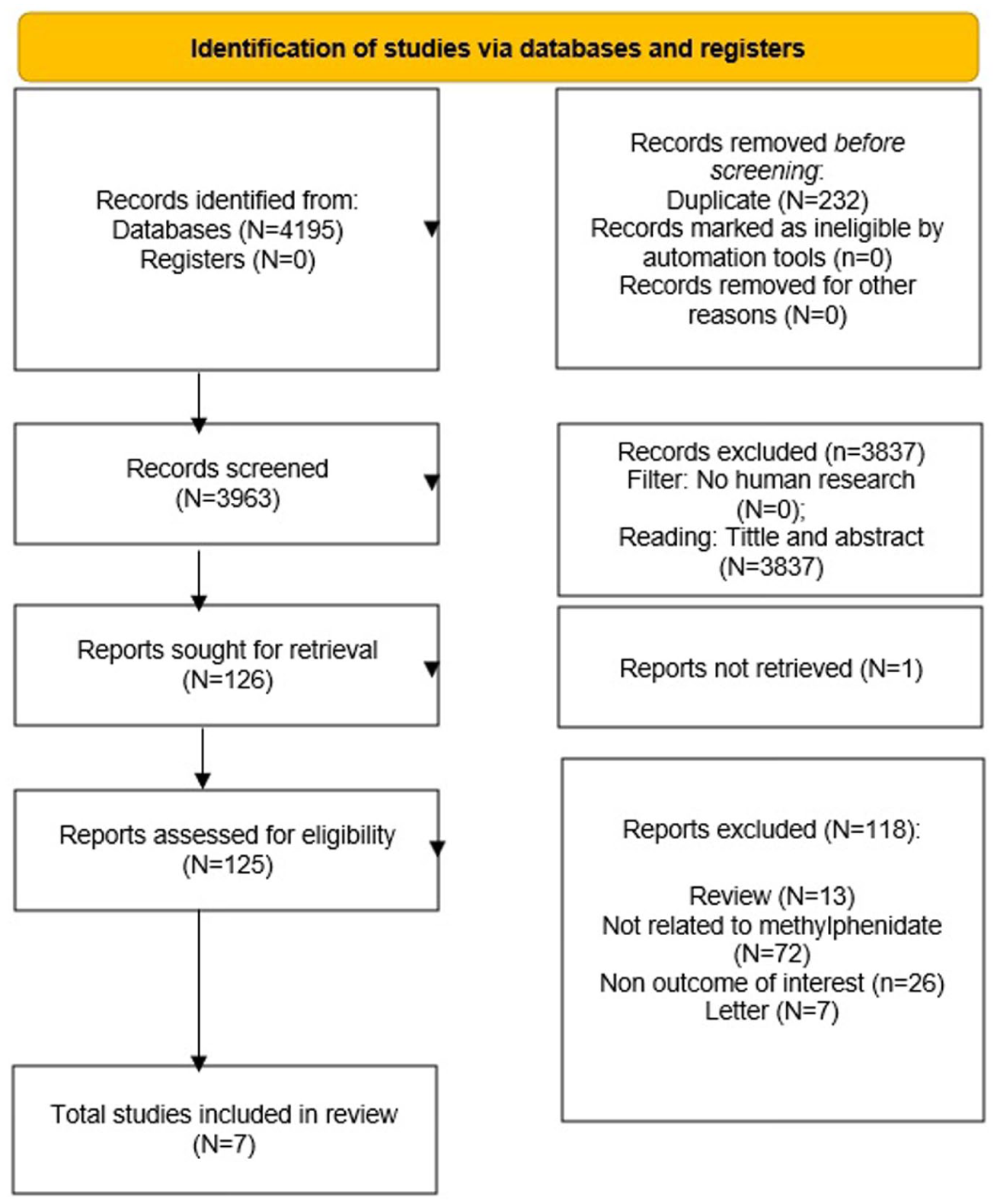
PRISMA 2020 flow diagram for new systematic reviews, which included searches of databases and registers only.
The references included were published between 2011 and 2020 (Table 1). Five studies originated from Germany (Buchhorn, 2014; Buchhorn & Christian, 2014; Buchhorn, Conzelmann et al., 2012; Buchhorn, Müller et al., 2012; Buchhorn et al., 2020), one from South Korea (Shim et al., 2015), and one from South Africa (Negrao et al., 2011). One publication was a pilot study (Buchhorn, 2014), five non-controlled (Buchhorn & Christian, 2014; Buchhorn, Conzelmann et al., 2012; Buchhorn, Müller et al., 2012; Buchhorn et al., 2020; Shim et al., 2015), and one was a non-randomized and controlled trial (Negrao et al., 2011).
Buchhorn, Conzelmann et al. (2012) considered children with ADHD and age-matched children without heart disease as a control group. Buchhorn, Müller et al. (2012) appraised children receiving methylphenidate intervention, children with ADHD without medication, and children without cardiac injury as a control. Buchhorn (2014) inspected participants with ADHD and control participants without ADHD. Negrao et al. (2011), Buchhorn & Christian (2014), Buchhorn et al. (2020) and Shim et al. (2015) examined only adolescents and children with ADHD.
In regard to exclusion criteria, Negrao et al. (2011) omitted children and adolescents undergoing pharmacotherapies other than methylphenidate, children with co-morbidities, children with intellectual disabilities, malnourished, and children and adolescents unable to give informed assent because of a lack of understanding. Buchhorn, Conzelmann et al. (2012) left out the examination of five children with ADHD with more than 20 premature ventricular contractions during 60 min. Buchhorn, Müller et al. (2012) excluded children who experienced over 20 premature ventricular contractions during an hour and children with hyperthyroidism, suffering from Graves’ disease. Buchhorn and Christian (2014) and Buchhorn (2014) did not explain or describe sample loss. Shim et al. (2015) excluded children and adolescents with neurodevelopmental or learning disorders and medical irregularities that necessitated specialist attention, including cardiovascular disorders and psychiatric comorbid conditions. Buchhorn et al. (2020) omitted children and adolescents with identified impaired autonomic activity.
Regarding methylphenidate treatment details, in the Negrao et al. (2011) study, the children were in receipt of methylphenidate for at least 10 days at a dosage of 10 mg, except one child who was prescribed 20 mg. Buchhorn, Müller et al. (2012), Buchhorn and Christian (2014) and Buchhorn (2014) did not state dose or duration of pharmacological treatments. In Buchhorn, Conzelmann et al. (2012), the mean daily methylphenidate dose was 0.8 ± 0.4 mg/kg/day. In the study conducted by Shim et al. (2015), the mean dose was 22.23 ± 8.93 mg (0.70 ± 0.20 mg/kg) during a 12-week period of intervention. In Buchhorn et al. (2020), the dosage was <0.5 mg/kg in 52.6%, between 0.5 mg/kg and 0.9 mg/kg in 31.6%, and >0.9 mg/kg in 15.8% of the children over a mean interval of 283 days after methylphenidate treatment onset.
Qualitative Analysis
Negrao et al. (2011) reported significant differences in HRV between stimulant-free children with ADHD and the control group. The root mean square of successive differences between normal heartbeats (RMSSD), Poincaré plot standard deviation perpendicular to the line of identity (SD1), Poincaré plot standard deviation along the line of identity (SD2), and RR triangular index were higher in children with ADHD. Alternatively, different data were recognized regarding the comparison between children with ADHD under methylphenidate treatment and the control group. Only the SD2 index was significantly greater in the children with ADHD under methylphenidate treatment. When comparing children with ADHD before versus after methylphenidate treatment, the authors observed that only the RR triangular index decreased for ADHD under methylphenidate intervention. The authors determined that methylphenidate assisted the restoration of control HRV in children with ADHD (Negrao et al., 2011).
Buchhorn, Conzelmann et al. (2012) reported that children with ADHD with no methylphenidate demonstrated lower HRV compared to children in the control group (RMSSD: 26 ± 4 milliseconds (ms) vs. 44 ± 10 ms, p ≤ .0001; percentage of adjacent RR intervals with a difference of duration greater than 50 ms (pNN50): 6.5 ± 2.7% vs. 21.5 ± 9.0%, p ≤ .0001). The authors recognized that methylphenidate improved the same indices in children with ADHD (RMSSD: 36 ± 8 ms; pNN50: 14.2 ± 6.9%), indicating a beneficial impact of methylphenidate on HRV.
Buchhorn, Müller et al. (2012) discovered a higher HRV in children and adolescents with ADHD with methylphenidate versus children with ADHD without methylphenidate (pNN50: ADHD without methylphenidate: 6.5 ± 2.7 vs. ADHD with methylphenidate: 14.2 ± 6.9, p < .001; RMSSD: ADHD without methylphenidate: 26.1 ± 4.1 vs. ADHD with methylphenidate: 36.7 ± 8.3, p < .001). The authors highlight the advantageous impact of methylphenidate on HRV in children and adolescents with ADHD.
Buchhorn and Christian (2014) recognized the inverse correlation between premature ventricular contractions and RMSSD in children with ADHD prescribed methylphenidate. Yet, the authors recommended that clinical caution is warranted when treating children with ADHD with cardiac rhythm dysfunctions and detected no increase in ventricular arrhythmias in children with ADHD receiving methylphenidate.
Buchhorn (2014) identified that children with ADHD with or without methylphenidate versus the control group resulted in lower pNN50 (10.3 ± 1.0 vs. 3.4 ± 0.3, p < .0001 and 6.8 ± 0.7, p = .008) and reduced RMSSD (44 ± 2 vs. 26 ± 1, p < .0001 and 37 ± 2, p = .008). Shim et al. (2015) reported diminished RMSSD (47.65 ± 25.12 vs. 38.88 ± 17.94; p = .018) and high frequency (HF) (6.14 ± 0.97 vs. 5.7 ± 1.22; p = .043) after methylphenidate intervention in children with ADHD, indicating that cardiac parasympathetic control in participants with ADHD might be affected by methylphenidate intervention. Buchhorn et al. (2020) suggested that inappropriate sinus tachycardia in adolescents with ADHD is linked to stimulant treatment. Still, methylphenidate treatment was theorized to have no significant effect on autonomic balance owing to the lack of heart rate changes.
Analysis of the Risk of Bias
Based on our assessment, the risk of bias across the included studies was heterogeneous and generally high (Figure 2). Table 2 summarizes the risk of bias judgments according to the Cochrane risk of bias domains.
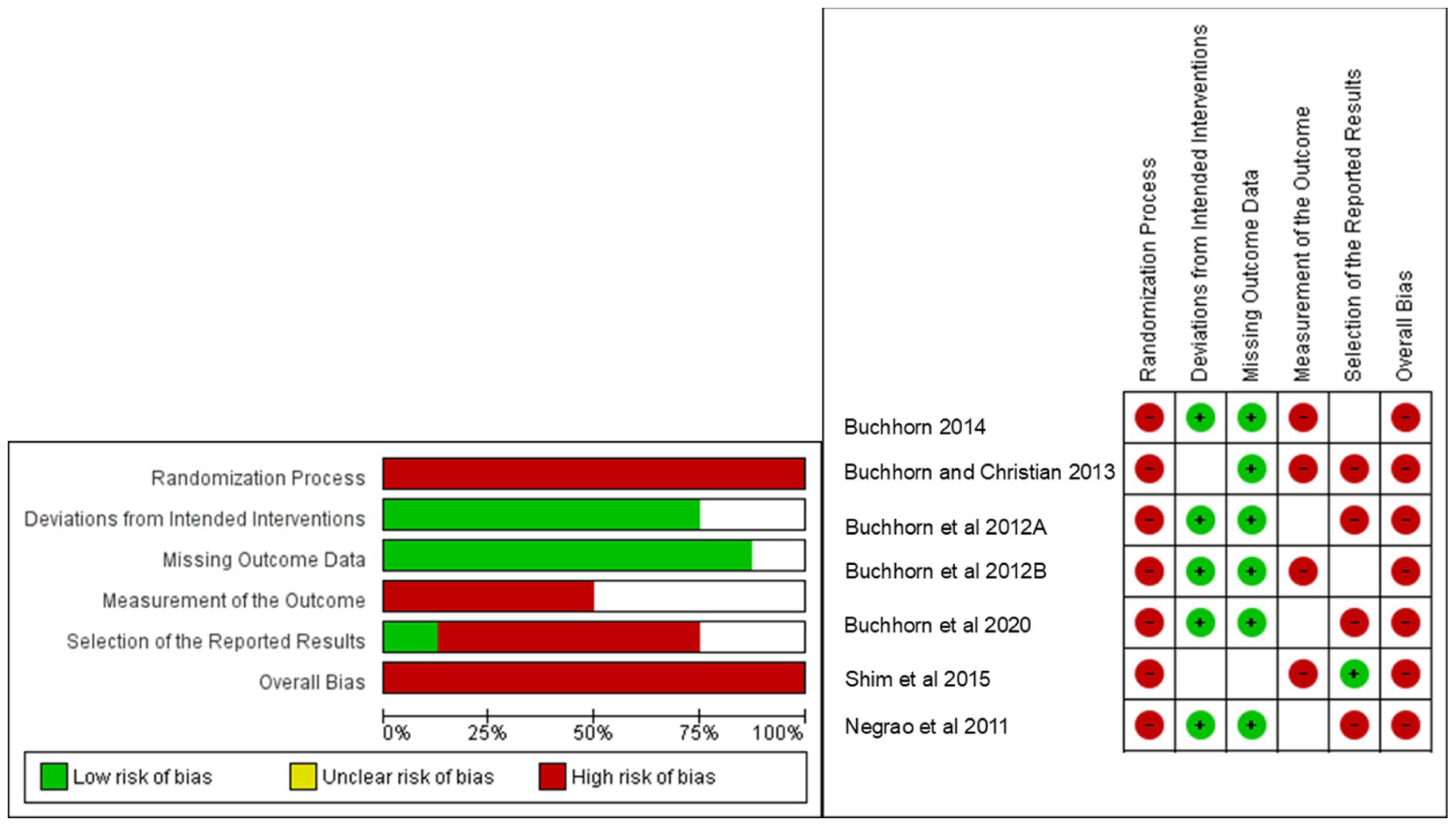
Cochrane risk of bias tool.
Cochrane Risk of Bias Tool.
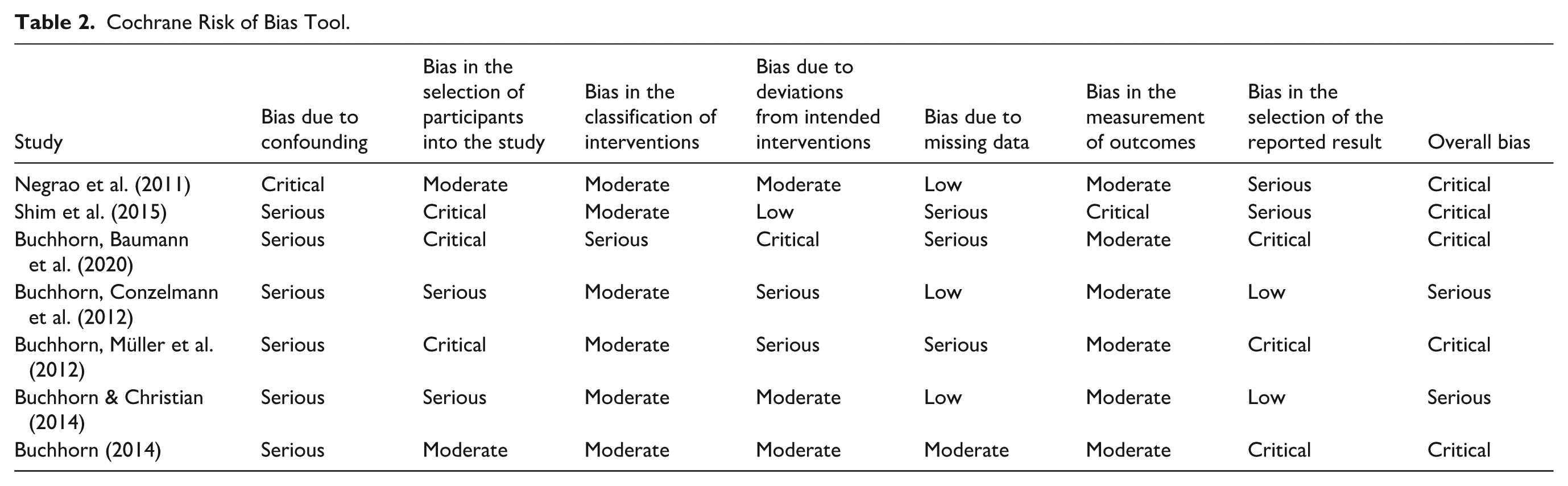
Bias Due to Confounding
Most studies presented important concerns related to confounding. One reference was judged as having critical risk, while the remaining studies were classified predominantly as serious risk of bias due to confounding, indicating limited control of prognostic factors that could influence the outcomes.
Bias in Selection of Participants Into the Study
Substantial concerns were observed in this domain. Several studies were rated as having serious or critical risk of bias because participants were selected from non-randomized clinical or observational samples, often without a clearly described recruitment process or evidence that eligible participants were included consecutively. In some studies, children already receiving methylphenidate were compared with untreated ADHD participants or non-ADHD controls, which may have introduced baseline differences related to disease severity, treatment indication, cardiovascular status, or clinical follow-up. In addition, several studies had small sample sizes and limited information on participant flow, exclusions, and losses before HRV assessment. These characteristics may have affected the comparability of study groups and increased the likelihood that the included participants were not representative of the target population.
Bias in Classification of Interventions
The majority of studies demonstrated a moderate risk of bias in the classification of interventions, while a smaller number were rated as serious. This judgment was mainly due to the incomplete specification of treatment conditions in the methods rather than clear evidence of incorrect classification. Several studies did not fully report methylphenidate formulation, dose, treatment duration, timing of HRV assessment in relation to medication intake, treatment stability, or adherence monitoring. In addition, because most studies used non-randomized or observational designs, intervention status was often based on clinical treatment history rather than prospective allocation according to a standardized protocol. These limitations introduced uncertainty regarding whether participants were consistently and accurately classified as exposed or unexposed to methylphenidate.
Bias Due to Deviations From Intended Interventions
Risk in this domain varied across studies, ranging from low to critical. Studies were judged as having lower risk when methylphenidate exposure and HRV assessment appeared to follow the intended comparison without evidence of relevant deviations. However, serious or critical concerns were identified when studies did not clearly report whether participants maintained stable methylphenidate use throughout the assessment period, whether dose changes occurred, whether adherence was monitored, or whether participants received concomitant interventions that could influence autonomic function. In some studies, the timing of HRV measurement in relation to methylphenidate administration was not clearly standardized, which may have affected the estimated intervention effect. The absence of blinding in most studies also increased the possibility that participant behavior, clinical management, or outcome assessment conditions differed between groups.
Bias Due to Missing Data
Most studies were judged as having low or moderate risk of bias due to missing data because outcome data appeared to be largely available for the participants included in the HRV analyses. However, a few studies presented serious concerns because participant exclusions, losses before HRV assessment, or unavailable HRV outcomes were incompletely described. In these studies, it was not always clear whether missing data were related to intervention status, baseline cardiovascular/autonomic characteristics, or technical limitations in HRV recording. No study clearly reported the use of formal imputation methods for missing HRV outcome data; therefore, the judgments were mainly based on the completeness and transparency of reported participant flow and outcome availability.
Bias in Measurement of Outcomes
Outcome measurement was generally considered moderate risk across most studies, although some were rated as critical. These findings suggest that, despite using appropriate measurement methods, outcome assessment may have been influenced by methodological limitations.
Bias in Selection of the Reported Result
This domain raised substantial concerns. Several studies were judged as having a critical risk of bias, indicating selective reporting or a lack of clarity regarding pre-specified analysis plans. Only a minority of references showed low risk in this domain.
Overall Bias
Taking all domains into account, the overall risk of bias was rated as critical for most studies, with a smaller number classified as serious. No study achieved an overall low or moderate risk of bias. This overall judgment was driven by recurrent methodological limitations across several ROBINS-I domains, particularly confounding, participant selection, deviations from intended interventions, and selection of the reported result. The main concerns included lack of randomization, limited control for baseline prognostic factors, incomplete description of recruitment procedures, small and clinically heterogeneous samples, unclear treatment stability or adherence, incomplete reporting of methylphenidate dose and duration, and absence of pre-specified analysis plans. These limitations were not isolated to a single study or domain but appeared repeatedly across the included evidence base, reducing confidence in the estimated effects of methylphenidate on HRV outcomes.
Quantitative Analysis
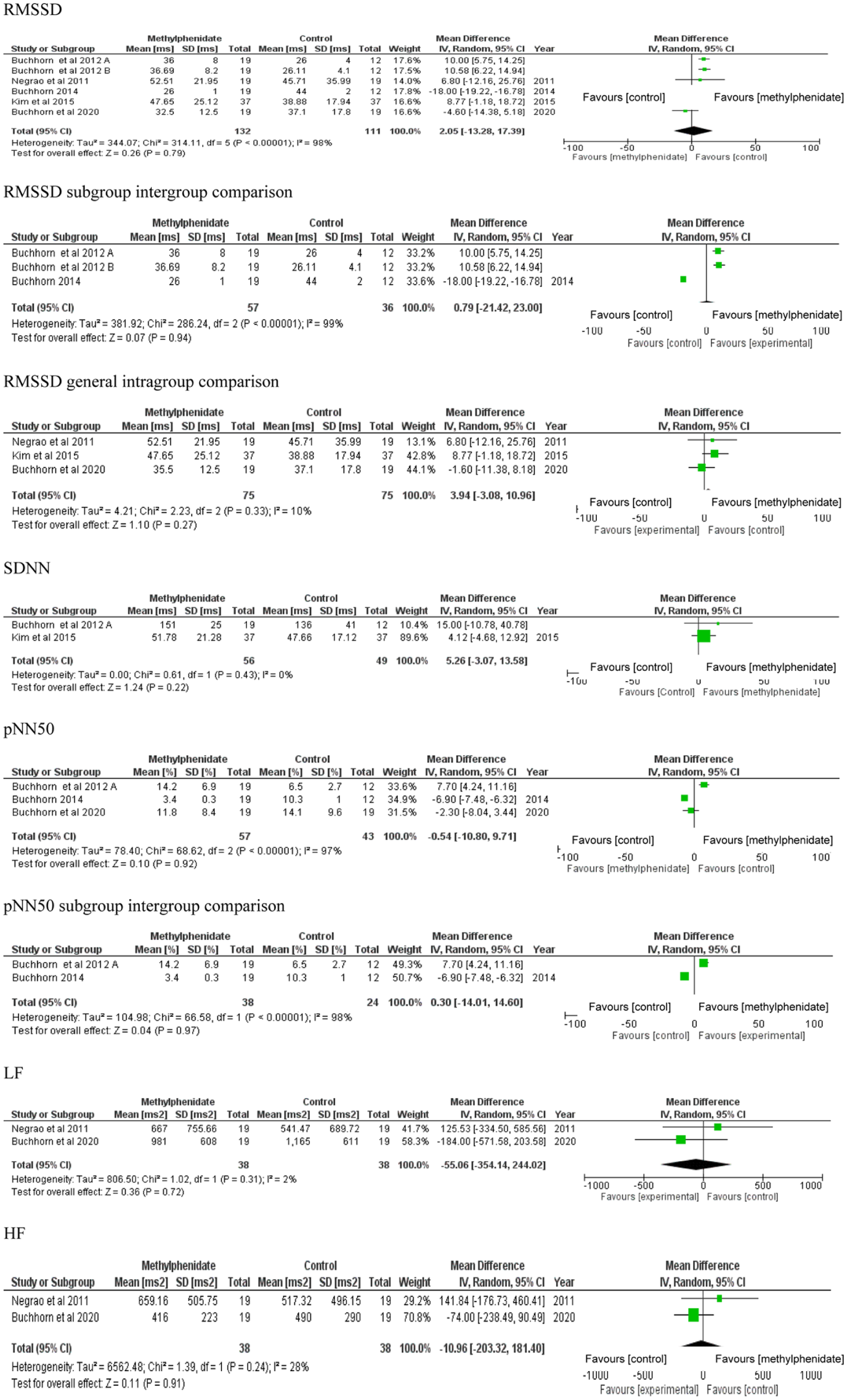
We used a random-effects model with mean difference (MD) as the effect measure to estimate pooled effects for RMSSD, standard deviation of all normal RR intervals (SDNN), percentage of adjacent RR intervals differing by more than 50 ms (pNN50), low-frequency power (LF), and high-frequency power (HF) HRV indices. In the forest plots, the black diamond represents the pooled effect estimate and its 95% confidence interval (CI). Negative effect estimates indicate higher values in the intervention group compared with the control group (Figure 3).
Meta-analysis for overall effects of methylphenidate on HRV indexes.
General group; Subgroup–Intergroup comparison; Subgroup–Intragroup comparison. HRV = heart rate variability; RMSSD = root mean square of differences between adjacent normal RR intervals/meta-analysis for overall effects of methylphenidate on SDNN HRV index. HRV = heart rate variability; SDNN = standard deviation of all normal RR intervals/meta-analysis for overall effects of methylphenidate on pNN50 HRV index. General group; Subgroup–Intergroup comparison. HRV = heart rate variability; pNN50 = percentage of adjacent RR intervals with a difference of duration greater than 50 ms/meta-analysis for overall effects of methylphenidate on LF HRV index. HRV = heart rate variability. LF = low frequency/meta-analysis for overall effects of methylphenidate on HF HRV index. HRV = heart rate variability; HF = high frequency.
RMSSD
Regarding RMSSD, we identified no significant changes. In the test for overall effect, the pooled mean difference was 2.05 ms (95% CI: −13.28 to 17.39; p = .79), with substantial heterogeneity (I2 = 98%) (Figure 3). In the intergroup comparison subgroup, no significant difference was observed: MD = 0.79 ms (95% CI: −21.42 to 23.00; p = .94), with substantial heterogeneity (I2 = 99%) (Figure 3). In the intragroup comparison subgroup, no significant difference was observed: MD = 3.94 ms (95% CI: −3.08 to 10.96; p = .27), with low heterogeneity (I2 = 10%) (Figure 3). The GRADE certainty of evidence for RMSSD was very low ⨁◯◯◯ because of serious risk of bias, absence of random allocation and blinding in the included studies, incomplete reporting of baseline differences and missing data handling, substantial heterogeneity, and imprecision due to wide confidence intervals crossing the null effect (Table 3).
Levels of Evidence Analysis Via (The GRADE Working Group, 2004).
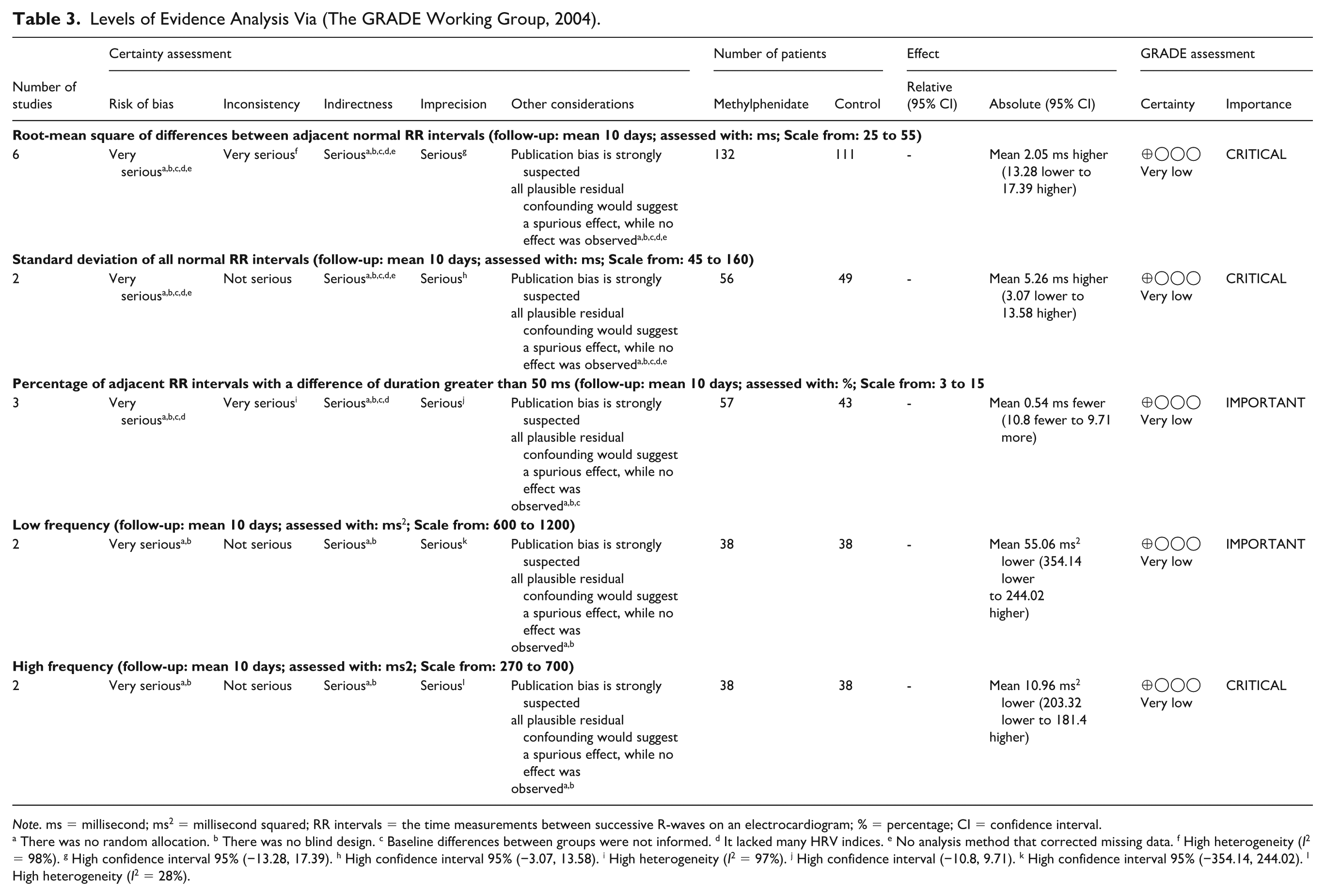
Note. ms = millisecond; ms2 = millisecond squared; RR intervals = the time measurements between successive R-waves on an electrocardiogram; % = percentage; CI = confidence interval.
There was no random allocation. b There was no blind design. c Baseline differences between groups were not informed. d It lacked many HRV indices. e No analysis method that corrected missing data. f High heterogeneity (I2 = 98%). g High confidence interval 95% (−13.28, 17.39). h High confidence interval 95% (−3.07, 13.58). i High heterogeneity (I2 = 97%). j High confidence interval (−10.8, 9.71). k High confidence interval 95% (−354.14, 244.02). l High heterogeneity (I2 = 28%).
SDNN
We observed no significant change in SDNN. In the “test for overall effect,” we observed a subtotal = 5.26 ms [95% CI: −3.07, 13.58], p = .22, and heterogeneity = 0% (Figure 3). The GRADE quality of evidence analysis was very low ⨁◯◯◯ (Table 3).
PNN50
Concerning the pNN50 index, we also observed no significant variation. In the test for overall effect, the pooled mean difference was −0.54 ms (95% CI: −10.80 to 9.71; p = .92), with substantial heterogeneity (I2 = 97%) (Figure 3). In the intergroup comparison subgroup, no significant difference was observed: MD = 0.30 ms (95% CI: −14.01 to 14.60; p = .97), with substantial heterogeneity (I2 = 98%) (Figure 3). The GRADE certainty of evidence for pNN50 was very low ⨁◯◯◯ because of serious risk of bias, absence of random allocation and blinding in the included studies, incomplete reporting of baseline differences and missing data handling, substantial heterogeneity, and imprecision due to wide confidence intervals crossing the null effect (Table 3).
LF
With reference to LF, we identified no significant change. In the test for overall effect, the pooled mean difference was −55.06 ms² (95% CI: −354.14 to 244.02; p = .72), with low heterogeneity (I2 = 2%) (Figure 3). The GRADE certainty of evidence for LF was very low ⨁◯◯◯ because of serious risk of bias, absence of random allocation and blinding in the included studies, incomplete reporting of baseline differences and missing data handling, and imprecision due to the very wide 95% confidence interval crossing the null effect (Table 3).
HF
We identified no significant change in HF. In the test for overall effect, the pooled mean difference was −10.96 ms² (95% CI: −203.32 to 181.40; p = .91), with low-to-moderate heterogeneity (I2 = 28%) (Figure 3). The GRADE certainty of evidence for HF was very low ⨁◯◯◯ because of serious risk of bias, absence of random allocation and blinding in the included studies, incomplete reporting of baseline differences and missing data handling, and imprecision due to the wide 95% confidence interval crossing the null effect (Table 3). Potential publication bias was considered qualitatively as part of the overall certainty of evidence assessment, in accordance with GRADE guidance. Formal statistical tests for publication bias were not performed due to the limited number of included studies.
Discussion
The present systematic review and meta-analysis aimed to evaluate whether methylphenidate use is associated with alterations in HRV, a well-established surrogate of cardiac autonomic and cardiovascular regulation (Sassi et al., 2015; Vanderlei et al., 2009). This hypothesis was grounded in the psychostimulant profile of methylphenidate, which enhances central dopaminergic and noradrenergic neurotransmission (Curatolo et al., 2009; Purper-Ouakil et al., 2011) and could theoretically increase sympathetic drive and reduce parasympathetic modulation, leading to lower HRV values at rest.
Neurobiological Context and Interpretation of HRV Findings
Contrary to the initial physiological hypothesis, the overall evidence did not show clinically meaningful changes in resting cardiac autonomic regulation associated with methylphenidate use. In practical terms, measures commonly used to assess autonomic balance at rest did not differ significantly between children and adolescents with ADHD treated with methylphenidate and comparison conditions.
From a clinical perspective, these findings suggest that the central stimulant effects of methylphenidate do not necessarily translate into detectable alterations in resting cardiac autonomic function. However, this conclusion should be interpreted with caution, as the available evidence is limited by methodological weaknesses and very low certainty, which may mask subtle or context-dependent autonomic responses.
Considering that methylphenidate is prescribed in children and adolescents with ADHD (Bellato et al., 2025) and that earlier data indicated cardiovascular disorders related to ADHD (Thapar et al., 2023), our main interest in this study was to provide the foundations of cardiovascular and autonomic risks induced by methylphenidate. In line with this therapeutic rationale, the American Association of Nurse Practitioners® (American Association of Nurse Practitioners, 2023) emphasizes that prescribing, including medications such as methylphenidate, falls inherently within the professional scope of nurse practitioners and should be regulated exclusively by state boards of nursing, ensuring that such treatments are provided in accordance with nursing practitioner, certification, and the delivery of timely and high-quality health care.
The rationale for investigating HRV in this context is grounded in neurobiological and clinical evidence indicating that ADHD is associated with dysfunction in fronto-subcortical circuits, which play a central role in autonomic and cardiovascular regulation (Arnsten & Li, 2005; Del Campo et al., 2011). Neuroimaging and neuropsychological studies have consistently implicated impairments in prefrontal cortical networks, which are modulated by catecholaminergic neurotransmission, particularly dopamine and noradrenaline (Arnsten & Li, 2005; Curatolo et al., 2009; Del Campo et al., 2011; Purper-Ouakil et al., 2011). Methylphenidate, by inhibiting the reuptake of these monoamines, enhances prefrontal cortical signaling and is highly effective in improving core ADHD symptoms (Belatto et al., 2024). From a physiological standpoint, such central stimulation could plausibly translate into increased sympathetic activity or reduced parasympathetic modulation, thereby altering HRV (Thapar et al., 2023). The absence of consistent changes in HRV observed in this meta-analysis, therefore, warrants careful interpretation.
Parasympathetic (vagal) HRV indices, particularly RMSSD and HF power, primarily reflect short-term beat-to-beat variability mediated by vagal efferent activity to the sinoatrial node, which clinically reflects the heart’s ability to adapt to stress and maintain cardiovascular stability. Physiologically, these indices are considered robust markers of cardiac parasympathetic modulation and are closely linked to adaptive cardiovascular regulation and stress resilience. Clinically relevant reductions in RMSSD or HF are typically interpreted as diminished vagal tone and have been associated with elevated cardiovascular risk, impaired emotional regulation, and increased all-cause mortality in both clinical and non-clinical populations (Sassi et al., 2015; de Oliveira et al., 2024). In the context of methylphenidate use, a reduction in vagal HRV would be consistent with heightened sympathetic dominance secondary to increased central catecholaminergic signaling. However, the absence of significant changes in RMSSD and HF observed in this meta-analysis suggests that enhanced prefrontal catecholamine availability does not translate into clinically meaningful suppression of parasympathetic cardiac control at rest. This finding supports the notion that prefrontal cortical modulation of behavior and attention may be functionally dissociable from peripheral vagal regulation under basal conditions.
In this context, overall heart rate variability is commonly used as an indicator of how effectively the cardiovascular system adapts to internal and external demands, reflecting the integrated influence of sympathetic and parasympathetic activity over time (Sassi et al., 2015; de Oliveira et al., 2024). Clinically, lower values of global autonomic variability have been associated with increased cardiovascular morbidity, autonomic dysfunction, and poorer prognostic outcomes (Sassi et al., 2015; de Oliveira et al., 2024).
In the present analysis, methylphenidate use was not associated with clinically meaningful changes in global autonomic variability, suggesting that resting cardiovascular adaptability remains preserved in children and adolescents with ADHD receiving this medication. However, this finding should not be interpreted as definitive evidence of cardiovascular risk, safety or long-term safety. HRV represents an intermediate physiological marker rather than a hard clinical endpoint (Sassi et al., 2015; Vanderlei et al., 2009). In contrast, traditional cardiovascular outcomes—such as blood pressure, resting heart rate, arrhythmias, and major adverse cardiovascular events—provide more direct and clinically actionable measures of cardiovascular risk (Fox et al., 2007; Lewington et al., 2002). Previous meta-analytic evidence indicates that psychostimulant therapies, including methylphenidate, may be associated with small but statistically significant increases in systolic and diastolic blood pressure and heart rate (Hennissen et al., 2017). Although these hemodynamic changes are often modest when considered in isolation, they may be more relevant to long-term cardiovascular risk accumulation than isolated resting measures of autonomic variability.
One plausible explanation for the absence of significant findings is that the central effects of methylphenidate on attention and cognition may not be directly reflected in resting measures of cardiac autonomic function. Measures of HRV obtained under resting conditions primarily represent baseline autonomic regulation and may be relatively insensitive to subtle or centrally mediated pharmacological influences (Sassi et al., 2015). It is therefore possible that the autonomic effects of methylphenidate are context-dependent and become more evident during situations that place greater demands on the autonomic system, such as physical activity, psychological stress, or cognitive challenge, conditions that were not systematically examined in the included studies. Consequently, the lack of observable changes in resting autonomic measures does not rule out altered autonomic responsiveness in children and adolescents treated with methylphenidate.
Strengths and Limitations
This systematic review and meta-analysis have several strengths. We used a comprehensive search strategy across multiple databases, followed PRISMA recommendations, assessed risk of bias using ROBINS-I, and evaluated the certainty of evidence using the GRADE framework. In addition, when possible, quantitative synthesis was performed using random-effects models, and subgroup analyses were conducted to distinguish intergroup from intragroup comparisons.
However, some limitations of the present review should be considered. First, the small number of eligible studies limited the statistical power of the meta-analysis and restricted the possibility of conducting more detailed subgroup or sensitivity analyses. Second, the included studies differed in design, comparison groups, HRV assessment protocols, methylphenidate exposure characteristics, and reported outcomes, which contributed to clinical and methodological heterogeneity. Third, because dosing regimens, treatment duration, and timing of HRV assessment were inconsistently reported, we were unable to explore dose–response effects or the influence of short-versus long-term methylphenidate exposure. Fourth, publication bias could not be formally assessed because of the limited number of studies included in each pooled analysis. Finally, most available evidence came from a small number of research groups and geographic settings, which may limit the generalizability of the findings to broader pediatric ADHD populations.
Therefore, although this review provides a structured synthesis of the available evidence, the findings should be interpreted cautiously. The absence of significant pooled effects should not be considered definitive evidence of no autonomic effect, but rather as an indication that current evidence remains limited, heterogeneous, and insufficiently powered to detect small or context-dependent changes in HRV.
Furthermore, the assessment of publication bias was limited by the small number of available studies, precluding formal statistical testing. Another critical limitation concerns the generalizability of the evidence. Five of the seven included studies were conducted by the same research group in Germany, raising concerns about institutional bias and homogeneity in methodological approaches and analytical decisions. While this consistency may enhance internal coherence, it limits external validity and reduces confidence that the findings are applicable to broader and more diverse populations. Moreover, this geographic concentration highlights important health equity considerations. The predominance of data from a single high-income country restricts representation of populations from varied socioeconomic, ethnic, and health care contexts, potentially overlooking differences in baseline cardiovascular risk, access to care, and treatment responses in underrepresented or underserved groups.
Despite these limitations, the findings of the present review are broadly consistent with existing cardiovascular safety literature on methylphenidate. Prior systematic reviews and meta-analyses have reported that, although psychostimulants may be associated with small increases in heart rate and blood pressure, methylphenidate generally exhibits a favorable cardiovascular safety profile (Nanda et al., 2023). Notably, previously reported changes in systolic blood pressure have been statistically significant but modest in magnitude and are often considered clinically negligible in otherwise non-ADHD pediatric populations (Hennissen et al., 2017). Our findings extend this literature by suggesting that resting autonomic cardiac regulation, as indexed by HRV, is not substantially disrupted by methylphenidate treatment.
Implications for Nursing Practice, Research, and Education
From a nursing perspective, the findings of this review provide preliminary reassurance regarding the autonomic cardiac safety of methylphenidate in children and adolescents with ADHD, particularly under resting conditions. In practical terms, commonly used indices of resting autonomic modulation did not indicate clinically meaningful disturbances in cardiac autonomic control among individuals receiving this medication. This finding is clinically relevant given long-standing concerns that psychostimulant-induced sympathoexcitation could translate into measurable alterations in cardiac autonomic regulation (Thapar et al., 2023).
Nevertheless, these findings must be interpreted with substantial caution. Although pooling was performed whenever outcomes were sufficiently comparable, the certainty of evidence for all autonomic outcomes was rated as very low because of high risk of bias, the small number of studies and participants available for each pooled analysis, heterogeneous study designs, incomplete reporting of medication dose and treatment duration, substantial heterogeneity across several indices, and imprecision reflected by wide confidence intervals. Importantly, the absence of statistically significant changes in resting autonomic measures does not equate to definitive cardiovascular safety, nor does it exclude the possibility of subtle or context-dependent autonomic effects, such as those emerging during physiological stress, physical exercise, long-term exposure, or in clinically vulnerable subgroups.
From a clinical nursing standpoint, these results reinforce the importance of continued and systematic cardiovascular monitoring in children and adolescents treated with methylphenidate. Baseline assessment and periodic follow-up of blood pressure and resting heart rate remain essential, as these traditional cardiovascular parameters provide more direct and clinically actionable indicators of cardiovascular risk than autonomic measures alone. Nurses should remain particularly vigilant when caring for patients with pre-existing cardiovascular risk factors, comorbid conditions, or a family history of cardiac disease. HRV should be regarded as an intermediate physiological marker rather than a hard clinical endpoint, and preserved resting autonomic modulation does not exclude the presence of meaningful hemodynamic or electrophysiological alterations.
In addition, it is important to note that, according to the American Association of Nurse Practitioners®, prescribing medications such as methylphenidate falls intrinsically within the professional scope of nurse practitioners. This prescriptive authority, regulated exclusively by state boards of nursing and aligned with formal training and certification, supports the delivery of timely, cost-effective, and high-quality care while underscoring the central role of nurses in pharmacological management and cardiovascular surveillance (American Association of Nurse Practitioners, 2023).
Prescribing and monitoring practices by psychiatric mental health nurse practitioners (PMHNPs) should be guided by individualized risk–benefit assessments that integrate symptom severity, functional improvement, cardiovascular profile, medication efficacy, adverse effects, and patient and family preferences. Because PMHNPs may be directly involved in both prescribing methylphenidate and monitoring treatment response and side effects, vigilant longitudinal follow-up is warranted, particularly given the predominance of non-randomized and open-label studies in the current evidence base. Well-designed, double-blind, placebo-controlled trials with standardized dosing regimens, longer follow-up periods, and comprehensive cardiovascular outcomes are urgently needed to clarify the autonomic and cardiovascular safety profile of methylphenidate in pediatric populations with ADHD. Future research should prioritize rigorously designed randomized controlled trials with adequate sample sizes, standardized heart rate variability measurement protocols, and assessments conducted under dynamic or stress conditions, which may provide deeper insights into context-dependent autonomic effects beyond resting states.
Conclusion
In conclusion, the available evidence suggests that methylphenidate use is not associated with clinically meaningful alterations in resting cardiac autonomic regulation in children and adolescents with ADHD. In practical terms, measures commonly used to evaluate autonomic balance at rest did not indicate impaired cardiac regulation among those receiving this medication. These findings offer preliminary reassurance regarding autonomic cardiac safety under resting conditions.
Nevertheless, this apparent preservation of autonomic function should not be interpreted as definitive evidence of cardiovascular neutrality or long-term safety. Autonomic measures represent intermediate physiological indicators and do not replace established clinical outcomes such as blood pressure, resting heart rate, or cardiovascular events. From a clinical perspective, these results underscore the importance of continued cardiovascular monitoring, particularly in children and adolescents with pre-existing risk factors, while highlighting that current evidence is insufficient to support changes in prescribing practices based solely on autonomic findings. From a research standpoint, well-designed randomized studies with standardized autonomic assessment methods, clearly reported dosing regimens, and evaluations under conditions of physiological or psychological stress are needed to better clarify the cardiovascular and autonomic effects of methylphenidate in ADHD populations.
Supplemental Material
sj-docx-1-jap-10.1177_10783903261456725 – Supplemental material for Effect of Methylphenidate on Heart Rate Variability in Children and Adolescents With ADHD: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-jap-10.1177_10783903261456725 for Effect of Methylphenidate on Heart Rate Variability in Children and Adolescents With ADHD: A Systematic Review and Meta-Analysis by Sílvia H. S. Gianini, Andrey A. Porto, Rodrigo D. Raimundo, Ingrid S. de Souza, David M. Garner and Vitor E. Valenti in Journal of the American Psychiatric Nurses Association
Footnotes
Acknowledgements
We sincerely thank Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) for providing essential infrastructure and financial support, which were instrumental in conducting this study. Their commitment to fostering scientific research has been invaluable to our work.
Ethical Considerations
This study is a systematic review and meta-analysis based exclusively on data extracted from previously published studies. Therefore, no new data were collected from human participants, and no direct involvement of patients, participants, or animals occurred. For this reason, approval by an institutional ethics committee was not required.
Consent to Participate
Informed consent was not applicable to this study, as it did not involve the recruitment of participants or the collection of individual-level primary data. All analyses were conducted using data already available in the published literature.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Vitor E. Valenti receives financial support from the National Council for Scientific and Technological Development, an entity linked to the Ministry of Science, Technology, Innovations and Communications from Brazil (Process number 302574/2021-2).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No new primary data were generated in this study. All data analyzed in this systematic review and meta-analysis were extracted from previously published studies cited in the manuscript. The data supporting the findings of this study are included in the article and its supplementary materials. Additional information may be made available by the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Any Other Identifying Information Related to the Authors and/or Their Institutions,Funders,Approval Committees,etc. That Might Compromise Anonymity
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.