
Abstract
Implications for Knowledge Translation
Self-care management is very important in managing diabetes mellitus. Adherence to self-care management mobile applications for diabetes may lead to increased knowledge about the disease, complications, and various aspects of self-management. Using self-care management mobile applications could lead to improved patient confidence in managing the disease, and better commitment to and performance of self-care activities.
Diabetes mellitus (DM) is a metabolic disease that causes hyperglycemia, which may cause serious and long-term complications (American Diabetes Association [ADA], 2014). The International Diabetes Federation (IDF) estimated the prevalence of Type 1 Diabetes (T1DM) among children and adolescents younger than 21 years as 1,106,200 worldwide (IDF, 2017). In Jordan in 2016, DM affected about 13.1% of adults and was the sixth leading cause of death, responsible for 7% of deaths among all ages (World Health Organization [WHO], 2016).
DM can have serious complications that affect patients’ quality of life (Stojanović et al., 2018). Lifestyle modifications are needed in order to prevent or delay these complications. The ADA's recommended lifestyle management for patients with DM includes education and support in self-management to help patients make decisions regarding their treatment plan, perform various self-care management activities, solve problems, and collaborate with health-care professionals to achieve better health outcomes and quality of life (ADA, 2017).
Various diabetes self-management support approaches may improve patients’ self-efficacy (SE), self-care agency (SCA), and self-care management (SCM). One of these approaches is mobile health (m-health), which is considered an easy, practical, and familiar method for all age groups (David & Rafiullah, 2016). Using mobile applications (apps) can be an effective way to improve patients’ knowledge about their disease, and consequently their SE and SCA, and can encourage active participation in and adherence to self-management and treatment plans (David & Rafiullah, 2016).
A literature review found limited studies of levels of SE, SCA, and SCM among patients with DM, and studies investigating patients with T1DM were even more scarce. Based on The Jordanian Database for Nursing Research (School-of-Nursing-JU, 2017), the current study is the first conducted in Jordan to investigate the effect of using a diabetes self-management mobile app on SE, SCA, and SCM among patients with T1DM.
Study Purpose
The purpose of this study was to explore the effect of using a diabetes self-management mobile app on SE, SCA, and SCM among Jordanian patients with T1DM. Figure 1 shows the research questions:
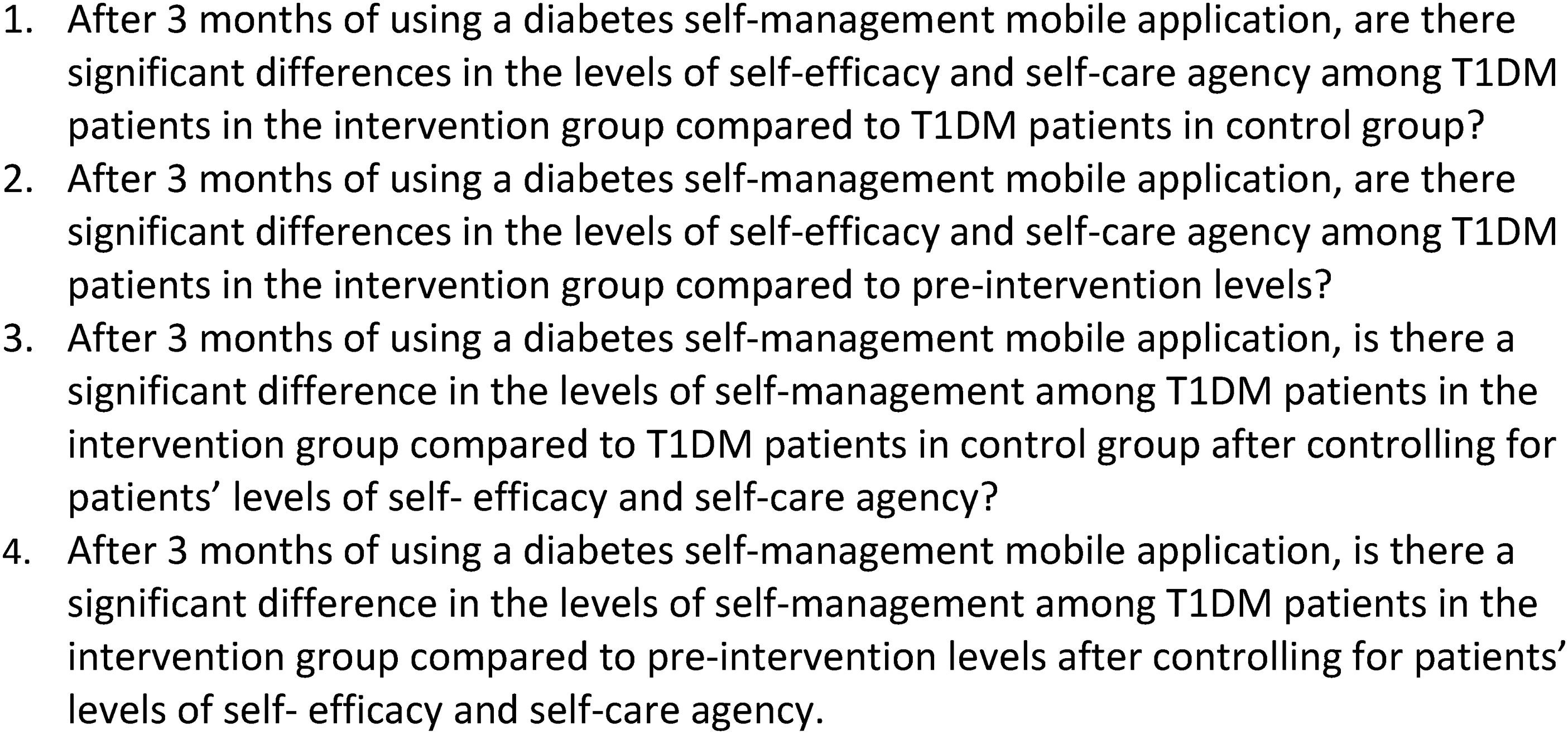
Research questions.
Methodology
Design
This study utilized a nonequivalent control group quasi-experimental design. Participants enrolled in the control group (CG) received the usual care provided by their health-care providers, whereas intervention group (IG) participants used the mobile app besides receiving usual care. Data were collected at baseline and post intervention at three-month follow-up.
Sample and Setting
The target population included all Jordanian adult patients with T1DM. However, the accessible population was a non-probability convenience sample of Jordanian patients with T1DM who visited outpatient clinics at a major public hospital in Amman, and Jordanian patients with T1DM approached through social media. Inclusion criteria were: 18 to 30 years old, able to read and write Arabic, diagnosed with T1DM more than 6 months, and having a smartphone and able to use it. Exclusion criteria were: critically ill and/or unable to cooperate; any mental disabilities; and visual, auditory, or physical impairment.
Sample size was determined based on Cohen's Power Primer (Cohen, 1992). Using conventional power of .8, medium effect size of 0.25, and level of significance of .05 and ANOVA, the minimum sample size was 64 for each group of the two groups. Additional subjects were recruited for anticipated attrition, resulting in 150 subjects as a total sample. Figure 2 summarizes the sample recruitment procedure.
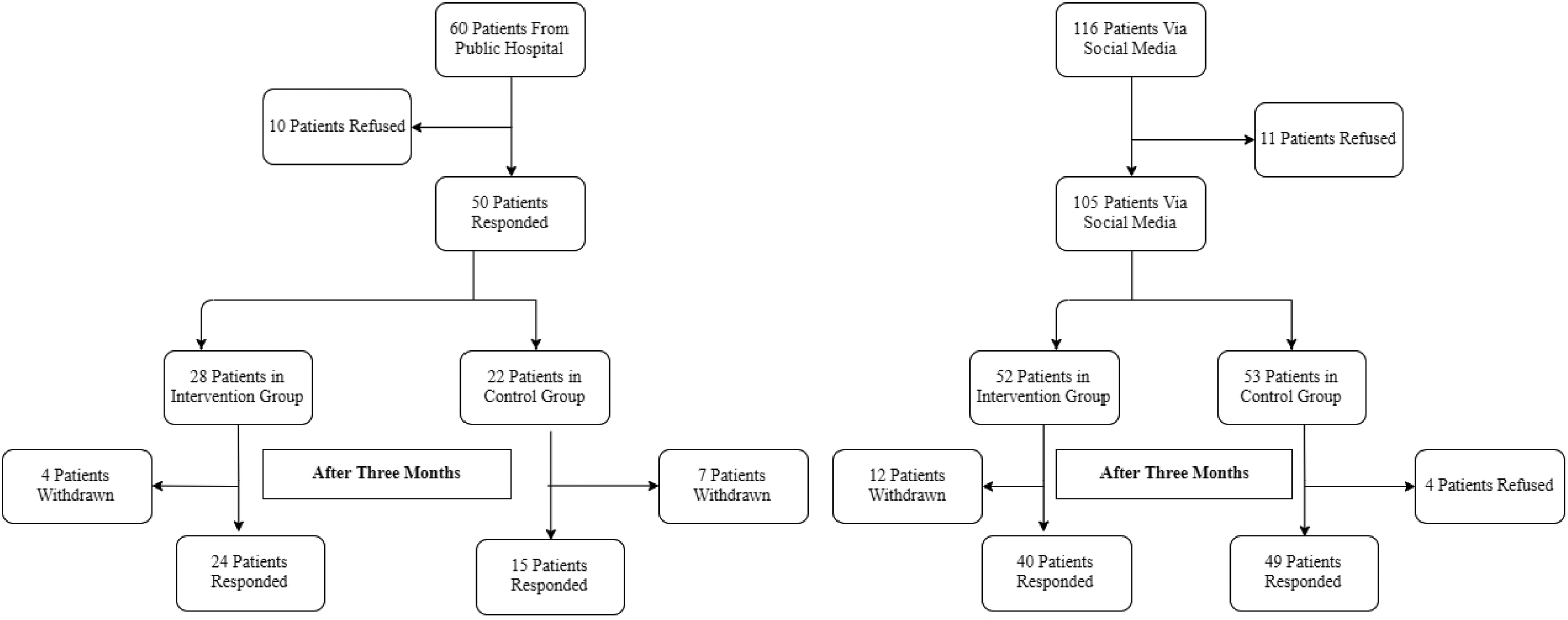
Sample recruitment procedure.
Intervention
The mobile app was developed by experts in programming for Android and iOS systems. It was posted on Play-Store and App-Store and can be played without an internet connection. It includes logs for blood glucose readings, and reminders and graphs for glucose that can be set. It also contains educational information about DM, including the disease; types of DM; complications and how to reduce the risk of developing them; DM management; medications, including Insulin; monitoring blood glucose levels; DM and hypertension; DM and fasting; and calories in various types of food. Pop-up messages appear twice daily with educational tips about various aspects of diabetes. Figure 3 shows a sample pop-up message.
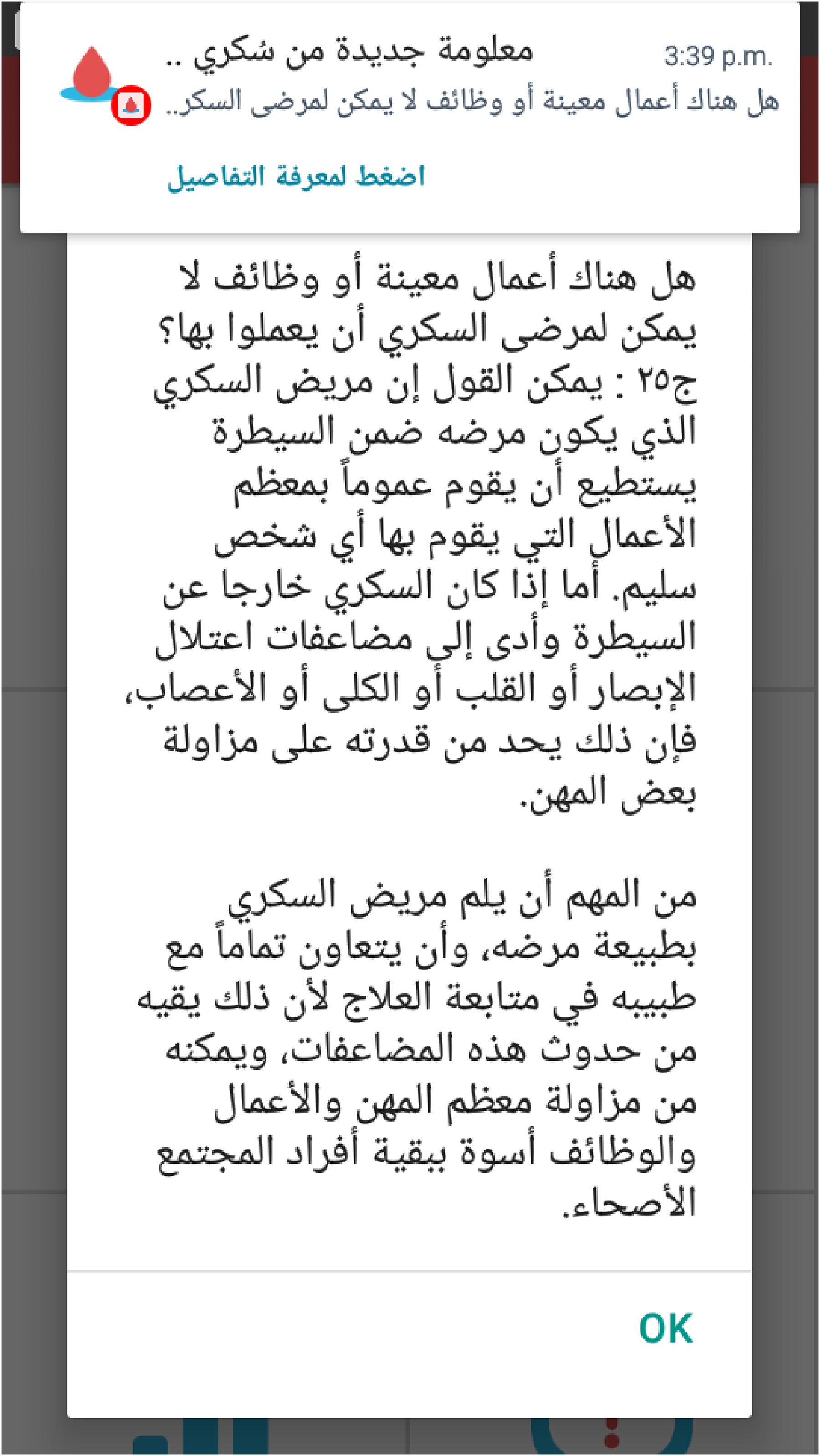
Sample pop-up message on app.
Validation of Content. The educational content, in Arabic, was obtained from a specialized center for diabetes, and was validated by two experts in DM with each subtitle evaluated for its relevance to currently used tools, ranked from 1 (not relevant) to 4 (very relevant) (Polit & Beck, 2006; Yaghmaie, 2003). Calculated Relevancy Index was 1.00 (range 0–1).
Instrument
The questionnaire in the current study consisted of four parts:
Demographics, Disease History and Diabetes Health Education, including any previous health education about DM, when was the last time, and the type of information provided. The Diabetes Self-Efficacy Scale (DSES; Sousa et al., 2009) measures patients’ level of confidence about performing specific activities and behaviors and managing their disease. It consists of 60 items, rating SE on a six-point Likert scale (0 = Strongly Disagree to 5 = Strongly Agree), with a possible score ranging from 0 to 300. Stronger agreement on each statement indicates higher SE. The Appraisal of Self-Care Agency Scale-Revised (ASAR-R; (Sousa et al., 2010) measures patients’ capability to perform self-care activities in managing their disease. SCA is rated on a five-point Likert scale (1 = Totally Disagree to 5 = Totally Agree), with a possible score ranging from 15 to 75; four items’ scores are reversed. Higher scores indicate higher levels of SCA (Sousa et al., 2009). The Diabetes Self-Management Scale (DSMS; Sousa et al., 2009) measures patients’ actual performance of specific activities and behaviors to manage their disease. The DSMS consists of the same 60 items as the DSES scale, with the same rating. The difference is that DSES measures patient's confidence in performing diabetes self-care management, and DSMS measures actual performance of these activities. Therefore, the DSMS rates self-care management on a six-point Likert scale (0 =Strongly Disagree to 5 = Strongly Agree) with a possible score ranging from 0 to 300. Stronger agreement on each statement indicates more adherence to self-care activities, and thus greater self-care management.
The Item-Level Content Validity Index (I-CVI) of DSMS for all items was higher than 0.78, except for one item, it was 0.7 (Sousa et al., 2009) (the minimum acceptable value is 0.78 (Lynn, 1986)). The Scale-Level Content Validity (S-CVI/Ave) was 0.96 (the minimum acceptable value is 0.9 (Lynn, 1986). The DSMS showed 100% inter-rater agreement for its clarity, except for two items. The DSMS gained support for its clarity, consistency, and content validity (Sousa et al., 2009).
Because Arabic is the native language of the study participants, the questionnaire was translated into the Arabic language according to WHO guidelines for translation (WHO, 2018). Then the questionnaire was reviewed by two experts in the fields of DM and self-management to ensure the content validity of the study instruments. Content Validity Index for the DSES was 0.97, for the DSMS was 0.98, and for the ASAR-R was 1.00, which are considered acceptable content validity indices (Polit & Beck, 2013; Yaghmaie, 2003).
Ethical Considerations
Institutional Review Board (IRB) approval was obtained from both the educational institution (19/2018/4865) and the public hospital (MOH REC 1800138). Filling out the questionnaire was considered agreement to participate. Participants were assured that participation was voluntary without any type of coercion.
Data Collection
After IRB approvals were obtained, the principal investigator (PI) approached physicians and nurses working in the endocrinology outpatient clinics in the public hospital in Amman, explaining the purpose and the procedure of the study. The PI asked the nurse who worked there most often to provide the eligible participants’ phone numbers (based on the inclusion criteria), after the nurse talked briefly with patients and got their preliminary assent to join the study.
The PI posted about the study on various Facebook groups, including Jordan universities’ groups. The information posted included the purpose of the study, what was required from participants, and ethical considerations of participation including confidentiality of the information provided. Participants who contacted the PI on Messenger were asked for their phone number and were called.
After attaining the preliminary assent from the clinic patients, the researcher phoned all the participants (recruited from the hospital and from Facebook), ensured that they met inclusion criteria, and explained the purpose of the study and what was required from them. The eligible participants were assigned to either the intervention or control groups; assignment was not random, and was based on patients’ choice or assignment to the opposite group from the previous entry.
Control Group
The PI phoned the participants of the CG, provided them with the questionnaire link on Google forms (the file size was too large to send by messenger or email), and asked them to complete the pretest questionnaire which comprised the demographics datasheets, the DSES, the ASAR-R, and the DSMS. After three months, participants in the CG were phoned and asked to fill out the questionnaire again.
Intervention Group
The PI phoned the participants of the IG, provided them with the questionnaire link on Google forms, and asked them to complete the pretest questionnaire which comprised the demographics datasheets, the DSES, the ASAR-R, and the DSMS. After they had completed the questionnaire, the principal investigator sent a link to a video explaining how to download the mobile app and how to use it, registering with username, password, and phone number. Then the researcher activated the account; this process decreased the possibility of participants in the CG using the app.
The patients in the IG were asked to record blood glucose readings on the app at least three times a day, and to read the educational information. In order to ensure consistency and effective use of educational materials, all participants in the IG were instructed how to access the elements of educational materials in the same order and the same time relative to beginning their participation (educational materials could not be accessed all at the same time). Articles appeared in phases (e.g., the first article showed up on Day 1 of participation; the second article after three days, to give time to read the first article). The PI contacted the IG participants by phone after two weeks to determine use of the app, get feedback, and respond to any questions. Phone contact was repeated monthly. After three months, participants in the IG were asked to fill out the questionnaire again.
Data Analysis
Statistical Package for the Social Sciences (SPSS) for Windows (version 25) was used for data analysis (IBM Corporation, 2017). Descriptive and inferential statistics were utilized based on variables, level of measurement, and research questions.
Results
Sixty patients from one public hospital were contacted by phone and 50 agreed to participate. In addition, 116 participants responded to the Facebook invitation and were contacted by phone; 105 agreed to participate. The total number of participants at the pretest phase was 155, a response rate of 88%. Reasons for refusal reported by patients who chose not to participate included time, fear of not performing self-care adequately as instructed on the app, and possible changes to their daily routine. After three months, at the post-test phase, 128 participants completed the questionnaire (64 participants in each group), an attrition rate of 17.4%. See Figure 2.
Demographics
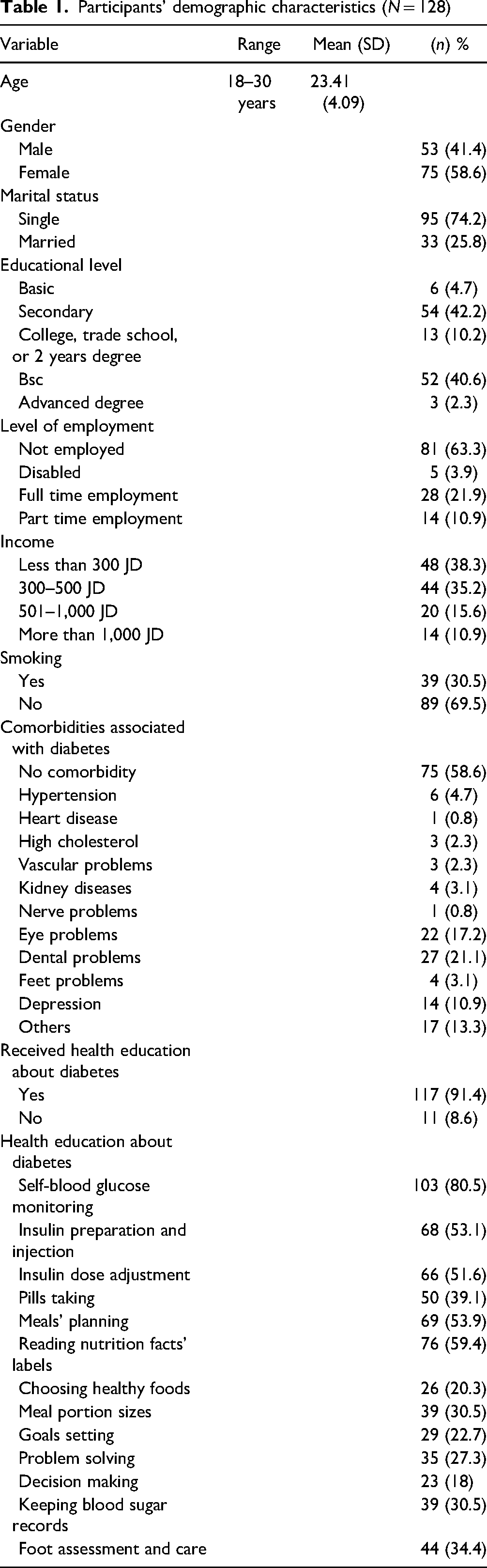
Participants were between 18 and 30 years old (M = 23.41, SD = 4.09), 58.6% were females (n = 75). For further details, see Table 1.
Participants’ demographic characteristics (N = 128)
To assess whether there was any difference in demographics between the CG and the IG before the intervention, independent samples t-test analysis and chi-squared test showed no significant differences in proportions of any variables between the groups.
Self-Efficacy, Self-Care Agency, and Self-Care Management
Independent samples t-test showed no significant difference in baseline levels of SE, SCA, and SCM between the CG and the IG. An independent samples t-test was performed to assess whether means of posttest scores of SE and SCA differed significantly for the IG compared with the CG. The posttest mean of SCA for the IG differed significantly compared with the CG, t (126) = - 3.102, p = .002, two tailed. Mean of SCA for the IG (M = 56.81, SD = 6.53) was higher than that for the CG (M = 53.38, SD = 5.99). See Table 2.
Comparison of posttest scores of self-efficacy and self-care agency between control and intervention groups using independent samples t-test (N = 128).
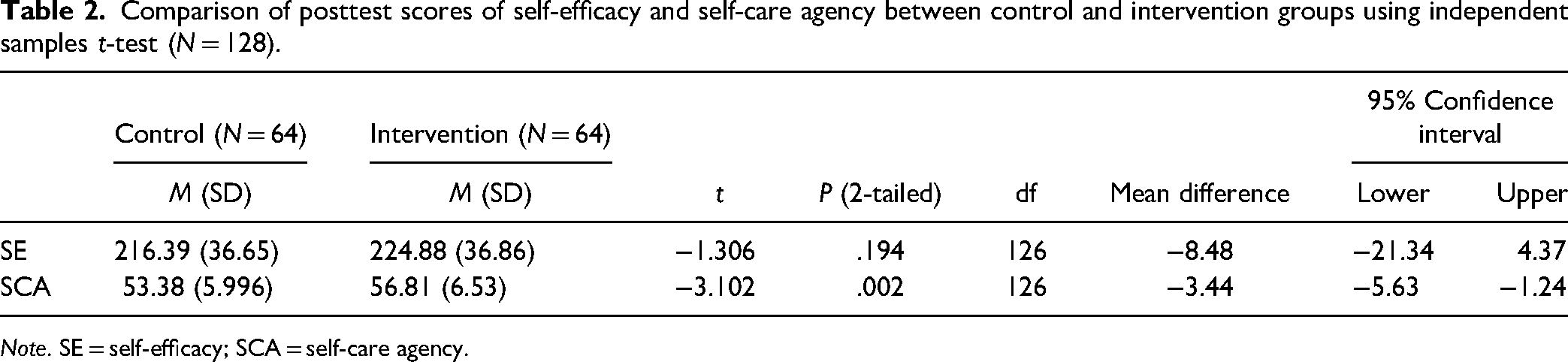
Note. SE = self-efficacy; SCA = self-care agency.
Participants in the CG didn’t show any significant improvement in SE (t (63)=-.358, p = .722, two tailed), SCA (t (63)= 1.362, p = .178, two tailed), or SCM (t (63) = .380, p = .705, two tailed) compared to pre-test levels. In regards to participants in the IG, t-test analysis showed improvement in the mean of SE after using the app (t (63)=-2.826, p = .006, two tailed). However, the means of pretest and posttest scores of SCA for the IG did not differ significantly, t (63)=-1.152, p = .254, two tailed.
Results of analysis of covariance (ANCOVA) revealed a significant difference between the CG and the IG in SCM after controlling for pretest scores of SE and SCA, F(1, 124) = 4.366, P = .039, Partial Eta Squared (η2) = 0.034. This means that 3.4% of the variance in SCM was explained by the intervention. Also, results revealed that SE (covariate) was significant, F(1, 124) = 44.164, P < .01, and explained 26.3% of variance in SCM. The covariance of SCA was not significant, F(1, 124) = 2.330, P = .129. See Table 3.
Comparison of posttest mean scores of self-management between control and intervention groups after controlling of pretest scores of self-efficacy and self-care agency using ANCOVA (N = 128).
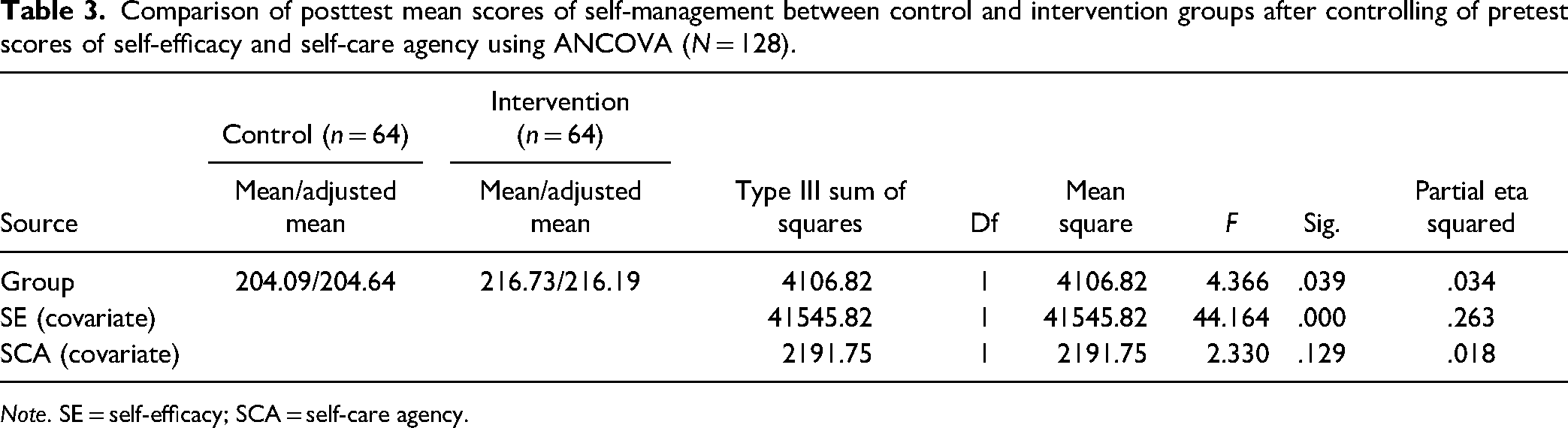
Note. SE = self-efficacy; SCA = self-care agency.
Repeated measures of ANCOVA showed a significant difference in the levels of SCM among patients in the IG at pretest and posttest after controlling for SE and SCA, Wilks’ Lambda = .921, F(1, 61) = 5.257, P = .025. Results indicated that 7.9% of variance in SCM was explained by the app. Also, results revealed that covariance of SE, Wilks’ Lambda = .986, F(1, 61) = .882, P = .351, and SCA, Wilks’ Lambda = .979, F(1, 61) = 1.329, P = .253 was not significant.
Discussion
The current study results showed that using the mobile app for three months was associated with a significant difference in mean score of SE within the IG, but not between the two groups. Previous literature showed that using various mobile technologies was associated with improved SE among patients with diabetes of different age groups (Aminuddin et al., 2018; Wang et al., 2017). As discussed in the literature, the relationship between self-care management mobile apps and SE could be explained by the fact that the major aim of the mobile app was to increase patients’ knowledge and awareness about the disease and appropriate management, improving their confidence in diabetes management (in other words, SE) (Adam & Folds, 2014; McCleary-Jones, 2011).
On the other hand, in the current study the mobile app was significantly associated with improved SCA between the control and intervention groups, but not within the IG, as the mean scores for SCA did not differ significantly before and after using the mobile app. In the literature review, no study investigated any of the mobile phone technologies’ effect on SCA. Few studies found positive impacts of various educational methods on SCA among various populations (e.g., patients with Type 2 DM [T2DM], chronic obstructive pulmonary diseases, or ileostomies or colostomies (Culha et al., 2016; Stockdale-Woolley, 1984; Surucu et al., 2017). The positive effects of the mobile app on SCA could be explained by patients’ increased knowledge and confidence about managing diabetes, which contributes to better performance of self-care behaviors.
In the current study, using the mobile app had a significant effect on scores of SCM within the IG and between the two groups, after controlling for SE and SCA. These results were consistent with many studies that showed positive impacts of different mobile phone technologies, including mobile apps, on SCM among patients with T1DM or T2DM (Aminuddin et al., 2018; El-Gayar et al., 2013; Guo et al., 2015; Holtz & Lauckner, 2012; Offringa et al., 2018; Wang et al., 2017). Other studies revealed positive impacts of education on adherence to self-care behaviors (DeJesus, 2016; Surucu et al., 2017; Wichit et al., 2017).
Influencing patient's knowledge about diabetes should improve SE, SCA and SCM. In addition, the effect of knowledge about diabetes on SCM is mediated by SE and SCA (Gharaibeh et al., 2016; Sousa et al., 2004). This supports the results of the current research, as the mobile app included educational material about diabetes. SE and SCA positively affect patients’ commitment to self-care behaviors, fostering improved SCM, which depends on one's commitment; this in turn facilitates better clinical outcomes and decreased emergency department visits and hospitalizations (Katz et al., 2012; Sousa et al., 2005).
Patients who used the app for three months reported higher levels of SCM compared to those in the CG, and compared to their own levels before using it. Most of the literature reported positive impacts of different mobile interventions on SCM. Results of the current study indicated significant effect of SE as covariate, while that was not the case for SCA. Health-care professionals should give more attention to supporting patients’ feelings of self-efficacy and self-care agency, so as to improve their effectiveness at self-care management (Mohebi et al., 2013).
Strengths, Limitations and Suggestions for Future Research
There are several strengths of the current study. First, the mobile app was created and programmed based on study needs, with collaboration of the researcher and the programmer. Based on the literature review, the current study is the first study that investigated the effect of a mobile app on SCA among patients with T1DM. Finally, the response rate was considered high, which provided better data quality and reliability, better external validity, and overall generalizability.
This study was subject to some limitations. The convenience sampling method limits generalizability (Polit & Beck, 2013); however, it was the most appropriate method to recruit participants with specific characteristics, to achieve the aim of the study. Part of the sample was recruited via social media rather than from a hospital; we don’t know which health-care sector these patients are referred to. However, t-test did not detect any difference in demographics between the CG and the IG. Self-report on questionnaires affects the validity and accuracy of the provided data (Waltz et al., 2010); however, this was the most appropriate way to collect data from geographically dispersed participants. Another limitation is the short period of study; it would be beneficial to investigate the long-term effectiveness of the mobile app.
Implications for Practice and Research
Mobile apps can be a good reference for patients to keep with them all the time, to return to needed information at any time, reduce visits to HCPs, and promote continuity of care. These apps could be provided to public hospitals and primary health-care centers that serve low-income patients, as well as private hospitals.
Similar apps could be part of patients’ electronic health records (EHRs) to enhance SCM for all patients. Other information recorded and transferred to EHRs could include meals eaten, calorie calculations, and activities performed. Applications might include individualized instructions and health education for each patient, based on their data, and/or messaging to alert a specialized provider based on specific information.
Conclusion
Self-care management plays a vital role in managing Diabetes Mellitus and its complications. One SCM method is diabetes self-management education, which can be achieved by advanced technologies like mobile apps. Using SCM mobile apps for self-care management of diabetes can lead to increased knowledge about the disease, complications, various aspects of self-management, and how to live with it. This can support patient's confidence in managing the disease, and better commitment to and performance of self-care activities, with the aim of slowing the progress of the disease, reducing complications, and improving health status and, as a result, quality of life.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deanship of Scientific Research, University of Jordan (grant number 19/2018/4865).