
Abstract
Background
Family members of patients admitted to the critical care unit (CCU) often face the challenging task of decision-making concerning treatment options, which could negatively affect their mental status. Visitation restrictions (VRs) for family members based on an infectious disease may contribute to mental distress.
Propose
This study aimed to examine the differences in anxiety and depression between family members with VRs and those without VRs after making decisions for patients in the CCU.
Methods
This cross-sectional study employed a questionnaire to collect data on the basic characteristics of the patients and their family members and the presence of VRs during the hospitalization. The Hospital Anxiety Depression Scale was used for the assessment of anxiety and depression.
Results
Of the 100 family members (68% with VRs), those with VRs reported higher post-decision-making anxiety than those without VRs, even in multivariate analysis. Conversely, post-decision-making depression worsened in family members without VRs compared to those with VRs.
Conclusions
Family members of patients in the CCU who had VRs reported higher post-decision-making anxiety, whereas those without VRs reported increased depression. Recognizing VR-dependent changes in post-decision-making anxiety and depression in family members could help them manage mental distress.
Implications for Knowledge Translation
Family members with patients admitted to the critical care unit have a high risk of mental distress, such as anxiety or depression. This study identified higher new-onset post-decision-making anxiety among family members with visitation restrictions than in those without visitation restrictions. Family members without visitation restrictions had more severe post-decision-making depressive symptoms than those with visitation restrictions. Visitation restrictions-based management of mental distress is a potential key factor for personalized family care after decision-making.
Family members of patients in the critical care unit (CCU) frequently experience mental distress, such as anxiety and depression, with an estimated incidence of 13–80% (Bastawrous, 2013; Haines et al., 2015; McAdam & Puntillo, 2009; Metzger et al., 2019; van Beusekom et al., 2016). The management of distress in family members is important, as the mental distress during admission is associated with symptoms of post-traumatic stress disorder following discharge (Azoulay et al., 2005; Jones et al., 2004); The incidence of post-traumatic stress disorder was estimated as 39% (Amass et al., 2020).
Family members are often called upon to make decisions concerning the patient's treatment plans after discussion with the medical staff; however, more than half of family members may be unwilling to participate in the decision-making process (Azoulay et al., 2004). Moreover, for family members, participation in the decision-making process may be associated with mental distress (Azoulay et al., 2005; Gries et al., 2010). Thus, adequate mental support for family members of patients admitted to the CCU may be critical even after decisions have been made.
Beginning in 2019, the coronavirus disease (COVID-19) spread worldwide (Rothan & Byrareddy, 2020). During the pandemic, some hospitalized patients were restricted from being with their family members to prevent the spread of this acute respiratory infection. Although the effectiveness of the SARS-CoV-2 mRNA vaccine has been proven, the effect of visitation restrictions on infection transmission remains unclear (Jefferson et al., 2023; Polack et al., 2020). Family members of patients admitted to the CCU sometimes faced visitation restrictions, which might have induced mental distress (Amass et al., 2022; Forsberg et al., 2023). It remains unclear whether decision-making under visitation restrictions worsens distress, such as anxiety and depression, in family members. Therefore, in this study, we aimed to assess differences in anxiety and depression in family members with visitation restrictions and those without visitation restrictions after decision-making for patients who were admitted to the CCU.
Methods
Participants
This cross-sectional study included individuals who had experience in making decisions for a family member admitted to the CCU between January 2019 and August 2022. The exclusion criterion was the family member being younger than 18 years at admission. Participants who were registered with a database at an online research company (ASMARQ, Tokyo, Japan) were recruited through an e-mail sent by the research company.
Tools
Questionnaire. The online questionnaires were completed in September 2022 by family members of patients admitted to the CCU. The questionnaires included basic characteristics of the decision maker (gender, age at the event, and type of relationship) and the patient admitted to CCU (gender, age at the event, consciousness, and reason for the admission), and presence of visitation restrictions during the admission.
Hospital Anxiety Depression Scale (HADS). This tool (Zigmond & Snaith, 1983) comprises 14 items with four choices on a Likert scale. Higher scores indicate more severe anxiety (HADS-A) or depression (HADS-D); a score greater than 10 indicates clinically significant mental disorders, whereas scores of 8–10 points indicate suspected cases (Zigmond & Snaith, 1983). We asked the participants to recall and report their state of anxiety and depression before and after decision-making. In this study, the instructions defined “decision-making” as “a collaborative process that involves a person and their healthcare professional working together to reach a joint decision about care” (Wohlgemuth et al., 2019).
Statistical Analysis
The obtained data are shown as means ± standard deviations (SD), frequencies (%), standardized beta (β) values, or odds ratios (ORs) with a 95% confidence interval (CI). The family members were divided into two groups based on the presence of visitation restrictions. The Shapiro–Wilk W test was used for the evaluation of Gaussian distribution. After the evaluation of the Gaussian distribution, the t-test and the Mann–Whitney U test were used to compare continuous variables. Fisher's exact tests were used to compare binary data. Additionally, multiple and logistic regression analyses were used for this study. Variables with a p-value <.10 in the univariate analysis (i.e., Model 1) were included in the multivariate analysis (i.e., Model 2). The minimum number of participants for this study was estimated as 90 (statistical power: 80%, two-sided significance level of 5%) (White et al., 2018). When the two-sided p-value was <.05, the null hypothesis was rejected. All statistical analyses were conducted using Stata version 15.1 (Stata-Corp, College Station, TX, USA).
Ethical Considerations
Informed consent was obtained from each participant through a consent field on the associated webpage. This study was approved by the Ethical Committee for Epidemiology of Hiroshima University (#E2022-0093) and conducted in accordance with the Declaration of Helsinki (World Medical Association, 2013). Participants were provided with detailed information regarding the purpose of the study, the nature of the data being collected, and how their responses would be used for research purposes only. They were explicitly informed that all data would be anonymized and handled confidentially, ensuring that no personally identifiable information would be disclosed in any publications. Furthermore, participants were assured their participation was entirely voluntary and that they could withdraw during the answering the questionnaire at any time without any penalty or adverse consequences.
Results
Out of 100 family members (age, mean ± SD: 52.1 ± 13.6 years; male: 62.0%) who were included in this study, 68% experienced visitation restrictions in the hospital (see Table 1).
Characteristics of Patients’ Family Members and Patients.
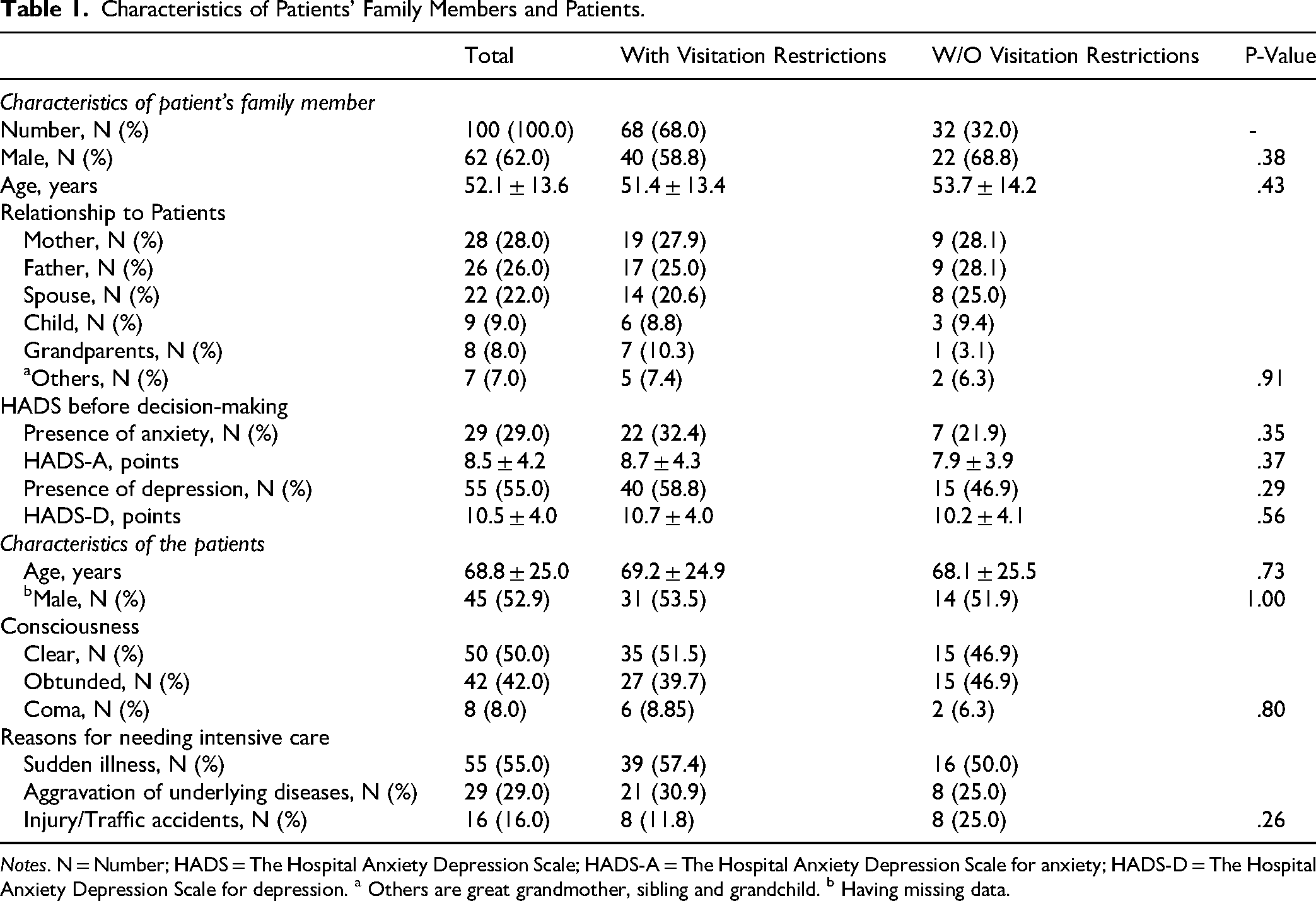
Notes. N = Number; HADS = The Hospital Anxiety Depression Scale; HADS-A = The Hospital Anxiety Depression Scale for anxiety; HADS-D = The Hospital Anxiety Depression Scale for depression. a Others are great grandmother, sibling and grandchild. b Having missing data.
The most frequently admitted patient was the mother (28.0%). Before the decision-making, 29.0% and 55.0% of the family members had anxiety and depression, respectively (HADS-A: 8.5 ± 4.2 points, HADS-D: 10.5 ± 4.0 points). There was no significant age- or sex-related intergroup difference between family members with visitation restrictions and those without visitation restrictions. The proportion and severity of anxiety and depression did not differ between the visitation restrictions-stratified groups. Regarding the admitted patients, the mean age was 68.8 ± 25.0 years (male: 52.9%), and half of the patients appeared obtunded (42.0%) or were in a coma (8.0%) (Table 1).
Concerning post-decision-making anxiety and depression, the proportion of family members with anxiety in the visitation restrictions group was suggestively higher than that in the without visitation restrictions group (35.3 vs. 12.5%, p = .02), whereas the changes in the HADS-A score did not differ between the visitation restrictions (−9.9 ± 37.9%) and w/o visitation restrictions (−8.4 ± 41.9%) groups (see Figure 1).
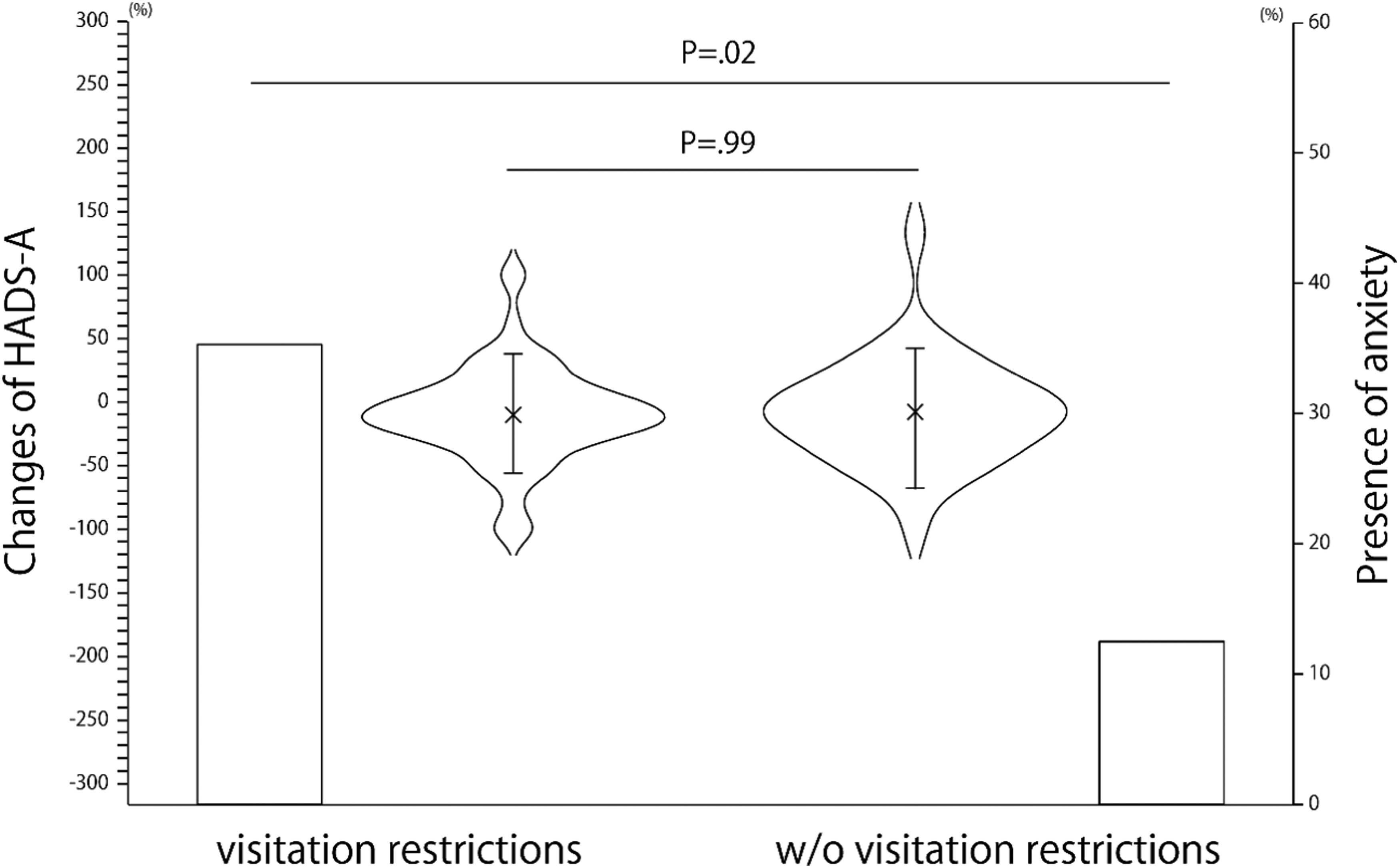
Presence of post-decision-making anxiety in family members and changes thereof. Note. Cross symbol, error bar, and open square represent the mean value, standard deviation, and percentage of family members with anxiety. The violin plot indicates the distribution of changes of HADS-A after the decision-making. HADS-A = Hospital Anxiety Depression Scale-Anxiety.
The proportion of family members with post-decision-making depression did not significantly differ between the visitation restrictions (50.0%) and w/o visitation restrictions (46.9%) groups, nor did the changes of the HADS-D scores (visitation restrictions: −5.3 ± 38.1%, w/o visitation restrictions: 11.9 ± 37.4%; p = .07; see Figure 2).
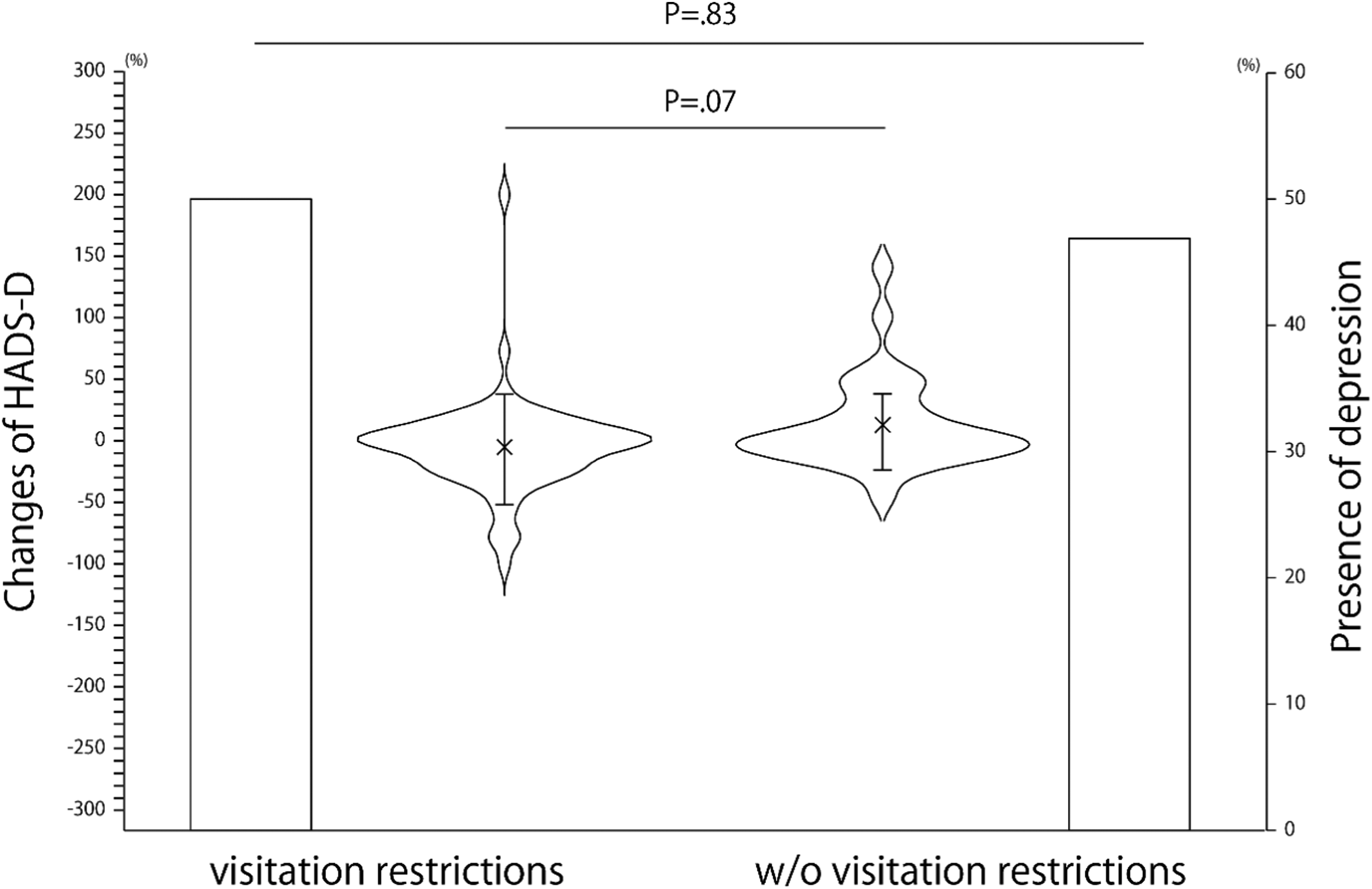
Presence of post-decision-making depression in family members and changes thereof. Note. Cross symbol, error bar, and open square represent the mean value, standard deviation, and percentage of family members with depression. The violin plot indicates the distribution of changes of HADS-D after the decision-making. HADS-D = Hospital Anxiety Depression Scale-Depression.
Among family members without anxiety before the decision-making, no family member had anxiety after the decision-making in the w/o visitation restrictions group, whereas 17.4% of the family members in the visitation restrictions group suggestively developed anxiety after the decision-making (See Table 2A; p = .04). Among the family members with anxiety before the decision-making, only 27.3% of those in the visitation restrictions group reported alleviation of their anxiety after the decision-making, whereas 42.9% of those in the w/o visitation restrictions group experienced alleviation of their anxiety after the decision-making, although this difference was not significant (See Table 2B). Among family members without depression, the proportion of those with post-decision-making depression was 42.9% and 57.1% in the visitation restrictions and w/o visitation restrictions groups, respectively (See Table 2C; p = .40). Among the family members with depression before the decision-making, 22.5% and 26.7% of those in the visitation restrictions and w/o visitation restrictions groups, respectively, experienced alleviation of their depression after the decision-making (See Table 2D; p = .73).
Detailed Trends of Changes of Presence of Anxiety and Depression in the Family Member.
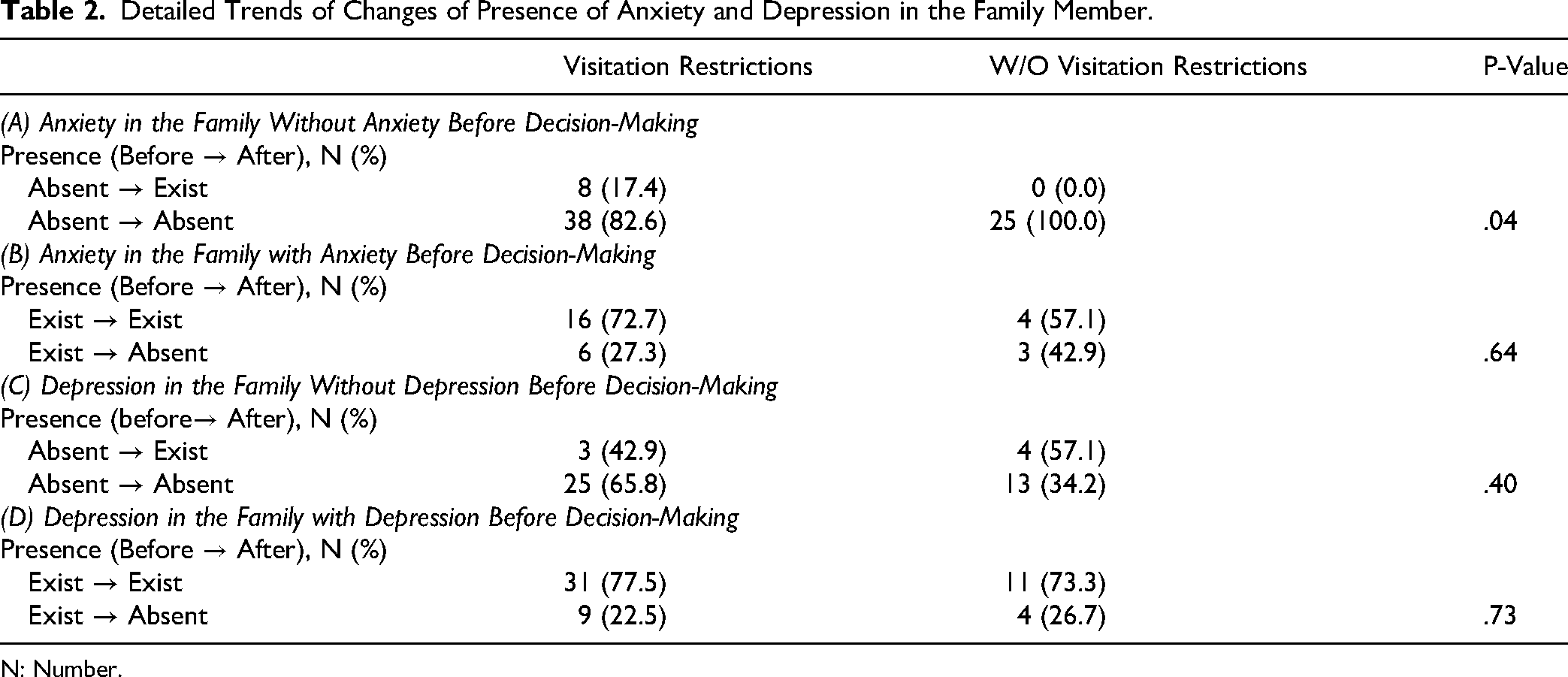
N: Number.
Next, factors associated with post-decision-making anxiety and depression were investigated using general linear models, as shown in Tables 3 and 4. The presence of visitation restrictions and poor consciousness levels, such as obnubilation and coma, were associated with the presence of post-decision-making anxiety (OR [95% CI]: 5.24 [1.49–18.43], p = .01; 8.40 [2.63–26.82], p < .001; and 17.30 [2.85–105.20], p = .002; respectively; See Table 3). Despite the association with the presence of depression, no significant associated factor for post-decision-making changes in HADS-A (i.e., changes as %) was identified (See Table 3).
Associated Factors for Post-Decision-Making Anxiety.
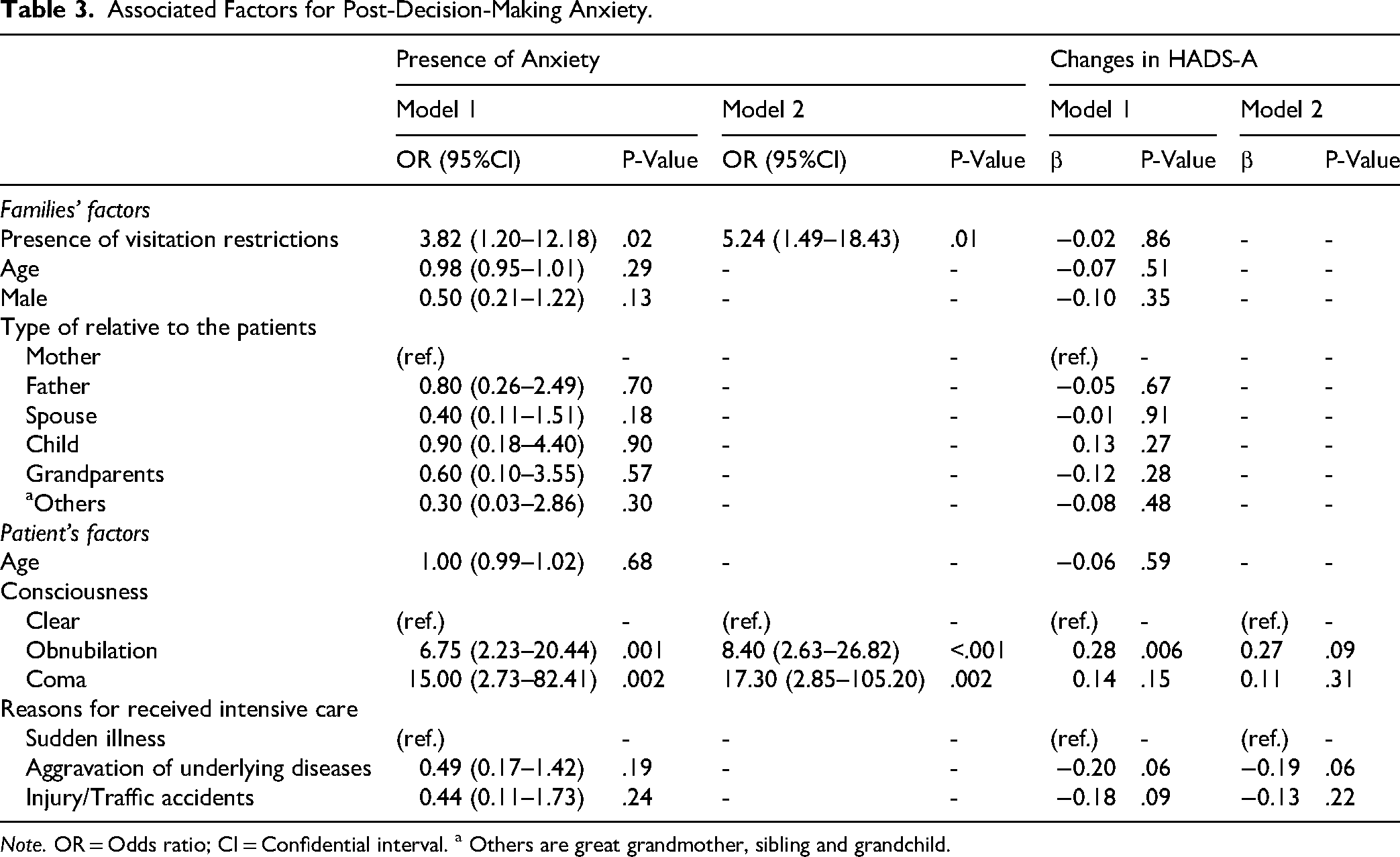
Note. OR = Odds ratio; CI = Confidential interval. a Others are great grandmother, sibling and grandchild.
Associated Factors for Post-Decision-Making Depression.
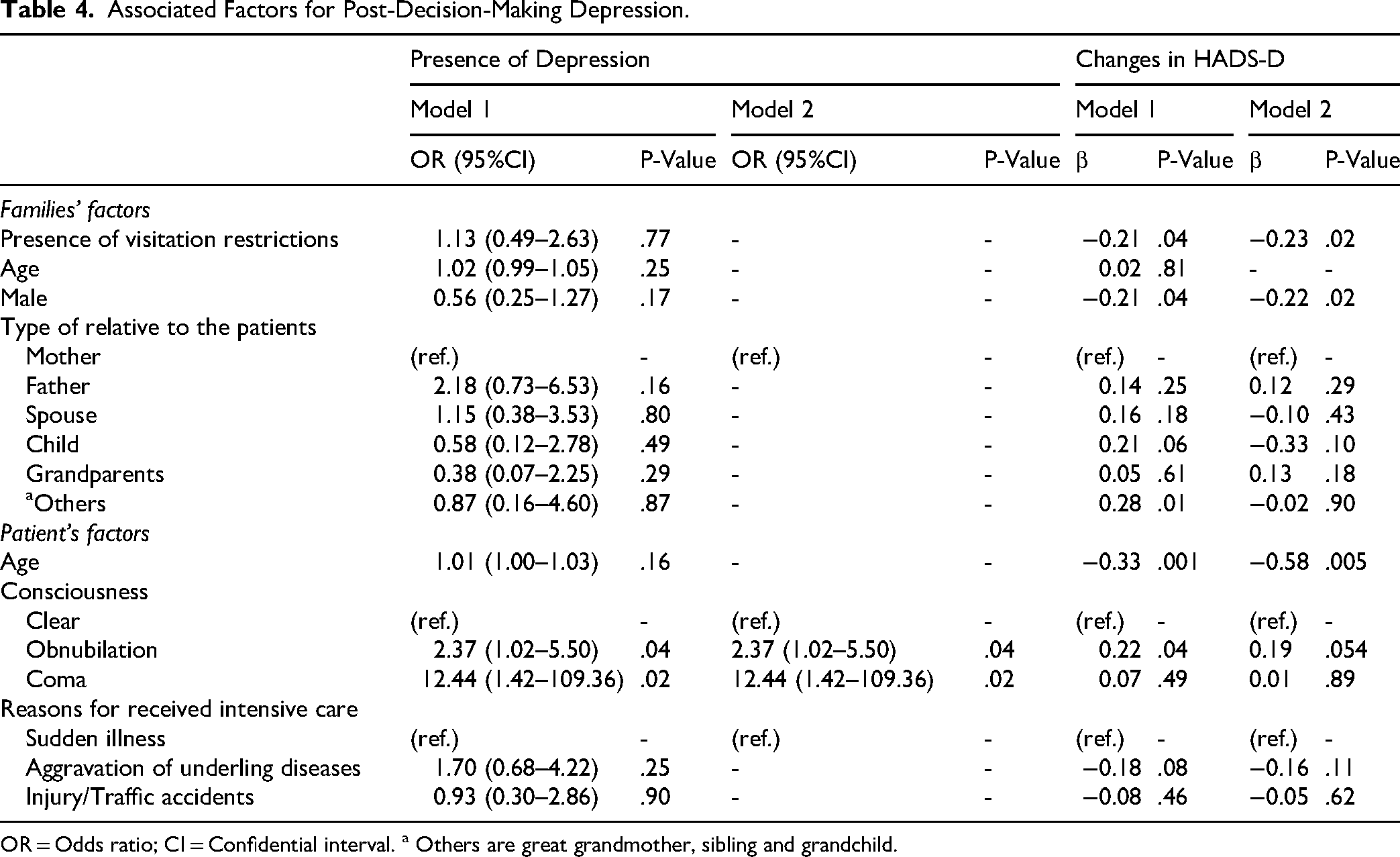
OR = Odds ratio; CI = Confidential interval. a Others are great grandmother, sibling and grandchild.
The presence of post-decision-making depression was associated only with poor consciousness levels (See Table 4). The post-decision-making change in the HADS-D score (i.e., changes as %) was suggestively associated with visitation restrictions, participant's age and sex, and the patient's age (β = −0.23, p = .02; β = −0.22, p = .02; and β = −0.58, p = .005; respectively; See Table 4).
Discussion
To the best of our knowledge, this is the first cross-sectional study showing the effects of visitation restrictions on post-decision-making anxiety and depression in family members with a patient admitted to the CCU. The presence of visitation restrictions was associated with the presence of post-decision-making depression in the family members, whereas visitation ability was associated with post-decision-making worsening of the HADS-D level. These results indicated that the circumstances of visitation restrictions have varying effects on post-decision-making anxiety and depression of the family members with a patient admitted to the CCU.
This study showed that 35.3% and 12.5% of the family members in the visitation restrictions and w/o visitation restrictions groups, respectively, had post-decision-making anxiety. A previous intensive care unit-based study, which included family members without visitation restrictions, showed that symptoms of anxiety were observed in 13% of the cohort (Metzger et al., 2019), in consistency with our findings. Moreover, another study reported that the incidence of anxiety during intensive care unit admission was 42–80%, which was higher than the incidence observed in this study (van Beusekom et al., 2016). The reason for the high presence of anxiety, even in this study, might be attributable to differences in the characteristics of the family members/patients. Anxiety in the family members warrants intervention. Blok et al. evaluated participants who had a patient admitted to the intensive care unit with anxiety; these family members reported the following: “It is a very anxious, stressful thing to constantly be waiting and watching and not knowing what's going to happen next” (Blok et al., 2023). Furthermore, visitation restrictions, owing to the COVID-19 pandemic, were associated with less understanding of complex medical needs and realistic expectations of the patient (Forsberg et al., 2023; Montauk & Kuhl, 2020). These results indicated that the degree of information might affect the anxiety level in the family members and highlighted that visitation restrictions would be an obstacle to getting information, as the family member cannot directly and correctly assess the patient's situation and gets information only from the medical staff (Creutzfeldt et al., 2021). Notably, this study showed that w/o visitation restrictions group without anxiety prior to decision-making did not develop new-onset anxiety after the decision-making, whereas 17.4% of those with visitation restrictions had new-onset anxiety after decision-making. This different trend of anxiety between the visitation restrictions and w/o visitation restrictions groups might be one of the reasons for the association between post-decision-making visitation restrictions and anxiety in the multivariate analysis. Therefore, more attention to the family members without anxiety before the decision-making and those with visitation restrictions is needed.
Furthermore, this study showed the association between the presence of visitation restrictions and changes in depression severity after decision-making in the family members. The exact reason for the result remains unclear, although potential reasons may include: perceived stress in the intensive care unit was associated with depressive symptoms in the family members (Fortunatti et al., 2023). It could be speculated that family members might experience significant post-decision-making stress when directly meeting the hospitalized patient. Moreover, witnessing treatments, such as the use of psychotropic drugs or attached monitoring lines/wires, had an impact on depressive symptoms in the family members (Kirshbaum-Moriah et al., 2018; Metzger et al., 2019). These studies indicated that visual information, which could be acquired from visiting, may have more impact than non-visual information, such as explanations from the medical staff (Creutzfeldt et al., 2021). The differences in the impact of information between the situations of visitation restrictions and those without visitation restrictions may have caused variations in the changes of depressive severity after decision-making among the groups in this study.
Limitations of Study
This study had some limitations. The sample size was relatively small for the multivariate analysis, which could lead to a type-II error. The sex variable was not included in the general linear analysis because of the multicollinearity with the sex of the family members, which could potentially distort the results of this study. This study was based on recall, as completing the questionnaire during a critical situation would have been difficult and ethically unfeasible. The findings were based on self-report, which could lead to social desirability and measurement bias. The questionnaire was online, limiting participation to people with Internet access and facility. The convenience sampling method could lead to selection and response bias. Further studies are required to address these limitations.
Regarding the levels of consciousness, we scaled the levels of consciousness in the patients as “clear,” “obnubilation,” and “coma,” although we recognized that showing levels of consciousness using scales such as the Glasgow Coma Scale would be more understandable for medical staff. But the goal of this study was to assess the effects of visitation restrictions on post-decision-making anxiety and depression in the family members of patients, not medical staff; we believed that people without a medical background would recognize levels of consciousness in the patients as “clear,” “being obtunded,” or “coma.”
Conclusion
Family members with a patient admitted to the CCU who experienced visitation restrictions reported higher post-decision-making anxiety levels, while those without such restrictions faced higher post-decision-making depression levels. Recognizing these distinct trends in post-decision-making anxiety and depression might be important for the prevention and/or management of mental distress in family members of patients admitted to the CCU.
Footnotes
Acknowledgements
None
Author contribution(s)
Ethical Approval and Informed Consent
Informed consent was obtained from each participant through a consent field on the associated webpage. This study was approved by the Ethical Committee for Epidemiology of Hiroshima University (#E2022-0093) and conducted in accordance with the Declaration of Helsinki. Participants were provided with detailed information regarding the purpose of the study, the nature of the data being collected, and how their responses would be used for research purposes only. They were explicitly informed that all data would be anonymized and handled confidentially, ensuring that no personally identifiable information would be disclosed in any publications. Furthermore, participants were assured their participation was entirely voluntary and that they could withdraw during the answering the questionnaire at any time without any penalty or adverse consequences.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.