
Abstract
Highlights
Waterborne and vector-borne diseases are on the rise due to climate change. Climate-induced declines in agricultural output jeopardize food security and livelihoods, with negative consequences for community health and socioeconomic stability. Home-visiting programs confront numerous hurdles to service delivery and must create flexible, accessible delivery approaches. Extreme weather puts physical hardship on home-visiting nurses and poses safety issues.
Climate change is one of the biggest health threats facing humanity, and health professionals worldwide are already responding to the health harms caused by this unfolding crisis (World Health Organization, 2021). The Earth's average surface temperature has risen about 1.2°C since the late nineteenth century, with most of the warming occurring in the past few decades (Noor et al., 2021). There is an increasing frequency and intensity of extreme weather events, including hurricanes, droughts, heat waves, and heavy rainfall events (Intergovernmental Panel on Climate Change [IPCC], 2021). Climate change is affecting ecosystems and biodiversity, leading to shifts in species distributions, changes in natural habitats, and disruptions to food chains through frequent extreme weather events, such as heat waves, storms, and floods (Díaz et al., 2019). These climate-sensitive health risks are disproportionately felt by the most vulnerable, including women, children, ethnic minorities, poor communities, migrants or displaced persons, older populations, and those with underlying health conditions (World Health Organization, 2021). Accordingly, more than 930 million people in the world's population spend at least 10% of their household budget to pay for health care. This burden is further affected by climate change, resulting in more disease conditions. Research shows that approximately 706 heat-related deaths occurred each year from 2004 to 2018 (Vaidyanathan et al., 2020).
Climate change affects the work of public health nurses (PHNs), especially those in rural communities engaged in home-visiting programs (Nies, 2015). Home visiting is a key strategy used by community health nurses to provide preventive care and support to families with young children (Diema Konlan et al., 2021). Climate change not only disrupts the lives of PHNs, but also makes their jobs more challenging, raising the risk of burnout. Storms, floods, wildfires, and other extreme events often prevent them from traveling to health-care facilities or communities to render services (IPCC, 2021).
Climate change is one of the major factors making home visiting more challenging and complex (Sokey & Adisah-Atta, 2017). The escalating impacts of climate change pose a critical threat to the accessibility and effectiveness of home-visiting health-care services in most parts of Ghana. As extreme weather events become more frequent and intense, disruptions in transportation, infrastructure, and living conditions hinder PHNs’ ability to reach and serve vulnerable populations, including the elderly, children, and those with other special health needs. Climate change contributes to the increase in the prevalence of certain health conditions, such as heat stress and vector-borne diseases, which makes home visiting more time-consuming and demanding (Paavola, 2017).
Though climate change is known to affect every aspect of life and work, including health-care services, it is not clear how the changes affect the activities of PHNs during home visits in the Ho Municipality. This phenomenon and its problems necessitate an in-depth examination of the specific challenges and potential solutions to mitigate the adverse effects of climate change on home visiting, especially in a local Ghanaian context.
Purpose
The purpose of this study was to explore the effects of climate change on home visit practices of public health nurses in the Ho Municipality, Ghana.
Methods
Study Design
This study employed a qualitative descriptive design to examine the effects of climate change on the home visiting program in the Ho municipality. This design is suitable because it allows for an in-depth exploration of the phenomenon of interest, staying close to participants’ perspectives and operating within a naturalistic setting (Doyle et al., 2020).
Sampling, Study Population, and Data Collection Procedure
Eligibility for participation was limited to community/PHNs with a minimum of 1 year of work experience who performed home visits and were working in Ho Municipal Hospital, Ho Polyclinic, Hopedo Community-based Health Planning and Services (CHPS), Deme CHPS, or Akoefe CHPS at the time of the study. The size of our study population was guided by the point of data saturation, which occurs when additional data no longer yields new or relevant information or insights (Fusch & Ness, 2015). In this study, inductive thematic saturation was employed, as data collection and analysis were conducted concurrently, and no new themes emerged after successive interviews; this approach ensured that the findings adequately captured the range of participants’ experiences while maintaining depth and richness in the data (Braun & Clarke, 2021).
A purposive sampling method was used to recruit 19 PHNs from the Ho Municipality. According to records, 162 Public/Community Health Nurses were working within the municipality during the study period (Ho Municipal Assembly, 2022). The participants were purposively selected based on their eligibility and ability to provide rich information relevant to the study objectives. Interviews were conducted until data saturation was achieved.
Data were collected through semistructured interviews. An interview guide comprising participants’ demographic characteristics and questions relating to the experiences, challenges, and coping strategies of PHNs regarding climate change and home visiting in the Ho Municipality was used. The study details and procedures were explained to each participant in clear and simple language, and informed consent was obtained. With participants’ approval, the interviews were audio-recorded and subsequently transcribed verbatim in sequence for analysis.
Data Analysis
The audio-recorded data was transcribed verbatim. In this study, Braun and Clarke's six-step process of thematic analysis was employed to analyze the data (Braun & Clarke, 2019). The process began with familiarization, where the researchers immersed themselves in the data by repeatedly reading the transcriptions to gain a deep understanding. Next, initial codes were generated to identify significant features within the data. Before and during the coding process, the first, second, and fourth authors coded the same interviews to identify and discuss differences and check for intercoder reliability. These codes were then organized into potential themes, which were reviewed and refined by all authors to ensure they accurately captured the essence of the data. The themes were clearly defined and named before the final step of producing the report, where the analysis was presented in a coherent narrative linked to the research questions. All authors were involved in all steps of the data analysis, including agreeing on the themes collectively. This iterative process reflects the reflexive thematic analysis tradition, in which codes and themes are developed during the analytic process rather than imposed before coding begins, and where the researcher's interpretations contribute to shaping those themes.
Rigor
This qualitative research design, essential for trustworthiness, involved strategies like purposive sampling, iterative analysis, reflexivity, audit trails, peer debriefing, and data saturation (Johnson et al., 2020). These enhance credibility, dependability, confirmability, and transferability of findings (Forero et al., 2018). Credibility was ensured through the authors’ checking, triangulation, and prolonged engagement (Cope, 2014). Dependability was strengthened by audit trails and triangulation, while confirmability was enhanced by reflexivity and peer debriefing (Awan et al., 2023). Transferability was supported by providing detailed descriptions of data, context, and assumptions (Younas et al., 2023).
Ethical Considerations
Ethical approval for the study was granted by the Research and Ethics Committee of the University of Health and Allied Health Sciences (UHAS-REC A.3[9] 23-24). Permission was obtained from the Nurse Managers of the selected hospitals, as well as the selected CHPS compounds, before the start of the study in the facilities. Before participation, all eligible participants received detailed information about the study, including its purpose, procedures, potential benefits and risks, and their rights as research participants. They were assured that participation was entirely voluntary, that they could withdraw from the study at any stage without penalty, and that measures would be taken to ensure confidentiality and anonymity of their responses. After having the opportunity to ask questions and seek clarification, participants provided written informed consent before data collection.
Results
Quantitative Data
Table 1 presents the sociodemographic characteristics of participants.
Sociodemographic Characteristics of Participants.
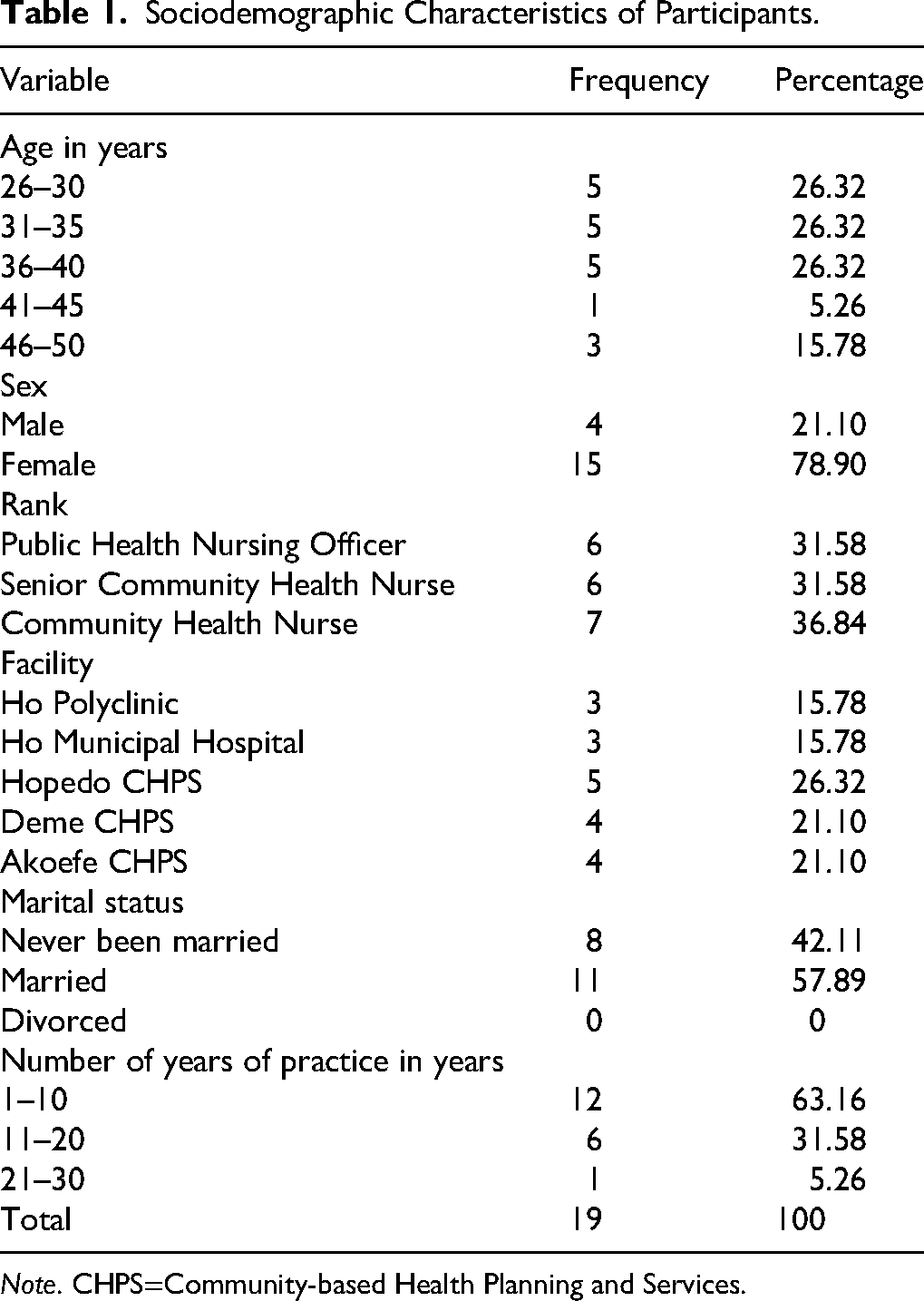
Note. CHPS=Community-based Health Planning and Services.
Themes
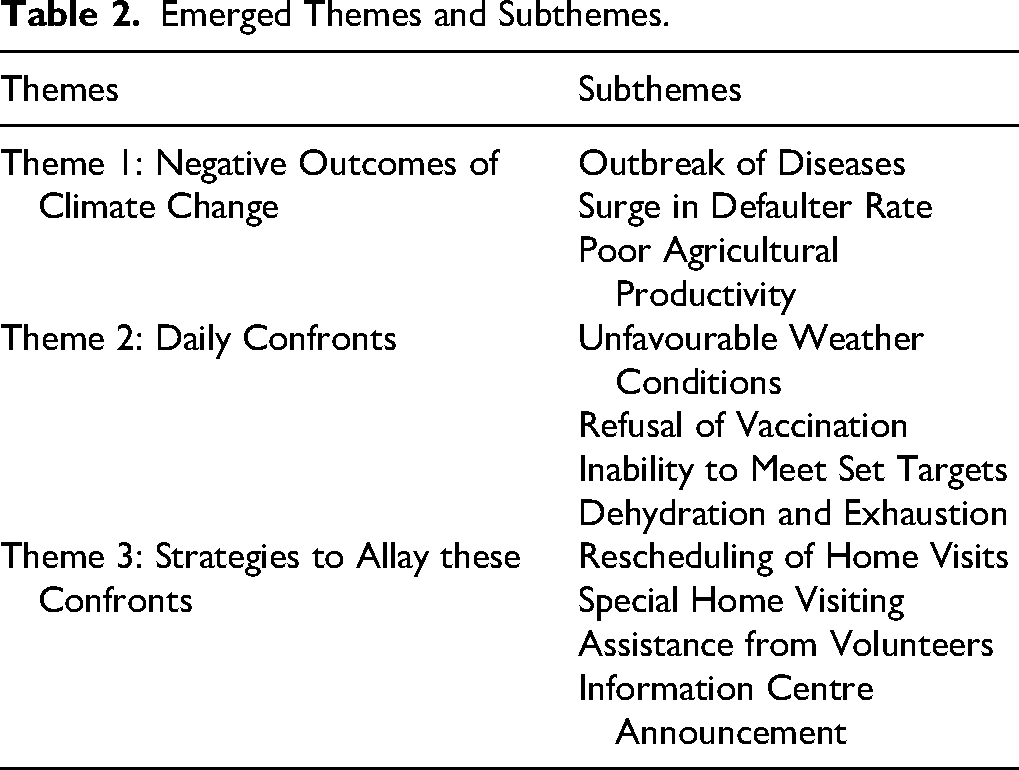
Table 2 presents an analysis of data that generated three major themes with a total of 11 subthemes.
Emerged Themes and Subthemes.
Theme 1: Negative Outcomes of Climate Change
The repercussions of climate change significantly influence the execution of the home visiting program administered by public health nurses. Among the notable outcomes highlighted by the participants, the most commonly identified outcomes of climate change include the outbreak of diseases, a surge in defaulters, and poor agricultural productivity.
Subtheme: Outbreak of Diseases. Alterations in the climate and weather conditions within the municipality, as highlighted by the participants, have culminated in the emergence of diverse health complications such as malaria, cough, skin rashes, and other related ailments. Their insights are encapsulated in the following excerpts: Climate change has altered the raining pattern and the amount of rainfall. When it rains too much, and the whole place is flooded, we meet lots of people with malaria, as well as cold and coughing due to excessive wind. So yeah, climate changes are leading to global health problems. (Participant F) The wind carries a lot of dust, which causes many people to develop colds. The heavy rainfall also leads to erosion and destruction of farms, resulting in a risk of an unhealthy diet. When excessive rainfall is recorded, cholera is usually one of the conditions that we notice in the community. Malaria cases are also high. (Participant J)
One participant highlighted how climate change has triggered a surge in immigration rates, consequently causing overcrowding. This situation, particularly within confined spaces, has contributed to the spread of communicable diseases. Climate change has led lots of immigrants into the community resulting in overcrowding in rooms, increasing the risk of spreading of infection. In this community, you could find about 7 adults living in one single room. If one should get an infectious disease, before you know everyone would have gotten it too. (Participant C)
Subtheme: Surge in Defaulter Rate. Participants informed that there has been a noticeable surge in the number of individuals failing to attend these crucial home-based initiatives, designed to provide essential support and guidance to vulnerable communities. Participants said: Most people don’t come to the facility to access health care due to excessive rain, or extreme heat which induces rashes. And when we go to the communities too, they are nowhere to be found. (Participant H) This is a farming community, so people don’t come to the facility when it's raining heavily, leading to defaulters. And that is why home visits is necessary, but it will interest you to know that we visit their homes and they are not at home. Most of them go to farms. No one knows when the rain will stop, so everyone wants to plant something before the rain ceases. (Participant B)
Subtheme: Poor Agricultural Productivity. Shifts in temperature, erratic rainfall patterns, and the prevalence of extreme weather events have disrupted traditional farming practices and jeopardized the stability of agricultural systems. These adverse conditions have reduced harvests, increased crop failures, and susceptibility to pests and diseases, posing a serious threat to food security and livelihoods in affected regions. Climate change has impacted on the health of the community in many ways. An example is that climate change has affected the growth of food crops in the community. Because of the unpredictable weather conditions, farmers are not able to plan crops at appropriate times, and crops are sometimes destroyed by the weather or the crops grow poorly. (Participant N) Yes, climate change affects the health of the community. Unstable weather conditions have contributed to low yields on farms; hence, malnutrition is usually recorded in this community during home visits. Because members of this community rely mainly on their farm produce for money, adverse weather conditions make it difficult for them to pay for healthcare for sick family members. Pressure, therefore, falls heavily on public health nurses during home visits” (Participant L)
Theme 2: Daily Confronts
The public health nurses, in their open dialogue, shed light on the diverse set of hurdles they confront in the line of their essential duty. Specifically, their accounts underscored the demanding nature of contending with unpredictable and adverse weather conditions, as well as the complexities surrounding addressing cases of vaccine refusal within the communities they serve.
Subtheme: Unfavorable Weather Conditions. The nurses reported that sudden weather changes, such as heavy rain or intense heat waves, significantly hinder the success of home visiting programs. They highlighted the risks of traveling in heavy rain, which often forces them to cancel or cut visits short when unexpected rain disrupts their sessions. These quotes are their testimonials: We are not able to go to the community sometimes due to heavy rain because we always walk and we don’t sit in cars or on a motorcycle, we also hide under the shade of trees, especially during the scorching sun, because our home visiting services are done under the trees, sometimes, we will get to the community and it will start raining which means that you can’t render services or you might start but the rain will stop you. (Participant E) When it rains heavily, we are unable to go to the community and therefore cannot meet our targets. There is also a risk of falling due to slippery ground conditions caused by rainfall. In addition, we become very exhausted when travelling to some communities, since we usually walk long distances to provide home visiting services. (Participant F)
Some participants reported that adverse weather conditions, such as extreme temperatures and heavy precipitation, have caused logistical issues that led to significant vaccine wastage, undermining public health efforts. Weather events such as rain, sometimes extreme, destroy the items needed to provide care services. Too hot weather usually threatens the potency of vaccines. All those factors sometimes make it difficult for PHNs to render effective services during visits. (Participant J)
Participants noted that unpredictable and extreme weather conditions have disrupted the home visiting program, making it difficult to reach vulnerable communities. First of all, PHNs are not able to give the best service to the community due to extreme weather events like heavy rainfall and extremely high temperatures. For example, children younger than 5 years may not be vaccinated because PHNs have not gone for home visit. Elderly people who may need care or support, like replenishing their medications, may have difficulties because climate change has prevented these home visits. (Participant J)
Subtheme: Refusal of Vaccination. According to the participants’ accounts, there have been instances where individuals declined vaccination during home visits, often citing extreme weather conditions such as excessive heat or cold as their primary reason for refusal, while others are just not available at the scheduled location and time. They said: Everyone has rights. For vaccinations, too, you must seek consent. It happened on some occasions that some people refused an injection due to excessive heat. So, there was nothing we could do but just move on. (Participant H) We are not able to get people immunized, and it's hard to trace defaulters. Some will intentionally not be available because they don’t want the vaccine. That is why we keep educating community members on why they should be immunized. (Participant E)
Furthermore, other participants highlighted that the refusal of vaccination has led to the unfortunate wastage of valuable vaccine doses, explaining that once certain vaccines are prepared and remain unused beyond a specific time frame, they become unusable, with extreme heat also exacerbating this issue. The cold chain system is affected by this behavior. The vaccines we bring to the community have an allocated potent period when we constitute it. So, when we do, and the people don’t take it, the drug becomes wasted. (Participant B)
Subtheme: Inability to Meet Set Targets. Home visiting nurses face challenges in meeting program targets due to unpredictable weather patterns, including heavy rainfall and heatwaves, disrupting scheduled visits and affecting timely care provision to beneficiaries, consequently hindering their efforts in providing essential health-care services to vulnerable communities. Climate change affects the targets or goals of home visiting. For instance, if the goal for a particular visit day is to reach 10 homes, it could be reduced to about 5 homes due to climate issues. Sometimes, weather events such as heavy rainfall prevent the visit from happening. (Participant M) Yes, the hot weather can interfere with effective home visits. A very good example happened today. Today, we decided to go on home visits in one particular area of the Akoefe community. On our way to the community, we could not bear the heat anymore and decided to join public transport, which took us to the location. Because we took public transport, multiple stops could not be made on the way to check on the people away from the final destination. We probably missed some clients who needed health-care services. Our target for the day was also not met. (Participant L)
Subtheme: Dehydration and Exhaustion. In conjunction with existing obstacles, home-visiting nurses contended with additional burdens of dehydration and exhaustion, which amplified the difficulties of their work, leading to prolonged physical exertion and exposure to extreme temperatures, ultimately impeding their ability to provide optimal care and posing risks to their own health and well-being. Walking under the hot sun is one of the most difficult challenges during home visits. This makes us burn out easily and even causes us to dehydrate. Heavy rain also causes delays, as we have to stop for minutes or hours under shaded structures and continue the journey when the rain goes down. The rain mostly destroys pathways used for the visits and therefore interferes with walking. (Participant L) “Extreme weather events first of all makes the PHN uncomfortable. For instance, hot weather may make PHNs sweat profusely and cause dehydration when moving from home to home. A dehydrated and physically uncomfortable nurse is likely not to give you the best of service. (Participant J)
Theme 3: Strategies to Allay These Negative Outcomes
Despite numerous obstacles, participants showed unwavering determination and resilient commitment to sustaining home visiting programs. This theme explores the adaptive strategies they employed to navigate challenges and ensure continued community care. Noteworthy approaches include strategic rescheduling of visits, implementing specialized visitation methods, leveraging support from dedicated volunteers, and disseminating critical information through local information centers. These measures reflect their dedication to overcoming the hurdles posed by climate change in home visiting initiatives.
Subtheme: Rescheduling of Home Visits. Many participants emphasized frequently rescheduling visits due to adverse weather. This adaptive measure accommodates unpredictable weather and varying community member availability. The strategy we employed to adapt to the changing climate conditions during our home visits, we reschedule our itinerary, and we do mop up. (Participant E) One major strategy we have adopted is changing or rescheduling visiting hours. For instance, when the weather is expected to be hot, we usually schedule our visits very early in the morning and end the visit before the temperature becomes unbearable. For rainy days, we reschedule to days that will be favorable. (Participant N)
Participants also emphasized practical adaptation strategies, such as consistently carrying umbrellas to mitigate challenges posed by scorching heat and unexpected rainfall. We have umbrellas that we use when the sun is scorching or it's not raining heavily, we have observed the rain pattern to reschedule our itinerary. (Participant I)
Subtheme: Special Home Visiting. Home-visiting nurses have adopted a targeted strategy, focusing on specific individuals in the community who need assistance rather than conducting routine visits throughout the entire community. This approach allows them to allocate resources more efficiently, directing efforts toward those needing immediate attention and support. We don’t go as often as we used to, we also visit a few houses, and most of the time we do special home visits rather than routine ones. (Participant A) We used to do routine home visits in the communities, but with these changes in rainfall, we resorted to special home visits. When we get reports on individual people, we visit them and render the needed care to them. (Participant L)
Subtheme: Assistance from Volunteers. The active involvement of community volunteers has been instrumental in supporting the home visiting program and aiding nurses. This collaborative approach has facilitated the execution of tasks, reducing the challenges of the home visiting program. Participants said: The community knows that we cannot be with them every day, so they gave us able people who can assist us. We partner with local volunteers in the community who assist us when it rains. (Participant C) It would have been very cumbersome, but we have volunteers in the communities now who help us reach out to the community members. So, on days that are crucial yet we cannot go because of climate change issues, we inform these volunteers to step in for us. They are good; we trained them. (Participant B) The community is helping in its own way to help improve home visiting service and health in general. For instance, members of the community who have been educated on a particular topic help spread the education to other members of the community, thereby reducing the workload on us to educate others, especially during bad weather events e.g., a mother who has practiced exclusive breastfeeding educated other mothers on the importance of the practice. (Participant K)
Subtheme: Information Center Announcement. Participants highlighted the strategic use of community information centers to broadcast impending visits, alerting residents and encouraging participation. Leveraging these hubs enabled the dissemination of vital details and schedules, ensuring community members were well-informed and prepared. The quotes below represent their voices. We work with opinion leaders in the communities. They provide places for us to provide services. They also give us directions when we go into the community. There are community information centers as well. (Participant R) We use community information centers to announce our coming to the community. We also use mosques to render services. We tell those in charge of the announcements to do it at specific times during the day. (Participant C) The community provides information centers where information and other forms of education are made. It helps us a lot, so we don’t need to move from house to house. We just make it there, and everyone is captured. (Participant P)
Participants also emphasized the practice of making personalized calls to individuals and families scheduled for home visits. This direct outreach established intimate communication, fostering rapport and trust. So, we call the clients to inform them about our coming or that of the volunteers. When we reschedule a visit, a day before the date, we call them; even though the information center will broadcast our coming, we don’t want anyone to say he/she didn’t hear. (Participant B)
Discussion
Findings revealed that climate change creates favorable conditions for disease vectors and the spread of diseases like malaria, diarrhea, and heat-related illnesses. This finding agrees with Coates et al. (2020), wherein the outbreak of similar conditions was spelled out. The exacerbation of shifting temperature and rainfall patterns, according to Acosta et al. (2018) has also posed a significant health risk, necessitating the implementation of preventive measures such as the distribution of bed nets and the promotion of insecticide use. Similarly, the increased incidence of diarrhea, a waterborne illness influenced by altered water sources and sanitation facilities, was revealed by Muñoz-Millán et al. (2018). Zawiah Mansor et al. (2019) sought nurses to educate communities on effective heat prevention strategies to overcome heat rashes and similar conditions stemming from elevated temperatures.
The challenge of patients defaulting in home visiting programs often stems from competing priorities, including agricultural responsibilities and limited access to transportation, which can hinder participants from attending scheduled meetings, as suggested by Diema Konlan et al. (2021). To address this issue, implementing tailored strategies becomes crucial. These strategies may include offering flexible scheduling options that accommodate participants’ daily routines and work commitments (Irani et al., 2018), fostering community engagement to build trust and support for health-care initiatives (Laurenzi et al., 2021), introducing mobile clinics or outreach services to improve accessibility in rural areas (Tulimiero et al., 2021), and enhancing communication and education efforts to emphasize the importance of regular health-care visits (Burgdorf et al., 2022).
Climate change poses significant threats to global food security, with rising temperatures, erratic rainfall patterns, soil degradation, increased pest pressures, and extreme weather events adversely impacting agricultural productivity and crop yields, as found in the current study. In the studies of Molotoks et al. (2021) and Richards et al. (2021), smallholder farmers, in particular, bear the brunt of these challenges, facing increased risks of crop failure, reduced harvests, and income loss. The implications of poor agricultural productivity extend beyond food availability, affecting livelihoods, rural economies, and the overall socioeconomic well-being of communities dependent on agriculture. These effects collectively affect the health of people in the communities, as published by Manning and Clayton (2018).
Home-visiting nurses often encounter challenges related to unfavorable weather conditions, particularly during extreme climate events such as heatwaves, storms, or heavy rainfall. These adverse weather patterns can impede travel to remote or vulnerable communities, affecting the timely delivery of health-care services and posing risks to the safety and well-being of both nurses and patients. Perera et al. (2020) suggest that strategies such as the pre-identification of high-risk areas prone to weather-related disruptions and the development of contingency plans for alternative service delivery methods can enhance the resilience of home health-care systems in the face of adverse weather conditions.
The refusal of vaccination by some individuals or communities poses a significant challenge for home-visiting nurses striving to promote preventive health-care measures, particularly in the context of emerging public health concerns and vaccination campaigns. Misinformation, cultural beliefs, and mistrust in health-care systems often contribute to vaccine hesitancy and refusal. Galagali et al. (2022) conducted a comprehensive review of vaccine hesitancy, identifying similar factors contributing to the reluctance of individuals to accept vaccines. The study highlighted concerns such as misinformation, mistrust in health-care systems, and fear of adverse effects as key drivers of vaccine hesitancy. Others may express a general distrust in the health-care system, leading to skepticism about the necessity and efficacy of vaccines (Hornsey et al., 2020). The refusal of vaccines during home visits not only poses risks to the individuals who decline vaccination but also jeopardizes community immunity, making it easier for preventable diseases to spread. In response to these challenges, health-care providers conducting home visits must be equipped with tailored communication strategies that address the specific concerns and beliefs of the individuals they encounter (Brooks et al., 2020).
Home-visiting nurses face health challenges such as physical strains, dehydration, and exhaustion. The demanding nature of home-based care, coupled with extended work hours and travel, contributes to physical strain and burnout among nurses, potentially compromising the quality of care. The above findings are in line with Moradi et al. (2021) and Ziemann et al. (2023). Strategies like weather-related risk assessments and support systems for hydration and rest breaks are vital in ensuring nurses can navigate these challenges, sustain their well-being, and continue to provide high-quality care to patients in home settings (Maben & Bridges, 2020).
Home-visiting programs often employ rescheduling as a coping mechanism to accommodate unforeseen circumstances, such as unfavorable weather conditions or logistical challenges, that may hinder the timely provision of health-care services. Rescheduling allows for the flexible adjustment of home visit appointments, enabling nurses to prioritize patient needs and ensure the continuity of care without compromising health-care services’ quality and effectiveness (Irani et al., 2018). Also, the implementation of special home visiting initiatives serves as a proactive coping mechanism. Special home visiting programs often target specific at-risk populations, including the elderly, individuals with chronic illnesses, and those living in remote or disaster-prone areas, to provide tailored and comprehensive health-care services that prioritize their safety and well-being (Schuchman et al., 2018). In addition, engaging volunteers as a coping mechanism is pivotal in supporting the delivery of home-based health-care services, particularly in times of increased demand, resource constraints, or operational challenges. Volunteers contribute to various aspects of home visiting programs, including patient support, community outreach, and the facilitation of health-care activities (Woldie et al., 2018).
Information center announcements also served as a vital communication tool and coping mechanism to disseminate timely and relevant health-care information, updates, and guidance to communities, home-visiting nurses, and stakeholders involved in health-care delivery, aligning with Morris et al. (2020).
Limitations
The 19 nurses interviewed were a purposive sample, which limits generalizability of the findings.
Implications
The study calls for more studies exploring climate change's intersectionality with health and tailored strategies for mitigating challenges faced by home-visiting nurses. Nursing education should integrate climate change impacts, gender diversity, and skills to handle weather-related disruptions. The study also advocates for resources for climate-affected areas, sustainable practices, reliable transport for nurses, and strategies to combat vaccine hesitancy, aligning nursing policies with the dynamic health-care landscape shaped by climate change.
Recommendations
The study's recommendations include incorporating diversity training into nursing curricula, creating health-care plans that are climate resilient, looking into the long-term coping strategies of home-visiting nurses, pushing for sustainable practices in nursing policies, and promoting interdisciplinary collaboration.
Footnotes
Acknowledgments
The authors are most grateful to the participants who took part in the study.
Author Contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.