
Abstract
Health-care workers are at an elevated risk of anxiety due to their high emotional and operational demands. While social support is recognized as a buffer against psychological distress, little is known about how its protective role differs according to sex, marital status, and departmental setting. A cross-sectional survey was conducted at a regional general hospital in Greece, with 162 health-care professionals. Participants completed the State-Trait Anxiety Inventory and Multidimensional Scale of Perceived Social Support. The data were analyzed using correlation, regression, and PROCESS-based mediation and moderation models. Perceived social support was significantly and negatively associated with both state and trait anxiety. Regression analysis showed that social support was a robust independent predictor of lower anxiety. Female participants reported higher anxiety levels, which was partially mediated by lower perceived support. Marital status moderated the support–anxiety relationship, with divorced individuals benefiting most from support. Departmental differences emerged, with psychiatric staff showing lower anxiety and a stronger protective effect of social support than administrative staff. Perceived social support reduces anxiety among health-care professionals, and the magnitude of its effect is influenced by sex, marital status, and occupational context.
Implications for Knowledge Translation
Occupational health nurses can reduce anxiety by strengthening social support systems in the workplace. Targeted strategies such as peer mentoring, debriefings, and sex- or role-sensitive interventions are especially important for high-risk groups, including administrative staff and divorced employees. Organizational interventions should prioritize non-clinical staff, particularly administrative personnel, who may experience elevated anxiety despite lower clinical exposure. Interventions should account for both perceived support and individual differences in help-seeking or emotional disclosure, especially when designing mental health screening and support initiatives.
The health-care sector, particularly hospitals, represents a unique and high stakes work environment characterized by emotional labor, time constraints, and clinical uncertainty (Hill et al., 2022; Saragih et al., 2021). Health-care professionals regularly face emotionally challenging situations involving heavy workloads, ethically complex decisions, and challenging outcomes (Tamminga et al., 2023; Toska et al., 2025). These conditions heighten vulnerability to psychological distress, with anxiety being one of the most common and harmful manifestations. Anxiety not only undermines the mental health and well-being of health-care staff but also impairs cognitive functioning, clinical judgment, and patient safety (Iraís et al., 2025; Toska et al., 2024).
Anxiety has been linked to increased absenteeism, reduced job satisfaction, and higher turnover intentions, which threaten the sustainability and operational resilience of health-care systems, particularly during periods of acute stress, such as the COVID-19 pandemic (Lai et al., 2020; Modaresnezhad et al., 2021). One of the most consistently identified protective factors against psychological distress is perceived social support, defined not just as the presence of social networks, but also as the subjective appraisal of available emotional, informational, or instrumental support (Labrague, 2021; Zhang et al., 2023). According to the stress-buffering hypothesis, social support can mitigate the adverse effects of stressful experiences by enhancing coping resources and reducing perceived threats (Cohen & Wills, 1985). This theoretical framework is supported by previous research showing that both family and peer support are inversely associated with symptoms of depression and psychological distress (Ortiz-Calvo et al., 2022). Similarly, the VOICE study in Germany demonstrated that social support exerted a stronger protective effect on symptoms of depression and anxiety than many established sociodemographic or occupational risk factors, including sex or direct exposure to COVID-19 patients (Schug et al., 2021).
Despite its importance, the protective role of social support among health-care workers in hospital settings remains underexplored. The literature mainly focuses on clinicians in tertiary hospitals, particularly physicians and nurses, whereas administrative staff, outpatient staff, and allied health workers receive less attention (Ahlstedt et al., 2024; Hamama et al., 2019; Miao et al., 2024). Moreover, studies often treat social support as a singular concept, failing to examine how its perceived quality or source might differ based on marital status or professional department. These gaps limit our understanding of the role of social support as a buffer in diverse health-care environments and staff categories.
This study addresses these gaps by examining both clinical and non-clinical personnel in a regional general hospital using a validated multidimensional measure of perceived social support. Specifically, it investigates the association between perceived social support and anxiety and explores whether this relationship differs according to key sociodemographic and occupational characteristics. By assessing potential mediating and moderating effects of sex, marital status, age, and hospital department, this study aims to clarify how social support functions as a protective mechanism within diverse health-care roles and contexts. Based on the stress-buffering hypothesis (Cohen & Wills, 1985) and existing empirical evidence, the following hypotheses were formulated:
Materials and Methods
Setting and Participants
This study was conducted at the General Hospital of Corinth, a regional public hospital comprising both clinical and administrative departments. The inclusion criteria were as follows: (1) medical, nursing, or administrative staff employed at the hospital; (2) aged 18 years or older; (3) possessing excellent proficiency in the Greek language; (4) cognitively capable of independent participation; and (5) willing to complete a self-administered questionnaire. Exclusion criteria were (1) insufficient literacy or (2) incomplete responses. The participant pool represented a range of departments, including internal medicine, surgery, pediatrics, psychiatry, diagnostic laboratories, emergency units, and administrative services.
Instruments
Data were collected through a structured self-administered questionnaire comprising three primary components: a demographic and occupational section, an anxiety assessment scale, and an assessment of perceived social support.
Demographic Characteristics of Participants
The initial section of the questionnaire collected data on participants’ age, sex, marital status, educational attainment, professional role, and employment department. These sociodemographic and occupational variables were used to describe the sample and evaluate their potential associations with anxiety and perceived social support.
Anxiety
To assess anxiety levels, the study employed the State-Trait Anxiety Inventory (STAI-40), originally developed by Spielberger, Gorsuch, and Lushene in 1983 (Spielberger et al., n.d.). The STAI-40 consists of 40 items equally divided into two subscales: the State Anxiety Scale (STAI-S), which evaluates transient anxiety experienced at the time of assessment, and the Trait Anxiety Scale (STAI-T), which reflects a stable predisposition to anxiety. Participants responded to each item using a 4-point Likert scale ranging from 1 (“Not at all”) to 4 (“Very much so”), with reverse scoring applied to select items. Each subscale yielded a total score ranging from 20 to 80, with higher scores indicating higher anxiety levels. In the present study, the validated Greek version of the STAI was employed, which was culturally adapted by Fountoulakis et al. (2006). The internal consistency of the instrument in this sample was excellent, with Cronbach's alpha coefficients of 0.938 and 0.905 for the SA anxiety subscales, respectively.
Social Support
Perceived social support was measured using the Multidimensional Scale of Perceived Social Support (MSPSS), developed by Zimet et al. (1988). The MSPSS comprises 12 items designed to assess support perceived from three sources: family, friends, and significant others. Each item is rated on a 7-point Likert scale ranging from 1 (“Very strongly disagree”) to 7 (“Very strongly agree”). The total score ranged from 12 to 84, with higher scores indicating greater levels of perceived social support. The validated Greek version of the MSPSS, adapted by Theofilou in 2015 for use in clinical and general populations, was used in this study (Theofilou, 2015). The scale demonstrated excellent internal consistency in our sample, with a Cronbach's alpha value of 0.927. Given its brevity, ease of interpretation, and relevance to the health-care setting, the MSPSS is particularly well-suited for assessing the psychosocial environment of hospital staff. For ease of interpretation, MSPSS scores were calculated as mean item scores ranging from 1 to 7, with higher scores indicating greater perceived social support.
Data Collection
Data were collected between January and February 2024. A total of 220 printed, self-administered questionnaires were distributed across clinical and administrative departments of the hospital. The distribution followed a pragmatic, convenience-based approach, whereby questionnaires were provided to staff members who were present and available during the data collection period. Departments were approached to ensure representation from different professional roles; however, no formal random sampling procedure was applied, and not all eligible staff necessarily received a questionnaire.
Each questionnaire was delivered in a sealed envelope containing the study information sheet, informed consent form, and the questionnaire. Participation was voluntary and anonymous, and no personal or identifiable information was collected. The estimated completion time was 10–15 min.
In total, 162 completed questionnaires were returned, corresponding to a response rate of 73.6% based on the number of distributed questionnaires. As the total number of eligible staff was not formally recorded, this response rate reflects the proportion of returned questionnaires rather than a population-based response rate. All returned questionnaires were reviewed for completeness prior to data entry, and only fully completed responses were included in the final analysis
The sample size for this study was determined using a pragmatic rule-based approach, as no formal power analysis software was employed. Based on widely accepted methodological guidelines for correlational and multivariable analyses, a minimum of 10–15 participants per independent variable is recommended to ensure sufficient power and model stability in regression analyses (Green, 1991). Given that the primary analysis involved up to five predictors, including social support, sex, age, marital status, and department, a minimum sample of approximately 100–120 participants was considered adequate. The final sample consisted of 162 fully completed responses, exceeding this threshold, thereby enhancing the robustness of the statistical testing, including subgroup comparisons, regression, and mediation/moderation analyses.
Data Analysis
Data were entered and analyzed using IBM SPSS Statistics, Version 28. Descriptive statistics were used to summarize the demographic and occupational characteristics. Categorical variables were expressed as absolute and relative frequencies, whereas continuous variables were reported as means, standard deviations (SD), and ranges. The distribution of continuous variables was evaluated through visual inspection of histograms and by examining skewness and kurtosis values.
The relationship between anxiety scores and perceived social support was assessed using Pearson's correlation coefficients. Group differences in anxiety and support levels based on sex, marital status, and department were tested using independent sample t-tests or one-way analysis of variance (ANOVA). When ANOVA revealed significant differences, Bonferroni post-hoc tests were applied to identify specific group contrasts. To examine the predictors of anxiety, multiple linear regression was conducted using state anxiety as the dependent variable and perceived social support, sex, age, and marital status as independent variables.
For a more advanced analysis, mediation and moderation models were performed using the PROCESS macro (version 4.0) for SPSS, developed by Hayes (2013). A mediation analysis (Model 4) was used to determine whether perceived social support acted as a mediator between sex and anxiety. A moderation analysis (Model 1) tested whether the relationship between social support and anxiety varied according to marital status. In both models, a bootstrapping procedure with 5,000 resamples was used to generate confidence intervals for indirect and interaction effects. This non-parametric method increases the accuracy of the estimates, particularly when the sampling distribution is unknown or not normally distributed. All statistical tests were two-tailed, and a p-value of <.05 was considered the threshold for statistical significance.
Ethical Considerations
The study protocol was reviewed and approved by the Scientific Committee of the General Hospital of Corinthos, which granted permission for its implementation in the hospital setting (Ref. number 01/09-01-2023). All procedures adhered to the principles outlined in the Declaration of Helsinki (World Medical Association, 2013) and the relevant national ethical regulations governing research involving human subjects.
The participants received a detailed information sheet explaining the study's purpose, voluntary nature, anonymity, and data confidentiality. Informed consent was obtained from all individuals prior to participation through a signed consent form that was submitted along with the completed questionnaire. No personal or identifying data were collected, ensuring full anonymity.
Results
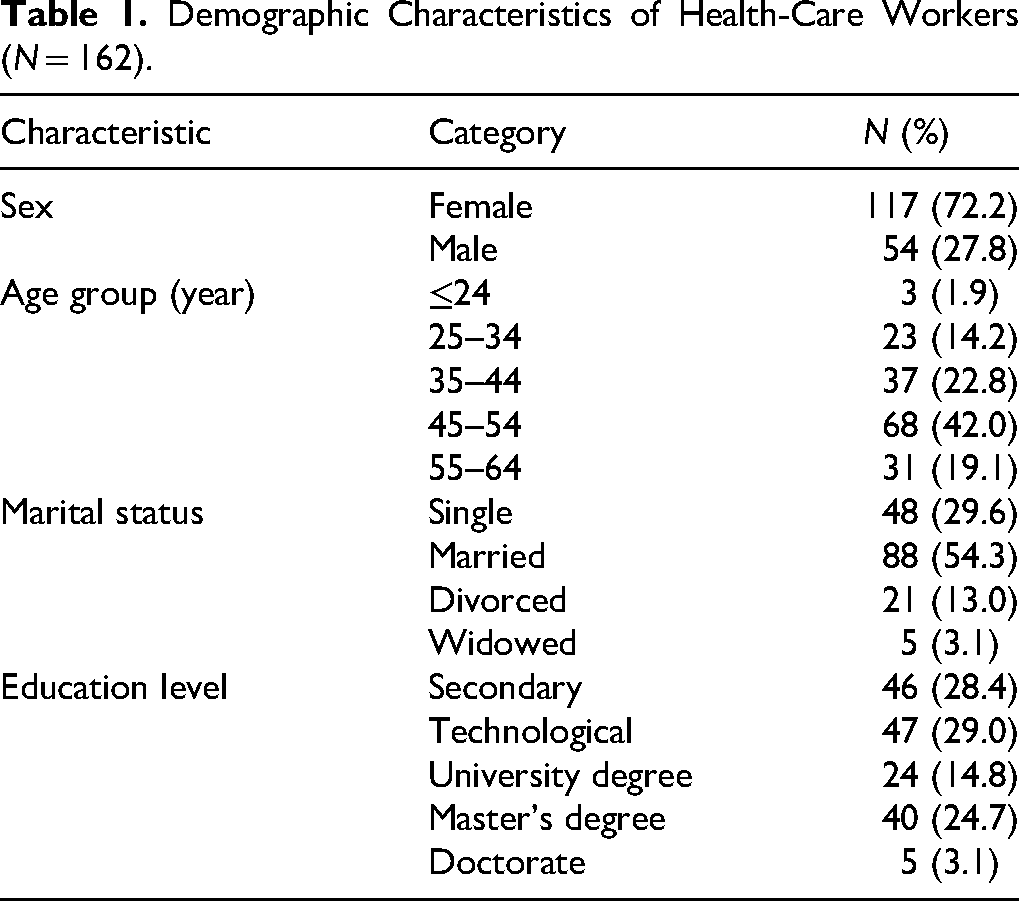
A total of 162 health-care professionals participated in the study. The majority were female (72.2%), with the most represented age group being 45–54 years (42.0%). Most participants were married (54.3%), and their educational attainment varied, with 29.0% holding a technological degree and 24.7% holding a master's degree (Table 1). These characteristics provide a heterogeneous basis for exploring psychosocial predictors of anxiety.
Demographic Characteristics of Health-Care Workers (N = 162).
The measures demonstrated excellent internal consistency (Cronbach's α = 0.903 for state anxiety, 0.895 for trait anxiety, and 0.927 for social support). The mean state anxiety score was 43.0 (SD = 10.1) and the mean trait anxiety score was 39.0 (SD = 9.3). Perceived social support was relatively high, with a mean item score of 5.85 (SD = 0.90) on a 7-point scale, suggesting a generally supportive social environment (Table 2).
Descriptive Statistics and Reliability of Psychometric Scales.
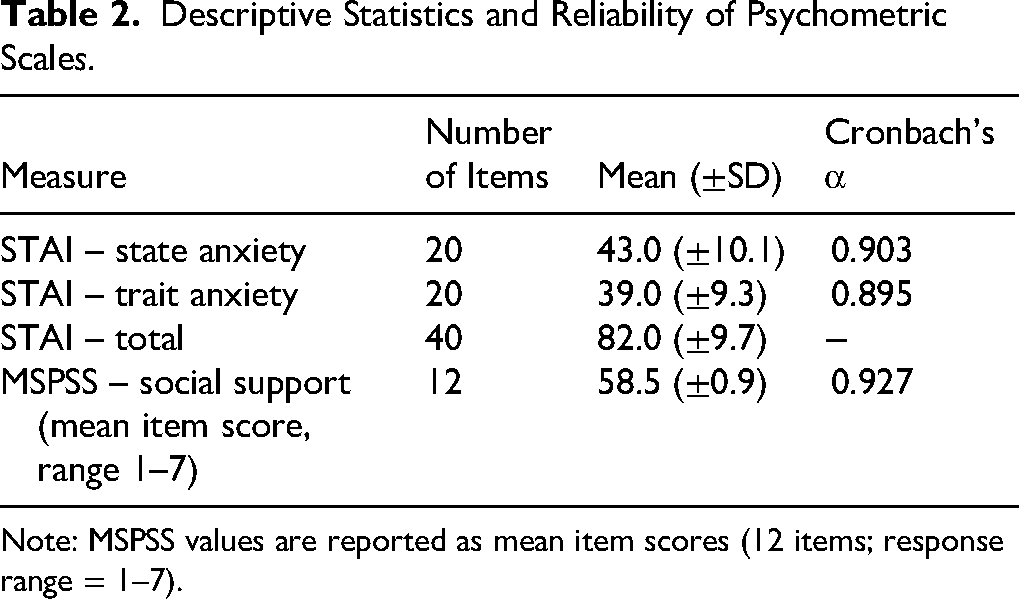
Note: MSPSS values are reported as mean item scores (12 items; response range = 1–7).
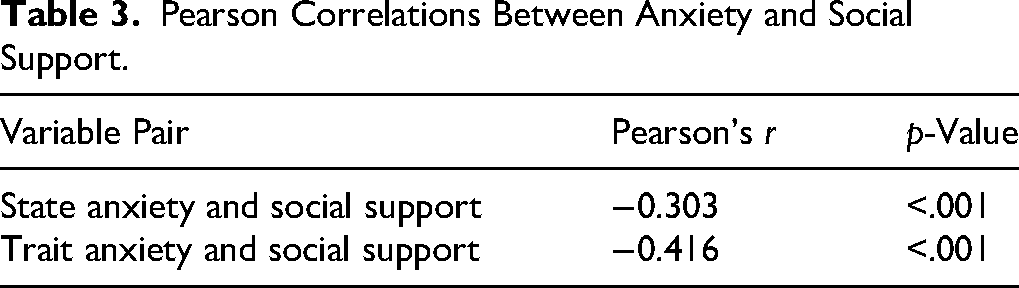
Social support was significantly and negatively correlated with both state (r = –0.303, p < .001) and trait anxiety (r = –0.416, p < .001). These moderate inverse relationships suggest that individuals who perceived higher social support reported lower levels of situational and dispositional anxiety (Table 3). A stronger correlation with trait anxiety may indicate a buffering role for social support against chronic emotional vulnerability.
Pearson Correlations Between Anxiety and Social Support.
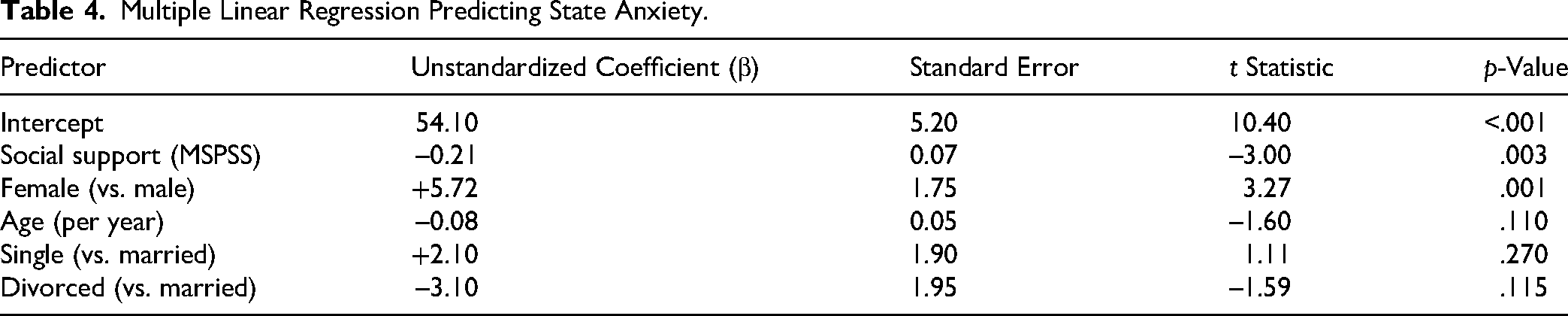
In the adjusted regression model (R2 = 0.27, p < .001), female sex emerged as a significant positive predictor of anxiety (β = +5.72, p = .001) independent of other demographic factors. Perceived social support remained a robust negative predictor (β = −0.21, p = .003). The age and marital status categories were not significant (Table 4). The explained variance suggests that psychosocial factors, rather than demographic factors, are more central in predicting acute anxiety levels.
Multiple Linear Regression Predicting State Anxiety.
The mediation model tested whether social support mediates the relationship between sex and anxiety. The indirect path from sex to support anxiety was small and marginally non-significant (indirect β = −0.01, p = .088), while the direct effect of sex remained strong (β = + 5.60, p = .001). This finding suggests partial mediation, whereby lower support partially accounts for, but does not fully explain, higher anxiety among women (Table 5).
Mediation Analysis: Social Support as Mediator Between Sex and State Anxiety.
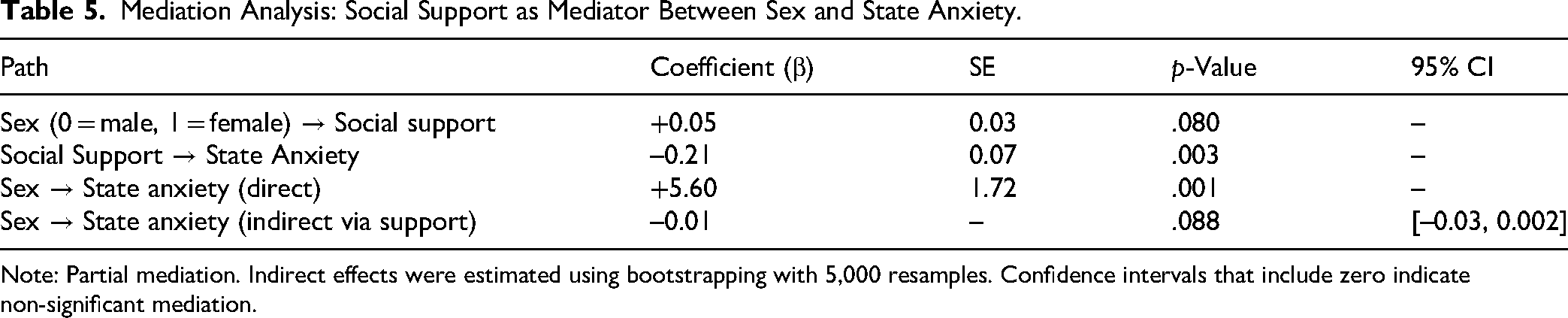
Note: Partial mediation. Indirect effects were estimated using bootstrapping with 5,000 resamples. Confidence intervals that include zero indicate non-significant mediation.
Moderation Analysis: Marital Status × Social Support Predicting State Anxiety.
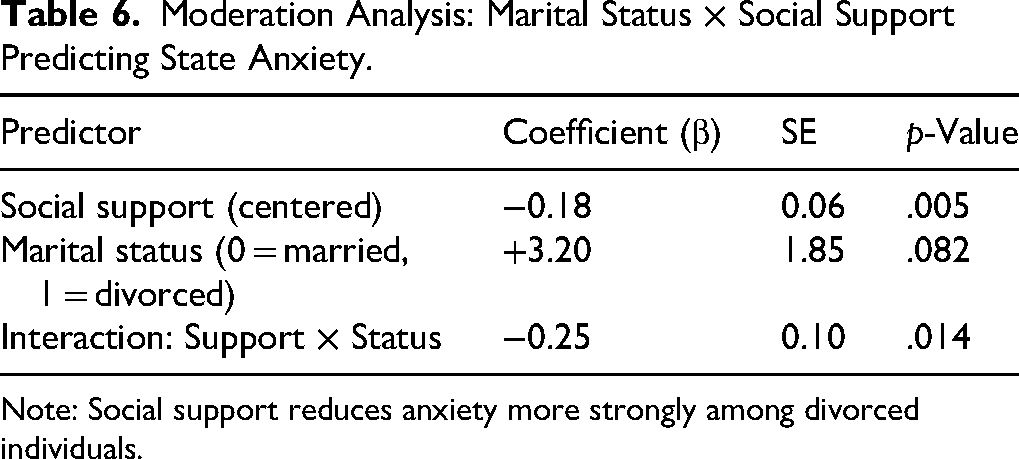
Note: Social support reduces anxiety more strongly among divorced individuals.
Moderation analysis tested whether the protective effect of support differed by marital status. A significant interaction was found (β = –0.25, p = .014), indicating that social support attenuated anxiety in divorced individuals more strongly (Table 5). This finding suggests a differential benefit of support, particularly for those lacking formal spousal networks.
Department-specific regressions revealed that social support was more strongly associated with lower anxiety among psychiatric staff (β = –0.28, p = .002) than among administrative staff (β = –0.12, p = .080) (Table 7). This pattern may reflect greater baseline exposure to psychological distress in clinical roles, in which support exerts a more protective effect.
Subgroup Regression by Department (Psychiatry vs. Administration).
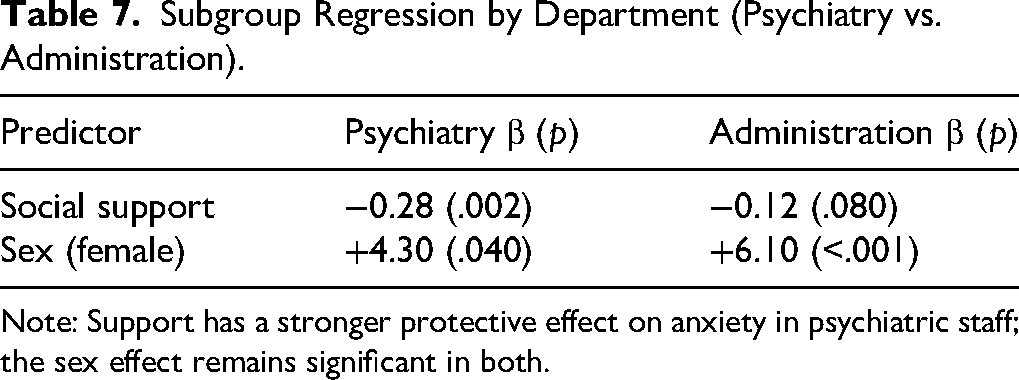
Note: Support has a stronger protective effect on anxiety in psychiatric staff; the sex effect remains significant in both.
Sex-based comparisons showed that females reported significantly higher anxiety in both state (mean = 45.1 vs. 38.3, p < .001) and trait domains (mean = 40.3 vs. 35.0, p < .001), with Cohen's d values of 0.68 and 0.60, respectively, indicating medium to large effect sizes (Tables 8 and 9). Notably, social support did not differ significantly according to sex (d = 0.06). Departmental comparisons showed markedly higher anxiety among administrative staff, reinforcing the importance of context. Married participants reported significantly higher levels of perceived support than did divorced individuals (Bonferroni-corrected p < .05).
Differences in Anxiety and Social Support Scores by Sex, Marital Status, and Department.
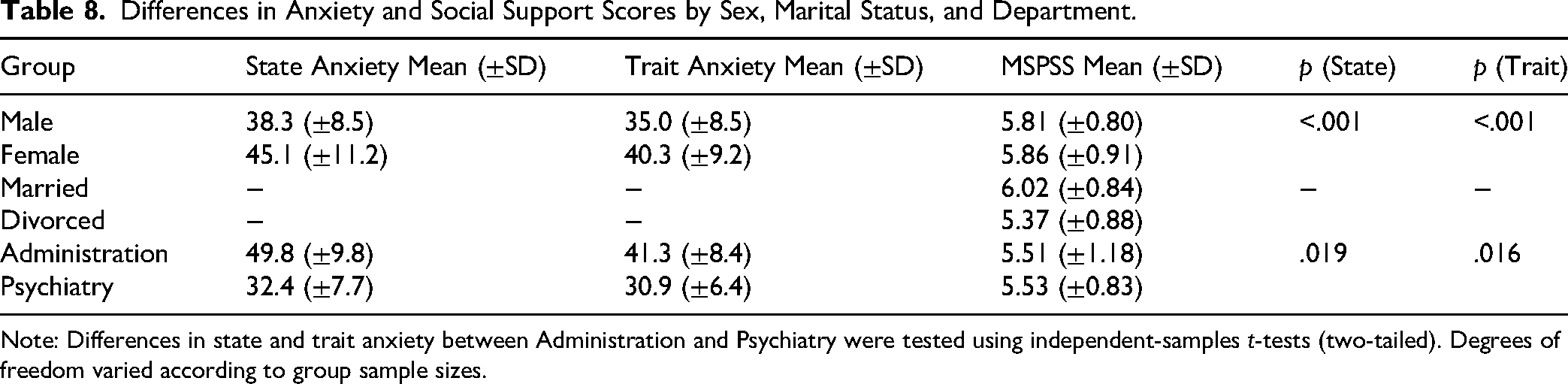
Note: Differences in state and trait anxiety between Administration and Psychiatry were tested using independent-samples t-tests (two-tailed). Degrees of freedom varied according to group sample sizes.
Effect Sizes (Cohen's d) for Sex Differences.
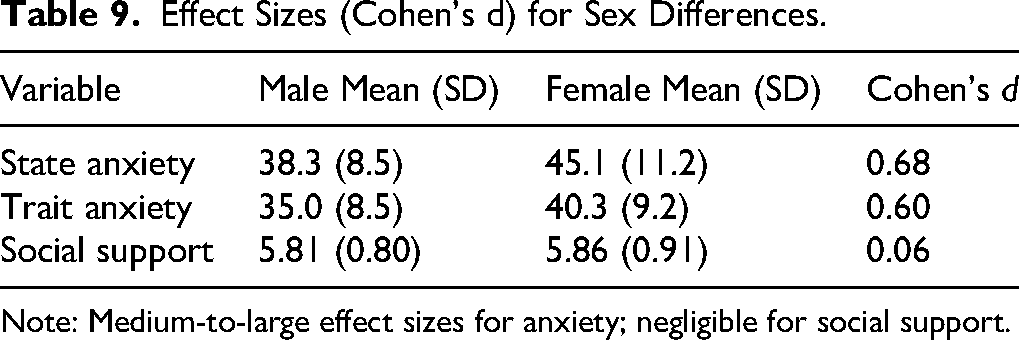
Note: Medium-to-large effect sizes for anxiety; negligible for social support.
Discussion
The critical hospital environment imposes substantial psychological demands on employees, thereby heightening their susceptibility to anxiety. However, research frequently concentrates on clinical roles and often overlooks non-clinical staff (Lake et al., 2022; Pala et al., 2022). Additionally, while perceived social support is recognized as a moderator of anxiety, its varying impact across different occupational and demographic groups remains insufficiently explored.
This study aimed to investigate the relationship between perceived social support and anxiety among both clinical and administrative hospital staff, thereby addressing existing gaps in subgroup analysis and contextual diversity (Mei et al., 2024; Wu et al., 2022). By employing validated instruments and examining the mediating and moderating effects, this study offers a comprehensive understanding of social support as a protective factor in diverse health-care settings.
The primary outcome of our study demonstrated a significant inverse relationship between perceived social support and state and trait anxiety among health-care workers. Social support not only exhibited a negative correlation with anxiety scores but also emerged as a strong independent predictor in multivariable regression models. This finding corroborates our primary hypothesis (H1), indicating that health-care professionals who perceive greater emotional or instrumental support experience reduced psychological distress. Notably, this relationship persisted even after adjusting for sex, age, and marital status, underscoring the direct relevance of support as a standalone psychological resource in high-stress work environments.
The secondary outcomes highlight the robust and consistent sex difference in anxiety, with women reporting higher levels. These differences should be interpreted with some caution; they may not be totally in perceived or experienced anxiety, but at least partly in willingness to report anxiety. Although social support was slightly lower in women, it did not significantly mediate the association between sex and anxiety; however, the indirect effect showed a non-significant trend toward mediation.
The moderating role of marital status is noteworthy. While married participants reported the highest levels of perceived social support, divorced individuals experienced the most pronounced benefits from support in reducing anxiety. The interaction between marital status and social support was statistically significant, indicating that the anxiety-buffering effect of support was stronger among divorced individuals. Additionally, occupational department was a meaningful determinant of both anxiety levels and the effectiveness of social support. This supports our moderation hypothesis (H2 extension), which suggests that individuals without formal familial support may rely more on alternative social networks. Administrative staff exhibited the highest levels of both state and trait anxiety, whereas psychiatric staff reported the lowest levels.
Moreover, regression analyses revealed that the inverse association between social support and anxiety was significantly stronger among psychiatric staff than administrative personnel. This pattern supports Hypothesis 3, suggesting that individuals in emotionally intensive clinical roles may derive more psychological benefits from interpersonal and social resources, perhaps because of their heightened exposure to emotionally charged work environments.
Furthermore, age and marital status did not emerge as direct predictors of anxiety in the regression model despite their roles in moderation or subgroup contrasts. Although older participants tended to report slightly lower anxiety scores, the effect of age was not significant. Similarly, marital status categories did not directly predict anxiety levels, reinforcing the notion that interaction effects, rather than main effects, better explain the psychosocial landscape in the health-care workforce. Finally, the internal consistency of the psychometric instruments used in this study was exceptionally high, with Cronbach's alpha values exceeding 0.90 for all subscales of both the State-Trait Anxiety Inventory and the MSPSS.
These findings are consistent with previous research on the buffering role of perceived social support in managing occupational anxiety in health-care settings. The significant inverse relationships between perceived support and both state and trait anxiety align with earlier studies. Labrague (2021) found that high levels of perceived social support predicted lower anxiety and burnout among frontline nurses during the COVID-19 pandemic (Labrague & De los Santos, 2020). Similarly, Xiao et al. (2020) conducted a meta-analysis of 12 countries and identified social support as a key protective factor against anxiety symptoms.
Sex differences in anxiety, with female health-care workers reporting higher levels, are consistent with existing literature. Studies by Al Maqbali et al. (2021) and Rossi et al. (2020) documented increased anxiety among female health-care workers, which was attributed to sex expectations and caregiving roles. Our study indicated that perceived social support only partially mediates this relationship, suggesting that other structural and occupational factors influence sex differences in psychological outcomes.
Notably, the moderation analysis revealed that divorced individuals benefited more strongly from social support in reducing anxiety compared to married individuals. This aligns with findings by Li et al. (2020), who showed that the absence of spousal support increases reliance on alternative social resources, magnifying the protective impact of perceived social support among single or divorced workers (Li et al., 2020).
In contrast to assumptions that clinical roles inherently involve more emotional burden, administrative staff in our sample reported the highest anxiety levels. This may reflect organizational stressors such as workload ambiguity and lower autonomy. Ruotsalainen et al. found that non-clinical hospital staff reported significant emotional exhaustion. In contrast, psychiatric ward staff members exhibited lower anxiety levels and stronger associations between social support and reduced anxiety, reflecting better coping strategies in mental health settings (Ruotsalainen et al., 2014). Meanwhile, psychiatric staff reported lower anxiety levels and a stronger inverse relationship between support and anxiety, which may reflect greater familiarity with psychological distress, enhanced emotional awareness, and the routine use of coping strategies acquired through professional training and clinical exposure to mental health conditions. Alternatively, a selection effect may also contribute to this pattern, whereby individuals who are less prone to anxiety or who possess stronger baseline coping resources may be more likely to enter or remain in psychiatric roles.
The lack of significant effects for age and marital status as direct predictors of anxiety in regression models suggests that their influence may operate more through interaction effects. Although older participants reported slightly lower anxiety, the differences were not statistically significant, which is consistent with findings from a multi-country analysis by Pappa et al. (2020) showing that age was not a consistent predictor of psychological distress among health-care workers (Pappa et al., 2020).
The strengths of this study are its conceptual contributions and practical relevance. By deliberately including both clinical and non-clinical staff, this research captures the often-overlooked emotional burdens faced by administrative personnel, an important yet neglected population in mental health research. Second, the study did not stop at measuring associations; it explored how social support functions differently, depending on demographic and occupational variables. The use of moderation and mediation analyses moved beyond surface-level findings to uncover meaningful interaction effects, such as the heightened benefit of support for divorced individuals and stronger impact within psychiatric units. Third, the study was grounded in real-world conditions, conducted during a non-crisis period in a typical regional hospital, which offers a baseline understanding of staff well-being outside of exceptional events, such as pandemics. This enhances its relevance to the ongoing workforce planning and emergency preparedness.
Limitations
Despite its contributions, this study had several limitations. Its cross-sectional design restricts conclusions regarding the causality between support and anxiety. However, the consistency of our findings with those of previous longitudinal studies lends credibility to the proposed relationship. Self-reported data may be subject to bias; nonetheless, we used well-validated instruments and ensured anonymity to encourage honest responses. While the study was of a convenience sample and conducted in a single hospital, the diversity of staff roles and departments improved the internal variability and allowed meaningful subgroup analysis. A further limitation of this study concerns the measurement of social support. Perceived social support was assessed using the MSPSS, which captures support from family, friends, and significant others, but does not specifically assess workplace or organizational sources of support. While perceived support from personal networks is strongly associated with psychological well-being, the absence of a measure targeting supervisor, peer, or institutional support within the workplace limits the ability to directly link the findings to specific organizational support mechanisms. Therefore, while limitations exist, they were either mitigated through the study design or did not significantly threaten the internal validity or relevance of the findings.
Future research should employ longitudinal designs to examine how perceived support influences anxiety over time and in response to organizational changes or crises. Multi-site studies across different regions or health-care systems would enhance generalizability and help identify the systemic factors influencing support structures. Qualitative or mixed-methods approaches could provide richer insights into how support is experienced and mobilized, especially by underrepresented groups, such as administrative staff. Additionally, future work should aim to differentiate between types (emotional, informational, and instrumental) and sources (family, peers, and supervisors) of support to determine which are the most effective in mitigating anxiety. Evaluating targeted interventions, such as peer mentoring, team-based support models, and institutional well-being initiatives, will be key to translating research findings into practice.
Conclusion
This study confirms that perceived social support reduces anxiety among health-care professionals, including both clinical and non-clinical staff. The findings demonstrated that the effectiveness of support varies across demographic and professional subgroups, with particularly strong benefits observed among divorced individuals and psychiatric staff. Enhancing perceived support within health-care settings may serve as a key strategy for improving staff's mental health, resilience, and overall functioning in the workplace.
Footnotes
Authorship Statement
All authors meet the authorship criteria as defined by the International Committee of Medical Journal Editors. Each author has made substantial contributions to the conception, design, data collection, analysis, and/or interpretation of the study; participated in drafting or critically revising the manuscript; and approved the final version for submission. All authors are in full agreement with the content of the manuscript and consent to its submission for publication.
CRediT Authorship Statement
Toska Aikaterini contributed to conceptualization; methodology; investigation; writing–original draft.
Dimitriadou Ioanna contributed to supervision; project administration; writing–review and editing.
Oikonomopoulou Maria contributed to data curation; formal analysis; visualization.
Fradelos C. Evangelos contributed to validation; writing–review and editing; resources.
Papathanasiou V. Ioanna contributed to software; investigation; data curation.
Sarafis Pavlos contributed to formal analysis; visualization; methodology.
Saridi Maria contributed to supervision; funding acquisition; writing–review and editing.
Author Contribution(s)
Ethical Approval and Informed Consent Statements
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was obtained by the Scientific Committee of the General Hospital of Corinth, which granted permission for its implementation in the hospital setting (Ref. number 01/09-01-2023).
All participants were fully informed about the purpose and procedures of the study and provided written informed consent prior to their participation. Confidentiality and anonymity of the participants were strictly maintained throughout the research process.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
No Patient or Public Involvement
This study did not include patient or public involvement in its design, conduct, or reporting.